
Abstract
Background:
Recently, subjective cognitive decline (SCD) has been considered to be one of the first signs of Alzheimer’s disease (AD). Since this potential early marker is sensitive but not specific to AD, combining it with other markers could ensure higher accuracy when predicting which persons with SCD will convert to AD. Since olfactory dysfunction is observable in both AD and mild cognitive impairment (MCI), it is a promising marker that could help improve the early diagnosis of AD.
Objective:
The aim of this meta-analysis was to verify whether the presence of SCD is associated with a decrease in olfactory identification ability.
Methods:
We collected articles from the following databases: PsychNet, PubMed, Ebsco, and ProQuest using the keywords: “SCD”, “subjective cognitive decline”, “subjective cognitive impairment”, “subjective memory impairment”, “subjective memory decline”, “cognitive complaints”, “memory complaints”, “cognitive concerns”, “memory concerns”, “olfac*” and “smell”. We included articles according to the following criteria: 1) participants aged 50 and over; 2) presence of an SCD group or a conceptual equivalent; 3) presence of a healthy control group with the same age range; and 4) assessment of olfactory identification ability.
Results:
Five studies met the inclusion criteria. Small and homogeneous effects were observed for olfactory identification alteration in individuals with SCD relative to controls (g = –0.16, 95% CI [–0.46, 0.14]).
Conclusion:
Despite the low number of studies included, the findings suggest that odor identification is slightly altered in SCD compared to healthy older adults. This alteration in individuals with SCD could be an early marker of AD.
Keywords
INTRODUCTION
In 2017, approximately six million Americans were diagnosed with clinical Alzheimer’s disease (AD) or mild cognitive impairment (MCI) due to AD pathology and this number is expected to rise up to 15 million by 2060 [1]. AD is a neurodegenerative disease characterized by the accumulation of amyloid-β plaques and tau neurofibrillary tangles in the brain that lead to dementia. Given the difficulty of measuring these brain markers in vivo, the probable diagnosis of AD is solely based on clinical criteria and usually occurs at the dementia stage [2]. However, AD has a long progression and begins with a preclinical phase, lasting decades, during which brain damage occurs [3]. This preclinical phase of AD ends with the development of MCI, which is characterized by cognitive impairments in one or more cognitive domains, most commonly in episodic memory in patients who will convert to AD dementia [4, 5]. During the preclinical phase, the brain damage could express itself as subjective cognitive decline (SCD). SCD is subjective because, at this stage, the level of cognitive performance remains within normal range on classical clinical assessments [6]. Nevertheless, in individuals with SCD from the Consortium pour l’identification précoce de la maladie d’Alzheimer - Québec (CIMA-Q) cohort, hippocampal volume was linked to a decline in episodic memory performance, a relationship that was not present in healthy older adults [7]. However, although SCD is a sensitive marker for AD, it remains poorly specific. Not all cases of SCD will develop MCI or dementia [8] and combining other earlier symptoms with SCD might be an opportunity to increase the specificity of the early diagnostic of AD. One potential sign is the olfactory dysfunction, which is a clinical marker of AD.
Several meta-analyses have shown that olfactory function is impaired in patients with AD, with the identification and recognition of odors being the more impaired functions [9, 10]. A similar impairment in the ability to identify odors was also found in MCI [11–15]. Since MCI is considered as an early clinical stage of dementia [5], with a variable annual conversion rate from MCI to AD dementia of 7.5 to 16.5%[16], researchers have investigated the possible role of olfactory dysfunction as a predictor for the conversion from MCI to AD. Combined with other markers (informant report of functioning, verbal memory, hippocampal and entorhinal cortex volume), olfactory identification performance helped strongly predict conversion from MCI to AD after a 3-year follow-up [17]. In another study, MCI patients with pathological olfactory identification at baseline were more likely to develop dementia after a 2-year follow-up [18]. When looking into different MCI subtypes, a population-based study showed that impaired olfactory identification was associated with amnestic MCI (aMCI) incidence, but not with non-amnestic MCI (naMCI) [19]. In the same study, olfactory identification scores strongly predicted progression from aMCI to AD which suggests that olfaction is more altered in aMCI than in naMCI and could be used as a marker of AD in MCI.
