
Abstract
Background:
There are currently few biomarkers to assist in early diagnosis of dementias.
Objective:
To distinguish between different dementias: Alzheimer’s disease (AD), vascular dementia (VaD), and Parkinson’s disease dementia (PDD) using simple neurophysiologic (P300) and laboratory markers (transforming growth factor β1 “TGF-β1”).
Methods:
The study included 15 patients for each type of dementia and 25 age- and sex-matched control subjects. Dementia patients were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders 4th edition-revised (DSM-IV-R). Modified Mini-Mental State Examination (3MS), Memory Assessment Scale (MAS), P300, and TGF-β1 were examined for each participant.
Results:
There were no significant differences between groups as regard to age, sex, and education, social, and economic levels. Significant differences between groups were observed in registration and naming variables of the 3MS. Compared with the control group, P300 latency was prolonged in all groups, although to a greater extent in AD and PDD than in VaD. A serum level of TGF-β1 was significantly elevated in all groups but was significantly higher in AD and VaD than in PDD. 3MS tended to correlate with P300 more than TGF-β1, and to be stronger in AD than the other groups.
Conclusion:
Measurements of P300 latency and serum levels of TGF-β1 can help distinguish AD, PDD, and VaD. P300 was more prolonged in AD and PDD than VaD whereas TGF-β1 was significantly higher in AD and VaD than PDD. Thus P300 and TGF-β1 may be useful biomarkers for detection and evaluation of the extent of cognitive dysfunction.
Keywords
INTRODUCTION
Dementia is a chronic brain disorder that impacts cognition and produces mental degeneration [1]. Alz-heimer’s disease (AD) is the most common form, affecting 69% of the elderly population [2] and is characterized by the gradual loss of memory and cognition, and reduction in activities of daily life. AD is the only leading cause of death that currently unpreventable and incurable [3]. Vascular dementia (VaD) is the second most prevalent form of dementia [4] characterized by progressive worsening of cognitive function and memory cause exclusively by vascular disease within the brain [5]. Parkinson’s disease dementia (PDD) is one of the most prevalent non-motor manifestations of Parkinson’s disease (PD) affecting roughly 22.3% of PD patients [6]. Over the course of their illness, 80% of PD patients are affected by PDD [7].
There are currently few biomarkers to assist in early diagnosis of dementias. We consider two in the present report. P300 latency reflects the time to process information before making a response and is negatively correlation with mental function [8]. It is considered to be a sensitive temporal index of the neural activity underlying attention allocation and immediate memory. TGF-β1 is a multifunctional cyt-okine that plays a crucial role in tissue injury and repair, controlling neuronal growth and survival [9]. The exact role of this cytokine in neurodegenerative disorders remains controversial since it either aggravates or improves neurodegeneration [10]. It is suggested to play a role in neuronal development and synaptic plasticity [11].
The aim of the present study was to measure these two markers in three types of dementia: AD, VaD, and PDD to test whether they could help distinguish between them.
METHODS
Study design and participants
This was a cooperative study between Department of Medical Physiology and Department of Neuropsychiatry, Assiut University Hospital, Assiut, Egypt. It was conducted on 45 patients presenting with dem-entia at the outpatient clinic of the hospital of Neuropsychiatry, Assiut University. A group of 25 age, sex, and educationally matched controls was also recruited.
The study protocol was approved by the ethical committee at Faculty of Medicine, Assiut University and all participants or their caregivers gave written informed consent.
The study included three groups of patients presenting with dementia diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders 4th edition-revised (DSM-IV-R) [12]. They were classified to three groups AD, VaD, and PDD. For AD, the diagnosis was based DSM-IV-R [12] with a history of progressive cognitive worsening for at least 1 year, the diagnostic criteria of the National Institute of Neurological and Communicative Disorders Association [13] and a score ≤4 on Hachinski’s ischemic score [14]. For VaD, diagnosis was based on the DSM-IV-R and the AD Diagnostic and Treatment Centers criteria for ischemic VaD [15] and a score ≥7 on Hachinski’s ischemic score. All the patients with VaD showed a stepwise deterioration of cognitive function and one or more infarcts outside the cerebellum, which were detected by neuroimaging. For PDD, diagnosis was based on the UK Brain Bank criteria [16] with dementia causing a decline in function severe enough to impair the patient in daily activities and in at least one cognitive domain: attention, executive, visuo-spatial ability, or language.
