
Abstract
Background:
Dementia has become a public health priority as the number of cases continues to grow worldwide.
Objective:
To assess dementia incidence and determinants in the EPIC-Spain Dementia Cohort.
Methods:
25,015 participants (57% women) were recruited from three Spanish regions between 1992-1996 and followed-up for over 20 years. Incident cases were ascertained through individual revision of medical records of potential cases. Crude and age-adjusted incidence rates (IR) of dementia and sub-types (Alzheimer’s disease (AD), and non-AD) were calculated by sex. Neelson-Aalen cumulative incidence estimates at 10, 15, and 20 years were obtained for each sex and age group. Multivariate Royston-Parmar models were used to assess independent determinants.
Results:
Global IR were higher in women for dementia and AD, and similar by sex for non-AD. IR ranged from 0.09 cases of dementia (95% confidence interval: 0.06–0.13) and 0.05 (0.03–0.09) of AD per 1000 person-years (py) in participants below 60 years, to 23.2 (15.9–33.8) cases of dementia and 14.6 (9.1–33.5) of AD (per 1000 py) in those ≥85 years. Adjusted IR were consistently higher in women than men for overall dementia and AD. Up to 12.5% of women and 9.1% of men 60–65 years-old developed dementia within 20 years. Low education, diabetes, and hyperlipidemia were the main independent predictors of dementia risk, whereas alcohol showed an inverse association.
Conclusion:
Dementia incidence increased with age and was higher among women, but showed no geographical pattern. Dementia risk was higher among subjects with lower education, not drinking alcohol, and presenting cardiovascular risk factors.
INTRODUCTION
Dementia is a broad term that encompasses several mental disorders caused by brain disease or injury affecting memory, cognitive function, and behavioral and personality traits [1]. The most frequent type of dementia is Alzheimer’s disease (AD), which accounts for 60–70% of the overall cases [1]. Dementia is an age-related syndrome but it is not part of the normal aging process, and since there is no effective treatment to slow down its progression or ameliorate its symptoms [2], prevention remains as the most efficient strategy to reduce the burden of the disease. Several modifiable factors have been identified, such as education and cardiovascular risk factors [3], which seem to be related to the etiopathogenesis of AD and other dementia sub-types and are amenable to intervention.
The World Health Organization has recognized dementia as a public health priority, raising awareness of the dimension of the disease as a leading cause of death and disability and calling for larger research and innovation efforts. Near 50 million patients were estimated to have dementia in 2015 (overall prevalence in Europe is 7.1%) [4], but as the world population is steadily rising and aging, this figure is foreseen to more than double by 2050 [1]. Still, data on the incidence of dementia may not be accurate worldwide, as local (national or regional) estimates are lacking in many parts of the world. In Spain, there are no nationally-representative estimates on dementia incidence and the studies available show variability in their results, with overall incidence rates ranging from 7.6 to 13.1 per 1000 person-years (py) at 75–80 years, and from 12.6 to 25.4 per 1000 py in the 80–85 years-old group [5–7]. Literature on temporal trends is also heterogeneous, although some studies suggest a decline or stabilization of dementia incidence [8, 9].
In the absence of population-based dementia registries, cohort studies can be used to estimate the incidence of dementia. Although most cohorts have not been designed to be representative of the general population (which limits their external validity), when large enough they can be conveniently used to provide study-specific incidence estimates by population sub-groups, providing insightful data on incidence patterns and filling gaps in epidemiological knowledge of the disease. In addition, cohort studies are best suited for quantifying the magnitude of the association of potential risk factors, making possible to assess the dimension of the disease and to characterize their socio-demographic, lifestyle, and clinical correlates in a common study setting [10]. EPIC (European Prospective Investigation into Cancer and Nutrition)-Spain is a multi-center cohort study with a large sample size, long follow-up time, and geographical variability, which provides a convenient framework for obtaining incidence estimates of dementia and related factors. The purpose of this study was to assess the risk of dementia in the EPIC-Spain Dementia Cohort by sub-type, age group, and sex, and to assess how this risk varies according to selected variables.
