
Abstract
Background:
Hispanics/Latinos in the United States are more likely to live in neighborhoods with greater exposure to air pollution and are projected to have the largest increase in dementia among race/ethnic minority groups.
Objective:
We examined the associations of air pollution with performance on cognitive function tests in Hispanic/Latino adults.
Methods:
We used data from the San Diego site of the Hispanic Community Health Study/Study of Latinos, an ongoing cohort of Hispanics/Latinos. This analysis focused on individuals ≥45 years of age who completed a neurocognitive battery examining overall mental status, verbal learning, memory, verbal fluency, and executive function (n = 2,089). Air pollution (PM2.5 and O3) before study baseline was assigned to participants’ zip code. Logistic and linear regression were used to estimate the associations of air pollution on overall mental status and domain-specific standardized test scores. Models accounted for complex survey design, demographic, and socioeconomic characteristics.
Results:
We found that for every 10μg/m3 increase in PM2.5, verbal fluency worsened (β: –0.21 [95%CI: –0.68, 0.25]). For every 10 ppb increase in O3, verbal fluency and executive function worsened (β: –0.19 [95%CI: –0.34, –0.03]; β: –0.01 [95%CI: –0.01, 0.09], respectively). We did not identify any detrimental effect of pollutants on other domains.
Conclusion:
Although we found suggestions that air pollution may impact verbal fluency and executive function, we observed no consistent or precise evidence to suggest an adverse impact of air pollution on cognitive level among this cohort of Hispanic/Latino adults.
Keywords
INTRODUCTION
As average life-expectancy increases in the United States (U.S.) and worldwide, there is a heightened public health concern about impaired cognitive function with advancing age. Previous literature indicates that race/ethnic minorities are at higher risk for age-related cognitive dysfunction compared to non-Hispanic Whites [1, 2]. The Hispanic/Latino population has been projected to have the largest increase in Alzheimer’s disease and related dementias (ADRD) among other race/ethnic minority groups over the next four decades [2]. Cognitive impairment frequently precedes dementia. Thus, improved understanding of cognitive impairment and its determinants can reveal important insights into dementia prevention. Furthermore, understanding these determinants in Hispanic/Latino populations can inform targeted intervention strategies. In this study, we evaluate air pollution as a potential determinant of cognitive function.
Identifying ubiquitous and modifiable risk factors, such as ambient air pollution, is of key interest because they are highly prevalent, affect all populations, and can have multiple benefits if effectively intervened upon [3, 4]. Ambient air pollution is a mixture of particulate matter and gaseous pollutants. Emerging evidence suggests that increased exposure to air pollution is associated with cognitive impairment and dementia among older adults [5, 6]. Air pollutants including fine particulate matter (PM2.5) and ozone (O3) can impact the brain through both direct and indirect pathways [7]. First, pollutants can directly reach the brain through the nasal pathway or through systemic circulation by crossing the blood-brain barrier and trigger neuroinflammation [7–9]. Secondly, pollutants can produce inflammation in other organs and tissues (e.g., cardiovascular systems) that can indirectly affect the central nervous system [7, 10].
Unlike previous studies in the U.S. that have been conducted in predominantly white populations [11–16], this study investigates the association between air pollution and cognitive function in a U.S. Hispanic/Latino population. Examining this relationship in diverse race/ethnic populations, specifically in Hispanics/Latinos, is crucial given the expected relative increase in ADRD prevalence over the next 40 years [2]. Furthermore, there is a strong race/ethnic disparity in neighborhood environments [17]. In California, Hispanics/Latinos and Blacks are more likely to live in socioeconomically segregated communities that are disproportionally exposed to higher levels of ambient air pollution than White, Asian/Pacific Islander, and Native American populations [18]. These disparities highlight the need to examine the effect of air pollution on cognitive function among race/ethnic groups to inform the need to promote more equitable access to healthier neighborhoods. Currently, there is limited information available on the effect of air pollution on cognitive function among Hispanics/Latinos, the largest ethnic group in California [14, 18]. Thus, we aimed to examine associations between long-term exposure to air pollution and cognitive function in the San Diego metropolitan area using data from a representative cohort of community-dwelling Hispanic/Latino adults.