Exclusion criteria: age below 50 years and above 75 years; other neurological disorders or psychiatric disorders; previous history of stroke; metabolic disturbance; other major medical illnesses; epilepsy; inflammatory, autoimmune, or infectious disease.
The Socioeconomic Status Scale designed by Abd-El-Tawab [17] was used to assess the socioeconomic status of the family.
Each subject was assessed with the following:
Modified Mini-Mental State Examination (3MS)
3MS is a screening test for dementia with scores ranging from 0 to 100, with a higher score indicating less impairment. Subtests involve immediate and remote memory, orientation, attention and concentration, language and naming, verbal fluency, and executive function. A total score less than 79 indicates mild to moderate cognitive impairment, while a total score <48 indicates severe impairment [18].
Memory Assessment Scale (MAS)
MAS assess three areas of cognitive function: short-term memory, verbal memory, and visual memory. Total MAS represents verbal + visual memory scores [19].
Event related potential (P300)
Event-related potentials were elicited with an auditory discrimination task in which the participant was required to distinguish between two tones by responding to the target (pressing a button) and not res- ponding to the standard tone. Responses to 30 target and 120 non-target tones were obtained in each trial. Before recording; subjects were familiarized with the two tones. The recordings of the responses were performed with A Nihon Kohden Machine model 9400 (Japan) with silver-silver chloride surface electrodes, applied at frontal (Fz), central (Cz), and parietal (Pz) zones (according to International 10–20 system). P300 latency was measured as the major positive peak after N200, within a range of 250–500 ms [20].
Assessment of the serum level of human TGF-β1 by ELISA Kit
The serum level of human TGF-β1 was estima-ted according to the manufacturer’s manual TGF-β1, ELISA Kit, Catalog No: E-EL-H0110 96T-Elab-science Biotechnology, USA (Elabscience Biotechnology Co., Ltd).
Statistical analysis
Data were analyzed using Statistics Package for Social Sciences (SPSS) version 20. The data were expressed as mean±standard deviation (SD). All parameters were analyzed using the Mann Whitney test. In addition, sex and educational level in the AD group were analyzed using the Chi-square test. Mann Whitney tests were used to compare the control group with each dementia group and each dementia group with each other. A Kruskal-Wallis H Test was used to compare the three dementia groups with each other. Also, the same test was done between control group and each type of dementia. Non-parametric Spearman’s test correlations between TGF-β1 and neurophysiological parameters were calculated. Differences between the two groups were considered significant when p values were less than 0.05.
RESULTS
Demographic data of the included patients
The demographic data of the control, AD, VaD, and PDD groups are shown in Table 1. There were no significant differences between groups in age, sex, education, or social and economic level.
Demographic data of the control, Alzheimer’s disease (PD), vascular, and Parkinson’s disease (PD) dementia groups
*p < 0.05 control versus each group (Mann-Whitney test).
Modified Mini-Mental State Examination (3MS) of the study groups
3MS scores are given in Table 2. There was significant impairment in most of variables of 3MS in the different types of dementia compared with the control group. There significant differences between registration and naming variables in the three types of dementia, but there was no significant difference between the dementia groups in the total 3MS score (Table 2).
Modified Mini-Mental State Examination (3MS) among different groups: control, Alzheimer’s disease (AD), vascular dementia, and Parkinson’s disease dementia (PDD)
Data presented as mean±SD; 3MS, Modified Mini-Mental State Examination; *p < 0.05, **p < 0.001, ***p < 0.0001 (comparison between control group versus each group of dementia). There are no significant differences between each dementia group in comparison with each other using Mann-Whitney test.
The Memory Assessment Scale (MAS) among studied groups
Table 3 summarizes the MAS scores. All three types of dementia had reduced scores compared with the control group. But there were no significant differences between them.
