
Abstract
Background:
Growing evidence suggests that chronic pain and certain chronic pain conditions may increase risk for cognitive decline and dementia.
Objective:
In this systematic review, we critically evaluate available evidence regarding the association of chronic pain and specific common chronic pain conditions to subsequent decline in cognitive function, new onset cognitive impairment (CI), and incident Alzheimer’s disease and related dementias (ADRD); outline major gaps in the literature; and provide a preliminary conceptual model illustrating potential pathways linking pain to cognitive change.
Methods:
To identify qualifying studies, we searched seven scientific databases and scanned bibliographies of identified articles and relevant review papers. Sixteen studies met our inclusion criteria (2 matched case-control, 10 retrospective cohort, 2 prospective cohort), including 11 regarding the association of osteoarthritis (N = 4), fibromyalgia (N = 1), or headache/migraine (N = 6) to incident ADRD (N = 10) and/or its subtypes (N = 6), and 5 investigating the relation of chronic pain symptoms to subsequent cognitive decline (N = 2), CI (N = 1), and/or ADRD (N = 3).
Results:
Studies yielded consistent evidence for a positive association of osteoarthritis and migraines/headaches to incident ADRD; however, findings regarding dementia subtypes were mixed. Emerging evidence also suggests chronic pain symptoms may accelerate cognitive decline and increase risk for memory impairment and ADRD, although findings and measures varied considerably across studies.
Conclusion:
While existing studies support a link between chronic pain and ADRD risk, conclusions are limited by substantial study heterogeneity, limited investigation of certain pain conditions, and methodological and other concerns characterizing most investigations to date. Additional rigorous, long-term prospective studies are needed to elucidate the effects of chronic pain and specific chronic pain conditions on cognitive decline and conversion to ADRD, and to clarify the influence of potential confounding and mediating factors.
Keywords
INTRODUCTION
Burden and epidemiology of Alzheimer’s disease and related dementias
Prevalence of Alzheimer’s disease and related dementias (ADRD), which encompass a range of progressive and devastating neurodegenerative disorders, continues to increase steeply in both developing and developed countries, paralleling the rapid aging of populations worldwide and constituting a serious and growing global public health crisis. A leading cause of disability, institutionalization, and death globally, ADRD imposes an enormous clinical, societal, and economic burden [1–3]. Even in high-income countries, the economic costs and associated societal burden of dementia threaten to overwhelm existing resources as the population ages and longevity increases [4].
The development of ADRD is generally insidious, with onset of clinical signs preceded years earlier by perceived and/or objective cognitive decline [5]. With effective disease-modifying treatments for cognitive impairment (CI) or ADRD still lacking after decades of disappointing clinical trials, research is shifting increasingly to prevention and early intervention [6, 7], with large-scale risk reduction trials now underway in multiple countries [7–11], including the U.S. [7, 12]. Although still incompletely understood, the development of late onset ADRD, which account for the vast majority of ADRD cases, is thought to reflect a complex interplay among multiple interacting factors, including those that are non-modifiable as well as those that are modifiable [3]. Most important among the former is age, with ADRD risk increasing exponentially with rising age [13]. For example, in the U.S., the percentage of adults with AD increases from 3% in those aged 65–74 to 17% in elders 75–84 and 32% in people 85 and older [3]. ADRD risk is also elevated in those with a family history of dementia and rises in a dose-dependent fashion with the presence of one or more APOE ɛ4 alleles [3, 14]. In addition, many studies have documented increased likelihood of ADRD in women and in African American and Hispanic adults, although some investigations suggest these disparities may reflect differences in socioeconomic, health-related, and other modifiable factors [3, 15].
In addition to these predisposing factors, a number of modifiable risk factors have also been linked to the development of CI and ADRD, providing potential opportunities for intervention. These include socioeconomic factors (e.g., low educational attainment [3, 17], unemployment [18, 19], and poverty [3]); lifestyle behaviors (e.g., smoking, physical inactivity, and mid-life obesity [3, 20–29]); and psychosocial factors, including depression [30–34], anxiety [31, 36], post-traumatic stress disorder [37–39], and other distressful states [40, 41], as well as sleep impairment [26, 42] and lack of social engagement [3, 25]. Several physical health conditions have also been linked to subsequent cognitive decline, CI, and ADRD, including: traumatic brain injury (TBI) and other head trauma [3, 43–45]; and history of specific chronic disorders, including hypertension in mid-life [3], diabetes [3, 47], heart disease [48, 49], chronic obstructive pulmonary disease (COPD) [50], and stroke [20, 49], as well as multimorbidity, the presence of multiple chronic conditions [51, 52]. In addition, certain medications have been linked to both increased and reduced risk for ADRD. For example, statin use has been consistently associated with reduced risk for dementia [53, 54]; conversely, benzodiazepines have been associated with elevated dementia risk in some studies [55, 56], although evidence for this association remains more equivocal [56–58]. Recent studies also suggest that polypharmacy may also increase risk for accelerated cognitive decline [59] and the development of dementia [60, 61].
However, while there has been considerable progress in identifying modifiable risk factors for ADRD, major knowledge gaps remain, hampering the development of effective prevention and treatment strategies. Important among these is our still limited understanding regarding the contribution of chronic pain and common chronic pain conditions to the development of CI and ADRD. Like ADRD, chronic pain continues to increase rapidly in prevalence worldwide, and itself poses a looming global public health crisis [62–65].