METHODS
Sample and study design
The EPIC study is a large multi-center prospective cohort study with over 520,000 participants from 10 European countries, designed to study the association of dietary and sociodemographic factors with the incidence of cancer and other chronic diseases [11]. EPIC-Spain consisted of 41,437 volunteers (blood donors, employees from private companies, civil servants, and the general population), recruited between 1992-1996. Participants had to be physically and mentally able to take part in the study, to be between 30 and 70 years old, and not to be pregnant. The sample covered a wide range of socio-economic and educational levels, and all participants were fully covered by the public health system. A detailed description of the methodology is available elsewhere [12, 13]. The EPIC-Spain Dementia Cohort study comprises the three EPIC-Spain centers with available data on incident dementia: Gipuzkoa, Navarra, and Murcia. The study sample consisted of 25,015 participants (57% women), aged 30–70 years at recruitment.
The EPIC study protocol was approved by the IARC (International Agency for Research of Cancer) Ethics Committee, and all the participants gave written informed consent. The consent form included the express authorization of the participants to update their clinical information from available medical records in the future for research purposes within the EPIC study. The current research has been conducted in accordance with the principles of the Declaration of Helsinki and the paper was written according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (https://www.equator-network.org/reporting-guidelines/strobe).
Ascertainment of dementia cases
Although participants in the EPIC study did not undergo a baseline cognitive assessment, all volunteers were required to be mentally and physically able to participate and to complete extensive questionnaires which were demanding enough as to guarantee a normal cognition (including a dietary history interview which took 50–60 min on average). In order to ascertain incident cases of dementia in the cohort, a validation protocol was implemented, where dementia diagnosis (and sub-type) was established based on medical records. The protocol has been described in detail previously [14]. Potential cases were identified by record linkage between of each center database (Murcia, Gipuzkoa, and Navarra) and all health databases that could contain dementia-related clinical information: primary care registries, hospital discharge databases (Minimum Dataset), and regional and national mortality registries, using dementia-related codes of the International Classification of Diseases and Related Health Problems 9th and 10th editions (ICD-9 codes: 290, 331; ICD-10 codes: F00-F03, G30), International Classification of Primary Care (ICPC2 codes: P20, P70, N29, N99) and the Anatomical Therapeutic Chemical classification system (ATC codes: N06DA02 (Donepezil), N06DA03 (Rivastigmine), N06DDA04 (Galantamine), N06DX01 (Memantine)). In a second step, a validation procedure was carried out by an expert panel of neurologists through careful revision of all the available medical records of every potential case (either electronic data or paper medical records), including different sources of evidence: outpatient and hospital medical reports (admission, discharge, and emergency reports), drug prescriptions, diagnostic tests, and information of the previously selected codes recorded in health databases. The expert panel then judged whether the available data sufficed to establish the diagnosis of dementia. The decision-making process was guided by an ad hoc algorithm revised by the panel of neurologists participating in the study. Potential cases were validated as incident cases of dementia if a clinical diagnosis of dementia appeared in a medical report; alternatively, if no medical reports were available, dementia was established when any of the following codes appeared in the medical records: P70 and/or antidementia drug prescription, and/or ICD 9-10 codes. The subtype of dementia was specified when sufficiently detailed clinical information about the subtype was available in medical reports. If no detailed information or if only codes were available, the subtype was left unspecified.
Participants were followed up from recruitment until the date of diagnosis, death, loss to follow-up, or the last complete vital status check (December 31, 2017 for Gipukzoa, December 31, 2015 for Navarra, and November 30, 2016 for Murcia), whichever occurred first. Incidence date was defined as the date of the first neurological report where the diagnosis of dementia was recorded or, if only codes were available, the earliest date the code was recorded or the date of death when no other information was available (n = 2 participants).
Assessment of other study variables
Baseline questionnaires gathered data on socio-demographic and lifestyle variables at the recruitment, including educational level (less than primary, primary, technical school, secondary, university or higher), smoking habit (never, former, current), alcohol intake (g/day), and weekly recreational and household physical activity (dichotomized according to sex-specific medians). Data on self-reported diseases (diabetes, hypertension, hyperlipidemia, stroke, myocardial infarction, and cancer: yes, no, unknown) was also collected. Height, weight, and waist circumference were taken using standard methods, with subjects barefoot and in light clothing. Body mass index (BMI) was calculated as the ratio between weight (in kg) and square height (in m2).