Memory Assessment Scale (MAS) of the control, Alzheimer’s disease (AD), vascular dementia, and Parkinson’s disease dementia (PDD) groups
Data presented as mean±SD. *p < 0.05, **p < 0.01, and ***p < 0.001 when comparing control group (n = 25) versus each dementia groups (n = 15 in each group) using t-test. There are no significant differences between each dementia group in comparison with each other using Mann-Whitney test.
P300 latency among patients with dementia
Table 4 summarizes the P300 latencies, which were significantly prolonged in all three dementia groups compared with control. There were also significant differences between the types of dementia. Post hoc paired testing revealed that P300 was later in AD and PDD compared with VaD (t = 2.4, df = 22.5, p = 0.02, and t = 3.69, df = 17.7, p = 0.002) while there was no significant difference between AD versus PDD (t = –1.5, df = 24.3, p = 0.13).
Event related potentials including p300 latency of the control, Alzheimer’s disease (AD), vascular dementia, and Parkinson’s disease dementia (PDD) groups
Data presented as mean±SD. Average latency of P300, Hits and False response were recorded from three points (Frontal zone (FZ), cortical zone (CZ), and parietal zone (PZ). *p < 0.05, **p < 0.01, and ***p < 0.001 comparing each dementia group with control group.
Serum levels of transforming growth factor β1 (TGF-β1) among studied groups
Figure 1 shows that serum levels of TGF-β1 in all dementia groups were significantly elevated in comparison with control. However, there were significant differences between the types of dementia. Post hoc paired testing revealed that TGF-β1 was significantly higher in AD and VaD compared with PDD (t = 15.3, df = 17.7, p = 0.0001, and t = 4.8, df = 14.4, p = 0.0001, respectively) while there were no significant differences between AD and VaD (t = –1.5, df = 22.8, p = 0.126).

