
Abstract
Background:
The semantic variant of primary progressive aphasia (svPPA) is characterized by a progressive loss of semantic knowledge impairing the ability to name and to recognize the meaning of words.
Objective:
We aimed to evaluate the immediate and short-term effect of errorless learning speech therapy on the naming and recognition of commonly used words in patients with svPPA.
Methods:
Eight participants diagnosed with svPPA received 16 sessions of intensive errorless learning speech therapy. Naming and word comprehension tasks were evaluated at baseline, immediately postintervention, and at follow-up after 1, 3, and 6 months. These evaluations were performed using two item sets (a trained list and an untrained list).
Results:
In the naming tasks, patients showed a significant improvement in trained items immediately after the intervention, but that improvement decayed progressively when therapy ended. No improvements were found either in trained comprehension or in untrained tasks.
Conclusion:
Errorless learning therapy could improve naming ability in patients with svPPA. This effect may be due to the relative preservation of episodic memory, but the benefit is not maintained over time, presumably because there is no consolidation.
Keywords
INTRODUCTION
Primary progressive aphasia (PPA) is characterized by a progressive loss of language abilities but relative preservation of other cognitive abilities [1]. Three variants of PPA have been described: a non-fluent/agrammatic variant, a logopenic variant, and a semantic variant (svPPA), also known as semantic dementia [2]. The language impairment in svPPA is characterized by moderate to severe naming problems, altered single-word comprehension (i.e., altered word recognition) and object knowledge, empty speech (i.e., with low informative content) with semantic errors, and poor semantic fluency. However, syntax and phonology are spared, while other cognitive functions such as episodic memory are relatively preserved [3–5]. During the disease course, patients with svPPA typically also develop behavioral alterations [6]. Neuroimaging findings typically show asymmetric focal atrophy of an anterior and inferior part of the left temporal lobe [2].
Errorless learning (EL) is a promising method for cognitive rehabilitation that eliminates the possibility of errors during the intervention. The EL approach is based on the principles of learning and memory. Explicit memory, which refers to the conscious experience of remembering previously learned information, has been divided into episodic and semantic memory. By contrast, implicit memory refers to the performance of previously learned tasks that do not require conscious recollection of those experiences. It has been hypothesized that EL can leverage implicit or residual explicit memory while avoiding the semantic memory [7, 8].
A prevailing theory in the literature suggests that people with cognitive impairment learn new skills more successfully when errors are avoided during training [9]. In svPPA, rehabilitation by EL speech therapy involves relearning new information, avoiding the errors in naming, and enhancing the semantic network to relearn the name of the object and its meaning through both implicit memory and explicit episodic memory. The hippocampal system is the main structure involved in explicit episodic memory, and its relative preservation in patients with svPPA would theoretically allow the acquisition of new information [10].
The lack of semantic information during verbal learning makes patients with svPPA more vulnerable to errors committed during speech rehabilitation, and as such, EL may be the better approach in these patients [11, 12]. Only a few previous studies have tested EL in patients with svPPA [11–13]. Notably, Jokel et al. showed that EL speech therapy provides better outcomes for these patients than therapy in which errors may occur [11]. Jefferies et al. also observed in a single patient that EL speech therapy was more beneficial for svPPA when errors were minimized [12]. Less has been reported about the maintenance of this improvement or about the response in terms of single-word comprehension [14].
In this study, we aimed to evaluate the effect of EL therapy, together with its maintenance over time, on naming and single-word comprehension learning in patients with svPPA. Given that cognition has been reported to be an important factor for determining the outcome of EL therapy, we also evaluate patient response according to different cognition features [15].
MATERIAL AND METHODS
Participants
Participants were recruited from the Alzheimer’s and Other Cognitive Disorders Unit of the Hospital Clinic of Barcelona, Spain. All svPPA diagnoses were made by a specialist neurologist according to the International Consensus Criteria [2]. Participants were assumed to have capacity for consent and all provided written informed consent to participate. Additional oral information was provided if the participant had problems understanding relevant written terms. The study was approved by the Hospital Clinic Ethics Committee.