METHODS
Description of study participants
This study used data from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), an ongoing, prospective cohort study of 16,415 community-dwelling Hispanic/Latino adults from four U.S. sites: Bronx, New York; Chicago, Illinois; Miami-Dade, Florida; and San Diego, California. Details of this study have been previously published [19]. Briefly, adult participants aged 18–74 years were recruited for the study, with a two-stage probability sampling of households. Participants attended a clinic visit in 2008–2011 which included a clinical examination and questionnaire about demographic background and health conditions. Middle- and older-aged adults aged 45 years and older further underwent neurocognitive testing using a battery of five tests (see details below). The present study focuses on individuals who completed neurocognitive testing and reside in the San Diego field center catchment area. This analysis includes middle-aged adults to capture any early indication of dementia. The study population is predominantly Mexican heritage (immigrants, second and third generations). Out of 4,086 participants in the San Diego site, n = 1,658 were younger than 45 and were excluded from the analyses. An additional n = 339 participants were excluded for missing data. The final study included 2,089 participants. Differences in age, sex, Mexican heritage, and education level between those included and excluded in the study are presented in Supplementary Table 1. This study received approval from the Institutional Review Board of the participating study site.
Cognitive function
The primary outcome for this study was cognitive score, measured by performance on a neurocognitive battery of five tests at a single time point. Examinations were administered at the clinic visit by bilingual study staff trained and supervised by doctorate-level, licensed, clinical psychologists. Study participants were offered exams in either English or Spanish according to their language preference. The battery examined domains associated with aging and included a screener for overall mental status and tests of episodic verbal learning, memory, verbal fluency, and executive function.
Detailed information about the test battery and their application within HCHS/SOL has been previously published [20]. Briefly, the test included the Six-Item-Screener (SIS), Brief-Spanish English Verbal Learning Test (B-SEVLT Sum and Recall), Word Fluency (WF), and Digit Symbol Substitution test (DSST). The SIS is a mental status test derived from the Mini-Mental State Examination that includes three-item recall and three-item temporal orientation probes [21, 22]. Scores range from 1 to 6, with higher scores indicating better performance. The measure of overall mental status was dichotomized in line with previous work in this cohort, with normal mental status defined as SIS > 4 [20]. The B-SEVLT is an episodic learning and memory test. Participants were presented with and asked to recall a list of 15 common words immediately (B-SEVLT Sum) and after an interference task and short delay (B-SEVLT Recall). The total score for each is the number of correctly recalled words across three trials [23]. WF is a phonemic verbal fluency test. Participants were asked to recite as many words beginning with the letters “F” and “A” within 60 s. The total score is the number of correctly generated words during this time span [20]. The DSST is a mental processing speed and executive function measure. Participants were asked to encode symbols to numbers. The total score is the number of correctly coded symbols [24]. Domain-specific test scores were transformed into z-scores using the means and standard deviations of the measures in the study population, to allow comparability of results across the different tests.
Air pollution measurement
The air pollutants PM2.5 (μg/m3) and O3 (ppb) were the primary exposures for this study- specifically, a four-year average of daily estimates at the zip-code level. Neighborhood exposure to PM2.5 and O3 was estimated using 24-hour daily means and 8-hour daily maximums, respectively, sampled and analyzed by the U.S. Environmental Protection Agency Air Quality System. Measured concentrations within a 20 km radius of each population-weighted centroid were used for interpolation [25]. Values were estimated using an inverse distance weighting each point of interest; this gives greater importance to values reported by monitoring stations closer to the point of interest than monitoring stations farther away in distance [26, 27]. We assumed participants resided in the same zip code and estimated long-term exposure with a running average of daily estimates the four years before study entry. ArcMap10.3 was used to generate air pollution estimates.
Covariates
Demographic and socioeconomic characteristics were obtained from questionnaires administered at the clinic visit. The following covariates were considered in this analysis: Hispanic/Latino heritage (Mexican versus not), age, sex (male or female), educational attainment (less than 12 years, 12 years or equivalent, or greater than 12 years) and household income (less than $20 k, $20 k–$40 k, or more than $40 k).