Serum levels of transforming growth factor β1 (TGFβ1) in the Alzheimer’s disease dementia group (AD), vascular dementia group (VaD), and Parkinson’s dementia groups (PDD) versus the control. Data presented as mean±SE (***p < 0.001 and **p < 0.01 each dementia group versus control group). TGFβ1 are significantly higher in AD and VaD compared with PDD (***p < 0.001), while no significant differences between AD versus VaD.
Correlation of total 3MS and total MAS with P300 and TGF β1
The correlations between these variables are tabulated in Table 5 and plotted in Figs. 2, 3, and 4. However, if a strict statistical correction is made for the 15 separate correlations (a Bonferroni correction would multiply the p-values by 15), the only significant ones remaining are those between 3MS and P300 in AD and VaD.
Correlation of total 3MS and total MAS with P300 and TGF β1 in the 3 types of dementia
*p < 0.01, **p < 0.001, ***p < 0.0001.
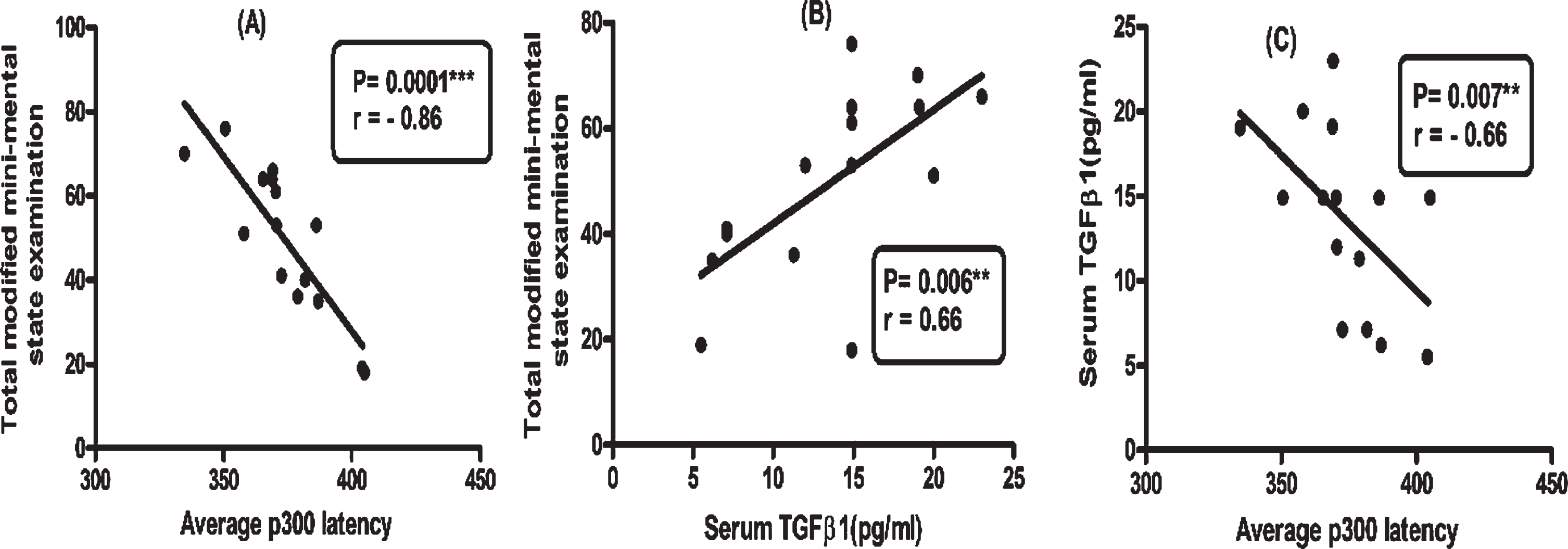
Correlation between total Modified Mini-Mental State Examination (3MS) with average P300 latency (A), and with transforming growth factor (B). Correlation between serum TGFβ1 and average P300 latency (C) in Alzheimer’s disease dementia.
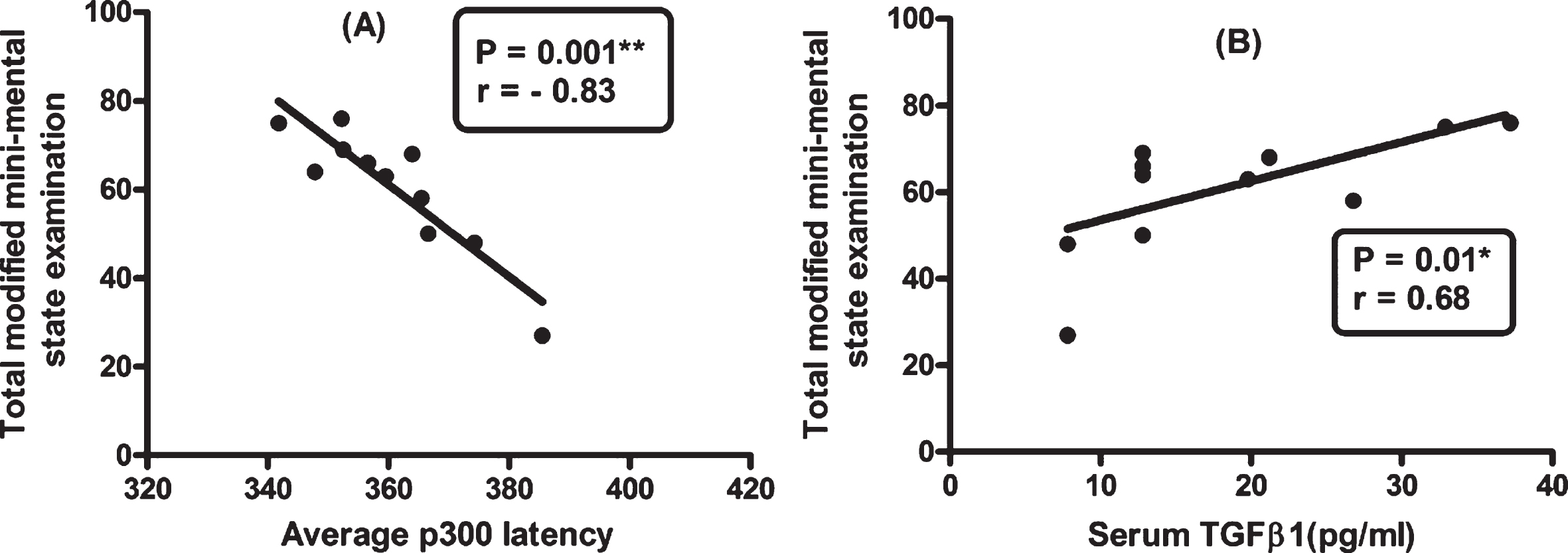
Correlation between total Modified Mini-Mental State Examination (3MS) with average P300 latency (A), and with serum TGF-β1 (B) in vascular dementia (VaD). A significant negative correlation between 3MS and P300 latency (p = 0.001) and significant positive correlation between 3MS and TGF-β1 (p = 0.01).