Longitudinal cohort studies on healthy community-dwelling older adults showed that olfactory dysfunction can predict cognitive decline. In cognitively healthy older adults, reduced olfactory function at baseline has been related to cognitive decline [20, 21], to a bigger proportion of conversion to MCI [22] and to a higher risk of developing dementia [23]. Moreover, a longitudinal study including 1,037 cognitively healthy older adults at baseline showed that olfactory identification is a better predictor than verbal episodic memory to predict cognitive decline in the transition to MCI [24]. Overall, these findings suggest that olfaction could be an early marker for cognitive decline in the preclinical stages of AD. These findings are in line with Murphy’s model (2019), which suggests that olfactory decline is one of the earliest clinical markers of AD, beginning at a stage when people are still cognitively within the norm [25], which might correspond to the SCD stage. Over the past decade, researchers have studied olfaction in SCD or a conceptually equivalent clinical entity. However, no consensus has been reached on whether the olfactory decline found in MCI and dementia is already detectable in this stage of the disease.
No meta-analyses have addressed olfaction in SCD. Thus, whether olfactory decline begins at the MCI stage or earlier remains unclear. The aim of this meta-analysis is to assess whether SCD is associated with a decrease in the ability of olfactory identification. In other words, we aim to address the following question: Do individuals with SCD have a reduced olfactory identification ability compared to healthy older adults?
METHODS
The protocol of this meta-analysis was not registered.
Eligibility criteria of the studies selected
To be eligible to be included in this meta-analysis, studies had to compare olfactory identification capacity between an SCD group and a healthy control group without cognitive complaint, with both groups comprising men and women aged 50 years and older.
Participants included in the SCD group had to report complaints of cognitive decline while having normal cognitive performance. There are two criteria to establish that an individual is experiencing a SCD: 1) subjective perception of cognitive decline relative to previous performance level; 2) a normal level of cognitive performance as assessed by valid cognitive tests such as the Mini-Mental State Examination (MMSE) [26], the Montreal Cognitive Assessment (MoCA) [27], or other cognitive tests that are used to exclude MCI [6]. Thus, studies where participants met both criteria of SCD were included in the meta-analysis. Given that the SCD term was only recently established in 2014 by the SCD-Initiative working group [6] to describe individuals that are at risk of developing cognitive decline or dementia, and since memory complaint is the most frequent cognitive complaint reported, other terms such as subjective cognitive impairment, subjective memory complaint or subjective memory impairment were used to characterize these individuals. Thus, all studies assessing olfactory identification in individuals with cognitive complaint and normal scores on classical cognitive tests were included in the meta-analysis.
Participants in the control groups were healthy individuals of 50 years of age and over with no objective cognitive impairment (> –1.5 SD score on cognitive tests), as measured by a valid cognitive assessment, and did not self-report any complaints of cognitive decline. General exclusion criteria for both groups included: 1) being under 50 years of age, 2) presenting a cognitive impairment, and 3) having any psychiatric diagnosis or other neurological condition that could affect cognition.
Outcome
To be included in the meta-analysis, studies had to measure the sense of smell through a score obtained in a behavioral examination using validated olfactory identification tests such as the Sniffin’ Sticks Identification Test [28], the Odor Percept Identification Test [29], the University of Pennsylvania Smell Identification Test (UPSIT) [30], and the Cross-Cultural Smell Identification Test (CC-SIT) [31].
Search strategy and information source
We searched for studies published up to July 2020. No studies were excluded from our meta-analysis because of their country of origin.
We searched for published studies in the following databases: PsychNet, PubMed, and Ebsco. The ProQuest Dissertations and Theses database was used to find unpublished theses. The following keywords were used in our search: “SCD”, “subjective cognitive decline”, “subjective cognitive impairment”, “subjective memory impairment”, “subjective memory decline”, “cognitive complaints”, “memory complaints”, “cognitive concerns”, “memory concerns”, “olfac*” and “smell”. After excluding duplicate studies, 322 titles and abstracts were reviewed (Fig. 1). Studies were excluded when they were off-topic (e.g., animal studies, assessment of other sensory modalities, absence of SCD group, etc.), reviews, case studies, qualitative papers or if they did not include a control group. This screening identified 18 potentially eligible studies.
