
Abstract
Background:
Voxel-based morphometry studies have not yielded consistent results among patients with mild cognitive impairment (MCI) and subjective cognitive decline (SCD).
Objective:
Therefore, we aimed to conduct a meta-analysis of gray matter (GM) abnormalities acquired from these studies to determine their respective neuroanatomical changes.
Methods:
We systematically searched for voxel-based whole-brain morphometry studies that compared MCI or SCD subjects with healthy controls in PubMed, Web of Science, and EMBASE databases. We used the coordinate-based method of activation likelihood estimation to determine GM changes in SCD, MCI, and MCI sub-groups (amnestic MCI and non-amnestic MCI).
Results:
A total of 45 studies were included in our meta-analysis. In the MCI group, we found structural atrophy of the bilateral hippocampus, parahippocampal gyrus (PHG), amygdala, right lateral globus pallidus, right insula, and left middle temporal gyrus. The aMCI group exhibited GM atrophy in the bilateral hippocampus, PHG, and amygdala. The naMCI group presented with structural atrophy in the right putamen, right insula, right precentral gyrus, left medial/superior frontal gyrus, and left anterior cingulate. The right lingual gyrus, right cuneus, and left medial frontal gyrus were atrophic GM regions in the SCD group.
Conclusion:
Our meta-analysis identified unique patterns of neuroanatomical alternations in both the MCI and SCD group. Structural changes in SCD patients provide new evidence for the notion that subtle impairment of visual function, perception, and cognition may be related to early signs of cognitive impairment. In addition, our findings provide a foundation for future targeted interventions at different stages of preclinical Alzheimer’s disease.
Keywords
INTRODUCTION
Alzheimer’s disease (AD), which is characterized by progressive memory decline and impairment of other cognitive functions, is currently considered the most common type of dementia [1, 2]. The number of dementia cases is estimated to reach 135 million by 2050, and brings enormous economic burden and decline in the quality of life of patients and their families reported by the Alzheimer’s Association (https://www.alz.org). Unfortunately, there has been no effective treatment that can alleviate the progression of AD and effectively improve cognitive function in AD patients. Thus, the researchers have turned their attention to studying the preclinical stages of AD spectrum, which are known as mild cognitive impairment (MCI) and subjective cognitive decline (SCD) [3, 4].
MCI, the preclinical stage of AD, is an intermediate state between normal age-related cognitive decline and dementia [5]. Approximately 10–15% of patients with MCI progress to dementia annually, compared to only 1–2% of healthy people [6]. A recent review, which included patients with MCI across 33 cohort studies, found that 34% of MCI patients progress to AD in an average clinical follow-up time ranging from 1 year to 7.6 years (median of 2 years) [7]. According to the presence or absence of memory impairment, MCI has been divided into amnestic mild cognitive impairment (aMCI) and non-amnestic mild cognitive impairment (naMCI) [8]. The aMCI subtype of MCI is characterized by memory deficits and either accompanied by or not subtle impairment of other cognitive functional domains. Patients with aMCI are at a higher risk of converting to AD compared to the naMCI subtype, which has been defined as non-memory domain decline in which patients can progress to non-AD dementia, including frontotemporal dementia (FTD), dementia with Lewy bodies (DLB), and vascular dementia (VaD) [8 –11]. The explosion of studies that have focused on structural brain changes in MCI patients compared to healthy controls (HCs) in recent decades have found gray matter (GM) atrophy in several region of the brain, though results have not been exactly consistent. Some studies reported brain atrophy in relative concentrated regions of the medial temporal lobe (MTL), including hippocampus, parahippocampal gyrus (PHG), and amygdala [12 –15]. However, in some studies, GM loss has been found in regions of the temporal lobe, frontal lobe, precentral gyrus, and insular and subcortical regions such as lentiform nucleus and putamen [15 –18]. SCD is defined as a state of self-aware cognitive decline without any evidence of objective cognitive impairment, and is currently considered a very early stage of the preclinical AD spectrum [19, 20]. Approximately 2.3% and 6.6% of the elderly patients with cognitive decline complaints progress to dementia and MCI per year, respectively, and the progression rate is twice than that of healthy people without SCD [21]. Based on these credible studies which state that SCD represents very early clinical manifestations of the AD spectrum, it is important to pay attention to the elderly with SCD, as it may provide a critical opportunity to delay or even prevent the progression of this disease. Additionally, structural change studies in SCD patients have revealed heterogeneous GM loss regions, including the hippocampus [22], precentral gyrus [15], temporal/frontal gyrus and cuneus [23]. These inconsistent findings in MCI and SCD studies have continued to confuse people that have a deep understanding of these diseases. Thus, it is necessary to bring together all existing studies respectively to explore the consistent areas of GM changes, which can help the scientific community better understand the neuroanatomical mechanism of MCI and SCD. Furthermore, our exploration of consistent neuroimaging changes in MCI and SCD are also crucial to its early detection and intervention, which may postpone progression to AD.