Statistical analyses
Descriptive characteristics were evaluated separately for cases and non-cases including frequencies or means and standard deviations, as appropriate. Follow-up time was defined from age at entry in the study until age at diagnosis of dementia, death, or end of the study between December 31, 2015 and December 31, 2017 (depending on the study center), whichever occurred first.
Crude rates of dementia (and sub-types), were calculated by sex for participants 50 years old and over, by dividing the observed number of events by the total person-time at risk in each age group. Individual person-years for each participant were allocated to their corresponding 5-year age group throughout the entire study period to compute the overall person-time at risk in each stratum.
Age-adjusted incidence rates, standardized to the 2013 European Standard Population (ASRE) [15], and the 2000–2025 World Standard Population (ASRW) [16], were estimated using the direct method for participants ≥65 years, to allow for comparability with other studies, using the ‘dstdize’ STATA command. Additionally, point estimates of the cumulative incidence of dementia at 10, 15 and 20 years were obtained by sex for the 50–54.9, 55–59.9, and 60–64.9 age groups, using the non-parametric Neelson-Aalen estimator to calculate the proportion of participants with dementia at different time points. Furthermore, the estimated cumulative hazards of dementia by age were modelled separately for men and women using flexible parametric Royston-Parmar survival models [17]. These models differ from conventional Cox models in that they use restricted cubic splines to define the baseline hazard rate, which allow for a smooth representation of the hazard function and equally precise point estimates. Hazard ratios of dementia and sub-types were estimated using such Royston-Parmar multivariable models with age as the time scale and adjusted by center to assess the independent associations of selected variables (sex, educational level, smoking, alcohol intake, physical activity, BMI, waist circumference, diabetes, hypertension, hyperlipidemia, myocardial infarction, stroke, and cancer) with dementia risk. Follow-up time was defined from age at entry in the study until age at diagnosis of dementia, death, or end of the study between December 31, 2015 and December 31, 2017 (depending on the study center), whichever occurred first.
Statistical analyses were performed using STATA/SE v.14 (Stata Corp., College Station, TX, USA), and p-values <0.05 were considered significant.
RESULTS
After a mean of 21.5 years, a total of 537,198 py were available for analysis. Within this period, 774 dementia cases were ascertained, 518 of which were validated as AD, and 256 as non-AD dementia cases. The median follow-up time of cases was 18.3 years.
Baseline characteristics of the sample are shown in Table 1. Dementia cases were more likely to be women, obese, to have a primary educational level or lower, and to suffer chronic diseases such as diabetes, hypertension, or hyperlipidemia. On the contrary, they were less likely to be alcohol consumers. Table 2 shows the incidence rates of dementia by sex and age groups. As shown, incidence rates increased exponentially with age for overall dementia and subtypes, and AD was the first cause of dementia representing 66.9% of all cases. Global incidence rates were higher in women for dementia and AD, while lower for non-AD (versus men). Overall rates of dementia and AD in people aged 65 and above were 4.2 (95% CI: 3.9–4.5) and 2.8 (7.0–9.4) per 1000 py respectively, while adjusted rates (ASRE) were 8.2 (7.0–9.4) and 5.5 (4.5–6.4) per 1000 py. As illustrated in Fig. 2, the models showed their steepest increase from the age of 75 onwards. Age-adjusted incidence rates of dementia were lower in Gipuzkoa (ASRE 65+6.9 (5.6–8.2) per 1000 py) and higher in Navarra (10.6 (6.2–14.9) per 1000 py) (Table 3), but there was not a clear geographical trend in dementia incidence, and differences by center were not statistically significant in multivariate models. Table 4 presents the cumulative incidence of dementia and AD in women and men for quinquennial age groups in the 50-65 age band. Noteworthy, 10.1% of the participants aged 60–65-years developed dementia in the following 20 years, whereas 7.5% developed AD.
Baseline characteristics in dementia cases and non-cases participating in the EPIC-Spain Dementia Cohort (N = 25,015)
1One alcohol unit defined as the intake of 10 g of ethanol per day. 2Median physical activity values (MET-h/sem): men = 42, women = 126. 3Elevated waist circumference defined as a WC≥102 cm (men) or ≥88 cm (women).
