
Abstract
Background:
Participation in exercise may be useful for dementia prevention; however, the specific exercise types which may best to reduce the risk of developing cognitive decline have remained unidentified in the literature.
Objective:
To examine the relationships of specific exercise types with the risk of developing cognitive decline in older women.
Methods:
This 1- to 2-year population-based cohort study included 687 community-dwelling older Japanese women without disability, neurological disease, dementia, or cognitive impairment assessed as <24 points on the Mini-Mental State Examination (MMSE) at the baseline survey. Developing cognitive decline was defined as a decrease of ≥3 points in the participant’s MMSE score during the follow-up. We classified individuals into participation (≥3 months) and non-participation (<3 months) groups for 17 different exercise types. Log-binominal regression analyses were applied to compare risk ratios and confidence intervals of developing cognitive decline between the two groups.
Results:
Thirty-nine participants (5.7%) developed cognitive decline during the follow-up period. After adjusting for confounders (age, MMSE score, depressive symptoms, body mass index, heart disease, hypertension, diabetes, smoking, low educational level, and the follow-up period in the baseline survey), those who participated in calisthenics demonstrated a significantly lower risk of developing cognitive decline than those who did not participate in calisthenics. No significant relationships between other exercise types and the risk of developing cognitive decline were found.
Conclusion:
Participation in calisthenics significantly reduced the risk of cognitive decline in community-dwelling older Japanese women, indicating that calisthenics may be a useful type of exercise for promoting dementia prevention.
INTRODUCTION
In 2013, the World Alzheimer Report predicted that the global number of dementia patients would increase to 65.7 million by 2030 and 115.4 million by 2050 [1]. Low- and middle-income countries will account for 65% and 71% of these numbers in 2030 and 2050, respectively [1], indicating the importance of finding effective approaches to preventing dementia in such countries. Participation in exercise can be an acceptable approach, especially in low- and middle-income countries, as it is a simple lifestyle modification that does not require complicated prescription medications.
Prospective observational studies have reported that habitual participation in physical activities and exercise may reduce the risk of dementia onset in older adults [2 –4]. Two meta-analyses that included data from these studies concluded that participation in physical activity and exercise is a useful strategy for dementia prevention [5, 6]. Thus, the potential number of future dementia patients may be significantly reduced if participation in physical activity and exercise is increased globally. However, for participation in physical activity and exercise to be effective in preventing dementia, we must develop appropriate evidence-based guidelines and recommendations regarding the amount and type of exercise that is most effective [7].
The optimal amount of physical activity and exercise for dementia prevention has yet to be identified, but the dose-response relationship of physical activity and exercise amounts with the risk of developing dementia has been systematically examined [8]. Xu et al. reported that an increase in leisure time physical activity by 10 metabolic equivalents*h/week could reduce the risk of all dementia by 9% and Alzheimer’s-type dementia by 13%, with significant dose-response relationships between the amounts and risks [8]. It should be noted that this meta-analysis included only three observational studies; thus, additional observational studies are needed in the future. However, the association between the amount of physical activity or exercise and the risk of developing dementia has been examined in many observational studies [7].
Despite this previous research on the topic, the question remains: what types of exercise are beneficial in reducing the risk of dementia onset [7]? Very few studies have examined the relationship between exercise type and the risk of developing cognitive decline or dementia [9, 10], indicating the difficulty of answering this question clearly. The physical activity guidelines of the American College of Sports Medicine divide exercise elements into four domains: aerobic, resistance, flexibility, and balance [11]. Thus, examining the effects of each of these four domains on cognitive function could help in the development of exercise guidelines for dementia prevention. However, some specific exercise types that older adults participate in voluntarily and habitually, such as calisthenics, dance, aqua exercise, golf, and ball games, overlap in multiple domains; as a result, it is cumbersome for older adults to determine and report what types of exercise they may be engaged in. To this end, it may be useful to investigate individual exercises for older adults as a way to complement exercise guidelines for dementia prevention. With this aim in mind, the present study examined the relationships between exercise types that community-dwelling older women participate in voluntarily and habitually and the risk of developing cognitive decline.
MATERIALS AND METHODS
Design and setting
We conducted a comprehensive prospective longitudinal study to identify risk and protective factors of geriatric syndromes in older women, including frailty, sarcopenia, pain, falls, incontinence, decline in oral function, and cognitive decline. Baseline surveys were conducted two times (the first wave in October 2017; the second wave in September 2018), and a follow-up survey was conducted in September 2019 at the Tokyo Metropolitan Institute of Gerontology.