Magnetic resonance imaging (MRI) is considered a very important auxiliary diagnostic method that can detect structural changes that reflect neuronal and synaptic damage. Thus, MRI images have etiological and prognostic value across various diseases [24]. In addition, MRI has several advantages, including repeatability, non-invasiveness, and cost-effectiveness. Therefore, MRI is widely applied in clinical practice to make an auxiliary diagnosis of AD spectrum disease. Voxel-based morphology (VBM) method involves a comparison of voxelization of the local GM concentration between two groups, and is considered the most frequently-used method to evaluate brain structural changes between groups that are superior to regions-of-interest (ROI) volumetry and regional manual volumetry [25, 26]. Activation likelihood estimation (ALE) is a powerful coordinate-based meta-analysis method that treats the activation foci reported in neuroimaging studies as spatial probability distributions that are centered on given coordinates, rather than a single point, and calculates the union of the activation probabilities of each voxel to obtain the ALE map [27]. Previous whole brain-based VBM meta-analyses have used the ALE software in order to explore GM changes in patients with MCI compared to HCs [28 –31]. However, no researchers have done a meta-analysis of MCI-HCs with SCD-HCs to explore the longitudinal GM changes that occur in different stages of the preclinical AD spectrum. Thus, the purpose of this meta-analysis was to two-fold. First, we wanted to explore brain changes in patients with MCI and SCD, respectively. Secondly, we wanted to distinguish the similarities and differences of GM atrophic regions between SCD and MCI, and to explore whether these changes overlap and proceed along the progression of preclinical AD spectrum. Detecting convergent affected brain regions with structural changes in MCI and SCD would help better understand the longitudinal neuroanatomy mechanism of onset and progression of preclinical AD spectrum and provide an objective foundation to select effective targeted interventions for different stages of preclinical AD.
METHODS
Literature search
We acquired the scientific literature published from January 1, 1996 to March 20, 2020 by systematic and comprehensive searches in PubMed, Web of Science, and EMBASE databases. We used the following key words to retrieve potential articles: ‘mild cognitive impairment’, ‘amnestic mild cognitive impairment’, ‘MCI’, ‘aMCI’, ‘subjective cognitive decline’, ‘subjective cognitive complaint’, ‘subjective memory concern’, ‘subjective memory impairment’, ‘subjective cognitive impairment’, ‘subjective memory loss’, ‘subjective memory deterioration’, ‘SMC’, ‘SCD’, ‘Voxel-based Morphometry’, ‘VBM’, and ‘voxel’. The detailed search strategies are outlined in the Supplementary Material.
Study selection
Study selection was done independently by two authors (Shanshan Chen and Wenwen Xu) and verified by another two examinants (Jiu Chen and Xingjian Lin). The disagreements among the four reviewers were discussed until a consensus was reached. After retrieving potential papers, the authors removed duplicated articles, browsed the abstract and full text of the remaining articles, and identified studies that met our inclusion criteria. Studies were included in the meta-analysis if they 1) reported GM volume or GM density changes of patients with MCI or SCD in comparison to HCs (including subgroups of aMCI and naMCI), 2) used VBM method, 3) reported stereotactic space in Montreal Neurological Institute (MNI) or Talairach coordinates based on whole-brain analysis, and 4) were written in English in a peer-reviewed journal. The studies included in the MCI group met the following criteria, including 1) memory complaints by patients, which was verified by informants, 2) normal activities in daily life, 3) objective evidence indicating impairment in memory domain or in other domains of cognitive function, 4) CDR score = 0.5, and 5) absence of diagnostic criteria for dementia [5, 32]. Furthermore, we divided the MCI group into subtypes of aMCI and naMCI based on the clinical manifestations that were dominated by memory impairment or other symptoms other than memory impairment, such as executive and attention dysfunction [8]. Among studies that met the above criteria, if the data from patient groups from one study overlapped with inter-subgroups or from another study, we choose the largest group to incorporate into the meta-analysis.