Chronic pain: Prevalence, burden, and relation to neurocognitive dysfunction
Chronic pain is a common and distressing condition associated with substantial clinical, economic, and societal burden in both developing and developed countries [66–68]. In the U.S., chronic pain affects up to 41% or more of the general population [67, 69–71] and up to 60% or more of older adults [72, 73], with prevalence continuing to increase [71]. Economic and social costs attributable to chronic pain are also high; for example, estimated excess annual healthcare costs in the U.S. range from $261–300 billion [74] and total costs, from $560 to $635 billion in 2010 dollars [75], far exceeding those for diabetes, hypertension, heart disease, cancer, and other common chronic disorders [73, 74]. Chronic pain can also lead to significant declines in productivity, physical function, quality of life, social engagement, and overall health, mood, and well-being [70, 76–78], and is a leading cause of disability both in the U.S. and globally [65, 79]. Moreover, as addressed in more detail in the discussion, many of these relationships are bidirectional, leading to a vicious cycle of increasing pain and social isolation, declining physical and mental health, disrupted sleep, and deterioration in mobility and function.
In addition, chronic pain can have significant effects on neurocognitive function. Because the neural systems involved in memory and cognition are closely linked to those involved in pain processing, these systems may affect one another reciprocally [76, 80] disrupting cognitive processing and contributing to a downward spiral of continuing pain, adverse neurostructural changes, and deteriorating cognitive function. Patients with chronic pain show changes in brain morphology paralleling those implicated in cognitive decline and CI, including grey matter volume reduction in brain regions involved not only in pain processing and emotional regulation, but in attention, memory consolidation, and cognitive processing [76, 80–84]. Chronic pain has also been shown to disrupt the functioning of the default mode network and other brain networks essential to normal cognitive function [82]. These alterations are thought to help explain the deterioration in memory and cognitive performance documented in many populations with chronic pain [76, 85], deterioration which may ultimately presage cognitive decline and the onset of CI and ADRD.
A growing body of evidence from epidemiologic studies suggests that chronic pain may be linked to subsequent cognitive decline, CI, and the development of ADRD. In this systematic review, we critically evaluate available evidence from published case-control and longitudinal studies regarding the association of chronic pain and specific common chronic pain conditions to incident dementia, as well as to adverse changes in cognitive function and new onset CI. We also outline major limitations and gaps in the current literature, provide a preliminary conceptual model illustrating potential pathways by which pain may influence cognitive change, and suggest directions for future research.
METHODS
To identify qualifying studies, we searched seven scientific databases, including Academic Search Complete, Scopus, MEDLINE, Pubmed, PsycARTICLES, and PsycINFO, as well as Google Scholar from their inceptions through February 2020 for original, peer-reviewed articles investigating the association of chronic pain or chronic pain conditions as a predictor of subsequent adverse changes in cognitive status. Search terms included (chronic pain or pain or arthritis or fibromyalgia or headache or migraine or rheumatic) AND (neurocogni* or neuropsych* or cogniti* or CI or memory or dementia or Alzheimer’s Disease). Titles and abstracts of the citations were scanned to identify potentially eligible articles for inclusion in this review. Potentially eligible papers were retrieved for more detailed review. In addition, we manually searched our own files, the citation sections of all identified articles, and the reference sections of recent review articles (2009–2020) regarding the relation of pain to cognition and/or dementia. Both authors reviewed the abstracts identified from the searches.
Original observational studies were included if they used longitudinal data to evaluate the association of chronic pain or common chronic pain conditions to subsequent changes in cognitive performance, new onset CI, and/or incident dementia. We excluded cross-sectional studies, studies that did not adjust at a minimum, for age and sex, studies for which the follow-up period was less than one year, as well as studies that were published only in dissertation or abstract form. We also excluded articles that were not published in English, compared only two clinical populations, included, as the major outcome variable, fewer than 50 cases, or did not report quantitative outcome data. In addition, studies assessing the association of rheumatological disorders to cognitive outcomes that did not distinguish types of arthritis were excluded from consideration. We also excluded studies regarding the relation of autoimmune and/or inflammatory rheumatic disorders (e.g., rheumatoid arthritis, systemic lupus erythematosus (SLE), ankylosing spondylitis, gout) to cognitive decline or dementia, as these relatively rare conditions are thought to be distinct in etiology and progression, and may thus differ in their effects on ADRD risk. We categorized into specific domains, both explanatory variables (specific individual chronic pain conditions, non-specific chronic pain symptoms) and cognitive outcomes (ADRD and specific ADRD subtypes, CI, and cognitive decline). For each domain, we summarized findings from relevant studies (with 95% confidence intervals), as well as indicators of external and internal validity. The latter included study design, sample size, data source, follow-up duration, study population selection procedures and characteristics, measures/assessment of pain/pain conditions and of cognitive outcomes, factors adjusted for in measures of association, attrition, and other information pertinent to study quality.