Crude and age-adjusted incidence rates (IR) of dementia (with 95% confidence intervals) in 25,015 participants from the EPIC-Spain Dementia Cohort
IR, incidence rate per 1000 person-years. ASRE, age-adjusted incidence rate standardized to the 2013 European Standard Population; ASRW, age-adjusted incidence rate standardized to the WHO 2000-2025 World Standard Population.
Crude and age-adjusted incidence rates (IR) of dementia (with 95% confidence intervals) by study center, in 25,015 participants from the EPIC-Spain Dementia Cohort
IR, incidence rate per 1000 person-years. ASRE, age-adjusted incidence rate standardized to the 2013 European Standard Population; ASRW, age-adjusted incidence rate standardized to the WHO 2000-2025 World Standard Population.
Nelson-Aalen cumulative hazard estimates (with 95% confidence intervals) of dementia and Alzheimer at 10, 15 and 20 years from enrolment in 25,015 men and women from the EPIC-Spain Dementia Cohort
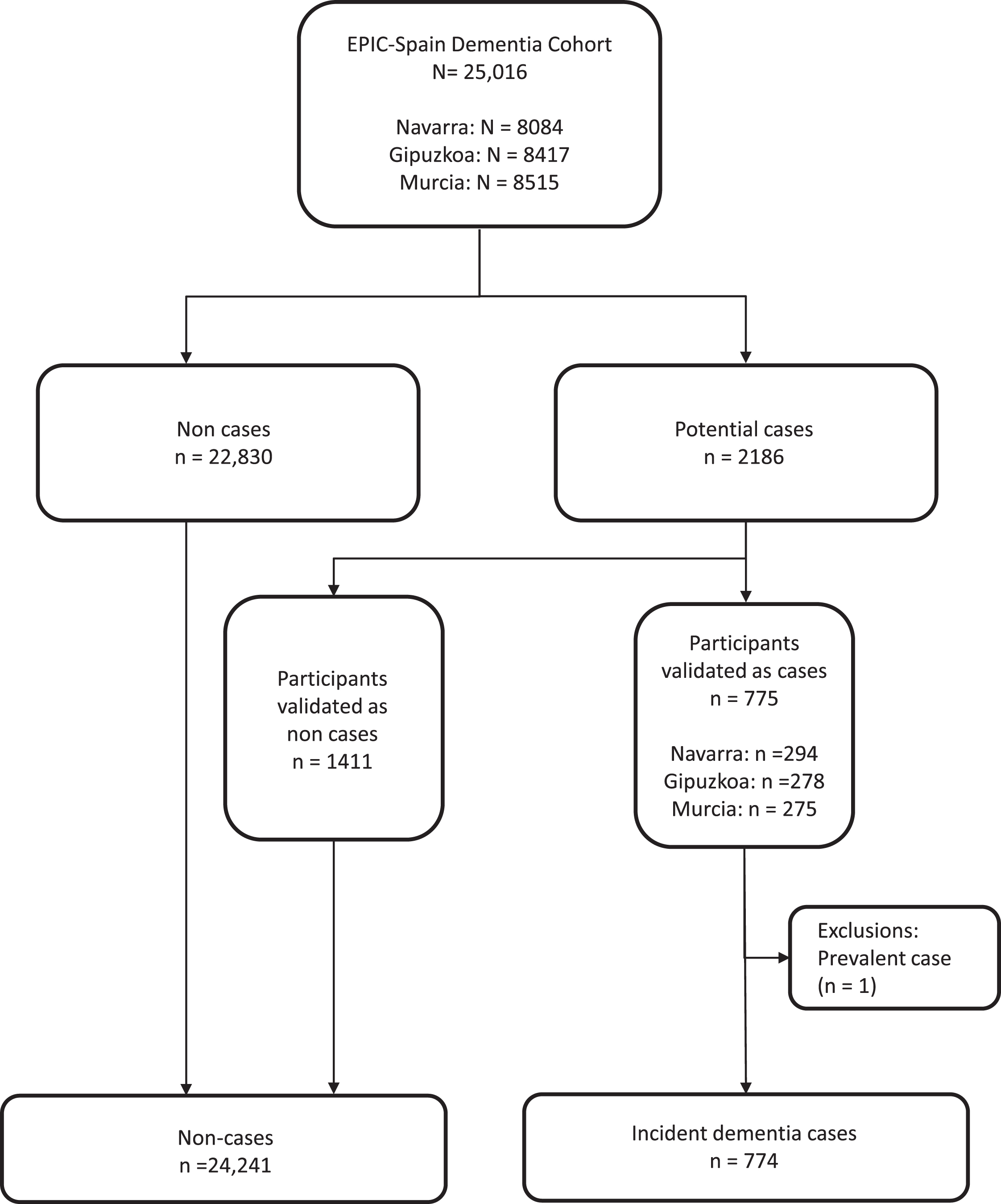
Flow-chart of the dementia case ascertainment process in the EPIC-Spain Dementia Cohort.
