
Abstract
Alzheimer’s disease (AD) is a complex, multifactorial neurodegenerative disorder that represents a major and increasing global health challenge. In most cases, the first clinical symptoms of AD are preceded by neuropathological changes in the brain that develop years to decades before their onset. Therefore, research in the last years has focused on this preclinical stage of AD trying to discover intervention strategies that might, if implemented effectively, delay or prevent disease progression. Among those strategies, mind-body therapies such as yoga and meditation have gained increasing interest as complementary alternative interventions. Several studies have reported a positive impact of yoga and meditation on brain health in both healthy older adults and dementia patients. However, the underlying neurobiological mechanisms contributing to these effects are currently not known in detail. More specifically, it is not known whether yogic interventions, directly or indirectly, can modulate risk factors or pathological mechanisms involved in the development of dementia. In this article, we first review the literature on the effects of yogic practices on outcomes such as cognitive functioning and neuropsychiatric symptoms in patients with mild cognitive impairment and dementia. Then, we analyze how yogic interventions affect different risk factors as well as aspects of AD pathophysiology based on observations of studies in healthy individuals or subjects with other conditions than dementia. Finally, we integrate this evidence and propose possible mechanisms that might explain the positive effects of yogic interventions in cognitively impaired individuals.
INTRODUCTION
Alzheimer’s disease
Alzheimer’s disease (AD) is a progressive, age-associated neurodegenerative disorder and represents the most common form of dementia. According to the 2019 World Alzheimer Report, around 50 million people worldwide are currently affected, and due to the increase in the population’s life span, the number of patients diagnosed with dementia is constantly rising. Without a breakthrough in prevention or therapy, current predictions and extrapolations suggest that 82 million dementia patients will accumulate worldwide in 2030 and 152 million in 2050 [1].
In Latin America, the demographic transition takes place at a faster rate when compared to Europe and North America. From 7.8 million people with dementia in 2013, the number of affected individuals is supposed to rise up to 27 million by 2050 [2]. In Mexico, the incidence of AD is 27.3 per 1,000 people/year. In 2014, around 86,000 people were affected by AD in Mexico and projection studies show that this number will rise up to 3.5 million until 2050 [3]. The impact of such an alarming increase in dementia cases on economic, social, and health systems in Latin American countries will be enormous.
Clinically, AD manifests as a progressive cognitive decline and memory loss. Between normal aging and dementia, mild cognitive impairment (MCI) represents an intermediate clinical state between the normal changes of cognitive functioning during aging and early features of AD [4]. The mild cognitive symptoms seen in MCI do not interfere with everyday life abilities; however, MCI patients start to show a decline in learning and memory ability [5]. The annual progression rate of MCI to clinically probable AD is approximately 5–10% [6]. Years or even decades before the clinical manifestation of AD, neuropathological changes become present in the brain of AD patients. These include the extracellular deposition of amyloid-β (Aβ) peptides in form of Aβ plaques and the formation of neurofibrillary tangles (NFTs) composed of hyperphosphorylated tau filaments. Aβ depositions and NFTs get physiologically cleared by processes such as autophagy and proteasome degradation and therefore form part of the normal aging process. However, in AD these processes become inefficient leading to an abnormal accumulation of the protein aggregates [7–10]. Moreover, AD pathology is associated with a neuroinflammatory reaction as well as the loss of neurons and synapses, leading to cerebral atrophy [11].
Epidemiologically, AD is classified into the rare familial (early-onset) form and the sporadic (late-onset) form. The familial form of AD develops before the age of 65 and is caused by mutations in the amyloid precursor protein (APP) gene or the presenilin genes PSEN1 and PSEN2, and accounts for less than 5% of all AD cases. The predominantly occurring sporadic form of AD develops above the age of 65 and so far, only risk factors have been identified [12], which include advanced age, diabetes, obesity, hypercholesterolemia, a history of head trauma, midlife hypertension, and genetic factors (the presence of the APOE4 allele) [13]. Moreover, psycho-affective states such as anxiety, depression, and chronic stress are increasingly linked to a higher risk of developing AD [14].
Although numerous large clinical trials have been performed in recent years, a causal therapy is not within reach and the currently available treatment options for AD only reduce associated symptoms but do not prevent the progression of the disease [15]. Therefore, preventive approaches are exceedingly discussed as means to minimize the risk of developing AD. As already mentioned, the first symptoms of AD are preceded by neuropathological changes that develop years to decades before their onset. Therefore, in most of the cases AD develops slowly, offering a large time window for therapeutic and non-therapeutic intervention. Non-pharmacological therapies such as memory training, physical and cognitive activity, or diet interventions have shown promising effects on cognitive function and functionality in both MCI and AD patients [16–19]. Especially physical activity is demonstrated to have a positive effect on brain function and plasticity. Neuroimaging studies with older adults showed that aerobic exercise training increases hippocampal volume associated with improved spatial memory. These observations are accompanied by increased serum brain-derived neurotrophic factor (BDNF) levels [20]. Furthermore, individuals with increased genetic risk for the sporadic form of AD demonstrated reduced hippocampal atrophy levels after 18 months of physical activity when compared to sedentary controls [21]. Next to the effect of exercise on the aging brain structure, a positive influence on functional connectivity between different brain areas associated with an improved executive function was observed in older adults due to aerobic training [22]. In AD patients, several studies reported significant cognitive improvements due to different types of exercise interventions (e.g., daily walking) [23, 24]. However, the precise molecular mechanisms responsible for the beneficial effects of regular exercise in AD patients remain to be elusive. Besides increased BDNF levels, one reported mechanism of physical activity might involve a change of microRNA expression profiles in the circulation. In AD patients, numerous miRNAs are either upregulated (e.g., miRNA 30e, miRNA 200c, miRNA 34c) or downregulated (e.g., miRNA 107, miRNA 485) in both brain and blood samples when compared to cognitively healthy control individuals [25]. Interestingly, the expression of several of them are restored by physical activity, for example miRNA 34c, which is upregulated in AD patients, decreases with exercise (for review, see [26]).
More recently however, mind-body therapies (MBT) have emerged as an important complementary and alternative medicine for many neurological diseases and conditions [27].
Mind-body therapies
MBTs include a wide range of practices such as yoga, meditation, mindfulness, Tai Chi, and Qigong that focus on breathing exercises, meditation, and structured movements. Being rooted in ancient eastern traditions, the goal of these techniques is an interaction between the brain, mind, body, and behavior with the intention to enhance the capacity of the mind in order to affect physical functions and promote health [28, 29]. Even though MBTs vary in their techniques, they commonly produce physical and psychological benefits in both healthy and clinical populations [30]. Among all mind-body interventions, yoga and meditation are most popular and widely accepted in the western society.