Inclusion and exclusion criteria
The inclusion criteria were as follows: 1) diagnosis of svPPA according to the International Consensus Criteria [2], with a Severity Rating Scale score of 2–5 (mild or moderate stage) according to the Boston Diagnostic Aphasia Examination (BDAE) and a raw score of ≥5 on the Boston Naming Test (BNT) [16]; 2) agreement to attend speech therapy twice a week for eight consecutive weeks; and 3) commitment not to participate in another cognitive or speech and language intervention during the study.
The exclusion criteria were as follows: 1) history of other pre-existing neurological or psychiatric comorbidities that may affect language; 2) severe disease stage (BDAE severity scale score of 0 or 1; BNT raw score of <5); 3) generalized dementia, as rated by a Mini-Mental State Examination (MMSE) score of < 15.
Baseline neuropsychological assessment
Prior to starting the intervention, all participants’ cognitive statuses were assessed using the MMSE [17]. We retrospectively reviewed neuropsychological memory results and classified the participants according to their results in delayed memory recall tests, including the Consortium to Establish a Registry for Alzheimer’s Disease neuropsychological battery [18], the Free and Cued Selective Reminding Test [19], and the Rey Auditory Verbal Learning Test [20]. Memory performance between tests were analyzed by comparing individual z-scores with the normal population: a delayed memory recall score at least three standard deviations below the mean was classified as severe memory impairment, with all other results classified as mild memory impairment. Assessments were performed 6 months before the intervention started. Language abilities were assessed using the BNT, the Category Denomination and Comprehension test, and the Camel and Cactus subtests from the Cambridge Semantic Battery [3, 21]. The Severity Rating Scale of the BDAE was used to classify participants as having mild (score=4 or 5) or moderate (score=2 or 3) language impairment.
Intervention
The EL speech therapy intervention was designed to minimize the possibility of errors during the intervention. We created a set of 25 everyday items from 5 semantic categories (i.e., food, hygiene, common objects, food utensils, and clothing). Training sessions were administered by a speech therapist with expertise in PPA (NM). The therapist started sessions by asking the participants four questions (yes/no) about each item from the 25-item list, including cues in an error-free learning environment, and presenting both a picture and the object simultaneously. For example, if a picture of an apple was shown, the speech therapist asked (with pauses after each question): “Is it food?”; “Could you put it on to cake?”; “Does it begin with the letter A?”; “Is it an apple?”; “Yes, apple”; “Please repeat: apple.” We helped with the gesture and/or the image for all words to ensure they understood the meaning of each word (e.g., food gesture with hand, a cake picture, and so on). Depending on the situation, the speech therapist could provide the correct answer before the patient used a word intrusion and made an error. After each session, participants did a grammar integration exercise that involved completing a sentence with the correct word from the trained list. Participants engaged in 16 therapy sessions (45 minutes each, twice a week) over an 8-week period. To minimize response bias through recall of a prior response, the order of image presentation was varied in each session.
Evaluation
We assessed semantic knowledge of words across input (comprehension) and output (naming) modalities, as summarized in the Supplementary Material. For this, we compared results for the list of 25 trained words with the results for a list of 25 untrained words that are commonly used and from the same semantic categories. Regarding category naming, images from the list were presented to the subject who was then asked to name the object as fast and accurately as possible. Regarding category comprehension, the examiner showed five words in the same semantic category and the participant was asked to indicate the word that they heard. In each case, we gave one point was given for every correct answer and zero points for every incorrect answer or failure to respond (maximum response time=20 s). Participants were evaluated with the same lists at baseline, immediately postintervention, and after 1, 3, and 6 months of follow-up.
Statistical analysis
Data analyses were performed using RStudio version 1.1.463 (RStudio Inc). The percentage of correct answers per task was calculated, and the mean and standard deviation of correct answers were calculated for each evaluation. The Wilcoxon test was used for pairwise comparison of non-parametric paired samples. Differences between patients with different memory or language states were also evaluated with the Wilcoxon test. The significance threshold was set at p < 0.05 for all analyses.