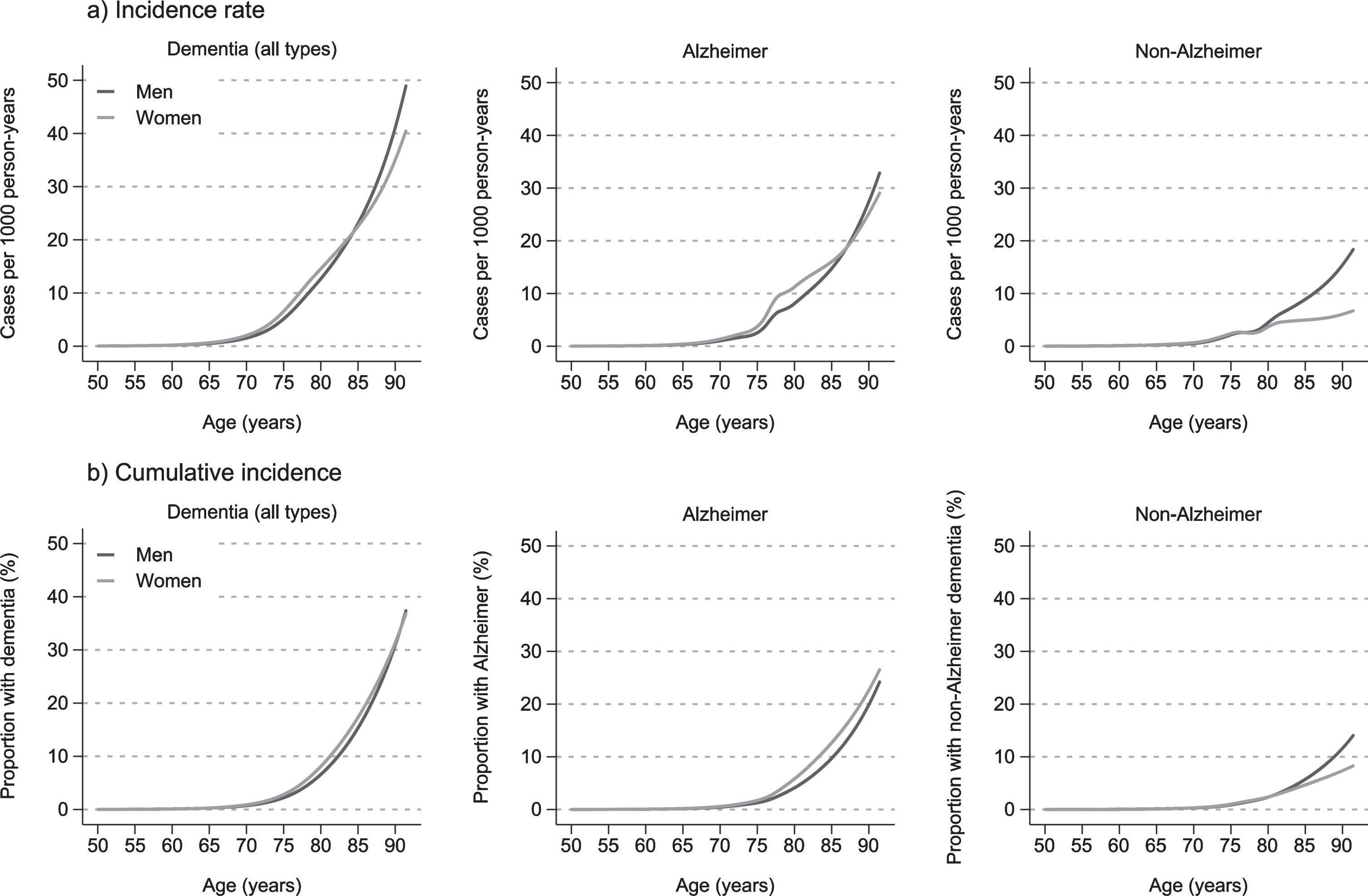
Royston-Parmar model-based incidence rates and cumulative incidence (incidence proportion) of dementia, Alzheimer’s disease, and non-Alzheimer’s dementia, by sex, in the EPIC-Spain Dementia cohort (N = 25,015). Estimates based on a restricted cubic spline parametrization of the baseline hazard function with 3 degrees of freedom.