RESULTS
The initial literature search yielded 8,204 records. After removal of duplicates, a total of 7,176 potentially relevant records were scanned and 97 potentially eligible papers retrieved for full text review (Fig. 1). After excluding ineligible studies, a total of 16 papers reporting findings from 16 original studies, including two nested matched case-control studies [86, 87], 10 retrospective cohort investigations [87–94], and 4 prospective cohort studies [95–99] met our eligibility criteria and were included in the systematic review (Fig. 1). Table 1 provides a brief synopsis, and Table 2, a more comprehensive summary of the longitudinal studies identified for inclusion, detailing the characteristics, target outcomes, and (Table 2) key findings of each study, stratified by chronic pain measure. Identified studies were conducted in a total of five countries, including Taiwan (N = 7, all using the Taiwan National Health Insurance Research Database (NHIRD) [86–88, 100]), Japan (N = 1 [96]), the U.S. (N = 4 [94, 97–99]), Canada (N = 1 [89]), Norway (N = 2) [92, 95]), and England (N = 1 [101]). Study outcomes examined varied from all cause dementia/ADRD (N = 13 studies), Alzheimer’s disease (N = 8 studies), other dementias (N = 5 studies), and CI (N = 1 study) to measures of decline in cognitive function (N = 3), with 6 studies examining multiple outcomes (Table 1). Overall, 11 studies investigated the association of specific chronic pain conditions to dementia, including osteoarthritis (N = 4), fibromyalgia (N = 1), and headaches (N = 6) in a total of 701,593 adults (N = 26,327 AD/ADRD cases). Five investigations examined the relation of non-specific chronic pain symptoms to subsequent cognitive outcomes, including cognitive decline (N = 2), CI (N = 1), and dementia/dementia probability (N = 3).
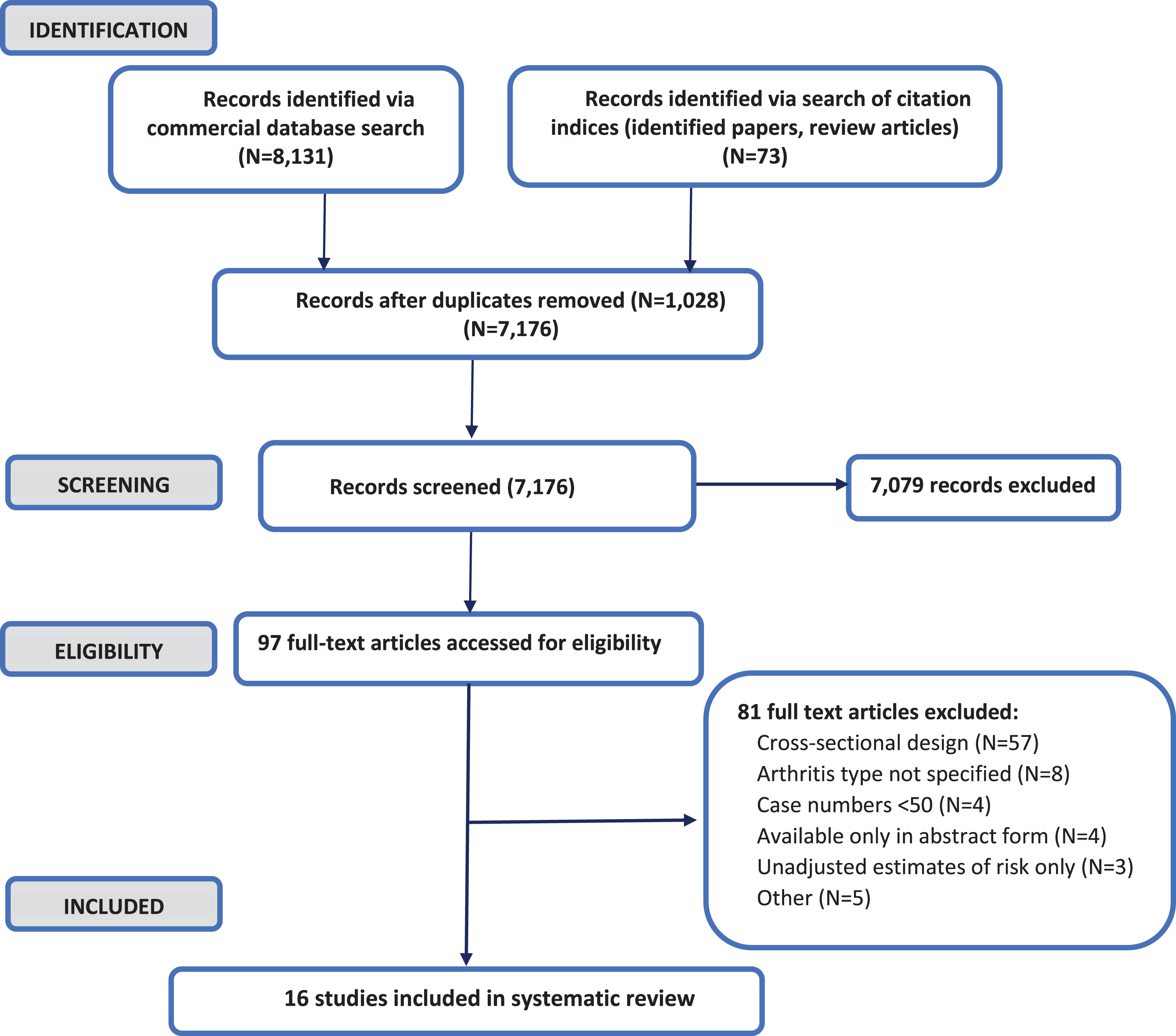
Study identification, screening, and selection for inclusion in systematic review.