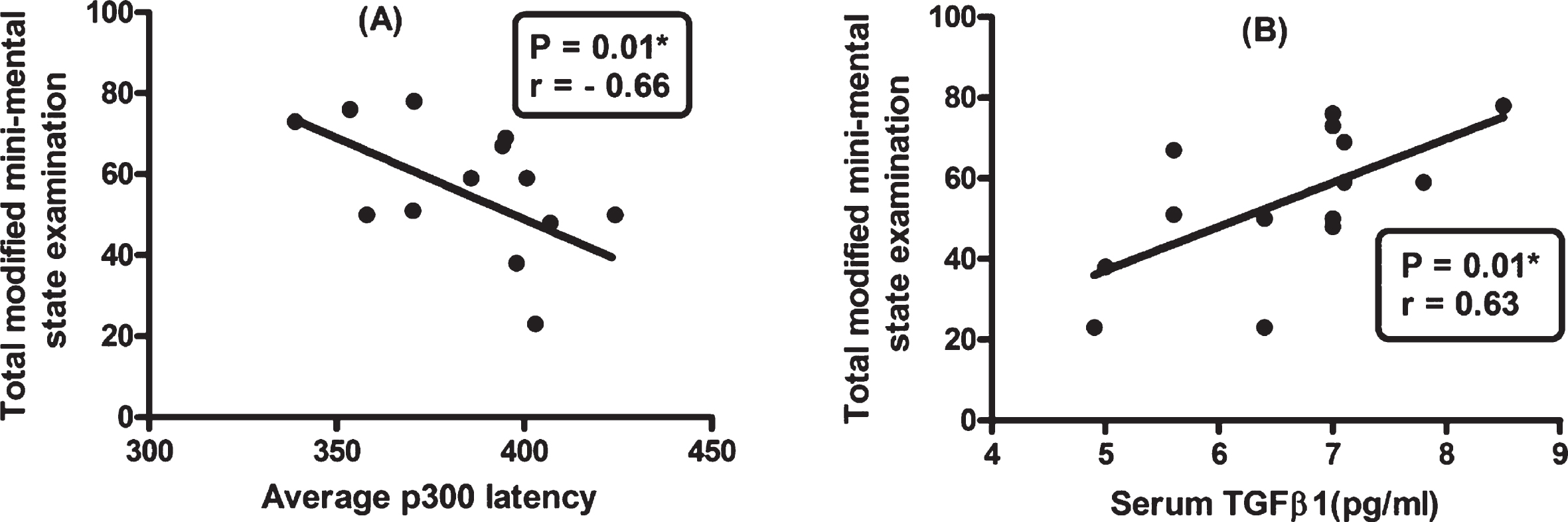
Correlation between total Modified Mini-Mental State Examination (3MS) with average P300 latency (A), and with serum TGF-β1(B) in Parkinson’s disease dementia.
In general, the correlations are stronger in AD (which also has a borderline correlation between TGF-β1 and P300) than in the other groups. There also is a tendency for there to be stronger correlations between dementia scores and P300 latency than TGF-β1.
DISCUSSION
The results of the psychometric tests (3MS and MAS) in the present study are similar to those reported previously in AD [21–23], VaD [24, 25], and PDD [26–28]. However, the cause of the symptoms differs. There is a primary disorder of the central cholinergic system [21] and loss of functional hippocampal synapses in AD [23, 29]. In contrast, in VaD cognitive impairment depends on the volume, number, and location of the infarctions [24]. The frontal lobe, responsible for executive function is the most vulnerable site to microvascular damage in VaD [30] and this might be the cause of altered executive function. In addition, the presence of cholinergic system damage in those patients could explain the impairment in learning and memory [31]. Finally, in PDD, the cognitive deficit has been attributed to the dopa-minergic and cholinergic dysfunction [26] as well as limbic and cortical deposition of Lewy body pathology [32].