We excluded papers from the meta-analysis if they 1) suffered from other diseases that may influence cognitive function (i.e., VaD, PD, and depression), 2) did not contain the sufficient information, even after contacting the corresponding author by email, and 3) number of subjects in any group was less than five. The detailed information of our retrieval process is shown in the flow chart (Fig. 1).

Flow chart showing study selection process.
Activation likelihood estimation
The meta-analysis was done using GingerALE version 3.0.2, which was based on the ALE method, for which more detailed information is available in BrainMap (http://www.brainmap.org) [33]. GingerALE was designed to determine whether there any anatomical or functional convergence among meta-analyses of human brain imaging studies, which was published with stereotactic MNI or Talairach space. In practical application, one of the difficulties in comparing different imaging studies is that the difference in positioning of the neuroanatomical area label leads to the uncertainty of the actual abnormal position, and thereby masks the site of true lesion. The merits of the ALE technique are that it uses the coordinates of the abnormal anatomical site, instead of labels, and thus neatly avoids the shortcoming [34]. Another benefit of this technique is that excluding negative data has little effect on the results [35]. We conducted four ALE meta-analyses, including in the SCD group, MCI group, and its sub-groups (aMCI and naMCI). Prior to calculation, we converted Talairach space into MNI coordinates using the “icbm2tal” transformation [36], which allowed these foci to be performed in MNI coordinates. We categorized the final studies into the MCI group, as well as its subgroups (including aMCI and naMCI group) or the SCD group. The foci extracted from each group were placed in independent text files, and imported into a software for calculation. ALE calculations were used to create a 3D image for each foci group. The foci and a Gaussian blur with a Full-Width Half Maximum (FWHM) was empirically acquired by subject size. We selected the cluster forming threshold at p < 0.001, with 1000 permutations, and a cluster-level family-wise error (FWE) correction at p < 0.05 to obtain the ALE map. It is worth noting that due to the small number of naMCI studies and SCD studies (including five studies and four studies respectively) and the use of uncorrected statistical thresholds, we used loose cluster forming threshold of p < 0.05 in the two groups. Finally, our ALE-maps were visualized by the MRIcron software (http://www.mricro.com). The Meta-Analysis was registered in advance on PROSPERO (https://www.crd.york.ac.uk/prospero/#recordDetails, registration number: CRD42020187491).
RESULTS
After careful screening, a total 45 publications, including 43 MCI studies and four SCD studies (two studies including MCI-HCs and SCD-HCs), were included in our meta-analysis. Overall, the studies that met the inclusion criteria included 1,396 subjects (1,262 MCI and 134 SCD patients) and 1,370 HCs. More detailed demographics and clinical characteristics of each study are illustrated in Table 1.
The demographics and clinical characteristics of 45 studies included in the meta-analysis
MCI, mild cognitive impairment; SCD, subjective cognitive decline; HC, healthy controls; MMSE, Mini-Mental State Examination; MNI, Montreal Neurological Institute; SD, standard deviation; FWHM, full-width at half maximum; F, female; M, male. ∗mean±SD.
Regions with GM changes between MCI and HCs
GM structural changes were detected in comparison to the MCI group and HCs. In total, 46 comparison groups from 43 MRI experiments (three experiments included two comparison groups) were encompassed in this meta-analysis. We observed GM loss of the four largest clusters in comparison of MCI and HCs (Table 2, Fig. 2a). The largest cluster was completely identified in the left cerebrum including the amygdala, PHG, and the hippocampus. The second one was focused on the right cerebrum, which was comprised of the hippocampus, amygdala, PHG, lentiform nucleus, and insula. The third one was located in the left hippocampus, and the fourth one was focused on the left medial temporal gyrus. Overall, our meta-analysis results indicate that GM loss was asymmetrical in the bilateral hemisphere and more severe in left cerebrum compared to the right. In addition, no studies in the MCI group have found larger GM volume compared to subjects in the HCs group.
Regions with GM changes between MCI and HCs
BA, Brodmann area; PHG, parahippocampal gyrus; L(R), left(right) hemisphere; MCI, mild cognitive impairment; HCs, healthy controls; GM, gray matter.