Summary table of observational studies using longitudinal data to assess the relation of chronic pain and chronic pain conditions to subsequent cognitive decline and incident cognitive impairment and dementia
¬=Non-specific arthritis or ‘rheumatism’ (excluded from consideration) *Probability of incident dementia **Defined as self-reported presence and interference with daily activities ¬= ¬= in 2000 (end of baseline period). AD, Alzheimer’s disease; ADRD, Alzheimer’s disease and related dementias; CD, cognitive decline; CI, cognitive impairment; Dem, dementia; f/u, follow-up; PI, pain interference; Sev, severity/intensity; sx, symptoms; y, year; Y/N, Yes/No (presence).
Association of chronic pain conditions to incident dementias
Osteoarthritis (OA) (N = 4 studies)
A total of four studies, two matched case-control studies [86, 100] and two retrospective cohort investigations [87, 94], assessed the relation of OA to incident ADRD [87, 100] or AD [86] using longitudinal data. Studies included one investigation of U.S. Medicare beneficiaries enrolled in fee-for-service plans [94] and three large, population-based studies of Taiwanese nationals (total N = 201,495 adults, 15,018 AD/ADRD cases). All of the latter studies used the Taiwanese National Health Insurance Research Database (NHIRD) or the Longitudinal Health Insurance Database (LHID, a randomly selected sample of 1 million adults from the NHIRD (1996–2011)) as the primary study data source (2000/2001/2004 to 2010/2011). The maximum follow-up period ranged from 2 [94] to 10 years [86, 100] (Tables 1 and 2).
Observational studies using longitudinal data to assess the relation of chronic pain and chronic pain conditions to subsequent cognitive decline and incident cognitive impairment and dementia: characteristics and key findings
AD, Alzheimer’s disease; ADL, Activities of daily living; ADAMS, Aging, Demographics, and Memory Study; ADRD, Alzheimer’s disease and related dementia; ADRDA, National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association; AF, atrial fibrillation; AHR, adjusted hazards ratio; AOR, adjusted odds ratio; ARR, adjusted relative risk; avg, average; CI, confidence interval; COPD, chronic obstructive pulmonary disease; DM, diabetes; dx, diagnosis; EOS, end of study; excl, excluding; F, female; f/u, follow-up; HF, heart failure; hx, history; HT, hypertensive; IHD, ischemic heart disease; incl, including; LtF, lost to follow-up; MCR, motoric cognitive risk syndrome; mod/sev, moderate/severe; MI, myocardial infarction; NINCDS-NINDS-AIREN, Neurological Disorders and Stroke (formerly NINCDS) and Association Internationale pour la Recherché et l’Enseignement en Neurosciences; NR, not reported; OA, osteoarthritis; RA, rheumatoid arthritis; RR, response rate; SLE, systemic lupus erythematosus; SS, Sjogren’s syndrome; sx, symptoms; VaD, vascular dementia; w/o, without; y, years; *Virtually universal; **Reported to correlate well with independent. physician panel assessment. ¥’Has a doctor ever told you that you have Alzheimer’s?’. ¥¥Those responding to headache questionnaire were younger, more likely to be women, and had higher socioeconomic status versus non-responders. ¬= ¬= Those excluded at wave 4 due to missing data or death were significantly older, were more likely to report pain, and scored significantly worse in all cognitive tests at wave 2. ¬= ¬= ¬= Eligible participants were significantly younger and more educated versus those excluded.
In their retrospective matched cohort study of 105,447 Taiwanese adults ≥18 years (N = 1,070 with incident dementia), Huang and colleagues reported significantly increased risk for ADRD in those with a prior OA diagnosis after adjustment for age, sex, urbanization, and multiple comorbidities (adjusted hazards ratio (AHR)=1.25, 95% confidence interval (CI) 1.10,1.43) [87]. Consistent with these findings, in our recent retrospective cohort study of 16,934 Medicare beneficiaries ≥65 years (N = 1,149 with incident dementia), those with OA at baseline were significantly more likely to be diagnosed with incident ADRD at follow up after adjustment for sociodemographics, lifestyle characteristics, medications, multiple health conditions, and other factors linked to ADRD (Adjusted odds ratio (AOR) = 1.23, CI 1.06-1.42); this association was particularly pronounced in those with OA and accompanying pain (AOR versus no OA or pain = 1.31, CI 1.08-1.58), and appeared to be in part mediated by diagnosed anxiety and depression [94]. Likewise, findings of a large case-control study matched on age and sex (N = 71,260≥40 y, 10,180 with incident dementia) indicated significantly elevated odds of developing ADRD in those with diagnosed OA after adjustment for (unspecified) comorbidities (AOR = 1.47, CI 1.40–1.54) [100]. In contrast, in a nested case control of 7,854 older adults matched on age and sex showed little evidence of an association between OA alone and Alzheimer’s disease (AD), but reported elevated risk among those with both OA and osteoporosis (OR = 1.23, 1.07-1.41) [86].
Collectively, findings of these investigations suggest that older adults with OA may be at elevated risk for incident ADRD, although the association of OA to incident AD alone is less clear, especially given published data to date have been restricted to a single investigation, and findings were adjusted only for age and sex. Moreover, while findings support a potential link between OA and the development of dementia, interpretation is hampered by certain important limitations. These include short follow-up period [87, 94]; lack of information on cognitive trajectory, incident CI or specific dementia types [87, 100]; and failure to assess the influence of OA-associated pain [87, 100], evaluate the potential role of psychosocial factors [87, 100] or survival bias [87, 100], and/or control for several potential confounders known to affect cognition, including certain: lifestyle and demographic factors, chronic health conditions, and medications. In addition, all but one study to date have been conducted in Taiwanese nationals using a similar data source, potentially limiting generalizability to other populations.