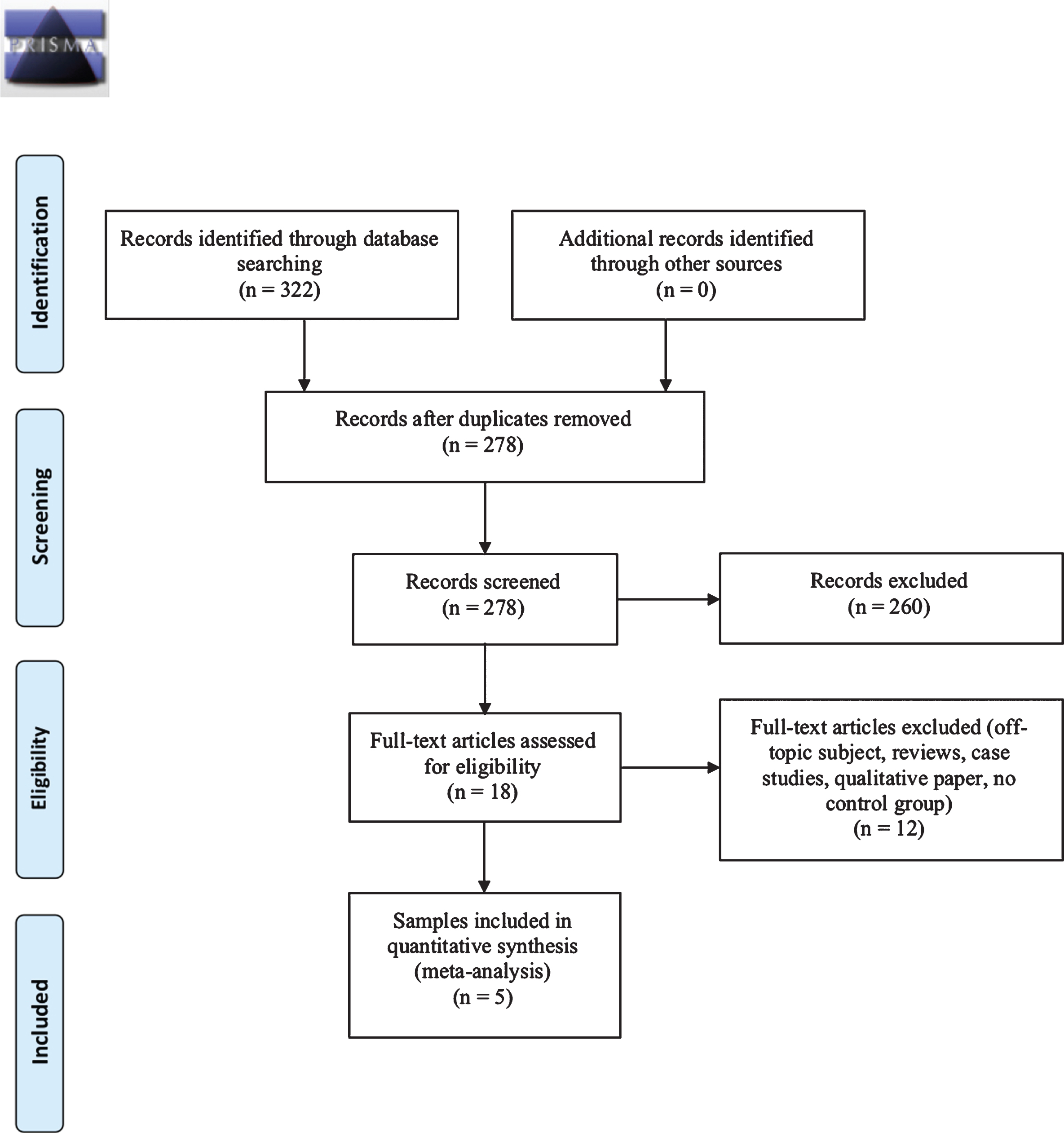
PRISMA flowchart illustrating the selection of studies.
Study selection
The first author (BJ) evaluated all of the selected studies to assess their eligibility according to the criteria mentioned above. He then sent the list of potentially eligible articles to a research assistant who was blind with respect to the purpose of this meta-analysis. An article was only included if it was approved by both evaluators based on the risk of bias assessment.