Yoga is an ancient Indian physical and mental practice that originated around 5,000 years ago. The word yoga is derived from the Sanskrit word “yuj” and means “to join”. Literally, yoga seeks the union of body and mind with the universal spirit. While the ancient yoga practice based on the Indian sage Patañjali includes eight distinct practices (also called limbs), yoga as practiced in our modern society emphasizes only three out of these eight traditional limbs, namely: physical postures (asanas), regulated breathing (pranayama), and meditation (dhyana). Hatha yoga includes the practice of these three limbs and therefore represents the most popular form of yoga in western countries [31]. The missing limbs include ethical behavior (yamas), personal behavior (niyamas), sensory inhibition (pratyahara), concentration (dharana), and integration (samadhi). Hence, yoga is a multi-dimensional behavioral practice and according to the National Center for Complementary and Integrative Health the most popular form of complementary therapies [32].
The term “meditation” includes several different techniques which all share common principles. Such techniques include focusing on the breath, repeating a mantra (affirmation), or overcoming emotional turbulence to achieve a mentally clear and emotionally stable state and inner calm [33, 34]. Among many types of meditation, “Mindfulness meditation” has gained interest in western countries [35]. The Mindfulness meditation approach aims to pay attention to thoughts and feelings and respond mindfully to them instead of reacting automatically. One can therefore cultivate kindness and compassion and overcome negative cycles of thoughts, feelings, and behaviors [36, 37].
In western cultures, yoga and meditation have emerged as tools to reduce stress, improve well-being, and promote general health. A regular physical yoga practice has shown to enhance posture, muscular strength, balance as well as increase flexibility and joint range of motion [38]. Furthermore, several studies described a beneficial effect of yoga on metabolic diseases such as diabetes and metabolic syndrome [39–41]. In the last few years, however, research has shown that mental, spiritual, and physical yoga and meditative practices also have regulatory effects on brain structure and function. Hence, positive impacts of these MBTs have been shown in a variety of neurological disorders such as depression [42], anxiety [43], epilepsy [44], stroke [45], Parkinson’s disease [46], and multiple sclerosis [47]. Despite the effectiveness of meditation and yoga techniques in neurological disorders, the molecular mechanisms of these benefits remain inadequately understood. There is scientific evidence that yogic interventions can influence biological concentrations of systemic biomarkers of neuroplasticity, which include hormones, neurotransmitters, inflammation markers, oxidative stress markers, DNA damage markers, and telomere metabolism markers [48]. In the following sections, we examine the effect of yoga and meditation on a subset of these biomarkers in more detail. As only a few studies have investigated the impact of yoga and meditation interventions in older individuals with cognitive impairments, in the first part of this article, we review relevant studies on the effect of these practices in patients with MCI and dementia. In the next part, we examine risk factors and pathological features implicated in the development of AD and seen modulated by these mind-body interventions in healthy individuals or people with other conditions than dementia. Finally, we integrate these results and propose how yogic interventions might slow down the progression of AD pathology. The pathogenesis of AD is complex and involves a multitude of direct and indirect mechanisms. Given the comprehensive literature on this topic, here we focus on selected AD-related risk factors and pathological features for which effects of yoga and meditation interventions have been described. As meditation is an active part of the yogic practice, their individual effects on the brain are difficult to separate. Therefore, studies with both yoga and/or meditation interventions are included in the present article (Tables 1 and 2).
Characteristics of intervention studies evaluating the effects of yoga and meditation practices reviewed in this article
Characteristics of cross-sectional studies evaluating the long-term effects of yogic practices mentioned in this article
THE EFFECT OF YOGIC PRACTICES IN INDIVIDUALS WITH SUBJECTIVE COGNITIVE DECLINE, MCI, AND DEMENTIA
Several studies have investigated the effect of yogic interventions in patients diagnosed with MCI. One study assigned MCI patients randomly to 12 weeks of Kirtan Kriya meditation practice (12 min daily) with weekly booster sessions of Kundalini Yoga (60 min) or an active control group receiving memory enhancement training (MET). Statistically significant improvements in measures of depression, visuospatial memory, verbal memory performance, and connectivity between default mode networks were revealed in both the yoga and active control group [49]. Another study performed by the same group of researchers employed a different cohort of MCI subjects, who were again randomly assigned to either KY (once per week for 60 min) and daily KK practice (12 min) or MET for 12 weeks. Cognitive (memory and executive functioning) and mood (depression, apathy, and resilience) assessments were measured before intervention, after 12 weeks and after 24 weeks as a follow-up examination. After 12 weeks and at the 24 weeks follow-up examination, patients of both yoga and MET group showed a significant memory improvement. However, only subjects who practiced yoga displayed improvement in executive functioning at these time points. Moreover, only those patients who were assigned to the yoga group demonstrated significant improvements in depression and resilience [50]. In a more recent study adults older than 50 years experiencing subjective cognitive decline (SCD) were randomly assigned to a 12-week KK meditation or Music Listening (ML) program (12 min daily). Both groups experienced significant improvements in memory function, cognitive performance, sleep quality, and mood. Interestingly, only the KK group showed reduced stress levels and a significantly improved quality of life (QOL), which is assessed by a health survey questionnaire for self-report measure of functional health and well-being. Improvements in all measures were maintained or even further improved in a follow-up examination 6 months after the beginning of treatment [51]. Related findings were reported from studies investigating the combination of different behavioral interventions in patients with impaired memory or MCI. McDougall et al. reported in 2010 that the SeniorWISE (Wisdom Is Simply Exploration) memory training improved cognitive performance in elderly [52]. In a follow-up study, the researchers added a 30 min yoga session before each memory training session to test if yoga would improve their performance even further. Over four weeks, participants attended two training sessions per week (in total 12 h of SeniorWISE memory training and 4 h of yoga). From baseline to post-intervention, 48% of the participating subjects increased their performance from one memory performance group to the next higher one (from severely impaired to moderately impaired; from moderately impaired to poor; or from poor to normal) [53]. In another study, MCI patients were randomly assigned to a group that included 4 of the following 5 interventions: memory compensation training, computerized cognitive training, yoga, patient and partner support group, and wellness education. Following a 2-week program (50 h of intervention in total), participants received a 1 h booster session after 6 and 12 months of intervention, respectively. Functional memory was assessed at baseline, treatment end, 6 months after intervention, and 12 months after intervention, among other parameters. Interestingly, 12 months after intervention, yoga had a greater effect on memory-related activities of daily living than all the other groups [54].
