
Abstract
Background:
Growing evidence suggests hearing loss is a risk factor for mild cognitive impairment and dementia, but few studies have examined its relationship to sub-clinical cognitive outcomes.
Objective:
To investigate the effect of self-reported hearing loss on longitudinal cognitive function in a risk-enriched cohort of clinically-unimpaired, late middle-aged adults.
Methods:
579 participants from the Wisconsin Registry for Alzheimer’s Prevention (WRAP) were included. Hearing status was determined via self-reported history of diagnosed hearing loss. Each participant with self-reported hearing loss was age- and sex-matched to two participants who never reported hearing loss using nearest-neighbor matching. Linear mixed-effects models were used to examine associations between self-reported hearing loss and age-related cognitive trajectories with covariates of sex, literacy, and ethnicity, person-level random intercepts and age-related slopes. Cognitive outcomes encompassed measures of speed and flexibility, visuospatial memory, and verbal fluency.
Results:
Participants with self-reported hearing loss exhibited significantly poorer performance on a speed and flexibility factor score and single test of psychomotor speed and executive function, relative to participants who never reported hearing loss. There was no association between self-reported hearing loss and visuospatial memory or verbal fluency. Longitudinally, self-reported hearing loss was associated with less rapid decline in speed and flexibility and no difference in rate of decline for any other cognitive measure.
Conclusion:
Self-reported hearing loss was associated with poorer speed and flexibility but not with accelerated decline in any domain studied, contrary to previous findings. Further studies involving behavioral auditory measures in this cohort would clarify the robustness of these findings.
Keywords
INTRODUCTION
Hearing loss and dementia both represent significant and growing public health concerns. Hearing loss is one of the most common chronic conditions among older adults, and has been associated with depression, social isolation, and decreased self-sufficiency [1–5]. Dementia is a primary independent contributor to disability, placing a heavy burden on patients, their families, and healthcare and long-term care systems [6, 7]. The prevalence of both conditions increases with age, and older adults, aged 65-year-olds and older, are the most rapidly growing segment of the U.S. population [8]. Thus, these conditions are expected to affect an increasing percentage of Americans and identifying ways to predict, treat, and prevent them is critical.
While a growing number of studies support associations between hearing loss and incident mild cognitive impairment (MCI) and dementia [9–14], the relationship between hearing loss and sub-clinical cognitive decline is less clear. Understanding earlier stages of cognitive decline is important as interventions are likely to be most effective prior to the development of significant cognitive impairments. In addition, most previous studies have focused on adults aged 70 years and older, and prospective, longitudinal data from middle-aged adults are lacking. Therefore, the aim of this study was to examine associations between hearing loss and longitudinal cognition in a risk-enriched cohort of cognitively unimpaired, late-middle-aged adults. We hypothesized that hearing loss would be associated with poorer baseline cognition and steeper cognitive decline.
MATERIALS AND METHODS
Sample
This study analyzed existing data from the Wisconsin Registry for Alzheimer’s Prevention (WRAP), a longitudinal observational cohort enriched for Alzheimer’s disease risk with multiple waves of cognitive assessment. Details about WRAP have been described previously [15, 16]. Briefly, 72% of WRAP participants have a parental history of Alzheimer’s disease dementia, either confirmed by autopsy or deemed probable by clinical criteria. Participants are 40–65 years old and cognitively healthy at study entry. Data are collected at Wave 1, approximately four years later at Wave 2, and then serially every two years thereafter. Because Wave 2 is the earliest visit for which hearing history data are available, Wave 2 was treated as the baseline visit for this report. Data from up to five visits were available for participants in the current sample with a median of three visits.
Preliminary descriptive analyses revealed that participants with hearing loss were older and disproportionately male, relative to participants who never reported hearing loss, in line with previous epidemiological studies [17, 18]. To ensure results would not merely reflect effects of sex and aging, propensity score matching was used to match two participants who never reported hearing loss to each participant who had reported hearing loss on sex and baseline age (Fig. 1). A matching ratio of 2:1 was chosen to minimize bias and mean squared error while maintaining a relatively large sample size [19]. Participants with clinical impairment at enrollment or at Visit 2 were excluded prior to matching, resulting in a sample size of 579. The University of Wisconsin Institutional Review Board approved all WRAP study procedures and each participant provided signed informed consent before participation.