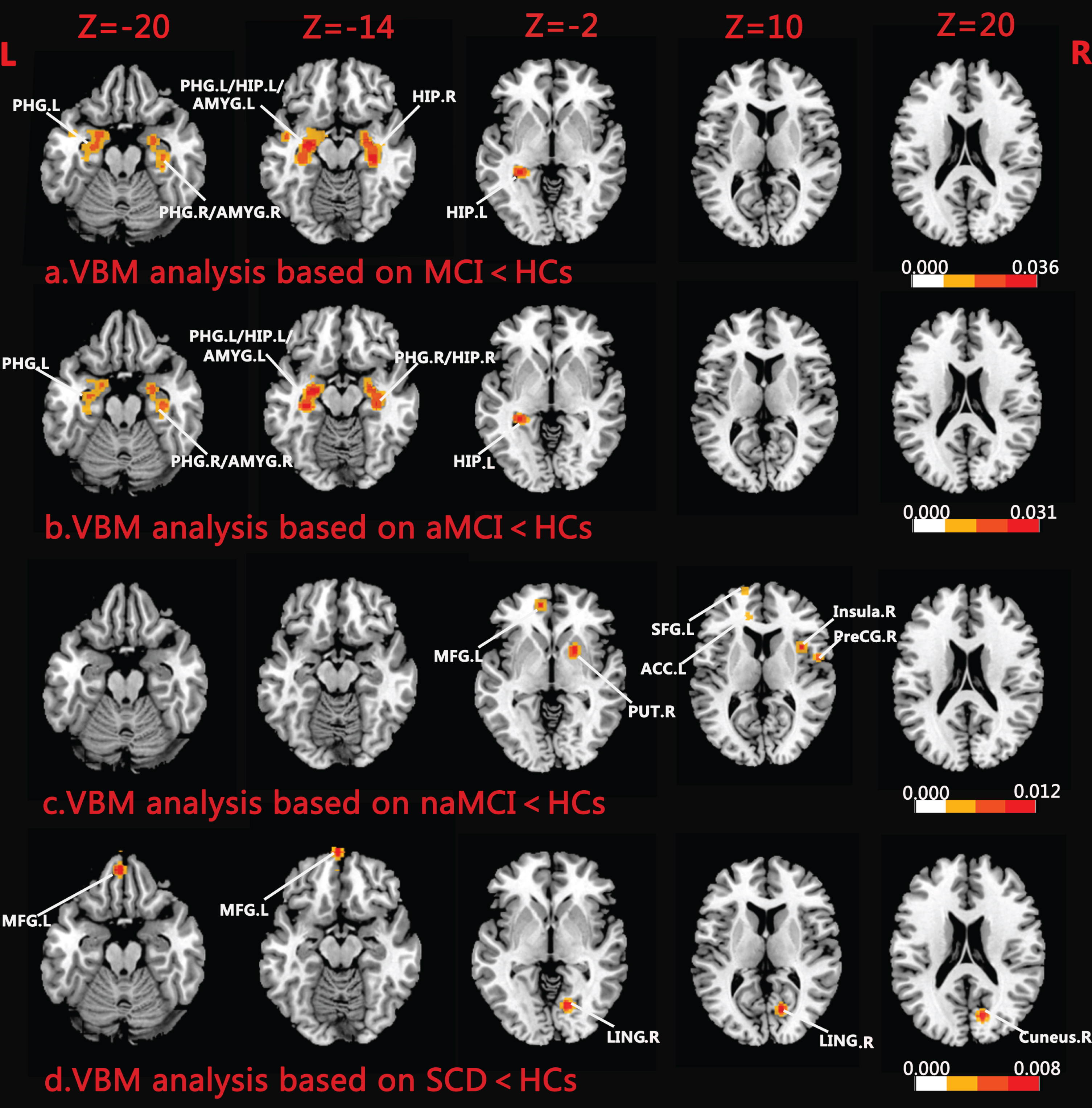
Regions of GM loss in MCI, aMCI, naMCI and SCD patients compared to HCs. a) VBM analysis based on MCI < HCs show GM atrophy in bilateral MTL including amygdala, PHG, hippocampus, and then spread to right lateral globus pallidus, right insula and left middle temporal gurus (FWE corrected p < 0.001). b) Regions of GM loss in aMCI < HCs present in bilateral MTL, including amygdala, PHG and hippocampus (FWE corrected p < 0.001) c) Pattern of gray matter reduction are located in right putamen, right precentral gyrus, right insula, left medial/superior frontal gyrus and left anterior cingulate in naMCI < HCs (FWE corrected p < 0.05). d) Gray matter reduction in SCD < HCs was mainly in right lingual gyrus, right cuneus, and left medial frontal gyrus (FWE corrected p < 0.05). VBM, voxel-based morphology; GM, gray matter; PHG, parahippocampal gyrus; MTL, medial temporal lobe; HIP, hippocampus; AMYG, amygdala; MFG, medial frontal gyrus; SFG, superior frontal gyrus; PUT, putamen; ACC, anterior cingulate cortex; PreCG, precentral gyrus; LING, lingual gyrus; MCI, mild cognitive impairment; aMCI, amnestic mild cognitive impairment; naMCI, non-amnestic mild cognitive impairment; SCD, subjective cognitive decline; HCs, healthy controls; L, left hemisphere; R, right hemisphere.