Next to the studies in individuals with SCD and MCI, a limited number of reports examining effects of yogic interventions in dementia patients are found in the literature. While Fan et al. demonstrated improved physical and mental health after 12 weeks of Chair yoga practice in dementia patients, a more recent study only reported a significant improvement in quality of life after the same intervention time in older adults with moderate to severe dementia [55, 56]. Furthermore, an 8-week program of “Sit ‘N’ Fit Chair Yoga” has shown to improve motor function in older subjects with moderate and severe AD. Physical function was measured using the six-minute walk test, gait speed test, and Berg balance scale and an improvement was seen in all tests after the yoga program [57]. Apart from chair yoga, another study investigated the effect of the yogic meditation KK in adults with MCI or early-stage AD. Eight weeks (twice daily) of KK practice was shown to be effective in improving perceived stress, mood, depression, sleep, and retrospective memory [58]. Similar research by Moss et al. investigated how KK affects mood and anxiety in subjects with memory loss, including three diagnosed with AD. Eight weeks of KK resulted in trends towards improved mood, anxiety, tension, and fatigue. Furthermore, the results of the meditation program correlated with cerebral flood flow changes [59]. In another 36-week pilot clinical trial, individuals with mild-to-moderate dementia were randomly assigned to a PLIÉ (Preventing Loss of Independence through Exercise) intervention or a Usual Care control group. PLIÉ is an integrative exercise program that combines elements of conventional and complementary exercise modalities (physical therapy, occupational therapy, yoga, tai chi, dance movement therapy). When compared to controls, individuals in the PLIÉ group showed improvements in physical function, cognitive function, and quality of life [60]. Next to the PLIÉ study, also Khoo et al. examined the feasibility of a combination of yoga and meditation with other approaches such as dance movements and conventional physical exercise in dementia patients. Interestingly, patients benefited both psychologically as well as physically from the holistic approach [61].
In summary, even though the literature on the effects of yogic interventions in older adults diagnosed with MCI or dementia is scarce, existing studies suggest that yoga might have beneficial effects on outcomes such as cognitive functioning (particularly on memory function), neuropsychiatric symptoms such as mood and perceived stress as well as motor functions and quality of life. Surprisingly, none of the studies have investigated whether yogic practices in cognitively impaired individuals affect directly or indirectly pathophysiological features of AD. Therefore, in the following section, we will review relevant pathological characteristics implicated in AD that are likely to be modulated by yogic interventions based on observations in healthy adults or subjects with medical conditions other than dementia.
PATHOLOGICAL FEATURES AND RISK FACTORS OF ALZHEIMER’S DISEASE AND THEIR MODULATION BY YOGIC PRACTICES
Grey matter atrophy
Grey matter (GM) atrophy is one of the most prominent pathological features of AD. The atrophy is caused by a region-specific neuron death as well as loss of synapses, and is characterized by enlarged ventricles, widening of cortical sulci, and shrinkage of gyri. Being part of the normal aging process, brain atrophy starts in the early twenties to mid-thirties and leads to a reduction of 0.2–0.41% of brain mass per year. However, in AD, these rates are much higher, especially in vulnerable brain areas [62, 63]. As brain volume and weight reductions can be detected at very early stages of disease progression (up to ten years before clinical diagnosis of AD), GM atrophy is a predictable marker for the progression of MCI to AD [64]. A brain region predominantly affected by GM atrophy is the medial temporal lobe, which plays a central role in memory processing and includes structures like the hippocampus, amygdala, and entorhinal cortex [65]. Studying hippocampal atrophy using magnetic resonance imaging (MRI) techniques is the best documented method to differentiate prodromal AD cases from healthy patients, as well as to differentiate AD from other pathological conditions [66]. With the new approach of hippocampal subfield atrophy assessment, De Flores et al. revealed that the CA1 region and the subiculum are the most vulnerable hippocampal regions to degeneration in normal aging and during the progression of AD [67]. The underlying causes of the decrease in the number of neurons in AD are still not known in detail. It is assumed that the reduction in neuron number originates from an increase in natural neuron death, together with impaired maturation and functional integration of new-born neurons in the dentate gyrus, and decreased levels of postnatal neurogenesis [68]. Moreover, the precise molecular mechanisms of neuron death in AD remain elusive; however, numerous studies suggest that neurotoxicity of intraneuronal and/or oligomeric Aβ peptides play a crucial role in this process [69–71].
Until now, there is no study investigating the effect of yoga and meditation on brain macrostructure in AD patients; however, a limited number of short-term longitudinal neuroimaging studies in MCI patients exists. Fotuhi et al. used a multi-disciplinary brain fitness program that includes the practice of mindfulness meditation to test its effect on hippocampal volume in MCI patients. After 12 weeks of the intervention, 84% of participants improved their cognitive function significantly. Furthermore, a random subset of 17 patients received a post-program MRI which showed that 70.6% displayed no hippocampal atrophy and, in some cases, even an increased hippocampal volume when compared to baseline values [72]. In another study, an 8-week long Mindfulness Based Stress Reduction (MBSR) intervention including mindfulness meditation and yoga led to a trend toward a reduced bilateral hippocampal volume atrophy in MCI patients as shown by MRI volumetric analysis. In the same study, Wells et al. demonstrated that the MBSR intervention leads to an increased functional connectivity between cortical areas and the left hippocampus when compared to controls using functional MRI (fMRI) resting state analysis [73]. Yang et al. revealed the effect of 12 weeks of MET or Kundalini Yoga (KY) on brain plasticity of MCI patients. They analyzed GM volume as well as concentrations of brain metabolites in bilateral hippocampus and the dorsal anterior cingulate cortex (dACC) using structural MRI (s-MRI) and proton magnetic resonance spectroscopy (1H-MRS), respectively. While the MET intervention led to significantly increased dACC GM volume and decreased hippocampal choline levels, no changes in dACC or hippocampus GM volume were found in the yoga group [74].
Apart of studies performed in MCI patients, several short-term longitudinal studies have investigated the possible modulating effects of yoga and meditation practices on brain macrostructure changes in healthy individuals. In one of the first studies investigating the effect of mind-body interventions on brain volume changes, 8 weeks of MBSR intervention in healthy, meditation-naive individuals revealed an increased volume in left hippocampus, posterior cingulate cortex, temporo-parietal junction, and the cerebellum as shown by anatomical MRI scans [75].
In another study conducted among healthy elderly subjects, Hariprasad et al. performed structural brain MRIs before and after a 6-month yoga intervention. Interestingly, the yoga practice increased hippocampal GM volume bilaterally while no volume changes were observed in the occipital cortex, which is least affected in age-related brain atrophy and therefore was used as a control brain region [76]. In another anatomical MRI study done in two cohorts of in total 102 young and healthy individuals, the effect on brain structure was compared between a yoga group, an active sport group, and a passive control group. After 10 weeks of Hatha yoga, right hippocampal GM density was increased, while no such effect was seen after the active sport intervention or under control conditions [77]. Recently, Dodich et al. reported that 4 weeks of Sahaja yoga meditation leads to increased GM density in healthy, meditation-naive individuals as measured by structural MRI analysis. Furthermore, resting state fMRI studies revealed that the intervention induced intrinsic brain activity in brain regions associated with self-control, self-awareness, and attention [78].