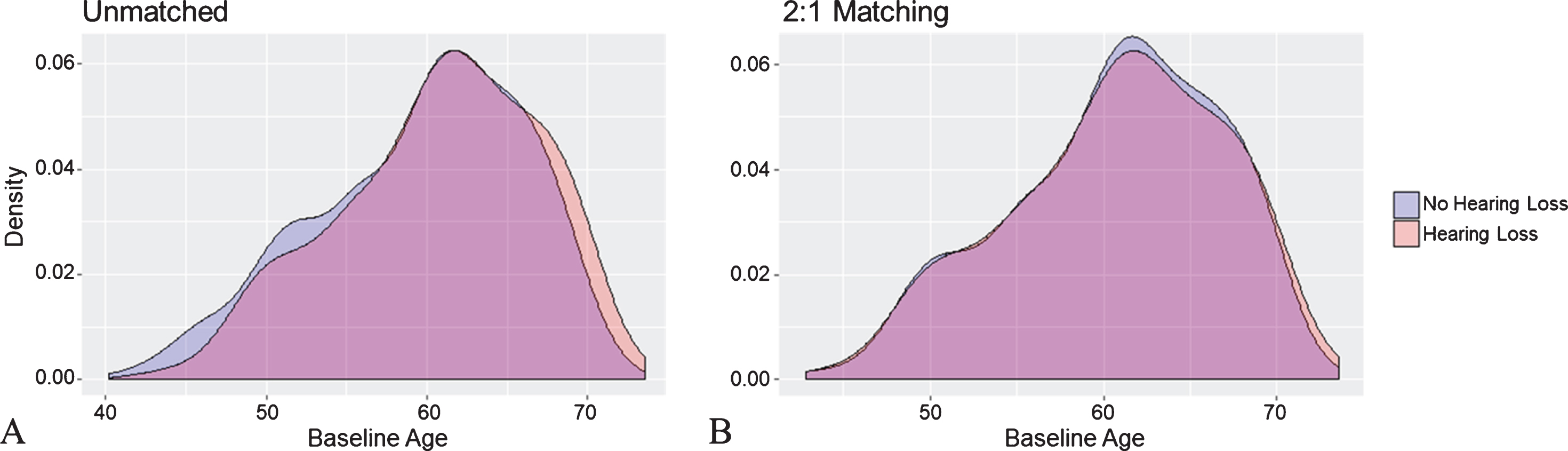
Proportion density plots of baseline age for participants who never reported hearing loss and those who reported hearing loss at any visit, before (A) and after (B) matching.
Hearing status and covariates
At each visit, participants complete questionnaires assessing various demographic, clinical, and lifestyle factors. Ethnicity, smoking status, stroke history, and self-report of hypertension or diabetes were obtained from these questionnaires. Presence of diabetes was based on a fasting glucose >125 mg/dL or self-reported history of diabetes. Presence of hypertension was based on systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or self-reported history of hypertension. Beginning in Wave 2 and onward, participants were asked a single question about the presence of hearing loss as part of a larger medical history questionnaire. In order to accommodate the fact that some participants developed hearing loss after Wave 2, hearing status was expressed as the proportion of visits with hearing loss. That is, a participant who reported hearing loss at Wave 2 would have a proportion of 1, a participant who reported no hearing loss their first two visits but reported hearing loss their subsequent two visits would have a proportion of 0.5, etc. Standardized baseline Wide Range Achievement Test-III (WRAT-III) [20] Reading scores were used as a measure of premorbid intellect [21] rather than years of education which has been found to be an inadequate measure of educational experience [22]. Genotyping for the two APOE single nucleotide polymorphisms that determine the ɛ2, ɛ3, and ɛ4 alleles was done by WRAP previously and has been described in detail elsewhere [23]. APOE ɛ4 carriers were participants who had at least one APOE ɛ4 allele.