Risk of bias in individual studies
Risk of bias for each of the selected studies was assessed independently by two evaluators [BJ and AR] according to the Newcastle-Ottawa Scale (NOS) [32]. The NOS is a scale used to evaluate the quality of non-randomized case-control studies published in meta-analyses (i.e., evaluation of participants’ selection, comparability between groups, ascertainment of olfactory identification), which was recommended by Zeng and colleagues in 2015 [33]. A consensus was reached after pooling the results (Table 2). A score between 0 and 3 was considered a high risk of bias, between 4 and 6 a moderate risk of bias, and between 7 and 9 a low risk of bias. When disagreement emerged at this stage, it was agreed that the most conservative result would be selected. No major disagreement emerged and no studies were excluded following this evaluation.
Risk bias assessment of included studies
OI, olfactory identification; OPID, Odor Percept Identification; UPSIT, University of Pennsylvania Smell Identification Test; SSIT, Sniffin’ Sticks Identification Test; CC-SIT, Cross-Cultural Smell Identification Test; NOS, Newcastle-Ottawa Scale.
Analyses
Analyses were performed using Meta-Essential [34]. For each study, Hedges’ g was calculated to obtain a standardized effect size. When an article did not contain means and standard deviations, we calculated them when possible. When it was not possible, we contacted the authors to obtain the missing data. One author has been contacted and confirmed that two studies [35, 36] used the same sample and provided us the data of the full sample. The combined effect size was then calculated. According to Brydges [37], Cohen’s guidelines [38] are probably overestimated average effect sizes in gerontology. After analyzing 88 meta-analyses in gerontology, he suggests that a g = 0.16 can be interpreted as a small effect size, g = 0.38 as a medium effect size and g ≥ 0.76 as a large effect size. Finally, the more conservative random effects model has been used to compute the significance level of the mean effect sizes for each study since selected studies are not functionally 100%equivalent (i.e., not every study used the same olfactory identification test and the same exact design).
Risk of bias across studies
To quantify heterogeneity in effect sizes, we used Cochrane’s Q-statistic [39]. We assumed heterogeneity if PQ was significant at p < 0.05. Then, the testing of potential moderators, such as age, sex and type of olfactory identification tests, was allowed if there was presence of heterogeneity. I2 was generated to quantify the degree of heterogeneity among studies. Thus, the decision to test potential moderators or not was not only based on a significance test, which could be underpowered with a small number of studies.
Publication bias was assessed using the visual inspection of the funnel plot and confirmed using Begg’s rank test and Egger’s regression test [40, 41].
RESULTS
Study selection and characteristics
After analyzing full-text articles, six were eligible for extraction of quantitative data (Fig. 1). Two studies used the same sample, therefore the entire sample was used and counted for one study. Thus, five studies (samples) met the criteria for a total of 264 participants with SCD and 334 controls (Table 1). According to study quality assessment, no studies were excluded for a high risk of bias (i.e.,<3 on NOS scale) (Table 2). In all studies, the two compared groups were reported as equivalent in terms of age, and a significant difference on sex distribution was only found in one study [42].
Characteristics of studies included in the meta-analysis
OPID, Odor Percept Identification; UPSIT, University of Pennsylvania Smell Identification Test; SSIT, Sniffin’ Sticks Identification Test; CC-SIT, Cross-Cultural Smell Identification Test. Tahmasebi et al., 2019 data set was provided by the authors and has been used in both Tahmasebi et al., 2019 [35] and Tahmasebi et al., 2019 [36] articles. aMedian (25th percentile/75th percentile).
Main effect
The aim of this meta-analysis is to determine whether identification olfactory ability is altered in SCD compared to healthy older adults. The analysis reveals a small effect size (g = –0.16, 95%CI [–0.46, 0.14]; k = 5) that was not significantly heterogenous (Q = 5.72, pQ = 0.23) (Fig. 2). The homogeneity of the effect sizes was also confirmed with a second indicator (I2 = 30.0%). Thus, moderator analysis was not necessary.