In addition to these intervention studies, numerous cross-sectional studies have investigated the possible long-term effect of yoga and meditation on changes in cerebral macrostructure using structural MRI methods. These investigations revealed increased GM volume in long-term meditators when compared to meditation-naive controls. Additionally, Chételat and colleagues demonstrated that life-long meditation reverses age-related decreases in brain glucose metabolism as elderly expert meditators showed increased fluorodeoxyglucose (FDG) metabolism in FDG-positron emission tomography (PET) Scans when compared to meditation-naive elderly controls [79–81]. Likewise to long-term meditation, structural MRI studies revealed that various years of regular yoga practice seem to increase GM volumes in brain regions such as hippocampus, prefrontal cortex, and cerebellum [82–85].
Plasma amyloid-β levels
Beside GM atrophy, one of the major neuropathological hallmarks of AD is the extracellular accumulation of Aβ peptides in form of plaques. Aβ peptides are liberated via the sequential cleavage of α- and γ-secretases from the longer AβPP protein. While the full-length Aβ1–40 and Aβ1–42 peptides form the main components of the extracellular plaques, a variety of shorter C- and N-terminally truncated Aβ versions have been identified in the brains of AD patients [86]. Besides total tau (T-tau) and phosphorylated tau (P-tau) levels, Aβ42 levels represent one of the core AD neurochemical biomarkers in the cerebrospinal fluid (CSF). Numerous studies have reported low Aβ42 CSF levels in patients with MCI or AD. As this decrease in Aβ42 concentration is negatively correlated with the uptake of the 11C-Pittsburgh compound B in in vivo amyloid PET imaging, it appears to display the grade of Aβ plaque accumulation in the brain [87]. While the collection of CSF requires lumbar puncture, blood can be sampled by minimally invasive procedures and therefore would be a more practical approach. However, one major challenge is that Aβ blood plasma levels are roughly 50–100 times lower than in CSF [88]. Furthermore, it has been suggested that only between 30–50% of the Aβ peptides in blood plasma derive from the brain [89]. Despite these challenges, the diagnostic potential of Aβ peptides as candidate AD biomarkers in blood plasma samples has been investigated in various studies. Numerous reports suggested that a low Aβ42/Aβ40 ratio and/or low Aβ42 levels in blood plasma serve as a potential biomarker of AD [89–92]. Consequently, higher Aβ42/Aβ40 ratios are associated with a lower risk to develop dementia [93].
So far, two studies have investigated the effect of mind-body interventions on Aβ blood plasma levels. In the first controlled trial, healthy individuals were randomly assigned to a 1-week meditation/yoga retreat or a ‘vacation-only’ control group. Members of both groups had no or little meditation experience before the intervention. As a third comparison group, regular meditators were recruited to study different effects of the meditation/yoga retreat in meditation-naive and meditation-experienced individuals. Blood samples were collected at baseline and after the retreat and Aβ40 and Aβ42 plasma levels were analyzed. Interestingly, regular meditators had higher Aβ42/Aβ40 ratios at baseline when compared to the other two groups. However, these levels did not change further due to the intervention. On the other side, the novice meditator group as well as the vacation control group showed significantly decreased plasma Aβ40 levels after the retreat, which also led to significantly increased Aβ42/Aβ40 ratios. These results indicate a beneficial effect of consistent meditation as well as short-term meditation and relaxation on brain health [94].
A more recent study employed Aβ plasma levels in individuals reporting SCD. Subjects were randomly assigned to a KK intervention or a music-listening control group. Following a 12-week program (12 min of KK or music-listening per day), the music-listening group displayed a higher increase in Aβ42/Aβ40 ratio than the KK group, which is contradictory to the results reported by Epel and colleagues [51].
Neurotrophin imbalances
Neurotrophins are a family of polypeptides that regulate neuronal development, survival, function, and plasticity. In mammals, neurotrophins include BDNF, nerve growth factor (NGF), neurotrophin-3 (NT-3), and neurotrophin-4/5 (NT-4/5). BDNF is the most abundantly expressed neurotrophin in the central nervous system (CNS) [95]. Both BDNF mRNA and protein show a widespread distribution throughout the CNS with a predominant localization within neurons in regions relevant for cognitive function, such as cortex and hippocampus. Hence, the neurotrophin plays an important role in modulating cognition and memory. BDNF functions by inducing hippocampal long-term potentiation, enhancing neurogenesis, inducing neurotransmission across synapses, modulating synaptic plasticity, and stimulating synaptic growth [96]. However, BDNF is also expressed in peripheral tissue such as kidneys, prostate, liver, retina, adipose cells, and skeletal muscle. Translation of BDNF mRNA in the endoplasmic reticulum initially results in the synthesis of the pre-pro-BDNF precursor protein. Following removal of the signaling peptide of pre-pro-BDNF, pro-BDNF is converted to mature BDNF by intra- and extracellular proteases. Once secreted to the extracellular space, BDNF can elicit its physiological function by binding to the high-affinity receptor tropomyosin receptor kinase B (TrkB) or the low-affinity receptor neurotrophin receptor p75 (p75NTR) of adjacent neurons [97].
The physiological levels of BDNF are extremely low; however, only picomolar concentrations are needed to elicit biological responses, thus making it a highly potent substance. The neuronal expression of BDNF can be affected by hormones, neurotransmitters, pathological states, as well as numerous physiological stimuli and therefore represents a highly dynamic process. Importantly, BDNF crosses the blood-brain barrier and therefore it is assumed that serum BDNF levels reliably reflect cerebral BDNF concentrations [98–100]. A recent meta-analysis of studies on BDNF serum levels in individuals with MCI, AD, and in healthy controls concluded that AD patients have significantly lower BDNF serum levels compared to healthy individuals. However, MCI patients do not show significant differences when compared to controls. Therefore, significant changes in peripheral BDNF levels seem to be characteristic for late stages of disease development [101]. In accordance with this meta-analysis, Weinstein and colleagues discovered that higher serum BDNF levels in older adults might be protective against developing AD in the future [102]. To our knowledge, no study so far investigated the effect of mind-body interventions on BDNF serum levels in individuals with MCI or dementia, but numerous studies demonstrated that yogic practice increases serum BDNF levels in healthy individuals [103, 104], subjects with chronic lower back pain [105] as well as in patients with depression [48, 106]. Like AD, depressive disorders are associated with low serum BDNF levels and these levels are inversely correlated with the severity of the disease [107, 108]. Furthermore, hippocampal volume is reduced in depressive patients and decreased BDNF serum levels significantly correlate with this volume reduction [109]. Halappa and colleagues reported that the more BDNF serum levels increased due to yogic practice, the better depressive patients performed in neuropsychological tests, however, without reaching significant difference in most of the tests [106].
Besides BDNF, also NGF has been demonstrated to be important for cognitive functioning and its levels decrease with aging [110]. NGF is particularly involved in the function and survival of cholinergic neurons of the basal forebrain complex (BFC). Cholinergic BFC neurons are highly vulnerable to degeneration during AD progression and therefore administration of NGF is examined as a potential therapeutic option for AD patients [111]. While studies investigating NGF level changes caused by mind-body interventions in individuals with cognitive decline are still missing, a pilot study with cognitively normal volunteers investigated if yogic breathing (Pranayama) stimulates the expression of salivary NGF. Healthy participants were randomly assigned into yogic breathing (YB) or attentional control (AC) groups and NGF concentration was measured in saliva before and after the 20 min intervention. Both ELISA and western blot experiments demonstrated an increase in salivary NGF levels after YB, but not in the control group [112]. It was demonstrated before that after intranasal administration, NGF bypasses the blood-brain barrier as it can be detected in the spinal cord 24 h after a single dose [113]. Therefore, the stimulation of endogenous NGF expression by yogic intervention might directly affect cholinergic BFC neurons.