Cognitive measures
At each visit, WRAP participants complete a com-prehensive neuropsychological test battery [15] comprising measures that assess the cognitive domains of memory, attention, psychomotor speed and executive function, language, and visuospatial ability. Psychomotor speed and executive function have previously been shown to decline more rapidly in individuals with hearing loss [30, 34]. Therefore, we investigated two outcomes related to psychomotor speed and executive function: the Digit Symbol Substitution Test (DSST) [27], a single measure which has been used in previous studies of hearing loss and cognitive decline, and a Speed and Flexibility Factor Score, a z-score derived from a weighted composite of the Stroop Color-Word Test Interference Trial [25] and Trail-Making Test Parts A & B [26] identified from previous analyses [24]. The Speed and Flexibility Factor Score was chosen as the primary outcome because it encompasses multiple tests. Previous studies have also found associations between hearing loss and global cognitive decline [30, 31]. Thus to probe cognitive domains beyond psychomotor speed and executive function, we also investigated single tests of visuospatial memory (Brief Visuospatial Memory Test –Delayed Recall [BVMT-D]) [28] and verbal fluency (Multilingual Aphasia Examination (C, F, L) [CFL]) [29]. DSST, BVMT-D, and CFL scores were standardized [ N (0,1)] into z-scores. All measures examined rely on non-auditory performance to avoid confounding by reduced audibility.
Statistical analyses
Differences in participant characteristics were examined by hearing status (no hearing loss versus prevalent or incident hearing loss). Because baseline age, WRAT-III standardized Reading score, and years of follow-up were not normally distributed, non-parametric (Mann-Whitney) tests were utilized for group comparisons. Pearson chi-square tests or Fisher’s exact tests, where appropriate, were used to compare categorical variables.
Linear mixed-effects models were used to test whether hearing status was associated with longitudinal cognitive performance. In the primary analyses, the base model included fixed effects of age at each visit (centered on the sample mean of 63.6 years), sex, literacy (centered on the sample mean of 107.3), ethnicity, hearing status (proportion of visits with hearing loss) and the interaction of age×hearing status. All models included random effects of intercept and slope nested within subject. The overall significance of the hearing status and age×hearing status interaction were assessed by likelihood ratio tests comparing the primary model and a model that did not include these terms. Additional models investigated the effect of adding blocks of cardiovascular or genetic risk factors as covariates. Data analysis was performed using the lme4 package [30] in R [31] with tests of significance set at p < 0.05.
RESULTS
Participant characteristics
Table 1 details participant characteristics overall and by hearing status. The mean age at baseline for the total study sample was 60.6±6.1 years. Participants were majority female (57.0%), primarily non-Hispanic white (93.6%), and had a high prevalence of parental history of dementia (70.1%) and APOE ɛ4 allele carriers (37.7%). Participants who reported hearing loss at baseline or follow-up were more likely to be non-Hispanic white (p = 0.002) and had more years of follow-up (p < 0.001) and more follow-up visits (p = 0.002) than those who never reported hearing loss. There were no other differences between those with and without self-reported hearing loss. Of the 193 participants who reported hearing loss, 106 (54.9%) had prevalent hearing loss at Visit 2 while 87 (45.1%) had incident hearing loss at a later visit. The mean proportion of visits with hearing loss was 0.76.
Table 1
a“No hearing loss” refers to participants who never reported hearing loss at any visit. b“Hearing loss” refers to participants who reported hearing loss at baseline or a follow-up visit. This encompasses 106 prevalent and 87 incident cases of self-reported hearing loss. cLiteracy as measured by the Wide Range Achievement Test-III (WRAT III) standardized Reading score. dNumber of visits, beginning with Visit 2 (baseline). ePresence of hypertension, diabetes, or stroke and smoking status at baseline.