RESULTS
Baseline characteristics
The baseline demographic and neuropsychological results for the eight patients with svPPA are summarized in Table 1. The mean MMSE score was 24.5. According to the BDAE severity scale, four participants had mild aphasia (score=4) and the other four had moderate aphasia (score=2 or 3). All patients exhibited moderate to severe alterations in word naming, with a mean score of 15 out of 60 items on the BNT. All eight participants completed the full intervention and were evaluated immediately and at 1-month postintervention, but only six participants completed all follow-up evaluations. The others only attended follow-up to 1 and 3 months.
Demographic characteristics and results of baseline evaluations
BNT, Boston Naming Test; CSM, Cambridge Semantic Battery; F, female; M, male; MMSE, Mini-Mental State Examination.
Effect of the errorless learning intervention
Figure 1 and Table 2 show the individual and average results for each evaluated task.

A–D) Individual percentages of correct answers at each assessment by evaluations. E–H) Mean percentages of correct answers at each assessment by evaluations. t0 = baseline; t1 = immediate postintervention; t2 = 1 month postintervention; t3 = 3 months postintervention; t4 = 6 months postintervention.
Mean numbers and percentages of correct answers, together with the percentage improvement, shown by assessment
SD, standard deviation.
All participants showed significant improvement in naming tasks between the assessments at baseline and immediately after the intervention. Regarding group comparisons, participants correctly named a mean of 11.6±5.8 items (46% correct) before the intervention, which increased significantly to 21.9±3.5 for trained items (87.5% correct, p < 0.05) after the intervention, with three participants gaining a maximum score. However, this gain decayed progressively thereafter, and although improvements from baseline remained significant at 1 month (19.2±5.75 items; 77% correct, p < 0.05) and 3 months (16.4±8.3 items; 74.9% correct, p < 0.05), item naming had nearly returned to baseline by 6 months (12.9±9.9 items; 68.7% correct; p = 0.178). No significant improvement was found for untrained items either after the intervention or in the longitudinal evaluations.
In the comprehension tasks, four participants improved between baseline and immediately after the intervention, two participants had already obtained the maximum scores at baseline, and the two remaining cases displayed no significant improvement. Participants recognized a mean of 23.0±1.5 items (92% correct) and 24.1±1.4 items (96% correct) in the trained and untrained lists, respectively. No significant differences existed between baseline and any follow-up evaluation for either the trained items or the untrained items, with several participants obtaining maximum scores.
Results according to memory and language severity
We investigated if the severity of language or memory impairment could explain differences in response to the intervention. No significant differences in outcomes were found between participants with mild and moderate language impairment (Fig. 2A) in either the conditions (trained and untrained) or the language functions (naming and comprehension). Concerning the impact of mild and severe memory impairment (Fig. 2B), there was a non-significant trend for a better mean improvement in those with mild impairment (13.5 items [54%] versus 7.0 items [28%]; p = 0.102). Severity of memory impairment did not lead to statistical differences in either the comprehension tasks or the naming of untrained items.