Serotonin imbalances
The loss of cholinergic neurons in the basal forebrain as well as decreased choline acetyltransferase (ChAT) activity represent one of the earliest neuropathological events in AD. Therefore, a primary role in AD pathology was traditionally assigned to a defect in the acetylcholine neurotransmitter system [114]. Besides the cholinergic system, the serotonergic neurotransmitter system also undergoes pathological changes in AD. In the CNS, the biogenic monoamine serotonin (5-HT) is produced by clusters of neurons located in the raphe area of the brainstem [115]. Serotonin regulates multiple physiological functions including mood, sleep, appetite, and sexual function. Moreover, 5-HT regulates learning processes and memory storage as raphe nuclei project the serotonergic signal to brain areas critical for cognitive functions such as hippocampus, prefrontal cortex, or amygdala [116]. Serotonin mediates its action via 15 subtypes of specific 5-HT receptors while each receptor shows a specific expression pattern in the CNS [115, 117]. These receptors, together with enzymes and transporters, regulate local serotonin concentrations and therefore modulate its action on cognitive functions [118].
In AD, multiple factors are described to contribute to the alteration of the serotonergic system. First, a reduction of levels of serotonin and its metabolites has been reported in postmortem brains of AD patients [119]. Second, a decrease in cortical 5-HT receptors expression and/or function is described in various brain regions including the hippocampus and neocortex [120, 121]. Moreover, raphe nuclei represent a preferential site for the formation of NFT and show a high susceptibility for neuronal loss, thus leading to the loss of cortical 5-HT projections [122, 123]. For a long time, it was not clear whether the deficit of the serotonergic system is only a cause of AD-related brain changes or if it is part of AD pathogenesis. A recent study by Smith et al. leads to the suggestion that deficits in the serotonin system develop very early and therefore might represent a target for prevention of the transition from MCI to AD. Smith and colleagues demonstrated that serotonin transporter availability is already declined in MCI patients in brain areas typically affected by AD. Additionally, they showed that lower serotonin transporter binding is associated with a poorer performance in verbal and visual-spatial memory tests [124].
Yoga and meditative practices are shown to increase blood plasma or serum serotonin levels in healthy subjects and women with chronic low back pain [103, 125]. It is, however, important to note that it is still under debate whether serotonin levels in the bloodstream reflect cerebral serotonin levels as only 1–2% of its total amount is produced in the brain [126]. Studies on the effect of mind-body interventions on serotonin levels in people with dementia are still lacking. However, Hassan and colleagues recently investigated the effect of neurotransmitters released during yoga in an in vitro AD model. Their aim was to illustrate potential molecular mechanisms underlying the therapeutic effects of yogic practice on AD synaptic dysfunction. Hassan et al. used an in vitro model of human induced pluripotent stem cell-derived basal forebrain cholinergic neurons with physiological levels of oligomeric Aβ1–42 (OAβ1–42) as oligomeric Aβ peptides have been identified to be the main driver in AD pathology progression [127]. OAβ1–42 induces the loss of ChAT in the basal forebrain cholinergic neurons and therefore promotes synaptic dysfunction in their model. Interestingly, the synergistic combination of serotonin + dopamine and serotonin + histamine rescued the cholinergic function in basal forebrain cholinergic neurons as the loss of ChAT was reversed. Therefore, serotonin in combination with dopamine or histamine has a protective effect on cholinergic neurons exposed to toxic Aβ oligomers [128].
Sleep disturbances
One of the lifestyle risk factors associated with AD are sleep problems as more than 40% of AD patients suffer from insomnia, daytime fatigue, sleep fragmentation, and sleep phase shifts [129, 130]. Sleep problems display an early behavioral symptom of AD. Pistacchi and colleagues demonstrated that MCI patients display the same frequency of sleep disturbances of any type as patients with AD [131]. Sleep disorders start to become present as early as amyloid depositions and therefore precede the presence of cognitive symptoms by years. Over the course of disease, sleep disruptions as well as amyloid depositions proceed simultaneously [132, 133]. A direct bidirectional relationship between sleep and Aβ was proved for the first time by the observation that Aβ levels in the interstitial fluid (ISF) of a rodent AD mouse model are higher during wakefulness and decrease during sleep. Furthermore, chronic sleep restriction significantly increased amyloid plaque formation in the same AD model [134]. Related findings were reported in humans where sleep deprivation led to increased Aβ42 levels in the CSF in cognitively healthy adults [135]. Similarly, in a more recent study, Chen et al. demonstrated that chronic insomnia patients display significantly increased CSF Aβ42 levels [136]. Another recent study could show that acute sleep deprivation also increases Aβ burden in human brains, especially in brain regions implicated in AD [137].
So far, only a low number of studies investigating the effect of MBTs in patients with cognitive decline included sleep as an outcome. As mentioned earlier, Innes et al. showed that 12 weeks of KK improved sleep quality in the long-term in adults with SCD [51]. In another study, a mixed group of frail older adults and individuals with dementia were assigned to either a mindfulness or a cognitive therapy intervention. While in both groups no changes in total sleep time, sleep efficiency, sleep latency, and sleep fragmentation were observed, participants of the mindfulness group showed reduced daytime sleep times [138]. Studies in healthy older adults and individuals suffering from medical conditions such as depression or breast cancer revealed that a regular yoga practice decreases the time to fall asleep, increases sleeping hours, improves subjective sleep quality, and enhances the sensation of restfulness in the morning [139–142]. The probable mechanisms that might improve sleep due to yogic practices include a reduction in sympathetic arousal (decrease in heart rate, decrease in plasma catecholamine levels, increase in vagal tone) and consequently a shift toward parasympathetic dominance. Furthermore, regular yogic breathing has been associated with strengthened upper airway muscles. Weakness of these muscles causes snoring, which increases sleep disturbances. Related findings showed that the improved strength of respiratory muscles due to yoga leads to a better tissue perfusion and in turn to an improved oxygen saturation. As sleep plays a crucial role in memory consolidation, sleep disruption in AD patients may represent a causative factor for ongoing memory decline. In fact, a decrease in fast sleep spindles during post-learning sleep was correlated with poorer memory performance in a study with AD patients by Rauchs et al. [143]. Interestingly, Janelsins and colleagues reported that post cancer treatment patients with memory problems showed an increased sleep quality that significantly mediated reduced memory difficulties after participating in a yoga program. These results indicate that yoga, through improving quality of sleep, can directly affect cognitive performance [144].