Regions with GM changes between aMCI/naMCI and HCs
In total, 37 studies met the inclusion criteria in the aMCI-HCs group. The sub-analysis results of aMCI-HCs indicated GM reduction mainly located in the bilateral MTL, including amygdala, PHG, and hippocampus (Table 3, Fig. 2b). Additionally, these regions were also observed in the MCI-HCs results, as described above. Similar to the MCI-HCs results, atrophy was found to be asymmetric and more obvious in the left MTL.
Regions with GM changes between aMCI/naMCI and HCs
BA, Brodmann area; PHG, parahippocampal gyrus; L(R), left(right) hemisphere; aMCI, amnestic mild cognitive impairment; naMCI, non-amnestic mild cognitive impairment; HCs, healthy controls; GM, gray matter.
Furthermore, five naMCI studies in accordance with our inclusion criteria were included in the analysis. The GM atrophy areas of the naMCI-HCs were more scattered than the concentrated atrophic regions of the aMCI-HCs (Table 3, Fig. 2c). GM loss in naMCI-HCs was observed in the right precentral gyrus (BA 6), left superior/medial frontal gyrus, right insula (BA 13), left anterior cingulate (BA 32), and right putamen.
Regions with GM changes between SCD and HCs
After systematic searches, four SCD studies were included in the study, encompassing 134 subjects and 156 HCs. We found a pattern of GM loss in subjects with SCD, including volume loss within the occipital lobe, comprised of right lingual gyrus and right cuneus, as well as the frontal lobe, which was comprised of the left medial frontal gyrus (BA10) (Table 4, Fig. 2d).
Regions with GM changes between SCD and HCs
BA, Brodmann area; L(R), left(right) hemisphere; SCD, subjective cognitive decline; HCs, healthy controls; GM, gray matter.
DISCUSSION
Our voxel-based quantitative meta-analysis is the first quantification of GM changes that examines both SCD and MCI. Additionally, when compared to previous MCI meta-analyses, which have only included 5, 22, and 26 eligible MCI-HCs studies respectively [29 –31], our results are likely more credible due to the large number of eligible MCI papers (n = 43) included in this study. Overall, our results demonstrate unique GM change patterns in the MCI group, SCD group, as well as the MCI subgroups (including aMCI group and naMCI group). The GM atrophy patterns observed in the MCI and SCD groups provide in-depth insights into the neuroanatomical mechanisms at different stages of the preclinical AD spectrum.
Patterns of regional GM atrophy in MCI-HCs
The atrophic regions identified in the MCI-HCs analysis have been mainly located in bilateral MTL, including the hippocampus, PHG, and amygdala. It also spread to regions outside the bilateral MTL, including the left middle temporal gyrus, right insula, and subcortical region (right lateral globus pallidus). The structural changes of brain GM are consistent with results from previous meta-analyses [29 –31].
The hippocampus, PHG, and amygdala, which belong to the MTL, are important parts of the memory system. The hippocampus, anatomically, is buried deep inside the temporal lobe and resembles an elongated structure. It is engaged in the formation of new episodic memories and long-term storage of memory [37, 38]. Additionally, evidence indicates that the anterior hippocampus contributes to high-level cognitive functions of perception and imagination beyond memory [39]. The amygdala is located at the anterior border of the hippocampus structure and the anterior part of the lateral ventricle’s inferior horn. The amygdala is responsible for processing information between the prefrontal-temporal cortex and the hypothalamus. Thus, it plays a key role in regulating emotions, behaviors, and memory formation. The amygdala also participates in consolidating and restoring emotional memories by connecting to the hippocampus [40, 41], and exerts a modulatory influence on both the hippocampal and caudate-putamen memory systems [42].