Participants
The target population of this cohort study was women aged 65 to 81 years living in one of 19 areas near the Tokyo Metropolitan Institute of Gerontology. To recruit participants, we recorded all names and addresses of individuals living in the target area from the Basic Resident Register in 2017 (N = 6,788). After removing 422 individuals who had participated in another cohort study, we sent invitation letters to 6,366 candidates. A total of 1,845 candidates agreed to participate in the baseline survey. The baseline surveys were conducted in 2017 and 2018, as we did not have enough capacity to accept all candidates during the initial survey period in 2017. In 2017, we invited 1,401 women, and 1,035 individuals participated in the first baseline survey. In 2018, we invited the remaining 806 individuals, and 330 individuals participated in the second baseline survey. In total, 1,365 participants completed the baseline survey. Of these, 759 participants (55.6%) completed the follow-up survey. We excluded participants who: 1) had a disability in basic activities of daily living, neurological disease, or dementia (Alzheimer’s disease, vascular dementia, and other types of dementia), as diagnosed by physicians at the baseline survey (n = 56, 7.4%); 2) had a cognitive impairment (strongly suspected dementia) assessed as <24 points on the Mini-Mental State Examination (MMSE) [12] at the baseline survey (n = 13, 1.7%); or 3) had missing variables for the MMSE at the follow-up survey (n = 3, 0.4%). Ultimately, 687 participants (90.5%) were included in the analyses. Figure 1 shows a flowchart of participant enrollment in the study.

Flowchart of the study participants. MMSE, Mini-Mental State of Examination.
This study complied with the guidelines of the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of the Tokyo Metropolitan Institute of Gerontology. All participants provided written informed consent.
Measurement
Outcome measure
We assessed cognition function by using the Japanese version of the MMSE [12]. The MMSE has been shown to have sufficient or good validity and reliability for assessing global cognitive function in older populations. Scores range from 0 to 30 points, with higher scores indicating better cognitive function [13]. During face-to-face interviews, participants were asked to perform 10 cognitive tasks: 1) orientation (answering questions about “time” and “location”), 2) word memorization (listening to and repeating words), 3) calculation (performing subtraction using mental arithmetic), 4) word recall (repeating words memorized previously), 5) naming (providing the names of common items), 6) repetition (repeating infrequently used sentences), 7) auditory comprehension (performing actions based on verbal instructions), 8) reading comprehension (performing actions based on written instructions), 9) writing (writing a sentence that makes sense), and 10) figure drawing (drawing a figure on a paper based on instructions) [12]. A change in a MMSE score of at least 2–4 points over 1.5 years indicates a reliable change among cognitively intact individuals [14]. A 1–3 point decrease in a MMSE score over 1 year is considered a minimal clinically important difference [15]. In the current study, participants whose scores decreased more than 3 points on the MMSE from baseline to the follow-up were considered to be developing cognitive decline [14 –16].
Exercise participation
We developed a questionnaire to evaluate exercise participation. This questionnaire asks individuals, via a face-to-face interview, whether or not they participate in any of the 17 types of exercise that older Japanese adults commonly participate in, including calisthenics, walking, strength exercise, dancing, yoga, aqua exercise, ball games, bicycling, hiking, tai chi, golf, quoits, Japanese croquet, ten-pin bowling, jogging, martial arts, and others. Our previous studies also used this questionnaire, but did not assess exercise adherence using parameters such as exercise duration, frequency, and period of continuation for each exercise type [17, 18]. In the current study, we modified the questionnaire to assess exercise adherence by asking individuals about overall exercise duration, frequency per week, and length of the continuous period for each exercise type. Previous studies have not reported specific criteria to define a continuous period for exercise participation [9, 10]; however, exercise interventions for Alzheimer’s disease have included periods of at least three months to observe the effects on cognitive function [19]. Thus, we operationally defined exercise participation as participating in each exercise type for at least three months, and divided participants into participation and non-participation groups for each exercise type. Finally, the amount of exercise for each exercise type (duration per week, min/wk) was calculated by multiplying duration per time by frequency per week.