Chronic stress
Numerous epidemiological studies revealed that long-term psychological stress is associated with a higher risk to develop dementia later in life [145, 146]. Cortisol is a steroid hormone belonging to the class of glucocorticoids and is produced in the adrenal cortex of the adrenal gland due to stress or low blood glucose levels. The release of cortisol is mediated by the hypothalamic-pituitary-adrenal (HPA) axis and follows a circadian rhythm with highest levels in the morning (cortisol awakening response) and declining levels throughout the day [147]. The HPA axis response targets different brain regions including the hippocampus, the amygdala, and the prefrontal cortex [147]. There is growing evidence that a chronic activation of the HPA axis due to physical and psychological stressors may increase the risk of neurodegeneration by affecting the function and structure of these brain regions [148]. The hippocampus is particularly responsive to cortisol as this region contains a high concentration of cortisol receptors [149]. Cortisol plasma concentrations were found to be dysregulated in AD patients [150, 151]. In both humans and animal models, increased cortisol levels have been related to AD pathology. In aged macaque, cortisol treatment increased levels of pathogenic Aβ42 levels when compared to less toxic Aβ40 levels [152]. In AD patients, higher baseline cortisol levels in an early disease stage led to an accelerated disease progression [153]. Furthermore, higher cortisol levels in healthy older adults or AD patients were associated with higher cerebral Aβ deposition [154]. On the other side, glucocorticoid inhibition seems to have neuroprotective effects [155]. To our knowledge, there is no study examining how yogic interventions affect cortisol levels in dementia patients. In one pilot study performed by Chouinard et al., amnestic MCI patients demonstrated a slight reduction of the cortisol awakening response upon an 8-week long mindfulness-based intervention while no such changes were seen in the control group [156]. Moreover, multiple studies reported a regulating effect of yoga and meditation on cortisol levels in the blood, urine, or saliva in healthy subjects or people with other medical conditions than dementia. To name a few, Bisht et al. assessed parents of children with retinoblastoma undergoing a 12-week yoga-based lifestyle intervention program. Results showed that the intervention was associated with reduced blood cortisol levels along with decreased psychological stress [157]. Naveen and colleagues assessed serum cortisol levels of patients suffering from depression at the beginning and at the end of a 3-month yoga program. The authors were able to show a significant reduction in serum cortisol in the yoga group [158]. In a study with familial caregivers of AD patients, a 2-month yoga and compassion meditation program reduced the concentration of salivary cortisol and decreased stress, anxiety, and depression levels in the participants [159]. In a more recent study, Magan et al. demonstrated that long-term meditators have significantly lower plasma cortisol levels when compared to controls [160]. However, it is important to mention that numerous studies have not found any effect of yoga and meditation on cortisol levels [161–163].
POSSIBLE CONNECTIONS BETWEEN YOGA- AND MEDITATION-MEDIATED EFFECTS AND DEMENTIA PROGRESSION
Research on the impact of yoga and meditation practices on the brain in aging and neurodegenerative disorders is scarce. As reviewed earlier here, the limited studies with MCI or dementia patients mostly show beneficial effects of these mind-body interventions on cognitive and neuropsychiatric outcomes. However, to our knowledge, there is no literature describing how yoga interventions affect characteristic pathological AD features in dementia patients. Therefore, until now, the mechanistic link between positive effects of yoga interventions and AD-related pathological processes is unknown. On the other hand, numerous studies in healthy subjects and patients suffering from other conditions than dementia have yielded interesting results showing effects of yoga and meditation on brain volume, Aβ blood levels, and levels of cortisol, BDNF, and neurotransmitters, as well as effects on sleep quality. All these parameters, directly or indirectly, are part of the pathogenesis of AD and there is a mechanistic connection between them as depicted in Fig. 1 (left panel). Based on the observations we review here, we suggest that yoga and meditation practices affect these parameters in MCI and dementia patients as described below, actively contributing to the beneficial effects on cognitive and neuropsychiatric outcomes and slowing down disease progression (Fig. 1, right panel).
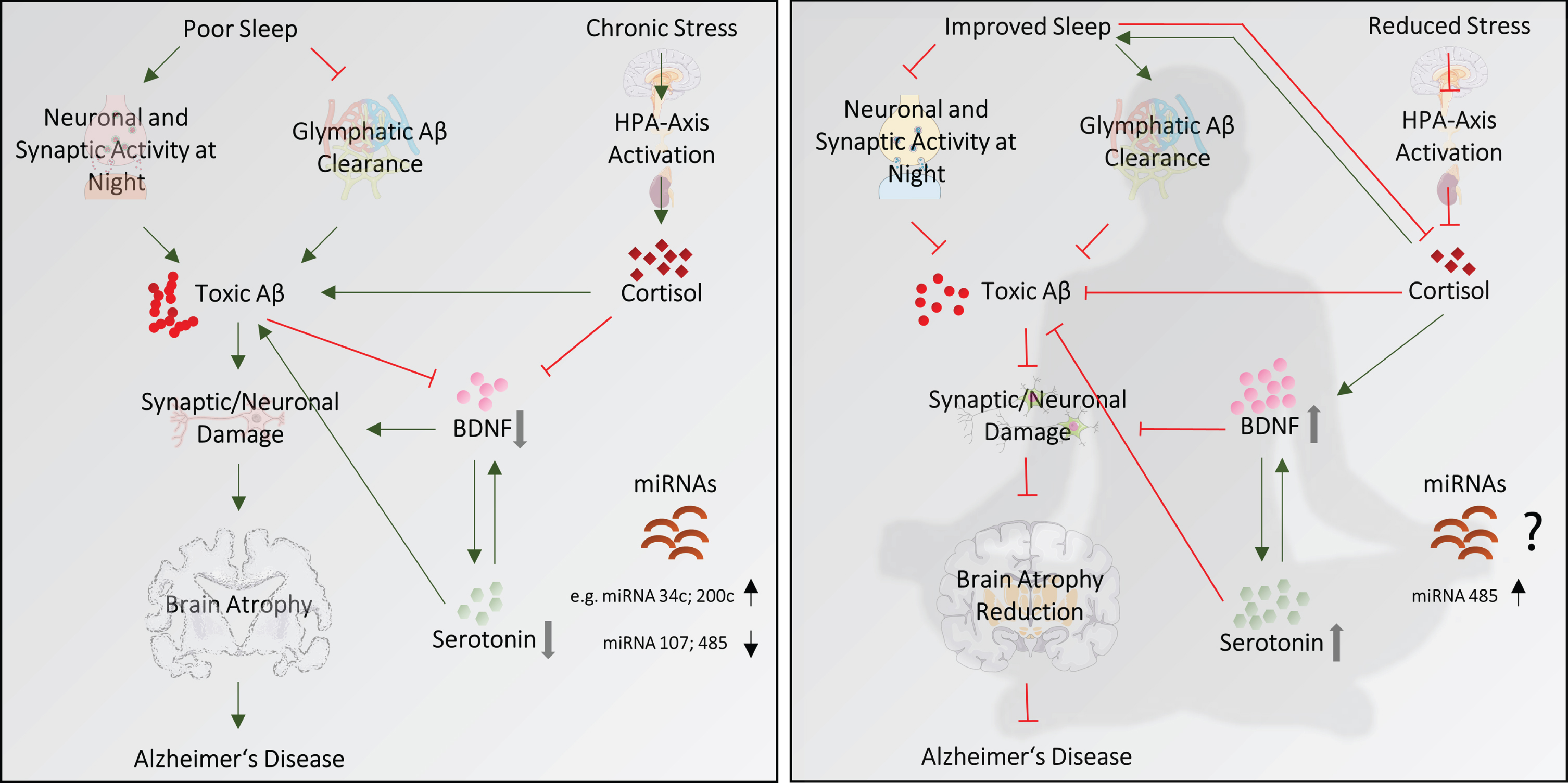
Suggested pathways by which yoga and meditation practices could prevent Alzheimer’s disease progression. Sleep disturbances, chronic stress and resulting increased cortisol levels, decreased levels of BDNF and serotonin, altered miRNAs expression as well as brain atrophy are, directly or indirectly, associated with AD progression (left). The right figure shows proposed ways how yogic interventions impact these parameters leading to a reduced disease progression. See text for details.