Fibromyalgia (N = 1 study)
Our search identified only one published longitudinal study to date evaluating the association of fibromyalgia (FMS) to cognitive outcomes, a large retrospective cohort study of over 165,000 Taiwanese nationals [88]. In this retrospective cohort study, the authors examined the association of newly diagnosed FMS to incident dementia in a nationally representative sample of adults ≥50 years of age drawn from the LHID (N = 41,614 with, 124,836 without FMS, of whom 6,213 were subsequently diagnosed with incident dementia) (Tables 1 and 2); the follow-up period ranged from 1 to a maximum of 10 years. In this cohort of older adults, FMS was associated with significantly increased risk for all cause dementia (AHR = 2.77, CI 2.61–2.95) after adjustment for a broad array of factors, including demographics, diagnosed chronic physical and mental health conditions, including arthropathies and connective tissue disorders, history of stroke and head injury, and certain medications. Those with newly diagnosed FMS were also at substantially increased risk for incident AD (AHR = 3.35, CI 2.57–4.32), vascular dementia (3.14, CI 2.60–3.78), and non-vascular dementia 2.72, CI 2.55–2.90). Findings of this single study suggest that FMS may contribute significantly to the development of dementia and its common subtypes. However, while this large cohort study has a number of strengths, information is lacking on certain demographic characteristics, lifestyle factors, and medications associated with cognitive risk, as well as on cognitive trajectory and pain symptoms. In addition to generalizability concerns, additional limitations include short follow-up times for a subset of participants, as well as the possibility of misclassification of incident dementia in those diagnosed shortly after identification of FMS.
Headache (migraine and non-migrainous) (N = 6 studies)
A total of six published longitudinal studies assessing the association of headache to incident dementia met our inclusion criteria (total N = 319,023 adults, 4,704 with incident ADRD) (Table 1). These included three large, population-based retrospective matched cohort studies of Taiwanese nationals, all using data from the NHIRD-LHID [90, 93], two large cohort studies (one retrospective matched cohort and one prospective cohort) of Norwegian adults [92, 95], and a small retrospective cohort study of Canadian elders [89]. Of these, three investigations examined the relationship of any headache (including tension-type and migraine) to incident dementia [90, 92] and/or dementia subtypes [90, 95]; all suggested increased risk. In their retrospective matched cohort study of 14,480 Taiwanese nationals (603 incident ADRD), Tzeng and colleagues found adults with any newly diagnosed primary headache disorder to be at over two-fold increased risk for both incident dementia (AHR = 2.05, CI 1.71-2.46) and new onset non-vascular dementia (AHR = 2.11, CI 1.75-2.55) in competing risk analyses adjusted for a wide range of potential confounders (Table 2). Likewise, in a prospective study of 51,383 Norwegian adults (378 incident dementia cases) using linked Nord-Trondelag Health Survey (HUNT2, 1995-7) and Dementia Registry data (1997–2010), Hagen et al. reported a similarly increased risk for vascular and mixed dementia (HRs adjusted for age, sex education, and depressive symptoms = 2.3 (1.4–3.8) and 2.0 (1.1-3.5), respectively) in those with self-reported headache at baseline [95]. In contrast, the authors indicated only a modest elevation in risk for all cause dementia (OR adjusted for age and sex = 1.3, CI 1.1-1.7). A subsequent study restricted to survey participants who also completed the next wave (HUNT3) (N = 15,601 adults, 746 with incident dementia) yielded comparable findings after adjustment for age, sex, education, depressive symptoms, and severe comorbid conditions (AOR for dementia in those who reported any headache at baseline = 1.24, CI 1.04-1.49) [92]. While reasons for the differing risk estimates for dementia is unknown, discrepancies may reflect differences in sample size, study population and design, follow-up period, ascertainment of headache and dementia, analysis and included covariates, and other factors.
Five studies assessed the relation of specific headache subtype, including tension-type [90, 91]/non-migrainous [95] and migraine headache [89, 93] to risk for ADRD [89, 93] and/or specific ADRD subtypes [89–91] [95] (Tables 1 and 2). In a large retrospective cohort study of Taiwanese adults, newly diagnosed tension-type headache was associated with significantly increased risk for both incident dementia (AHR = 1.77, CI 1.41, 2.22) and non-vascular dementia (AHR = 1.88, CI 1.49,2.37) after adjustment for multiple potential confounders [90]. A second, larger Taiwanese study using the same data source likewise indicated significantly elevated risk for all-cause and non-vascular dementia in those with tension-type headache, although reported risk estimates were more modest (AHR = 1.15 (1.05-1.27) and 1.21 (1.09-1.34) [91]. In their prospective study of Norwegian adults, Hagen et al. also noted increased risk for vascular dementia in adults reporting non-migrainous headache at baseline (AHR = 2.1 (1.2–3.7) [95].