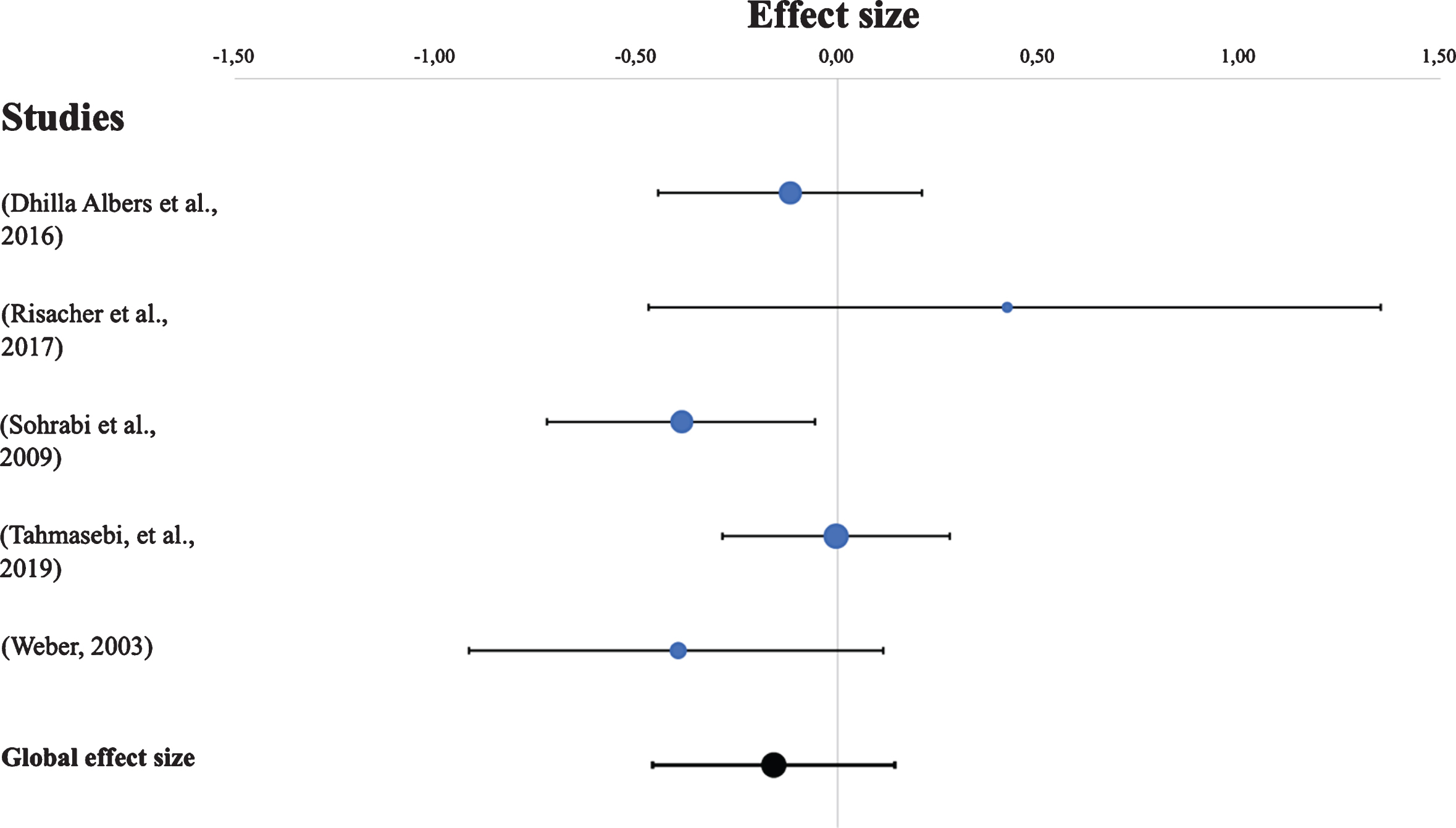
Forest plot of effect sizes. Error bars represent 95%CIs.
Publication bias
We did not performed regression-based analysis due to the insufficient number of included studies (5). Thus, a funnel plot was generated (Fig. 3). Asymmetry at the bottom (right) of the funnel plot may be due to a possible publication bias. This asymmetry suggests caution in interpretation of the results, until more studies have been conducted.