As mentioned before, no studies on the effect of yogic interventions on GM volume in dementia patients exist. However, numerous analysis in healthy older adults and limited studies in MCI patients mostly show positive effects of these MBTs on GM volume, especially on the hippocampus, which is one of first brain regions to be affected in AD [164, 165]. Hence, yoga and meditation seem to directly act on the structures of brain regions vulnerable to neurodegeneration and might help to retain their function and structure from the gradual age-related decline seen in dementia.
How these mind-body interventions counteract age-related mechanisms on a molecular level is not known yet, but based on several observations, the neurotrophin BDNF might play a causal role. BDNF is highly expressed in the hippocampus where it exerts its neuroprotective effects [166]. Both pre- and postsynaptically, BDNF binds to its two different transmembrane receptors TrkB and p75NTR. Binding to the main BDNF receptor TrkB leads to the activation of the three signaling cascades: PLCγ, PI3K, and ERK. In turn, the phosphorylation and activation of the transcription factor CREB induces the transcription of genes that mediate the differentiation and survival of neurons [167]. As reported in the previous section, yoga and meditation practices actively increase BDNF levels. Therefore, upregulated BDNF signaling might, at least partially, explain the repeated finding of increased hippocampal GM volumes related to these interventions. Accordingly, it is tempting to speculate that the positive effect on cognitive performance in MCI and dementia patients due to yogic interventions might be explained by BDNF-mediated mechanisms that attenuate or reverse hippocampal atrophy and thus promote cerebral neuroplasticity (Fig. 1, right panel).
Like BDNF, the neurotransmitter serotonin has shown to promote neuronal plasticity and both BDNF and serotonin levels have been shown to be decreased in AD patients [101, 119]. There is a reciprocal influence between BDNF and serotonin in the brain (Fig. 1, right panel). While serotonin signaling positively regulates BDNF expression in rat brains [168], BDNF promotes the survival and differentiation of neurons that respond to serotonin [169, 170]. Therefore, it is suggestive that the increase of one of these factors due to yogic interventions positively affects the other. Moreover, several studies reported a direct action of serotonin on Aβ peptides. It was demonstrated in vitro that serotonin effectively destabilizes Aβ oligomers and fibrils, leading to a protection against Aβ-induced neuronal death. One proposed mechanism underlying the neuroprotective effect of serotonin is the induction of SIRT1- and 2, heat shock protein 70 and heme oxygenase expression [171]. Moreover, the activation of specific 5-HT receptors induces the non-amyloidogenic processing of AβPP in vitro, leading to the production and secretion of AβPP ectodomain (AβPPs), which has neurotrophic and neuroprotective properties. Therefore, the production of toxic and aggregation-prone Aβ species is prevented [172, 173]. Furthermore, selective serotonin reuptake inhibitors (SSRIs) prevent Aβ42 aggregation and fibrillogenesis by directly interacting with the amyloid peptide at its N-terminus [174]. SSRIs also decrease cerebral Aβ levels in both human and mice after chronic administration [175, 176]. Accordingly, it is suggestive that the release of the neurotransmitter serotonin due to yogic practices might directly reduce harmful Aβ species and thus contributes to the protection of cholinergic synaptic transmission in AD (Fig. 1, right panel).
The two published studies that investigated how meditation interventions affect Aβ blood levels showed contradictory results. However, long-term meditators demonstrated higher baseline Aβ42/Aβ40 ratios when compared to meditation-naive individuals, which is associated with a lower risk to develop dementia [51, 94]. Therefore, long-term meditation seems to have a measurable effect on Aβ plasma levels. This result leads to the suggestion that a constant meditation practice has a direct regulative effect on Aβ and future research is needed to investigate the physiological mechanism behind.
Possible lifestyle risk factors associated with the development of dementia and sporadic AD are sleep quality and chronic stress. As mentioned before, the quality of night sleep directly affects cerebral Aβ levels. The underlying mechanisms of this phenomenon are not entirely clear; however, different hypotheses are under debate. Under physiological conditions, the brain maintains constant levels of Aβ by a dynamic balance between its synthesis, clearance, and re-uptake [177]. A plethora of studies demonstrated that the clearance of Aβ from the ISF out of the brain primarily occurs during sleep [178]. In rodent animal models, it could be shown that Aβ is transported from the ISF out of the brain by the “glymphatic system”, a clearance system that eliminates waste from the CNS to maintain brain homeostasis. During sleep, the action of the glymphatic system increases and therefore Aβ is cleared more efficiently than during waking hours [178]. In humans, however, the existence of such a clearance system is assumed but is still under investigation. Another potential mechanism underlying the bi-directional relationship between sleep and Aβ is neuronal and synaptic activity. Cirrito and colleagues demonstrated for the first time in a rodent AD mouse model that increased synaptic activity enhances ISF Aβ levels in vivo. Therefore, increased wakefulness and its accompanying excitotoxicity increase the production of toxic Aβ species. On the other side, decreased neural activity during sleep is associated with increased Aβ clearance and lower production of the peptide. As yoga and meditation have repeatedly shown to improve sleep quality in healthy older adults and people with other medical conditions than dementia, we propose that a better night sleep might contribute to the cerebral clearance of Aβ and a reduced production of toxic amyloid species in patients with MCI and dementia (Fig. 1, right panel).