Similarly, all three studies assessing the relation of migraine to overall dementia risk indicated significant positive associations, although risk estimates again varied among studies (Table 2). For example, reported AHRs for dementia in those with newly diagnosed migraine varied from 1.33 (1.22-1.46) to 2.00 (1.57-2.53) in two large retrospective cohort studies of Taiwanese nationals [93], whereas a small retrospective cohort study of Manitoba residents indicated a 3-fold increased risk in those with self-reported migraine at baseline (AOR adjusted for age, education, and stroke = 2.97, CI 1.25-6.61) [89]. Three studies also provided support for a potential link between migraine and the development of other forms of dementia, including non-vascular dementia [89, 90] and vascular dementia [95], although findings varied across studies (Table 2). Notably, of the four studies [89–91, 95] that examined the relation of any headache to incident dementia subtypes, only one reported a significant association of headache to vascular dementia [95], and only one indicated an increased risk for AD [89].
Collectively, these findings support a link between headache and subsequent risk for ADRD, with two studies suggesting an increased risk for incident vascular dementia in those diagnosed with headache at baseline.
Association of chronic pain symptoms to cognitive decline, cognitive impairment, and dementia
We identified five studies using longitudinal data to investigate the relation of chronic pain symptoms to subsequent cognitive decline [99, 101], new onset CI [97], or incident dementia [96, 98]/dementia probability [99]; three were conducted in U.S. populations [97–99], with the remaining two studies based on data from Japanese [96] and British [101] cohorts. While providing support overall for a link between chronic pain and risk for adverse cognitive outcomes, findings differed across studies, likely due in part to discrepancies in study design, population, measures, length of follow-up, attrition, and other factors. For example, a survey study of 10,065 older U.S. adults followed for up to 12 years, indicated a modest association between persistent pain and acceleration in both overall cognitive decline and probability of dementia. Broadly consistent with these findings, pain interference, although not pain intensity, was associated with significantly increased risk for dementia in a retrospective cohort study of 1,114 adults (114 new dementia cases) followed for an average of 4.4 years [98]. Conversely, studies in a representative sample of British adults (N = 6,515) [101] and a small U.S. cohort (N = 441) [97] followed an average of 2.75 [97] to 4 years [101] suggested a link only between high pain severity and deterioration in memory but not in other cognitive domains. A recent investigation of 14,627 elderly Japanese applicants to a national long term care program followed up to 3 years (482 with incident dementia), self-reported knee pain, but not back pain at baseline were associated with significantly increased risk for incident dementia after adjustment for demographics, lifestyle factors, social interaction, and certain physical and mental health conditions (AHR = 1.32, CI 1.06-1.64) [96].
While collectively, these studies suggest that chronic pain may accelerate cognitive decline and increase risk for CI and dementia, findings remain somewhat mixed and several factors limit conclusions. The latter include small sample sizes [97, 98] as well as the lack of adjustment for certain lifestyle characteristics and comorbidities associated with chronic pain and ADRD, potential self-report and/or survival bias, and the relatively short follow-up periods characterizing most studies. Pain was ascertained based on a single question in 3 of the 5 studies identified; in the one study reporting largely negative findings, associations may have been attenuated by adjustment for chronic pain conditions—notably arthritis, the major contributor to pain in this population, as well as by attrition bias and other factors.
DISCUSSION
Together, findings of studies to date suggest that chronic pain and certain chronic pain conditions may increase risk for the development of ADRD. Of the 10 studies assessing the relation of OA [87, 100], FMS [88], or headache [89–91, 95] [91–93] to risk for incident ADRD, all have yielded significant positive findings despite variation in study design, population, length of follow-up, and methodology. Specifically, as detailed above, recent large retrospective matched cohort studies in Taiwanese nationals [87, 100], a retrospective cohort study of U.S. Medicare beneficiaries [94], prospective cohort studies in Norwegian adults [92, 95], and a small retrospective cohort investigation of Manitoba residents [89] reported significantly increased risk for incident all cause dementia in those diagnosed with OA [87, 100], FMS [88], and headache [89–93, 95] after adjustment for demographics, comorbidities, and other factors. While longitudinal investigations examining the relation of chronic pain symptoms to adverse cognitive outcomes remain few, and studies have varied widely in design, study population, measures, length of follow-up and other factors, overall findings likewise suggest that persistent pain [99], severe chronic pain [97, 101], and/or reported pain interference [98] may predict subsequent deterioration in memory [97, 101], accelerated cognitive decline [99], and dementia [98, 99].
In contrast, findings regarding the association of chronic pain conditions to specific forms of dementia have been mixed. For example, while a large retrospective cohort study of Taiwanese nationals reported significantly elevated risk for incident AD in older adults with FMS [88], the single study of OA and AD risk suggested no relation [86], nor did three of the four studies of headache that included AD as an outcome [90, 95]. Likewise, of the five studies examining the association of FMS [88] or headache [89–91, 95] to incident vascular dementia, two studies reported significantly increased risk for vascular dementia in association with newly diagnosed FMS [88] or self-reported headache [95] at baseline, whereas the remaining three studies, including two in large samples of Taiwanese nationals [90, 91], found no evidence for an association of any headache type to vascular dementia risk [89–91].
In brief, as detailed above, findings of existing published studies of longitudinal data suggest that chronic pain and specific chronic pain conditions may contribute significantly to the subsequent deterioration in cognitive function and conversion to ADRD. However, conclusions are limited by a number of concerns. These include heterogeneity in study design, population, and methodology, as well as the short duration of follow-up, small sample sizes, potential self-report, detection, survival or other attrition bias, and/or incomplete adjustment for potentially confounding factors characterizing most studies. While external validity can generally be considered high in those studies based on large, nationally, or regionally representative samples, relatively low response rates, high attrition, and/or high missing data rates may have led to selection bias in some cohort studies, potentially influencing both internal and external validity of findings.