The results of the multivariate analysis showed that educational level and diabetes were the strongest factors associated to dementia and its sub-types. Risk of overall dementia or dementia sub-types was 29–37% lower among participants with higher education as compared to those with primary studies, whereas HR among participants with diabetes mellitus (versus non-diabetics) was 1.38 (95% CI: 1.10–1.72) for dementia, and 1.86 (1.32–2.62) for the non-AD subtype. Furthermore, hyperlipidemia was also significantly associated to AD (HR = 1.11, 1.01–1.21). On the other hand, alcohol consumers showed a 19% lower risk of overall dementia risk (CI: 4% to 32%) (Table 5), whereas no significant associations were found for other lifestyle variables, cardiovascular risk factors, or chronic diseases (myocardial infarction, stroke, or cancer) in multivariate models.
Multivariate associations between selected variables and the hazard of dementia (overall and by subtypes) in 25,015 participants from the EPIC-Spain Dementia Cohort
Estimates are hazard ratios (HR) with 95% confidence intervals (CI) obtained with flexible parametric Royston-Parmar models using age as the time scale and including all variables presented in the table. 11 alcohol unit defined as the intake of 10 g of ethanol per day. 2Median physical activity values (MET-h/sem): men = 42, women = 126. 3Elevated waist circumference defined as a WC≥102 cm (men) or ≥88 cm (women). 4Insufficient number of cases.
DISCUSSION
The main contribution of this work is the estimation of incidence rates of dementia according to sub-type, age, and sex in a large Spanish cohort. Our study is the first to contribute data on dementia incidence in areas from the north (Gipuzkoa and Navarra) and the south of Spain (Murcia), and one of the few studies available in the Mediterranean region. The estimated overall age-adjusted incidence rate of dementia in the EPIC-Spain dementia cohort was 6.7 to 8.2 cases per 1000 py (depending on the population standard). By sex, rates were higher in women, especially in younger age groups, and became comparable above 80 years old. Together with previous data, these results suggest that incidence of dementia in Spain is moderate as compared to other studies [18].
It is of concern that despite the importance of dementia as a public health problem worldwide, the epidemiology of the disease is not fully characterized, even in developed countries. While recent research has focused on the evolution of dementia trends, point estimates of its incidence are scarce, with most of the available data dating back one or two decades ago [19]. Assessing the incidence of dementia in different geographical areas and population groups is important for establishing the magnitude of the disease burden and detecting temporal trends to inform effective prevention policies.