Covariates
As covariates, we evaluated demographic factors, medical history, depressive symptoms, and lifestyle factors. Demographic factors included age, body mass index, years of education, and number of cohabitants. Body mass index was categorized as underweight (<18.5), normal (18.5–24.9), and obese (≥25.0). We defined participants who had fewer than 12 years of education (did not graduate from high school) as having a low educational level. Medical history was assessed by asking participants whether they had physician-diagnosed hypertension, heart disease, diabetes, hyperlipidemia, or osteoporosis in the past year. Depressive symptoms were assessed using the Japanese short version of the Geriatric Depression Scale (GDS), the scores of which range from 0 to 15 points, with higher scores indicating worse depressive symptoms [20]. Lifestyle factors included smoking and drinking history. Participants who had a current history of those behaviors were defined as a smoker or drinker, respectively.
Statistical analysis
First, to prospectively examine the relationships between participation in each exercise type and the risk of developing cognitive decline, the chi-square or Fisher’s exact test was applied to compare differences in the rate of developing cognitive decline between the participation and non-participation groups in each exercise type in the baseline survey. Then, we applied a log-binomial regression analysis adjusted for age, MMSE score, GDS score, body mass index, heart disease, hypertension, diabetes, smoking, low educational level, and follow-up period. Several studies suggested these as confounders in the relationships of physical activity or exercise amount with the risks of developing cognitive decline and onset of dementia [4 , 22]. Risk ratios (RRs) and 95% confidence intervals (CIs) for developing cognitive decline in the participation groups for each exercise type were compared to the non-participation (reference) groups for each exercise type. We analyzed the relationships of seven exercise types with ≥5% participation rate at the baseline survey with developing cognitive decline, as other exercise types were considered to have insufficient statistical power for the analyses due to their low participation rates [17, 18]. Next, to examine the dose-response relationship of each exercise type amount with developing cognitive decline, we applied adjusted log-binomial regression analyses that included tertiles of exercise duration per week for each exercise type at the baseline survey as independent variables and developing cognitive decline as the dependent variable. In the dose-response analyses, only the two exercise types (calisthenics and walking) that could be divided into tertiles were analyzed. Finally, to retrospectively examine the characteristics of the analyzed samples, we divided individuals who did or did not participate in the follow-up survey into responded and non-responded groups, respectively. We compared the differences in baseline characteristics between the responded and non-responded groups in the follow-up survey by applying the Mann-Whitney U test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. In all analyses, several independent variables were missing (see Tables 1 and 2; range, 0–1.0%); these were excluded from each analysis. All analyses were performed using IBM SPSS version 25.0 (IBM Corp., Armonk, New York, USA). p < 0.05 was considered statistically significant.
Baseline characteristics of analyzed participants, comparisons between non-responded and responded groups in the follow-up survey, and missing variable information
†Missing values in analyzed data (n = 687). ‡Missing values in all data (n = 1,361). Data shown as median [interquartile range] or n (%). N/A, not applicable; MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale.
Exercise adherence to 17 exercise types in the baseline survey
†The number (%) of individuals who participated in each exercise types for at least 3 months (n = 1,361). ‡Missing values in all data (n = 1,361). Data shown as median [interquartile range] or n (%).
RESULTS
Figure 2 shows the distribution of changes in MMSE scores. Developing cognitive decline was observed in 39 participants (5.7%) during the follow-up period. Table 1 shows the baseline characteristics of the prospectively analyzed participants and compares these parameters between the responded and non-responded groups, as recorded in the follow-up survey, and information on missing variables. Compared to the responded group, participants in the non-responded group were older, had significantly higher GDS scores and rates of low educational levels, lower MMSE scores, and lower prevalence of hyperlipidemia and drinking behavior, as recorded in the baseline survey.