Future directions for research and preliminary conceptual model
Research regarding the relation of chronic pain and chronic pain conditions to subsequent cognitive decline and conversion to CI and dementia remains relatively sparse, and that regarding the potential relation of certain chronic pain conditions (i.e., FMS) or specific chronic pain manifestations (e.g., chronic knee or back pain) to any cognitive outcome is currently restricted to single studies. To our knowledge, no investigations have yet examined the potential link between certain common chronic pain manifestations, including neck pain and neuropathic pain, to any adverse cognitive outcome or examined the relation of any pain condition to the entire cognitive trajectory, from cognitive decline to dementia. Moreover, of the 11 studies examining the association of common chronic pain conditions to incident dementia, 7 were conducted in Taiwan using the same data source. Additional rigorous prospective studies in other regions and populations are thus clearly needed to confirm and extend the findings detailed above. These include studies designed to: investigate the independent influence of specific pain conditions and associated chronic pain symptoms on subsequent cognitive decline, new onset CI, and conversion to dementia; assess the effects of pain chronicity, intensity/severity, and overall burden (including sites affected) on these associations; evaluate the potential mediating role of mood impairment, sleep deficits, and other psychosocial factors; assess the possible modifying effects of these and other ADRD risk factors on the relation of chronic pain and chronic pain conditions to adverse cognitive outcomes; identify underlying mechanisms and, and ultimately, explore the potential role of effective chronic pain management approaches in buffering the putative adverse long term effects of chronic pain on cognitive function.
Moreover, given that the development of ADRD is insidious and that both chronic pain and ADRD are influenced by a constellation of interacting factors, large, long term prospective studies that take into account the role of the multiple potentially confounding and mediating factors are clearly needed. Figure 2 provides a preliminary conceptual model to help guide future epidemiologic research, illustrating specific key interacting pathways by which chronic pain and chronic pain conditions may contribute to cognitive decline and the development of CI and dementia and the factors linked to both chronic pain and ADRD risk that warrant consideration in causal models. While other psychosocial factors, including pain catastrophizing, self-efficacy, and coping strategies may also play a mediating role, emphasis in this conceptual model is on those factors for which information is generally available in large clinical, government, insurance, and other existing databases.

Conceptual Framework: Possible pathways by which chronic pain and chronic pain conditions may contribute to the development of cognitive decline, cognitive impairment, and ADRD. Hx, history; CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; ADRD, Alzheimer’s disease and related dementias.
Link between chronic pain and adverse cognitive outcomes: Potential explanatory factors and underlying mechanisms
As illustrated in Fig. 2, chronic pain and chronic pain conditions may influence cognitive outcomes via multiple pathways. As summarized below, these pathways include both non-modifiable and modifiable factors linked to chronic pain and ADRD risk and are complex, interacting, and multidimensional.
Non-modifiable factors include increasing age and female gender, factors strongly and positively linked to risk for both chronic pain [15, 102] and dementia [3], as well as to certain risk factors for these conditions [3, 103–107]. In addition, black adults have been reported to be at elevated risk for ADRD [3] and to experience more frequent, severe, and disabling pain [108] relative to Caucasians, although other studies have found little or no evidence for this association after adjustment for socioeconomic status [15, 102].
Modifiable factors include multiple demographic/socioeconomic, lifestyle, and health-related risk factors. As illustrated in Fig. 2, most of the relationships of these factors to chronic pain and ADRD risk are likely reciprocal. Moreover, many of these risk factors may interact in a synergistic fashion to exacerbate risk for both pain and ADRD, contributing to a vicious cycle of increasing pain and pain-related dysfunction, deteriorating mood and sleep, reduced social engagement and physical activity, declining socioeconomic status and physical health, and increased use of medications, including those with documented adverse effects on cognitive health. Key demographic/socioeconomic factors include low educational level, poverty, unemployment, and social deprivation, which have been associated with significantly increased risk both for ADRD [3] and for chronic pain and specific chronic pain conditions [15, 102].
Lifestyle factors linked to increased risk for chronic pain and/or chronic pain disability include obesity [15, 109], physical inactivity [15, 109], poor diet [109], and social isolation/loneliness [110–112], as well as smoking [109], alcohol misuse [15], and substance abuse [113–115], factors which can contribute directly or indirectly to elevated risk for cognitive decline and the development of dementia [3, 116]. Moreover, most of the relationships between lifestyle factors and chronic pain/chronic pain disability are likely bidirectional [117, 118].
A number of physical and mental health conditions have also been linked to chronic pain and pain-related disability. These include diabetes [119–121], hypertension [122, 123], cardiovascular disease [15], COPD [15], and history of TBI [85] and stroke [124, 125], as well as multimorbidity [15]. As detailed above, these conditions have, in turn, been associated with increased ADRD risk [3, 46–52]. In addition, chronic stress [109], depression [15, 126–128], anxiety [15, 128], and sleep impairment [129, 130] can both result from and exacerbate chronic pain. These factors have also been significantly associated with cognitive decline [33, 132] and incident dementia [35, 132–135], and may in part mediate the observed relationships between chronic pain and the subsequent accelerated deterioration in cognitive function and development of ADRD [83, 94]. Finally, chronic pain often leads to the use of certain medications, including analgesics, benzodiazepines, and specific anti-depressants, factors which have been linked to ADRD risk in some [55, 56], although not all studies [56–58]. Chronic pain has also been associated with polypharmacy [136–138], an emerging risk factor for dementia [61].