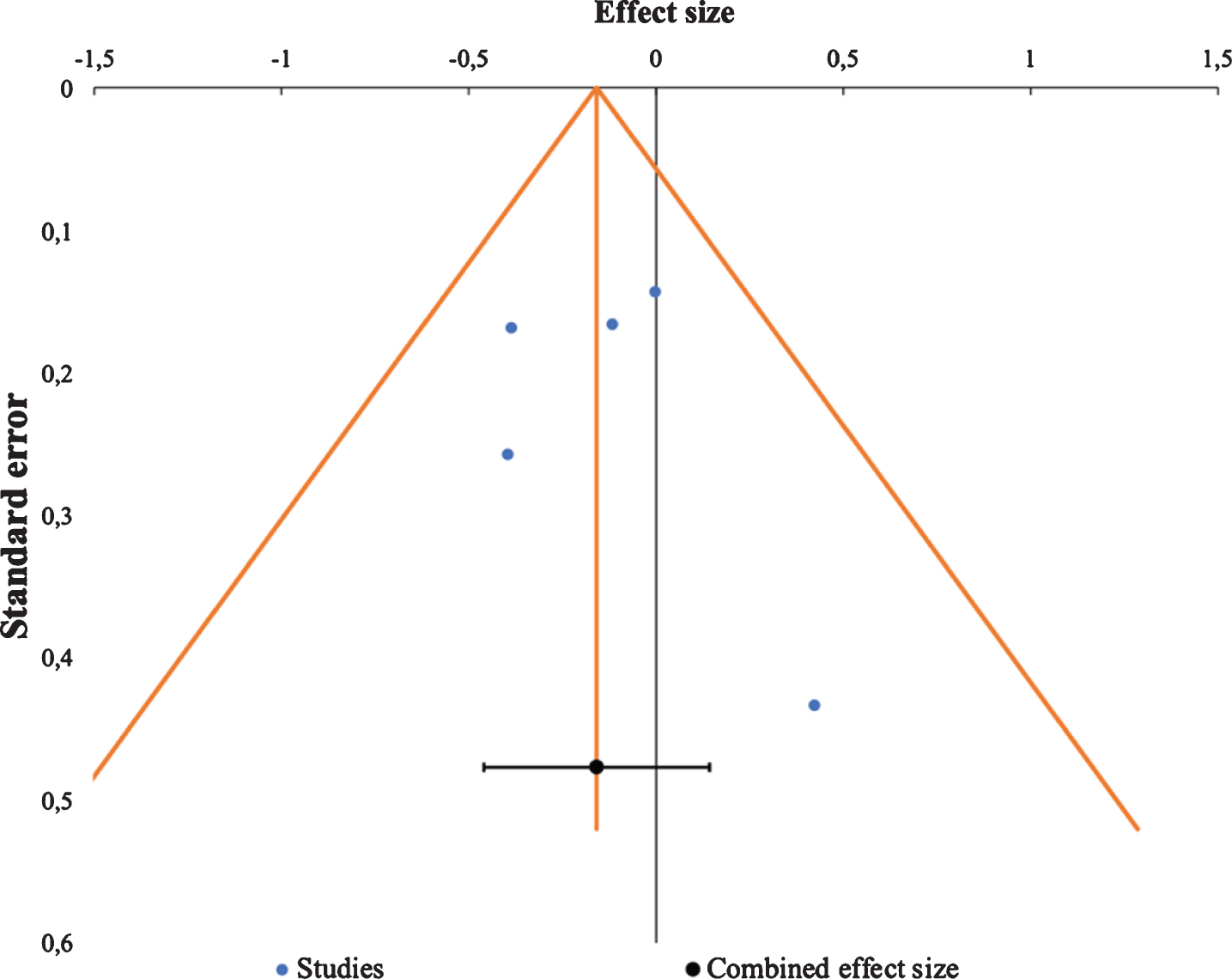
Funnel plot random effects (k = 5).
DISCUSSION
This study is the first meta-analysis on olfaction in individuals with SCD. We found that olfactory identification is slightly impaired in individuals with SCD compared to healthy older adults. In preclinical AD, at the SCD stage, individuals notice a decline in their cognition that causes them worries, but which classical neuropsychological tests are not able to detect [6, 43]. Our results suggest that olfactory identification declines in individuals with SCD. It seems that olfactory identification tests are more sensitive to objectify a decline than classical neuropsychological tests at the SCD stage.