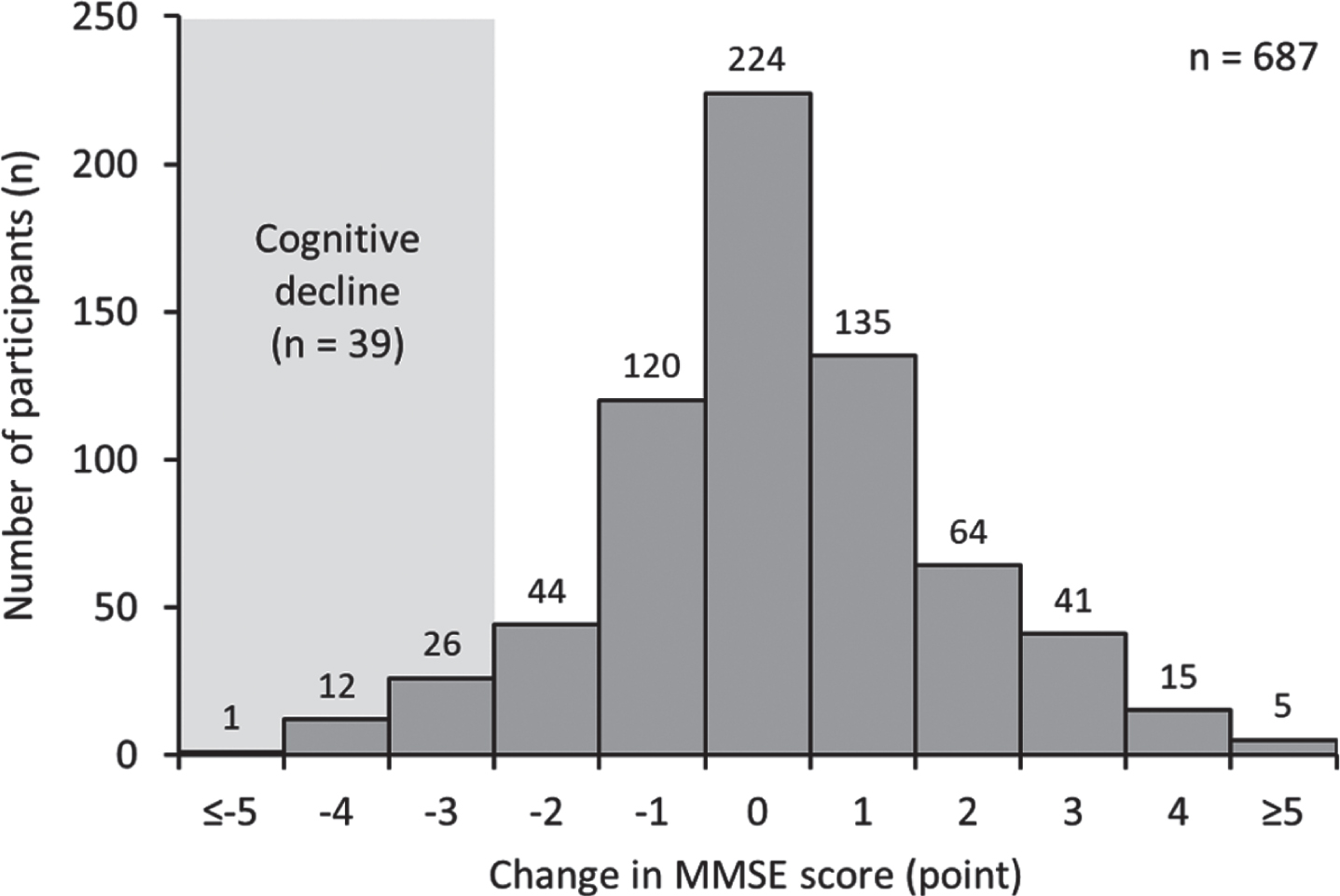
Distribution of changes in Mini-Mental State of Examination (MMSE).
Table 2 shows exercise adherence, including the number (%) of participants, duration, frequency, and amount of participation in each exercise type, as well as information regarding missing variables. The highest rate of exercise participation at the baseline survey was calisthenics (n = 780, 57.3%), followed by walking (n = 671, 49.3%), strength exercise (n = 151, 11.2%), dancing (n = 113, 8.3%), yoga (n = 109, 8.0%), others (n = 92, 6.8%), and aqua exercise (n = 90, 6.6%). The rates of participating in ball games, bicycling, hiking, tai chi, golf, quoits, Japanese croquet, bowling, jogging, and martial arts were all less than 5%.
Figure 3 shows comparisons of the proportion of participants with developing cognitive decline between the participation and non-participation groups for the seven exercise types. Although the rate of developing cognitive decline in the calisthenics participation group was significantly lower than that of the non-participation group (8.2% versus 4.1%, p = 0.023), no significant differences in the rates were observed for the other exercise types.

Comparison of the rates of developing cognitive decline between the participation and non-participation groups for seven exercise types. p values were calculated via the chi-square test (a) and Fisher’s exact test (b).