Chronic stress can increase an individual’s susceptibility to develop neurodegenerative diseases. Compared to healthy controls, AD patients demonstrate more than 80% increased CSF cortisol levels, illustrating a direct relationship between AD and stress [180]. An activation of the HPA axis as a response to physiological and psychological stressors leads to the secretion of cortisol into the blood stream, which crosses the blood-brain barrier and activates glucocorticoid receptors in various brain regions. As mentioned earlier, hypersecretion of cortisol and its downstream signaling has been associated with abnormal amyloid deposition in both humans and animal models, resulting in synaptic dysfunction and neurodegeneration [181, 182]. The mechanism of how stress accelerates the production and deposition of Aβ remains unclear; however, the activity of the corticotrophin-releasing factor seems to influence the production of Aβ. Studies in AD mice models revealed that stress increases the release of corticotrophin-releasing factor which in turn increases basal levels of neuronal activity, ultimately stimulating Aβ release [148]. Even though research on the effect of yogic practices on cortisol levels in dementia patients is still lacking, results from existing studies in other stressed individuals show promising results. These practices not only lead to measurable decreased cortisol levels but also to lower subjective stress, anxiety, and depression. Accordingly, yoga might downregulate cortisol levels and slow down pathological deposition of Aβ while at the same time decrease neuropsychiatric symptoms such as depression in MCI and AD patients (Fig. 1, right panel). Furthermore, there seems to be a direct connection between cortisol and sleep quality. While deregulated cortisol concentrations correlate with poor sleep quality, an acute sleep loss has been associated with elevated cortisol levels [183, 184]. Therefore, even though experimental demonstration is missing, it is tempting to speculate that decreased cortisol levels due to yogic practices in dementia patients might positively affect sleep quality while at the same time, improved sleep may normalize cortisol imbalances (Fig. 1, right panel).
As mentioned before, deregulated miRNAs have been proposed as biomarkers for AD. The miRNA miR-34c is upregulated in AD brain and blood samples when compared to healthy controls and regular exercise has shown to be sufficient to normalize its serum levels [26]. Interestingly, miR-485, which has been demonstrated to be downregulated in AD patients, is upregulated due to a yogic intervention in patients with myalgic encephalomyelitis/chronic fatigue syndrome [185]. Even though so far no such study exists with AD patients, it is tempting to speculate that a normalization of deregulated miRNAs could also occur in dementia patients due to yoga and meditation (Fig. 1, right panel).
CONCLUSION AND FUTURE DIRECTIONS
So far, research on how yoga and meditation practices might affect the process of neurodegeneration in MCI and dementia patients is scarce. Nonetheless, here we present sufficient evidence supporting the proposal that these mind-body interventions can, directly or indirectly, influence specific pathological characteristics of AD, acting as a barrier for neurodegeneration and slow down the progression of the disease (an integrative cartoon is presented in Fig. 1). In summary, we propose that yoga and meditation can reduce the presence of toxic Aβ species in the brain by improving sleep quality, lowering the stress hormone cortisol, and increasing the neurotransmitter serotonin and the neurotrophin BDNF levels. In dementia patients, improved sleep quality due to yoga and meditation [139, 140] could decrease the presence of toxic Aβ species in the brain, based on the findings that the clearance of Aβ peptides primarily occurs during sleep [177] and decreased neural activity during sleep is associated with a lower production of the peptide [186]. Yogic interventions decrease subjective stress and therefore lower cortisol levels [157, 158], and cortisol is associated with abnormal amyloid deposition [154]. A feedback loop could foster this positive effect, where decreased cortisol levels due to yogic interventions positively affects sleep quality, while improved sleep helps normalizing cortisol imbalances, since a reciprocal influence of one over the other has been proved [183, 184]. Yoga and meditation practices increase serotonin level [105], and serotonin prevents the formation of harmful Aβ species [171]. Additionally, yoga and meditation can stimulate neuronal plasticity through an increase of BDNF [103, 104], which also has a protective effect on neurons and synapses. In part, this function might explain increased brain volumes as well as improved cognitive performances. Based on the reciprocal influence of BDNF and serotonin in the brain [168, 169], we furthermore suggest that the increase of one of these molecules due to yoga and/or meditation has a positive feedback effect on each other. Furthermore, yogic interventions might balance the deregulation of miRNA expression seen in AD patients [185].
Both short- and long-term studies with subjects suffering from cognitive decline are necessary to draw up the relationship between yogic practices and molecular mechanisms involved in the development of AD. Future research needs to clarify if there is a correlation between increased GM volume, BDNF level changes, and improved memory performance due to yoga practices in patients with cognitive decline in order to reveal if there is a mechanistic link between them. Furthermore, it would be of interest to investigate if improved sleep quality due to yoga and meditation leads to changes in CSF and plasma Aβ levels and/or compositions in dementia patients. Moreover, an experimental demonstration is needed to clarify if decreased perceived stress and cortisol levels due to yoga interventions can directly affect the extent of amyloid deposition in the brain. It would be interesting to study also if misregulated miRNAs in AD are also modulated by yoga and meditation. Also, as so far missing, imaging studies such as structural and functional MRIs, PET scans, and electroencephalography analysis are clearly necessary to be conducted in dementia patients subjected to yoga and/or meditation interventions in order to study the direct effects of these practices on structure and function in AD brains.
Importantly, changes in nerve growth factors, serotonin, or Aβ levels due to yogic practices that are detected in blood samples must be interpreted with caution, as they do not necessarily reflect cerebral levels. Therefore, future studies should consider measurements of these markers in the CSF of AD patients to have a better understanding of how yoga interventions affect the brain.
Altogether, as yoga and meditation are both inexpensive and non-invasive, they should be considered as a complementary and alternative treatment option in Latin American countries.
Footnotes
ACKNOWLEDGMENTS
We acknowledge the technical assistance given by Dr. Beatriz Aguilar, as well as M.C. Ana Maria Escalante and Francisco Pérez at the IT Unit. Authors are thankful with Dr. Rammohan Rao and Dr. Dale Bredesen for their critical reading of the manuscript. We appreciate the editing support to improve the figure given by Camila del Rio-Castro (![]() ). SCO research work was supported by grants CONACyT FC921, UNAM-PAPIIT IN206518 and a grant from the Secretaria de Educación, Ciencia, Tecnología e Innovación de la Ciudad de México (RECITES INGER-DI-CRECITES-008-2018) “Red Colaborativa de Investigación Traslacional para el Envejecimiento Saludable de la Ciudad de México (RECITES)”. MH is a Feodor Lynen Fellow, awarded by the Alexander von Humboldt Foundation. JSLN received a grant from the Secretaría de Educación Pública (PROMEP- 511-6/2019-8848).
). SCO research work was supported by grants CONACyT FC921, UNAM-PAPIIT IN206518 and a grant from the Secretaria de Educación, Ciencia, Tecnología e Innovación de la Ciudad de México (RECITES INGER-DI-CRECITES-008-2018) “Red Colaborativa de Investigación Traslacional para el Envejecimiento Saludable de la Ciudad de México (RECITES)”. MH is a Feodor Lynen Fellow, awarded by the Alexander von Humboldt Foundation. JSLN received a grant from the Secretaría de Educación Pública (PROMEP- 511-6/2019-8848).