Cognitive trajectories across hearing groups
Longitudinal cognitive performance as a function of proportion of visits with hearing loss is displayed in Fig. 2. Results from likelihood ratio tests (χ23) indicated that hearing status and hearing status×age accounted for a significant amount of variation in the Speed and Flexibility Factor Score (χ2 = 13.80, p = 0.001) and DSST (χ2 = 8.78, p = 0.012), but not the BVMT-D (χ2 = 1.72, p = 0.424) or CFL (χ2 = 0.78, p = 0.677). Model parameters are displayed in Table 2. Relative to those with normal hearing, individuals with hearing loss had poorer scores on the Speed and Flexibility Factor Score (β[SE] =−0.284 [0.093], p = 0.002) and DSST (β[SE] =−0.195 [0.045], p = 0.028), but not the BVMT-D (β[SE] =−0.009 [0.009], p = 0.272) or CFL (β[SE] = 0.075 [0.093], p = 0.415). Considering the hearing loss×age interaction, hearing loss was associated with a less rapid decline with age on the Speed and Flexibility Factor Score (β[SE] = 0.021 [0.010], p = 0.044), but no difference in rate of decline for any other cognitive measure.
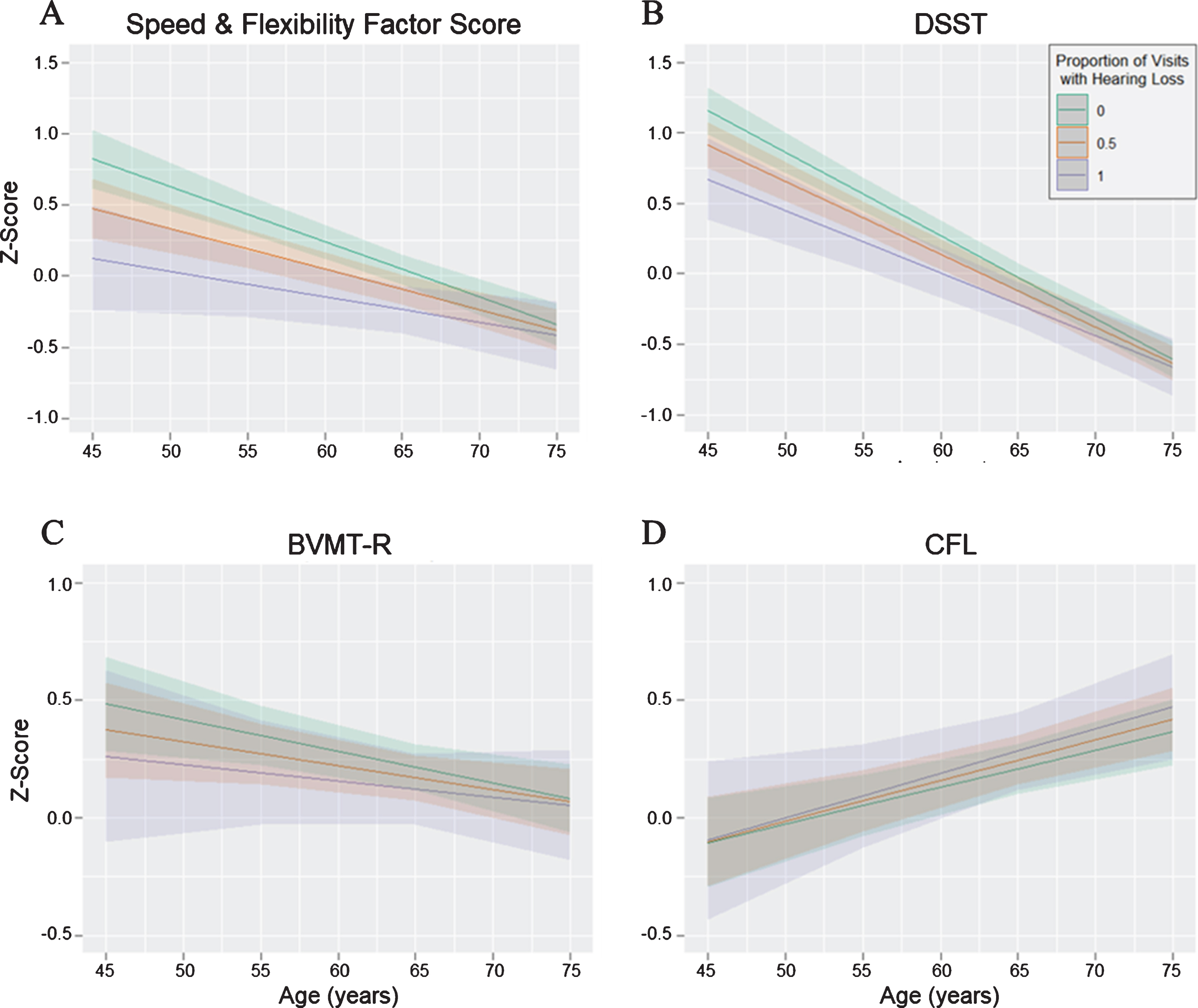
Longitudinal cognitive performance by proportion of visits with self-reported hearing loss. Graphs depict age on the x-axis and cognitive performance on the y-axis for the four measures (A–D). Higher scores indicate better performance on all measures. Proportion of visits with hearing loss was modeled as a continuous variable, but estimated slopes for three hearing groups (hearing loss at no visits, half of visits, or all visits) are depicted for simplicity.