The PHG, the prime cortical input of the hippocampus, plays a crucial role in emotion and cognition [43]. The PHG, along with hippocampus, papillary body, anterior nucleus of thalamus, and cingulate gyrus, forms an important hippocampal loop which participates in cognitive functions such as emotion, learning, and memory. In particular, this loop plays a role in encoding, consolidation, and retrieval of memory. Hence, damage to the PHG leads to abnormal emotional and cognitive behaviors [44]. The hippocampus, PHG, and amygdala, the main structures of the MTL memory systems, collaboratively engage in the encoding and retrieval of episodic and spatial memory by relying on their extensive cortex connections with memory storage sites within the neocortex [45 –48]. In postmortem autopsy studies, one or more neuropathological features, including argyrophilic grain disease, hippocampal sclerosis, vascular lesions, cortical neuritic plaques, diffuse plaques, synaptic loss, and neurofibrillary tangles, have been found in the hippocampus, PHG, and amygdala in MCI patients [49 –51]. Results indicating the loss of GM in the hippocampus, PHG, and amygdala are in line with previous quantitative MRI research based on ROI, synaptic loss, and hypometabolism in studies that utilized positron emission tomography in MCI patients [52 –54]. Resting-state abnormalities and task-stated hypoactivation of the bilateral hippocampus, PHG, and amygdala in MCI obtained in previous meta-analyses support our results [55, 56]. Besides, GM atrophy in the bilateral hippocampus, PHG, and amygdala are consistent with previous MCI-HCs meta-analyses [29 –31]. Loss of GM in the hippocampus, PHG, and amygdala lead to impairment of memory function, which is consistent with the prominent clinical manifestations associated with memory loss in MCI patients. From the perspective of quantitative meta-analysis, our results support the critical role of MTL structure in memory.
In our meta-analysis results, there have been brain structural changes of the left middle temporal gyrus, right insula, and right lateral globus pallidus. The left middle temporal gyrus, which participates in the formation of auditory cortex and visual cortex, engages in high-level cognitive functions such as auditory, vision, and language reception. The structural alternations of the middle temporal gyrus are consistent with those found in previous meta-analysis [29] and have also been proven repeatedly in multiple quantitative MRI studies based on ROI and default mode network in MCI patients [51, 57]. The insula has widespread interconnections with MTL structures, which allow access to somatosensory, auditory, olfactory, gustatory, and visceral sensation by connecting to the amygdala [58]. In addition, the insula has a high degree of functional diversity as it also plays a role in sensory, high-level perception, attention, and control, which indicates that it plays a critical role in integration of various types of information that are required for cognitive functions [59]. Amyloid deposition within the insula cortex of MCI patients are consistent with our findings [60]. A series of whole brain/ROI-based structural imaging and functional imaging studies have supported our results [61 –63]. The lateral globus pallidus, which obtains projections from the relevant striatal territories, participates in control of body movement and attentional processing [64, 65]. Damage to the globus pallidus induced dysfunction of motor and defective performance on tasks of learning and memory [66]. A recent volumetric analysis of subcortical GM in MCI patients has revealed changes associated with globus pallidus, instead of hippocampus account, for deficits in short-term memory binding, and has proposed the hypothesis that the globus pallidus may be part of a network that is located outside of the hippocampus and supports binding [67]. However, this hypothesis needs to be further studied to be verified.
Our meta-analysis of the neuroanatomical GM changes between MCI patients and HCs has demonstrated that MCI patients not only suffer from dysfunction of the entire neural network of episodic memory, but also affect other cognitive functions, such as language, attention, and visuospatial and motor impairments. Additionally, our results confirm the reliability of whole-brain based VBM method as a biomarker for identifying MCI from HCs.
Patterns of regional GM atrophy in aMCI/naMCI-HCs
According to impaired cognitive domains, MCI can be divided into two categories, including the aMCI subtype and naMCI subtype. The clinical progression of these two are different, as aMCI always progresses to AD dementia, while the latter tends to progress to non-AD dementia, such as DLB [8]. In order to explore the difference in neuroanatomy between aMCI and naMCI, we conducted meta-analyses of these subgroups group respectively.