Statistical analysis
The study population was described with means (SD) and frequencies (%) of demographic characteristics. All analyses were conducted for each pollutant, evaluating exposures as both continuous (per 10μg/m3 and 10 ppb for PM2.5 and O3, respectively) and categorical variables (cut points at the 5th, 25th, 50th, 75th, and 95th percentiles) to explore potential non-linear dose-responses. The primary outcome of interest was cognitive score measured at a single timepoint. Since scores were transformed, results reflect a change in outcome relative to a standard deviation increase. We used logistic regression models for survey data to estimate the effect of air pollution on normal mental status function (SIS >4). Linear regression models for survey data were generated to estimate the effect of air pollution exposure on performance on each domain-specific test. We assumed ordinary least squares (OLS) model assumptions for linear regression models and checked these by evaluating the homoscedasticity and distribution of error terms.
For all tests, higher scores reflect better performance. Models were adjusted for Hispanic/Latino heritage, age, sex, education, and income; this is a minimal set of variables, decided a priori, that may confound the relationship between air pollution and cognitive function. In sensitivity analyses, we stratified the domain-specific models by age group (<55 years and ≥55 years). All descriptive and regression models accounted for the complex sampling design of the HCSC/SOL, to improve generalizability to the target population. Survey weights were calibrated to 2010 US census characteristics by age, sex, and Hispanic/Latino heritage for each study site to account for nonresponse, oversampling of subpopulations, and spatial structure of participants. All analyses were executed using the survey function in Stata v. 16.
RESULTS
The mean age of the target population was 55.3 (SD: 9.5) years. Approximately 55%of the population were female and 70%reported an annual household income of less than $40,000 (Table 1). The majority of study participants (82%) completed exams in Spanish; demographic characteristics stratified by language preference are presented in Supplementary Table 2. The mean exposure concentration was 12.0μg/m3 (SD: 1.3, range: 10.2 to 13.3) and 50.1 ppb (SD: 4.1, range 39.4 to 52.6) for PM2.5 and O3, respectively.
Characteristics of study population (unweighted n = 2,089)
Approximately 90%of the study population were classified as normal cognitive function (n = 1,859). On average, individuals had raw scores of SIS: 5.4 (SD: 0.03, range: 0 to 6), B-SEVLT Sum: 23.7 (SD: 0.2, range 3 to 40), B-SEVLT Recall: 8.9 (SD: 0.1, range: 0 to 15), WF: 20.8 (SD: 0.4, range: 1 to 45), and DSST: 39.3 (SD: 0.6, range: 0 to 81).
In regression analyses, increased exposure to PM2.5 and O3 was associated with lower odds of normal mental status (SIS >4). For domain-specific measures, OLS model assumptions were met. Standardized performance on cognitive function exams was marginally worse for WF (β: –0.21 SD; 95%CI: –0.68, 0.25) but slightly better for B-SEVLT-Sum (β= 0.89 SD; 95%CI: 0.42, 1.35), SEVLT-Recall (β= 0.67 SD; 95%CI: 0.20, 1.13), and DSST (β= 0.13 SD; 95%CI: –0.33, 0.60) for every 10μg/m3 increase in PM2.5. For every 10 ppb increase in O3, we observed worse performance for WF (β= –0.19 SD; 95%CI: –0.34, –0.03) and DSST (β= –0.01 SD; 95%CI: –0.12, 0.09) and slightly better performance in standardized cognitive function scores for B-SEVLT Sum (β= 0.12 SD; 95%CI: –0.01, 0.25), and SEVLT Recall (β= 0.15 SD; 95%CI: 0.02, 0.29) (Table 2).
Associations between air pollution and cognitive performance
*Models adjusted for age, sex, heritage, marital status, education, and income PM2.5 (per 10μg/m3); O3 (per 10 ppb); SIS, Six-Item-Screener; B-SEVLT, Brief Spanish English Verbal Learning Test; WF, Word Fluency; DSST, Digit Symbol Substitution Test. Higher scores indicate better performance for all tests.
For PM2.5, we observed some indication of worsening performance on DSST for PM2.5 concentrations greater than the 50th percentile. We found no consistent pattern of worse cognitive performance with increasing exposure levels for either B-SEVLT test, WF, or overall mental status (Fig. 1, Supplementary Table 6). Similarly, we observed decreasing performance on DSST for higher O3 exposure groups and no pattern of worse cognitive performance with higher exposure levels for B-SEVLT exams, WF, or overall mental status (Fig. 1, Supplementary Table 7). In analyses stratified by age group, we found suggestions of a stronger effect of air pollution on worse performance on WF and DSST for PM2.5, and WF for O3 in the older age group (Supplementary Table 8).