Several studies have enriched the knowledge on dementia incidence in the last decades, most of them carried out in North America (such as the Framingham study, the MoVIES Project, the Mayo Clinic Study of Aging, or the Rochester Epidemiology Project) [9, 20–22], or Europe (MRC-CFAS, PAQUID, Rotterdam, or Lundby Studies) [23–26]. Unfortunately, only a few cover Southern European countries such as Spain [5–7, 27–29], and not in a geographically comprehensive manner. Furthermore, comparisons of overall rates across studies are difficult since dementia is a condition heavily determined by age and differences in the age structure of different studies could have a large impact in epidemiological estimates such as incidence or prevalence. The only one prior study in Spain which reported age-adjusted incidence rates of dementia, estimated an ASR of 10.6 cases per 1000 py, which is slightly higher than our results [6]. The fact that they had a significant proportion of participants in the oldest age groups (85–89 and ≥90 years) could partially account for their higher incidence. We had a small number of person-years in the oldest age band (≥85 years), and we admit this may limit the accuracy of our estimates in this group. We cannot discard that the lower incidence observed in our cohort could also be partially attributable to differences in the prevalence of risk factors or to methodological heterogeneity across studies. Of note, the cohort size and length of follow-up in our cohort study were much larger than those reported for other studies in our geographical area. Besides, our multi-center study includes data from three geographically dispersed populations within the country, which strengthens their external validity. While we did not perform repeated cognitive assessments of the participants (impractical in large cohort settings), case ascertainment of dementia was based on the revision of all medical records available for each potential case, also reducing the outcome misclassification bias inherent to single cognitive assessment tools. Some studies, such as the Rochester Project [22], used a similar case ascertainment approach, yet the number of participants and length of follow-up were much lower. It its worth considering the possibility that rates of dementia incidence could have changed throughout the two decades of follow-up. Some authors have suggested that incidence of dementia would be decreasing in developed countries [9], and this could partially account for a lower incidence rate in our cohort, since incidence of dementia would be decreasing in parallel with the ageing of the cohort. While such a possibility cannot be discarded, a recent meta-analysis suggested that the potential reduction in dementia incidence would be, if any, of small magnitude and not statistically significant, mainly due to the high variability across studies [8].
The cumulative incidence of dementia at different ages and time spans is an important estimator for evaluating the burden of the disease and for health planning and resource allocation. However, few data have been published on this matter so far. Estimates on lifetime risk of dementia around 15–25% for people aged 65 years have been published in the Framingham [30] or Rotterdam [31] studies, and by Lobo et al. in Spain [5]. Together, results highlight the exponential burden of dementia up to advanced ages, even when estimates are usually based on model projections. The long follow-up in our study allowed us to use a different approach, i.e., to estimate the cumulative proportion of dementia and AD cases, by sex, observed at 10, 15, and 20 years. Observed results showed that 12.5% of women and 9.1% of men 60–65 years-old developed dementia within a 20-year time frame, which again points out to a lower burden of dementia in our country. Of note, while a larger proportion of women suffered dementia overall, men were more likely to be diagnosed with non-AD at older ages (Fig. 2).
Education and diabetes were the major modifiable factors associated with dementia risk in our study. A lower educational level was associated to an approximately 30–35% higher risk of dementia, AD or non-AD (p < 0.01). A higher educational attainment contributes to the cognitive reserve of the brain (i.e., its ability to cope with the age-related decline in neurological functions), which has been widely recognized to prevent the onset and severity of dementia [32]. Our results thus agree with previous evidence showing the major effect of education on dementia risk. Of note, this association was independent of cardiovascular risk factors, such as diabetes mellitus and hyperlipidemia, which are known determinants of dementia and likely play a major role in the etiopathogenesis of the disease [3]. While our results confirmed the independent associations for these factors, other well-known determinants of the disease, such as obesity or hypertension [33] were not found to be independently associated with dementia or its sub-types in our cohort. While there was a larger proportion of hypertensive or obese participants among the cases, these associations were largely attenuated (and no longer significant) in multivariate models. Literature results on the association of BMI and dementia are conflicting [34, 35]. Previous evidence suggests that obesity in mid-life may increase the risk of dementia through increased production of inflammatory cytokines and hormones by the adipose tissue, whereas a higher BMI seems to be inversely associated to dementia risk when measured in late-life [35]. Furthermore, obesity is an upstream risk factor predisposing to diabetes, dyslipidemia, hypertension, and cardiovascular disease [36]. The weakening of statistical significance in the association of obesity in multivariate models accounting for other mediating cardiovascular risk factors would thus be an expected finding. On the contrary, the lack of a significant association for hypertension contrasts with most previous literature and needs to be considered with caution. Elevated blood pressure is recognized as a leading cause of neurovascular dysfunction, affecting cerebrovascular structure and ultimately impairing cognition [37]. The fact that the condition was self-reported (which implies some extent of misclassification) and the inability to account for the degree of pharmacological control or severity of the disease might partially explain our null results. Finally, we found alcohol consumption to be protective against dementia, as consumers had an estimated 18% lower risk than non-consumers in adjusted models. This result persisted after defining ‘never consumers’ as the reference group to avoid the sick-quitter bias. Although such an effect has been pointed out in previous works [6], we suggest caution in the interpretation of this finding, which warrants further analysis.