Compared with HCs, the aMCI group exhibited concentrated atrophy in the bilateral hippocampus, PHG, and amygdala. GM atrophy in those regions plays an important role in the core neuroimaging findings in aMCI and is considered to become more severe during the progression from aMCI to AD dementia [68, 69]. These atrophic regions are also typical patterns of AD and nicely confirm the previous view that patients with aMCI were at high risk of progressing to AD [70, 71]. In addition, our results are consistent with the clinical features of episodic memory deficits in aMCI patients, and support the key neuroanatomical role of the hippocampus, PHG and amygdala in the formation of neural memory networks.
Our results found that naMCI group demonstrated increased GM loss compared to HCs in the right putamen, right insula, right precentral gyrus, left superior/medial frontal gyrus, and left anterior cingulate (Fig. 2c). These regions were distinguished from the more concentrated atrophy pattern in the bilateral MTL of aMCI patients. In contrast to GM atrophy in aMCI patients, naMCI patients demonstrated a milder and scattered pattern without a specific focus, in keeping with the clinical features of naMCI patients that present with impairment of various cognitive functions but relative memory preservation [3]. The putamen, located in the striatum/dorsal part of the basal ganglia, functions in coordination with the cortex through complex cortical-basal ganglia networks to perform learning and motor control, which includes language functions, reward, cognitive function, and addiction [72]. The bilateral putamen especially engages in several aspects of written and spoken semantic, orthographic, and phonological processing [73]. The precentral gyrus that contains the primary motor cortex is located within the frontal lobe, and it known for its control of voluntary motor movement. Studies have also indicated that the precentral gyrus is involved in false retrieval of memory and topographic memory [74 –76]. However, it is still unclear whether it is indirectly affected by the dysfunction of other brain regions, or is potentially correlated with cognitive function. Further studies are needed to verify this hypothesis. GM atrophy in these areas leads to dyskinesia and cognitive impairment, and may be the early manifestations of some neurodegenerative diseases that are characterized by cognitive impairment and motor dysfunction, such as DLB, FTD, and PD. A number of studies, which demonstrate structural and functional changes in the putamen and precentral gyrus in patients with DLB, FTD, and PD [77 –79], also support our results.
The GM atrophy in the right insula in naMCI group is consistent with results from meta-analysis of MCI group. Anterior cingulate cortex and prefrontal cortex (PFC) are not only anatomically interconnected with one another but are also closely linked in functional connectivity levels [80]. Anterior mid-cingulate cortex, prefrontal cortex, and parietal cortex make up the main components of the cingulo-frontal-parietal (CFP) cognitive-attention network and has been identified as nodes of attentive and cognitive parallel networks along with the striatum, premotor areas, thalamus, and cerebellum [81, 82]. Additionally, PFC has been proven to be associated with extensive cognitive functions including perception, response selection, episodic memory and problem solving, and considered to be a special frontal-lobe network that recruits through diverse cognitive processes [83, 84]. Our neuroimaging findings in naMCI patients are consistent with the prominent clinical manifestation of naMCI patients, including dysfunction of executive function, language function and attention. Our results have confirmed the notion that some naMCI patients represent a distinct subgroup of MCI patients who may progress to non-AD dementia, such as PD, FTD, and DLB [85].
In conclusion, based on our study of quantitative meta-analysis, aMCI and naMCI have selective specificity in regions of GM loss, which provides a theoretical basis for targeted interventions in the early stages of different neurodegenerative disease states.
Patterns of regional GM atrophy in SCD-HCs
We found significant macrostructural atrophy in people with SCD compared with HCs, which confirms that SCD subjects are neuroanatomically distinct from healthy people. Our findings present two significant clusters of GM loss in SCD subjects, including the occipital lobe, comprised of right lingual gyrus and right cuneus, and medial prefrontal cortex (mPFC), which includes the left medial frontal gyrus. The lingual gyrus and the cuneus, located in the occipital lobe, are at the center of the visual cortex. The lingual gyrus and the cuneus not only participate in visuospatial processing, but also play a role in distance and depth perception, color determination, object and face recognition, and memory formation [86]. Thus, damage of these structures lead to abnormal visual function, memory deficits, and perception disturbances. Conformably, visual dysfunction, subtle cognitive impairment, and perception disturbances have been observed in patients with SCD [87 –89]. A series of structural and functional imaging studies have shown abnormalities of the lingual gyrus and the cuneus in SCD patients, which supports our results [90 –93]. Our findings of GM loss within the lingual gyrus and the cuneus in SCD has led to verification of the previous neuroanatomical hypothesis that damage of brain regions that are responsible for visual cognition and perception are related to early signs of cognitive impairment [87 , 95]. The mPFC is related to different cognitive function, including memory processing, decisive making, and emotion processing [96, 97]. Studies indicated that the communication between the hippocampus and mPFC is very important in the construction of episodic memory [98 –100]. For example, a study pointed out that the communication between the hippocampus and mPFC is related to the integration of new memories into the existing abstract framework [98]. Alterations of mPFC regions in SCD subjects have not only been reported on the structural level but also on the functional level [3, 101]. GM loss in mPFC, which involves cognitive function, is consistent with the idea that SCD subjects have subtle cognitive deficits [88].