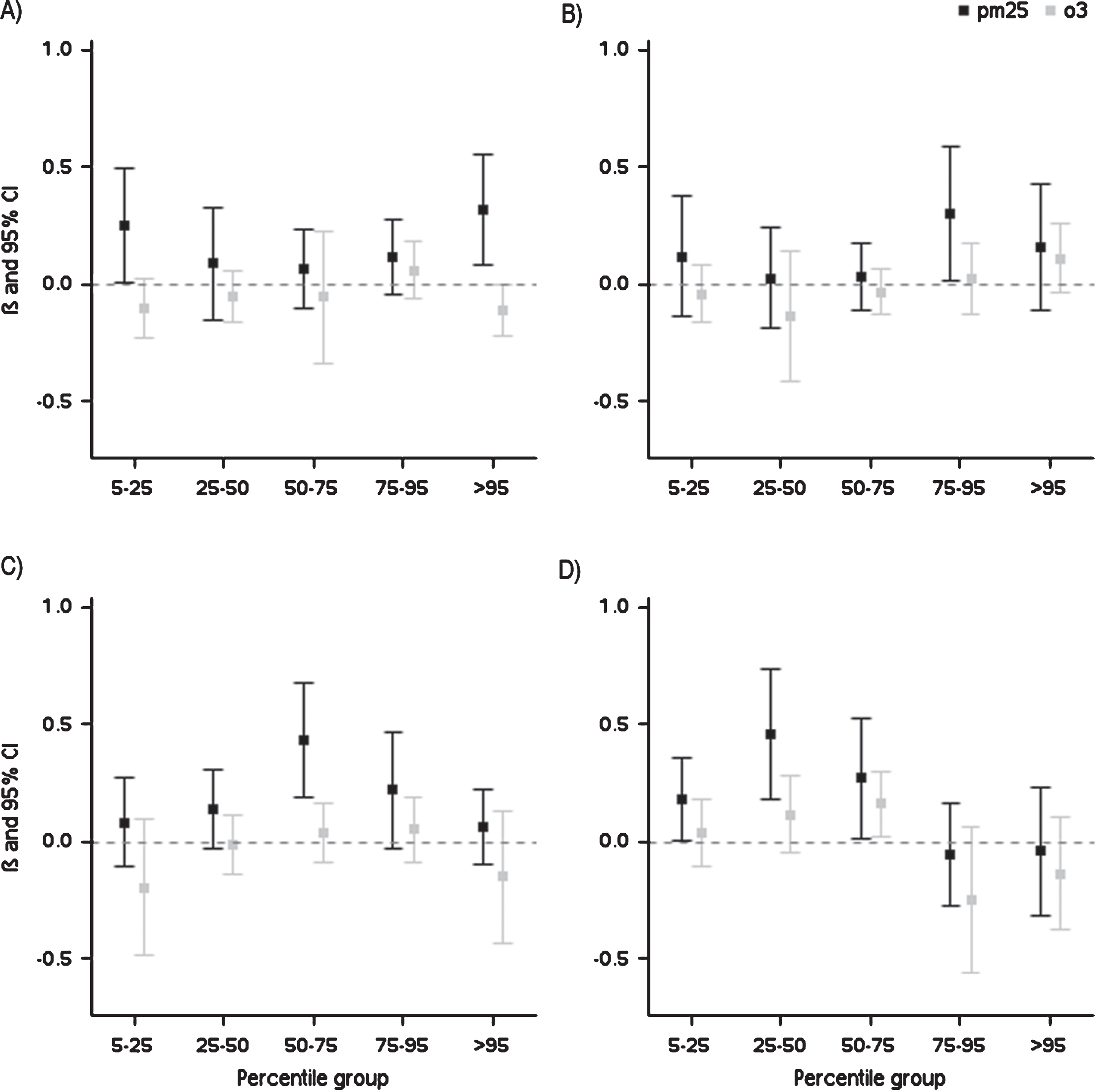
Domain-specific associations between standardized scores of cognitive function and air pollution percentile groups. Lowest exposure group (<5th percentile) is reference. A) Brief Spanish English Verbal Learning Test (B-SEVLT) - Sum; B) B-SEVLT-Recall; C) Word Fluency; D) Digit Symbol Substitution Test. Higher scores indicate better performance for all tests.