Parameter estimates from the base linear mixed-effects modelsa
aModels were adjusted for age, sex, literacy, and ethnicity. bHearing loss denotes the estimated mean difference in cognition between participants who never reported hearing loss and those with an increasing proportion of visits with hearing loss. cHearing loss×age denotes the estimated difference in annual rate of change in cognition between participants who never reported hearing loss and those with an increasing proportion of visits with hearing loss.
Adjustment for cardiovascular and genetic risk factors
Adding a block of cardiovascular risk factors (hypertension, diabetes, history of stroke, and smoking status) or genetic risk factors (APOE ɛ4 status and parental history of AD) to the base model did not substantively affect most results (Table 3). After adjusting for cardiovascular risk factors, individuals with hearing loss still performed more poorly on the Speed and Flexibility Factor Score (β[SE] =−0.271 [0.093], p = 0.004) and DSST (β[SE] =−0.198 [0.089], p = 0.037). However, the hearing loss×age interaction, which had been marginally significant in the base model for the Speed and Flexibility Factor Score, was no longer significant (β[SE] = 0.020 [0.010], p = 0.054). After adjusting for genetic risk factors, individuals with hearing loss still exhibited poorer scores on the Speed and Flexibility Factor Score (β[SE] =−0.282 [0.093], p = 0.003) and DSST (β[SE] =−0.196 [0.088], p = 0.027), and the hearing loss×age interaction remained significant for the Speed and Flexibility Factor Score (β[SE] = 0.021 [0.010], p = 0.041).
Parameter estimates from the linear mixed-effects models adjusted for cardiovascular and genetic risk factors
acardiovascular risk factors were hypertension, diabetes, history of stroke, and smoking status at baseline. bgenetic risk factors were APOE ɛ4 status and parental history of AD.
DISCUSSION
This study found self-reported hearing loss was associated with poorer performance in two of four cognitive domains examined, but not steeper cognitive decline in a cohort of risk-enriched, late-middle-aged adults. Specifically, individuals who reported hearing loss at a greater number of visits exhibited poorer performance on measures of psychomotor speed and executive function, the Speed and Flexibility Factor Score and DSST, than those who never reported hearing loss. There were no differences in average performance or decline in visuospatial memory or verbal fluency, but hearing loss was associated with less rapid decline in the Speed and Flexibility Factor Score.