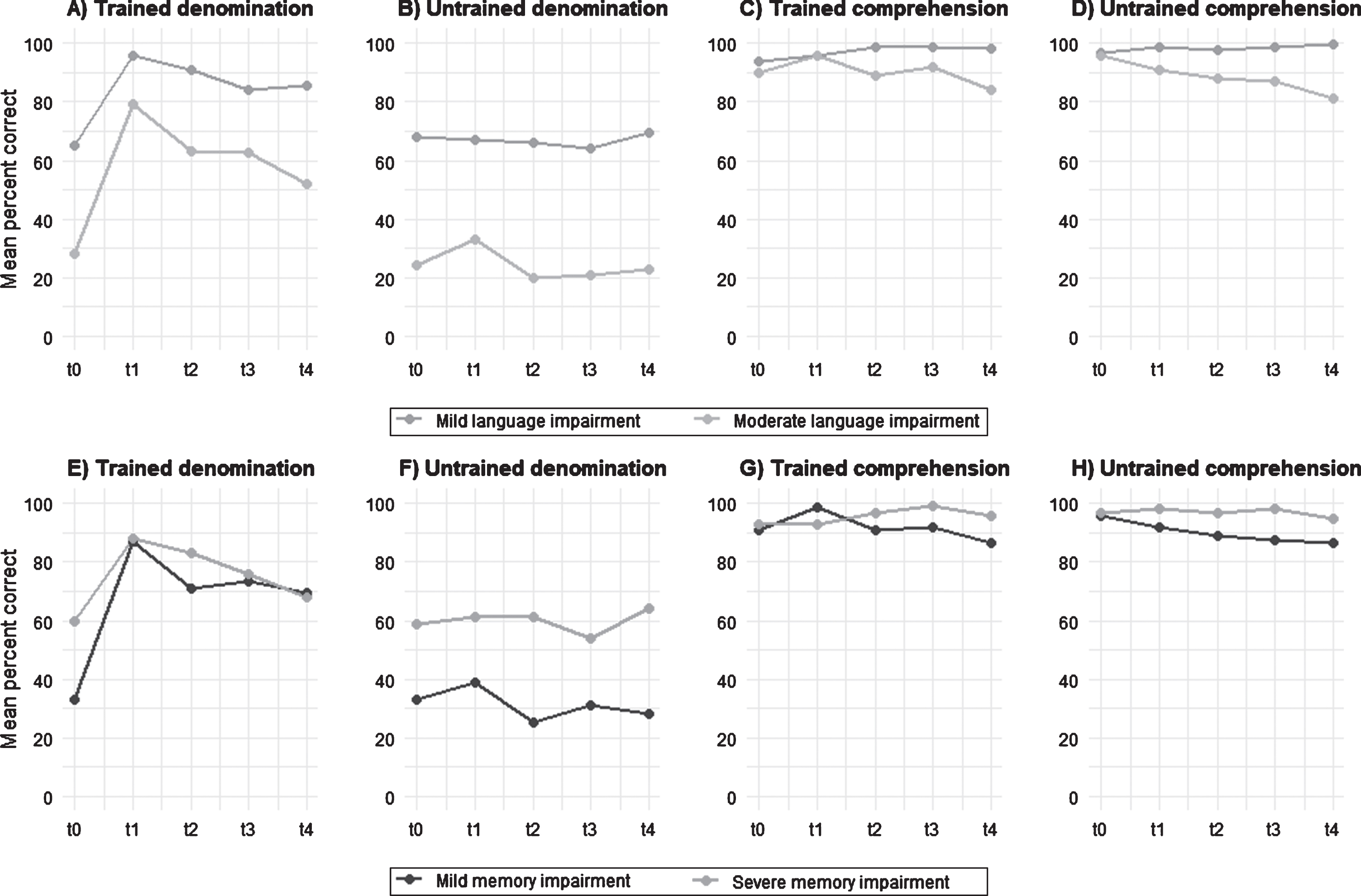
A–D) Individual percentages of correct answers at each assessment by evaluations. E–H) Mean percentages of correct answers at each assessment by evaluations. t0 = baseline; t1 = immediately postintervention; t2 = 1 month postintervention; t3 = 3 months postintervention; t4 = 6 months postintervention.
Tolerability and adverse events
The intervention was well tolerated. Only one patient, who trained at home without assistance, developed obsessive behavior about the words presented in the sessions. We also observed word intrusions from the training list in another patient, but the patient successfully corrected this without assistance.
DISCUSSION
In the present study, we assessed the effect of EL speech therapy on naming and category comprehension, which are two key language domains for patients with svPPA. There was a significant improvement in naming among the trained items, with this positive effect being maintained for at least 3 months after the intervention. However, there was no improvement in untrained items, suggesting a lack of generalization of the benefits. We also found no improvement in the comprehension tasks, but we cannot exclude the possibility of a ceiling effect in some participants.
Our findings are consistent with previous literature. An effect of language rehabilitation on picture naming has been reported for patients with svPPA [22, 23], while another study demonstrated that the reacquisition of lost vocabulary was possible through EL speech therapy for three patients with svPPA [24]. Jokel et al. have also suggested a possible benefit of implementing errorless strategies when comparing errorless and errorful learning approaches to anomia in seven participants with svPPA. They concluded that errorless therapy was more effective than errorful therapy [11]. In a series of experiments in a patient with svPPA, Jefferies et al. evaluated the circumstances under which speech therapy was most profitable. They concluded that their participant showed larger gains in phonological learning when item errors were minimized [12]. EL, which targets implicit memory, may therefore be more effective in patients who cannot utilize their semantic memory.