In conclusion, our findings indicate that the regions showing SCD-related GM changes are associated with visual function, perception, and cognition. Therefore, we speculate that SCD, as a very early stage of the preclinical AD spectrum, may first present as a series of subtle impairments affecting vision, perception and cognition. Then, as the disease progresses to MCI, destruction of important structures of the memory system, such as the hippocampus, gradually appear, and is followed by manifestation of various cognitive impairments, such as memory deficits. Furthermore, in our meta-analysis, SCD patients do not present with GM atrophy in structures such as the hippocampus. Because this region shows abnormal connectivity in many functional studies, our results also indirectly support a previous hypothesis that structural changes may occur after functional anomalies in SCD subjects [3 , 101].
Clinical implications
Our quantitative neuroimaging meta-analysis, which is based on comprehensive and systematic literature searches, has been essential in summarizing existing studies and conducting an in-depth exploration of the pathological mechanisms associated with the preclinical AD spectrum. Our meta-analysis results indicate that GM changes of the brain in different stages of preclinical AD spectrum show different atrophy patterns. In accordance with previous meta-analysis, the MTL structure, including the hippocampus, PHG, and amygdala, is still the hallmark neuroimaging marker of MCI. Significant clusters of GM loss in the lingual gyrus, the cuneus and the mPFC in SCD group indicate that these neuroimaging changes may become potential future biomarkers of SCD. Those important neuroanatomical regions can be further used as an objective foundation for further targeted interventions at the different stages of the preclinical AD spectrum. The current results also strengthen the imaging characteristics of specific GM changes in MCI and SCD, and pave the way for further in-depth study of the pathogenesis of AD.
Limitations
Limitations of our meta-analysis are well acknowledged. First, ALE meta-analysis cannot evaluate the extent of heterogeneity between studies. However, we tried to minimize heterogeneity through strict inclusion and exclusion criteria. Although the quantitative meta-analysis method has the advantage of integrating multi-coordinates of neuroimaging data, ALE is still limited by literature reviews [34]. Finally, studies that were unpublished, with insufficient data or not published in English were excluded from our meta-analysis, and the findings of these papers are not reflected in our results.
Conclusion
We conducted four ALE meta-analyses which included the SCD group, MCI group, and its sub-groups (aMCI and naMCI), with the goal of identifying brain structural changes at different stages of the preclinical AD spectrum. We report that the meta-analysis results of brain GM changes, which have indicated that the MCI group and SCD group have shown different patterns of atrophy respectively, and can effectively distinguish MCI, SCD, and normal subjects from the level of neuroimaging. The convergent pattern of regionally selective brain atrophy can be utilized as a framework of quantitative analysis for future image processing in MCI and SCD. These unique imaging results provides an objective foundation for future targeted interventions at the different stages of the preclinical AD spectrum in order to delay the progression of AD. However, it is essential to include more SCD studies and comparative studies between the MCI and SCD groups to validate our findings and further explore the potential role of imaging as a biomarker for the preclinical AD spectrum.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (No. 81701675); the Key Project supported by Medical Science and technology development Foundation, Nanjing Department of Health (No. JQX18005); the Cooperative Research Project of Southeast University-Nanjing Medical University (No. 2018DN0031); the Key Research and Development Plan (Social Development) Project of Jiangsu Province (No. BE2018608); and Innovation and Entrepreneurship Training Program for College Students in Jiangsu Province (No.201810312061X; 201910312035Z). Key scientific research projects of colleges and universities in Henan province (No:18A190003).