The latency of the P300 study was significantly delayed in all patient groups compared to the control group as reported previously by several groups [33–41]. The working memory and attention assessed by p300 potential mainly depend on cholinergic substrate [22] which also the main neurotransmitter generating P300 [42, 43], so cholinergic neuron damage in these types of dementia as reported by previous studies [44–46] could explain the delayed latency of P300 potential.
Interestingly P300 latency was significantly prolonged in AD and PDD than VaD, it may be attributed to cortical cholinergic degeneration, mainly in the temporal lobes as well as in adjacent limbic and paralimbic areas that recorded in AD [47]. In PD there is widespread cholinergic dysfunction involving cortical, nigral, striatal, and thalami [44, 49], and even more severe than AD with the same cognitive profile [50]. However, in VaD, the cholinergic dysfunction was mainly due to local hypoperfusion of ischemic area [45], and less evident than in AD and PDD [51]. On the other hand, the concentration of cerebrospinal fluid acetylcholine in VaD was lower than controls but it was still higher than AD type [51].
As P300 latency may reflect the general cognitive decline regardless its cause rather specific domain and could be used as a marker for global cognitive dysfunction [52–54]. In the present study the significant negative correlation between P300 and the total score of 3MS especially in AD of dementia support this idea.
In the present study, the significant elevation of the serum levels of TGF-β1 in patient groups compared to the control group could suggest that elevation of TGF-β1 considered as biomarker for dementia. An important result here was the significant higher level TGF-β1 in AD and VaD than in PDD. Since the intensity and levels of neuroinflammation and in-flammatory mediators are markedly increased in neu-rodegenerative (AD) and vascular lesions [55, 56]. In addition, the elevated level of TGFβ1 in AD could be attributed to Aβ triggered oxidative stress, neuroinflammation, as TGF-β1 generated an anti-infla-mmatory reaction to induce astrocytes and microglia to increase clearance of Aβ [57, 58]. Moreover, the AD and VaD may share the same vascular comorbidity like vasculopathies leading to Aβ accumulation [59] and nitric oxide oxidative stress [60]. However, the impairment of the TGF-β1 signal increases the deposition of neurofibrillary tangles in AD and 50% of PD patients with dementia [11].
The present study showed that the elevated TGF-β1 serve as an early neuroprotective effect in each demented group as the TGF-β1 level was weak pos-itively correlated with the total score of 3MS. However, this elevation of TGF-β1 continue for a time then with the progression of disease it decreased again as it correlated negatively with P300 latency.
We assumed that TGF-β1 increased in early and moderate stages of dementia and thus correlated with cognitive function, but as the disease progress and degeneration of neurons become evident, TGF-β1 starts to decline in line with cognitive deterioration. This assumption may explain the controversy of correlation between TGF-β1 and P300 latency, this in line with Moota and colleagues [61] as they found that higher level of TGF-β1 was recorded in early and moderate phases of disease, as a response to neuro-inflammation and decrease level in severe cases points to immune dysfunction. In this context, Malaguarnera and colleagues [62] analyzed plasma levels of pro-inflammatory interleukin-18 and TGF-β1 plasma levels in AD and VaD compared to healthy controls and concluded that levels of IL-18 and TGF-β1 are inversely linked in AD and VaD. In addition, TGF-β1 is overexpressed in other focal brain lesions and in PD non-demented patients [63].
Conclusion
The three types of dementias were hardly differentiated relaying on 3MS and MAS only. Measurements of P300 latency and serum levels of TGF-β1 can help distinguish AD, PDD, and VaD. P300 was more prolonged in AD and PDD than VaD whereas TGF-β1 was significantly higher in AD and VaD compared with PDD. Thus P300 and TGF-β1 may be useful bio-markers for early detection and evaluation of the ex-tent of cognitive dysfunction.