Research has been conducted to evaluate the maintenance of reacquired knowledge over time. Savage et al. demonstrated that, despite the progressive nature of svPPA, patients can preserve some improvement for at least 6 months [25]. By contrast, fewer studies have evaluated whether the effects of EL therapy are maintained over time. Robinson and colleagues evaluated the outcomes of EL therapy in two patients with svPPA immediately and at 1 month after the intervention [14]. During this month, no further speech therapy was offered, and although both participants showed improvement immediately after the intervention, only one had retained the improvement at the follow-up assessment. In our study, we observed no significant maintenance of improvement in any patient by 6 months, supporting the idea that the new information is not consolidated. This is probably due not only to deficits in consolidation circuits because of the loss of lateral temporal areas [25, 26] but also to the neurodegenerative nature of svPPA, which may affect the durability of rehabilitation effects.
Our findings indicate that patients with svPPA retain some ability to acquire new information [22, 24]. Neuroimaging studies also show that there is loss of temporal medial lobe grey matter in svPPA. These patients appear to have a better preserved hippocampal system, which is involved in episodic memory circuits, compared with their temporal neocortex, which is involved in the consolidation of learning into long-term semantic storage. These changes suggest that patients with svPPA can rely on episodic memory, and as a result, should be able to relearn information more efficiently than patients with other language presentations of Alzheimer’s disease [27]. Recent studies suggest that there is a potential differentiation along the longitudinal axis of the hippocampus that could explain this discordance: the anterior hippocampus may be more affected in svPPA, while the posterior hippocampus may be more affected in Alzheimer’s disease, correlating with episodic memory scores [10]. Thus, we hypothesize that patients with less memory impairment could benefit more from a speech therapy intervention. In support of this position we found a non-significant trend for better outcomes among patients with less severe memory impairment. This suggests that the benefit of the intervention may depend on the preservation of episodic memory circuits.
The benefit of the intervention in the present study was found to be independent of disease severity, with no significant differences in the maintenance of these improvements. This result indicated that patients with either mild or moderate aphasia can benefit from the speech therapy. Previous studies have suggested that relearning is dependent on the degree of residual semantic knowledge [13], and it is possible that we found no differences according to severity due to a ceiling effect in the mild group (with a high success rate after the intervention). Moreover, we did not identify any significant improvement in naming untrained items, and this lack of generalization has frequently been reported in previous work with patients with svPPA [28]. Finally, the lack of benefit with the comprehension tasks was affected by the high baseline success, which may have introduced a ceiling effect. Further studies with a higher requirement are needed to elucidate the effect of EL therapy on comprehension tasks.
Our study has some limitations. First, the small sample size unavoidably limits the generalizability of our results. Second, the lack of a control group of patients who did not receive therapy may have reduced the scale of any differences when comparing trained and untrained items. Finally, the low difficulty of the comprehension task could have masked the therapeutic effect by introducing a ceiling effect, which precludes meaningful conclusions about the impact on relearning words for comprehension.
In conclusion, our study shows that EL speech therapy on word relearning in svPPA may attenuate the progression of some language deficits, with benefits in word naming after intensive therapy. Therapy also tends to be more effective over time, especially in patients with mild impairments. Further studies are needed that employ larger cohorts and improved procedures to clarify the true efficacy of speech therapy in patients with svPPA.
Footnotes
ACKNOWLEDGMENTS
We are grateful to the patients and their families for generously donating their time and effort for this study. This research was supported by Pla Estrategic de Recerca I Innovació en Salut from Generalitat de Catalunya (PERIS SLT002/16/00408 awarded to RSV and PERIS 2016-2020, SLT008/18/00061awarded to AL). Fundació Marató de TV3, Spain (grant no. 20143810 to RSV).