These results qualify findings from previous studies investigating associations between hearing loss and longitudinal cognition. For example, Lin and colleagues (2013) [32] observed that older adults with baseline hearing loss exhibited accelerated cognitive decline relative to those with normal hearing. Yet the current study did not find associations with accelerated decline despite considering one of the same outcome measures, the DSST. This discrepancy may be due to differences in participant characteristics and methods for evaluating the presence of hearing loss. Participants in the Lin et al. study were more than 15 years older at baseline than those in the present study; were from a population-based, rather than risk-enriched, cohort; and they exhibited significant group differences in baseline age and gender which were controlled for here through propensity score matching. In addition, hearing loss was measured using pure tone audiometry rather than via self-report, as was done in this study. Amieva and colleagues (2015) [33] used a self-reported hearing loss measure and found that hearing loss was associated with 25-year decline in global cognition. However, the measure of global cognition used, the Mini-Mental State Examination (MMSE) [34], has been shown to be affected by reduced audibility [35]. As in the Lin et al. study, participants in the Amieva et al. study were more than 10 years older at baseline than the present study sample and from a population-based cohort. In addition, the Amieva et al. study used a self-report measure that assessed severity of hearing loss, which is more fine-grained than the measure used in the present study, where presence or absence of hearing loss was reported. Another study by Valentijn and colleagues (2005) [36], which used pure-tone auditory measures, found that hearing loss was associated with greater cognitive decline but not poorer baseline cognition in a population-based cohort approximately five years older than the present study participants. It is possible that differences in the rate of cognitive decline between adults with and without hearing loss become more apparent in advanced age or that such differences are overshadowed in a cohort at greater risk of decline than the general population. For example, APOE ɛ4 allele carriers have been shown to decline more rapidly on the DSST than non-carriers [37] and the prevalence of APOE ɛ4 carriers in the present study sample was more than twice that of the general population [38]. Continued follow up of this cohort over a longer time period will elucidate whether long-term cognitive trajectories differ between groups. An additional possibility is that if individuals with hearing loss performed considerably lower than those without hearing loss at baseline, regression to the mean contracted their rate of decline.
Although we did not find greater rates of cognitive decline in individuals with hearing loss, we did nevertheless find differences in cognitive performance. Individuals with lower cognitive performance would, in principle, require less decline to cross the threshold of what constitutes clinical impairment than those with higher cognitive performance, even if the two individuals had identical rates of decline. Thus, differences in MCI and dementia incidence between those with and without hearing loss may, in part, be due to differences in peak cognitive performance earlier in life. This study analyzed cognitive data collected beginning in middle age, so future studies of younger cohorts will be necessary to understand how early these differences in average performance arise.
A major strength of this study is the inclusion of hearing loss data beyond baseline. Considering a participant’s proportion of visits with hearing loss avoids collapsing individuals who reported hearing loss at later visits into the same category as those who never reported hearing loss at all or those who reported hearing loss from their baseline visit. Other strengths of this study were the use of demographically-matched participants and the use of a cognitive composite (the Speed and Flexibility Factor Score) which improves reliability and decreases measurement error [39]. A key limitation of this study was the reliance on a self-reported hearing measure as no behavioral hearing measures are available in this cohort. Hearing loss is known to be highly underdiagnosed [40] and therefore our results may have been affected by unreported hearing loss among participants categorized as having no hearing loss. In addition, demographic factors, education level, degree of hearing loss, and personality traits can influence an individual’s self-impression of their hearing ability [41–43]. Furthermore, although a single, global question has been found to be an adequate indicator of hearing loss [43, 44], it precludes analyzing the effects of hearing loss severity. In addition, our sample is enriched for Alzheimer’s disease risk and participants are predominantly highly educated and white, limiting the generalizability of our results to population-based samples of normally aging adults.
Despite these limitations, our findings suggest that hearing loss in late-middle-age is associated with poorer psychomotor speed and executive function but no greater rate of cognitive decline. Assessing auditory function using more objective approaches would help further clarify the link between hearing loss and cognitive trajectories.
Footnotes
ACKNOWLEDGMENTS
This work was supported by a National Institute on Aging grant R01 AG027161 (S.C.J.); by a National Institute on Deafness and Other Communication Disorders grant R01 DC003083 (R.Y.L); and a Clinical and Translational Science Award (UL1RR025011) to the University of Wisconsin, Madison. Portions of this research were supported by the Wisconsin Alumni Research Foundation, and by the Veterans Administration, including facilities and resources at the Geriatric Research Education and Clinical Center of the William S. Middleton Memorial Veterans Hospital, Madison, WI.
We thank the staff and study participants of the Wisconsin Registry for Alzheimer’s Prevention without whom this work would not be possible.