Table 3 shows the relationships between participation in one of seven exercise types and the risk of cognitive decline. Log-binomial regression analyses show that participation in calisthenics significantly reduced the risk of developing cognitive decline (RR: 0.50, 95% CI: 0.27–0.92) by 50%. This significance was maintained even after adjusting for confounders (RR: 0.44, 95% CI: 0.24–0.82). There were no significant differences in RRs for developing cognitive decline between the participation and non-participation groups for other exercise types. In addition, we found no significant dose-response relationships in tertiles regarding the amount of calisthenics (0 min/wk, reference; 1–59 min/wk, RR: 0.29, 95% CI: 0.11–0.75; ≥60 min/wk, RR: 0.57, 95% CI: 0.29–1.12; p for trend: 0.064) and walking (0 min/wk, reference; 1–140 min/wk, RR: 0.88, 95% CI: 0.40–1.91; ≥141 min/wk, RR: 0.69, 95% CI: 0.32–1.48; p for trend: 0.339) with a risk of cognitive decline.
Comparisons of the risk of developing cognitive decline over 1–2 years between participation and non-participation for seven exercise types
†n, number of participants with developing cognitive decline; N, number of all participants in each group. *Adjusted for age, low educational level, body mass index, hypertension, heart disease, diabetes, Geriatric Depression Scale score, follow-up period, smoking behavior, and Mini-Mental State Examination score at baseline. RRs, relative ratios; CI, confidence interval.
DISCUSSION
To the best of our knowledge, few studies have analyzed the relationship between various exercise types and cognitive decline in older adults [9, 10]. The current study identified that participation in calisthenics significantly reduced the risk of developing cognitive decline over 1–2 years by 56%. This finding supports the evidence that calisthenics, an activity in which older Japanese women participate voluntarily and habitually, may be a useful exercise type for promoting dementia prevention.
Calisthenics include radio calisthenics, television calisthenics, and community calisthenics. Our previous study showed that among community-dwelling older women, the group that participated in calisthenics had a lower risk of decline in instrumental activities of daily living than the non-participation group over a 4-year follow-up period [17]. The results of the current study may provide evidence that calisthenics can modify the risk of decline in instrumental activities of daily living via maintaining cognitive function, as cognitive impairment is a strong predictor of instrumental activities of daily living disability [23]. Calisthenics comprise light-intensity exercises and can be done anywhere and anytime; thus, they can easily be integrated into the long-term daily lifestyle of older adults. In particular, radio calisthenics have historically been popular as national health exercises, being implemented in education, workplaces, and community programs since 1928. Thus, this type of exercise is very familiar to Japanese people. Indeed, the current study showed that the participation rate for calisthenics was the highest of all exercise types. Calisthenics is often performed to music, and previous observation and intervention studies have reported that exercises with music, such as dancing, decreased the risk of dementia onset [9]; maintained white matter integrity in the fornix [24]; maintained volume in the superior frontal gyrus, anterior cingulate cortex, superior temporal gyrus, insular cortex, and hippocampus [25, 26]; and improved several cognitive domains in older adults [27].
Although specific neurophysiological mechanisms that show doing calisthenics reduces the risk of developing cognitive decline have not yet been identified, some researchers have argued that light-intensity exercise, such as calisthenics, promotes adult neurogenesis in the dentate gyrus [28] and increases hippocampal neuronal activity in rats [29]. It is also unclear whether specific movements used in calisthenics reduce the risk of developing cognitive decline. It is possible that other factors are at work, as in the process of participating in calisthenics, individuals may receive significant mental stimulation, such as uplifting or relaxing feelings due to music, memorization of the movements, coordination with music, and engagement with family and friends. The favorable effects of calisthenics on reducing the risk of developing cognitive decline may be the result of a combined effect involving intellectual, psychological, and social factors. It is relatively easy to implement calisthenics programs with minimal costs, making this type of exercise a good option for community adoption that is also generalizable for low- to middle-income countries. However, it should be noted that it is unclear whether calisthenics would be as widely accepted in other countries as it is in Japan, since it is a unique exercise that has been historically accepted by the Japanese population.