Link between chronic pain and adverse cognitive outcomes: Possible underlying mechanisms
As noted above, chronic pain can also have profound effects on neurocognitive function, with potentially significant implications for the development of CI and conversion to ADRD. In a recent review of 53 studies of cognitive performance in chronic pain populations, the authors concluded that chronic pain was related to deficits in several key neurocognitive domains, including memory, attention, and processing speed, and, albeit less consistently, executive functioning [85]. The neural systems involved in memory and cognition are closely linked to those involved in pain processing and likely affect one another reciprocally [76, 80], disrupting cognitive processing and contributing to a vicious cycle of continuing pain, adverse neurostructural changes, and deteriorating cognitive function [83]. Patients with chronic pain show changes in brain morphology paralleling those implicated in cognitive decline and CI, including grey matter volume reduction in the hippocampus, insular cortex, anterior cingulate cortex, thalamus, prefrontal cortex, and other brain regions involved in attention, memory consolidation, and cognitive processing [76, 139]. Chronic pain has also been shown to disrupt specific brain networks critical to normal cognitive performance [82]. As noted above, these alterations are thought to help explain the deterioration in cognitive function documented in many chronic pain populations [76, 85], deterioration which may ultimately contribute to accelerated cognitive decline and the development of CI and ADRD.
Chronic pain and chronic pain conditions may contribute to ADRD pathogenesis via other pathways as well. For example, OA and other chronic pain conditions have been associated with activation of central pain processing pathways [140, 141] and central nervous system hypersensitivity [141, 142], factors linked to disruption of cognitive functioning [76, 143]. Both systemic and peripheral inflammation may also play a role. For example, systemic increases in high-sensitivity C-reactive protein, interleukin-6, and other proinflammatory mediators have been implicated in the development and progression of both specific chronic pain conditions (e.g., OA, FMS) and CI [141, 144]. Likewise, local proinflammatory changes associated with chronic pain conditions have been linked to neuroinflammation [141, 144], cerebrovascular dysfunction [144], and adverse nociceptive and structural changes in the brain [141, 145], alterations that may impair cognitive processing and promote cognitive dysfunction [141, 146]. Chronic pain may also contribute to ADRD risk via adverse effects on cellular aging. For example, OA [147] and other chronic pain conditions [148] have been associated with shortened telomere length, a marker of accelerated cellular aging that has been linked to increased risk for ADRD [149–151].
Strengths and limitations
Our review included only studies that used longitudinal data, reported a minimum of 50 outcome cases, and that adjusted, at a minimum, for age and gender, helping to increase confidence in findings. In the tables provided, we include information on multiple domains of study quality, and take into account design and methodological limitations in our discussion of findings. However, this systematic review also has several potential limitations that warrant consideration. While studies were identified using a comprehensive, multi-pronged search strategy, our review was restricted to investigations published in English, potentially introducing bias. However, we did not identify any research published in non-English languages that met our inclusion criteria, reducing this likelihood. Publication bias may have resulted in disproportionate capture of studies reporting positive findings. However, pain is not yet an established risk factor for cognitive decline or ADRD, rendering this possibility less likely. Studies have, to date, been conducted in only a handful of countries, and the majority (7 of 11) of studies investigating the association of included chronic pain conditions were conducted in Taiwanese nationals using the same primary data source. It thus remains unclear if the findings discussed in the current review are generalizable to other populations, cultures, and/or regions. While overall, the investigations published to date have yielded results supportive of a link between chronic pain and the development of cognitive decline and dementia, the considerable heterogeneity in study populations (notably, those assessing the association of chronic pain symptoms to cognitive outcomes), design, follow-up periods, measures and ascertainment of outcome and explanatory variables, analysis, and other factors render direct comparisons across studies challenging. As detailed above, conclusions are limited by a number of design and/or methodological concerns characterizing the majority of studies, including small sample sizes; relatively short follow-up periods; lack of adjustment for the potential confounding influence of specific demographic, lifestyle, and health-related factors associated with both pain and dementia risk; potential selection, self-report, detection, and/or survival bias; and/or lack of information on pain chronicity, duration, intensity or other indicators of chronic pain burden.
Conclusions
Published case-control and cohort investigations to date suggest chronic pain and certain chronic pain conditions may increase risk for accelerated cognitive decline, new onset CI, and incident ADRD. However, research remains sparse, and interpretation of existing findings is hampered by the methodological and other limitations characterizing most studies. The relation of chronic pain and chronic pain conditions to specific forms of dementia also remains unclear. Additional large prospective investigations that address these concerns are needed to confirm and extend the findings of current studies, to elucidate the contributions of chronic pain and chronic pain conditions on the entire cognitive trajectory, to clarify the relation of chronic pain to specific dementia types, and to explore potential mediating factors and identify underlying mechanisms.
Footnotes
ACKNOWLEDGMENTS
This work was performed at West Virginia University, and was supported in part by the Alzheimer’s Research and Prevention Foundation and the National Institute of General Medical Sciences of the National Institutes of Health (Award Number 2U54GM104942). The contents are solely the responsibility of the authors and do not represent the official views of the Alzheimer’s Research and Prevention Foundation or the National Institutes of Health.