DISCUSSION
This study examined the effect of exposure to PM2.5 and O3 on performance in several domains of cognitive function in a cohort of middle- and older-aged Hispanic/Latino adults in San Diego, California. We observed that increased exposure to air pollutants was marginally associated with lower mental status, poorer verbal fluency and worse executive function; however, these results were not precise. We did not identify any detrimental influence of PM2.5 and O3 exposure on measures of learning or memory included in this study. Overall, we did not find consistent or robust evidence for a role air pollution exposure in worse cognitive function across the considered domains in this cohort of Hispanic/Latino adults.
In contrast with the present findings, previous studies have observed a link between particulate matter and worse verbal learning [14], abstraction [29], working memory [11, 28], and orientation [11]. Previous studies have also found exposure to ozone may be associated with reduced performance in neurocognitive tests of short-term memory, attention, and perceptual function, and executive function [13, 14]. Although it is biologically plausible that air pollution can produce a neuroinflammatory response resulting in structural brain changes [30, 31], findings in the present study were imprecise as indicated by wide confidence intervals. This may be explained by the relatively young age of our cohort (mean age is 55.26 years), the selection of our participants, and the limited variability of air pollution exposure in our study population.
Potential explanations for our findings first include the study population which was comprised of middle- and older-aged adults to potentially capture the prodromal stages of cognitive decline that develops at earlier ages. This selection of middle-aged adults may attenuate the effect of air pollution on cognitive function because notable influences on cognitive function may not be observed until later in life. We found suggestions of a stronger effect among the older age group and we recommend future cohorts of Hispanics/Latinos that include a wider age range of older adults to replicate this work.
Second, it is possible that Hispanic/Latinos have higher cognitive resilience and are less vulnerable to the effects of air pollution on cognitive function. This resilience is observed in a recent study of air pollution and cognitive decline in New York, where less decline in global cognitive function was observed among Hispanics compared to non-Hispanic White and Black participants, across PM2.5 and other pollutants [32].
Third, our study area focused on a relatively small geographic area within San Diego county. Despite applying survey weights to obtain a representative sample of the target population, we may not have had enough exposure heterogeneity to detect substantive effects. In this study population, exposure to fine particulate matter and ozone ranged from 10 to 13μg/m3 and 39 to 53 ppb, respectively. In contrast, a cohort study in Los Angeles, California of the same pollutants had exposures ranging from approximately 6 to 29 μg/m3 and 21 to 59 ppb [14]. We suggest future studies explore diverse geographical areas in order to capture various levels of air pollution exposure.
We acknowledge limitations in our study. Our participants were assigned individual exposure to pollutants based on residential zip code reported at study baseline. These measurements do not account for residential movement and each zip code is assigned a uniform concentration. Furthermore, we assumed that exposure is fully experienced at the residential zip code. Exposure misclassification may also arise due to seasonal and traffic characteristics that are not accounted for in our air pollution estimates. While we acknowledge some misclassification due to residential movement varying time spent at home, and modeling method, we expect this misclassification to be unrelated to cognitive performance. Any bias due to this misclassification would underestimate estimates.
In addition, we examined cognitive function measured at one time-point. This is susceptible to unmeasured confounding due to socioeconomic and sociocultural characteristics that affect both neighborhood residence and performance on exam. We recommend longitudinal studies of cognitive decline to examine within-person changes in cognitive function to overcome this challenge.
In this study, we examined the effect of long-term exposure to air pollution on cognitive function in a well-characterized cohort of Hispanic/Latino adults in San Diego. We did not find consistent evidence of an association between increased exposure to PM2.5 and O3 and worse performance on cognitive function exams. Further work among ethnically diverse older study populations and with repeated measures of cognitive function are important to confirm or challenge these findings.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Alzheimer’s Disease Resource Center for advancing Minority Aging Research at the University of California San Diego (P30AG059299 National Institute on Aging) and by the grant 1R01CA228147. PMV was supported by P30AG059299 and 5T32HL079891-13.