Our results did not show significant relationships between participation in other exercise types and the risk of developing cognitive decline. These results were unexpected, as findings from previous randomized controlled trials have shown that participation in aerobic or resistance exercises, including walking and strength exercises, is useful for maintaining cognitive function in older adults with dementia risk [30, 31]. In addition, previous studies have identified various favorable effects of dancing on the brain. Two possible reasons for the non-significant relationships between other exercise types and the risk of developing cognitive decline should be considered. First, although other exercise types also showed a trend toward reducing the risk of developing cognitive decline, relatively few events of developing cognitive decline in the group with participation in exercises such as dancing, aqua exercise, yoga, and strength exercise, caused a wide range of CIs, indicating that reliable RRs could not be obtained. One large-scale observational study (N = 15,589) reported that participation in aerobic exercise (such as jogging, running, swimming, hiking, ball games, and cycling) and mind-body exercises (e.g., tai chi and yoga) may significantly reduce the risk of developing dementia over six years (odds ratio [95% CI] were 0.81 [0.68–0.95] and 0.76 [0.63–0.92], respectively) [9]. Such a sample size and observation period provide statistical power and reliable risk estimation. Second, aspects of exercise adherence, such as intensity, frequency, and duration, might be not enough to maintain cognitive function with other exercise types. Four meta-analyses that examined the effects of exercise on cognitive function concluded that aerobic exercises, including walking, resistance exercise, and tai chi, significantly improved cognitive function in older adults [32 –35]. However, such studies often involve exercise supervised by professionals; thus, exercise adherence may be significantly different than in unmonitored voluntary and habitual exercise. In the current study, we could not examine whether adherence to each exercise type had an effect on the relationship between exercise type and the risk of developing cognitive decline due to sample sizes that were insufficient for quantifying the amount of each exercise except for calisthenics and walking. The above two reasons may reflect the weaker statistical power for detecting significant relationships of other exercise types with the risk of developing cognitive decline. Future studies should quantify adherence to each exercise based on information regarding intensity, frequency, and duration, and then analyze the association between exercise types and risk of cognitive decline using a larger sample size.
To the best of our knowledge, this study is the first of its kind to examine the relationships of seven specific exercise types with the risk of developing cognitive decline and to identify that participation in calisthenics can significantly reduce such risk in older women. However, the study also has several limitations. First, although the participants were selected through population-based sampling, sampling biases might have been present, as 78.6% of candidates and 44.2% of participants did not participate in the baseline and follow-up surveys, respectively. Our results indicated that, compared to individuals who did not respond the follow-up survey, individuals who did respond were younger and had a better psychophysiological status in the baseline survey (see Table 1). Moreover, we targeted only older women living in a large city. These sampling biases may have reduced the external validity of our results. It also should be noted that the results of our study may be specific to one group of older Japanese women, and generalizability to other populations may be limited. For example, in the older Chinese population, the participation rate of tai chi (22%) is extremely high compared to that of walking (7%), dancing (4%), and jogging (3%) [36]. These results indicate that the types of exercises in which individuals participate is strongly affected by historical and cultural preferences, suggesting that future studies should examine the relationships of exercise types with dementia onset or developing cognitive decline in different populations. Second, we could not collect information regarding other potential confounders, such as participation in unstructured physical activities including domestic work, transportation, or occupational activities. In addition, we could not mutually adjust for the seven exercise types in the multivariable analyses, as we were limited in the number of possible covariates that could be included as independent variables in the log-binomial regression analysis. Therefore, it is unclear whether calisthenics reduces the risk of cognitive decline independent of other potential confounders, such as physical activities and exercise types. To control potential confounders more conservatively, a randomized control trial identifying the effects of doing calisthenics on cognitive function will be needed in the future. Third, self-reported exercise participation may result in recall and instrument biases, which could lead to a decline in internal validity for the study’s results. Finally, we did not follow the onset of dementia based on international diagnostic criteria; thus, we are unable to provide results regarding the association between specific exercise types and dementia onset. Future studies should therefore identify specific exercise types that reduce the risk of dementia onset. However, developing cognitive decline is one of the primary predictors of dementia onset; thus, exercise types that reduce the risk of developing cognitive decline could be expected to promote dementia prevention.
In conclusion, our results showed that participation in calisthenics significantly reduced the risk of cognitive decline in older Japanese women. This result indicates that calisthenics can be a useful exercise type for delaying cognitive decline or maintaining cognitive function in older women. This finding may help construct exercise guidelines for dementia prevention, allowing recommendations of exercise types as complementary resources. To determine whether there are any significant associations between other exercise types and reduced risk of cognitive decline, larger cohort studies that target different populations will be needed in the future.