A number of strengths and limitations needs to be considered. Our results come from the largest cohort in Spain, and cover geographical areas in which only prevalence data on dementia had been available to date [38], thus helping filling the gaps in the epidemiology of the disease in Southern Europe. Major strengths of the study are the large sample size and number of cases, a long follow-up, geographical variability, and the ability to study socio-demographic, lifestyle, and clinical factors.
The main limitation of our study was the lack of a baseline cognitive assessment of participants. As the study EPIC was not initially designed for the study of dementia as a primary outcome, participants did not undergo a cognitive evaluation at baseline or during follow-up, so the diagnosis was based solely on clinical records and we could not fully discard baseline conditions related to cognitive decline, such as mild cognitive impairment (MCI). However, the mean age of the cohort was 49.3 (±7.8) years at baseline, and only 142 participants (0.57%) were between 65–69 years, in whom prevalence of MCI in our area was estimated below 9.7%, whereas prevalence of dementia was below 0.3% [38]. Furthermore, most of the cases were diagnosed after a long follow-up time: the median follow-up time of cases was 18.3 years, whereas less than 6.6% of the cases were diagnosed within the first 10 years. Finally, our results do not suggest an over-estimation of dementia incidence, as it have been the case if a significant proportion of MCI or dementia cases had been included at baseline. For the above-mentioned reasons, we consider that the lack of a baseline cognitive assessment, despite a limitation, did not have a significant impact in our estimates. As another limitation, a selection bias was implicit since we could only ascertain those cases that accessed the health system, and this might have resulted in an underestimation of dementia rates in our population, particularly in older participants with cognitive decline who may have not sought for a medical diagnosis. Nevertheless, the fact that healthcare in Spain is universal and free would have reduced the extent of such a bias (less than 1% of the Spanish population have private health coverage exclusively). Also, the scarcity or participants in the oldest age band limits the accuracy of incidence estimates in this group. Another limitation is that data on lifestyles and co-morbid conditions were only evaluated at baseline, and so we were unable to assess changes in these variables throughout study time. Also, a potential left-truncation bias due to death or emigration before enrollment could not be discarded. Furthermore, as in any observational study, residual or unmeasured confounding cannot be ruled out. Finally, the lack of representativeness of the cohort would limit the generalizability of our results.
Conclusions
In conclusion, incidence rates of dementia in the EPIC-Spain-Dementia study were lower than previously reported in other Mediterranean or North-American studies, and similar to previous estimates in Spain and Northern Europe. Up to 9% of men and 12.5% of women aged 60–65 years at enrollment suffered dementia after 20 years, whereas major modifiable factors associated with dementia were low educational level, diabetes, and hyperlipidemia. On the other hand, alcohol consumption showed an inverse association with dementia overall.
Footnotes
ACKNOWLEDGMENTS
We are grateful to Jone Alkorta for her assistance during the case validation phase of the study. We also thank all EPIC-Spain participants for their contribution to the study. The EPIC study received financial support from the International Agency for Research on Cancer (AEP/93/06), the European Commission (SO-97-200302-05F02, SP23-CT-2005-006438), the Health Research Fund (FIS) of the Spanish Ministry of Health, the Red Temática de Investigación Cooperativa de Centros de Cáncer (RTICCC C03/10, RD06/0020), the CIBER de Epidemiología y Salud Pública (CIBERESP), the participating Regional Governments of Andalusia, Asturias, Basque Country, Murcia (no. 6236), and Navarra, and the Catalan Institute of Oncology (ICO). The EPIC-Murcia study received partial funding from the Fundación Séneca (19487/PI/14), the Murcia Biomedical Research Institute (IMIB)-FFIS and the Spanish Biomedical Research Network Center (CIBER) (BOE-A-2020-6018).