Our results are in line with those from Sohrabi et al. (2009), who found that among olfactory functions, olfactory identification was linked to subjective memory complaints in community-dwelling older individuals, whereas olfactory detection, i.e., the ability to detect odors, was not [44]. Other studies have shown that olfactory identification is associated with semantic memory and verbal capacities [45, 46]. Thus, the decline of olfactory identification in individuals with SCD might be related to a decline in semantic memory and verbal capacities that is nevertheless not detectable with clinical tests. However, in 2019, Tahmasebi and colleagues did not find a significant link between olfactory identification and semantic memory in individuals with SCD [35]. They suggest that the decline in olfactory identification might be due to neuropathology consequences that are not limited to semantic memory and conclude that the ability to identify odors is distinct from semantic memory. This conclusion is in accordance with the model of aging and memory decline proposed by Larsson et al. (2016). This 3-component model includes olfactory, semantic and episodic memory and better explains the effect of age on memory performance in older adults than a 2-component model limited to semantic and episodic memory. In other words, they found that olfactory memory as indexed by episodic odor recognition and odor identification is modeled separately from episodic and semantic memory for visual and verbal information [47]. Interestingly, they found that among older individuals, those carrying APOE ɛ4 allele, which is a high-risk factor for developing AD, showed poorer memory performance, and these effects tended to be larger for olfactory memory. Thus, these results suggest that a decline in olfactory memory might be one of the early signs of AD. As a proxy of olfactory memory, assessing olfactory identification in individuals with SCD might help discriminate those who will convert to MCI or AD.
Another interesting point to discuss is the amplitude of the effect we found in our meta-analysis. No consensus had been reached on whether the olfactory decline found in MCI and dementia is already detectable in the SCD stage of the disease. Some studies found significant differences between healthy older participants and participants with SCD on olfactory identification scores [44, 48], while other studies did not [35, 49]. This meta-analysis confirmed that an olfactory decline is detectable at this early preclinical stage of the disease. The slight effect we found on olfactory identification may be due to the lack of specificity of the SCD diagnosis to discriminate those who will convert to MCI or AD from those who will remain stable. Interestingly, Jessen et al. (2014) propose a subcategory of SCD, the subjective cognitive decline plus or “SCD+” to better characterize those who are more at risk of developing an objective cognitive decline. SCD+ features include: (a) a subjective decline in memory, (b) an onset of SCD within the past 5 years, (c) and at 60 years and older, (d) a concern associated with SCD, (e) a persistence of SCD over time, (f) a seeking of medical help, and (g) a confirmation of cognitive decline by an observer [6, 8]. Thus, one may hypothesize that individuals with SCD+ may have lower odor identification abilities than individuals with SCD or healthy older adults. Unfortunately, results from our meta-analysis cannot help verify this hypothesis given that the characteristics of the participants in the included studies were not sufficiently detailed to apply the SCD+ criteria.
Furthermore, in order to interpret our results on the pathological course of AD, we hypothesize that neuropathological changes occur on olfactory function at the earliest phase of the disease. In 2017, Risacher et al. showed that tau deposition, but not amyloid-β pathology, is associated with the olfactory identification score in individuals with SCD [42]. These data are consistent with the results of the literature where olfactory identification scores were related to neurofibrillar pathology in the entorhinal cortex and hippocampus [50]. Thus, the decline of olfactory function would be much closer to a marker of tau pathology. This is an interesting hypothesis given that tau predicts cognitive decline in individuals with SCD [51, 52]. Unfortunately, we cannot verify whether individuals with greater olfactory decline had a greater amount of tau pathology, since the tau pathology status of the participants was not available for all the included studies in our meta-analysis. Another AD biomarker is neurodegeneration. Structures involved in olfactory treatment, such as the hippocampus and the primary olfactory cortex, are atrophied in patients with AD and MCI. Notably, the atrophy of these structures is correlated with olfactory performance [15]. The atrophy found in these regions could also explain the olfactory decline observed at the SCD stage. Cross-sectional and longitudinal olfactory studies including AD pathologic and genetic markers (tau, amyloid-β, neurodegeneration and APOE ɛ4 positives) in combination with SCD+ components could allow for a better qualification of preclinical patients at risk of AD. In other words, future studies should focus on combining olfactory measurements with other AD markers in the SCD stage to better predict those at risk of AD.
This meta-analysis has some limitations. First, this study compared effect sizes that are from different behavioral olfactory identification tests. Some tests are well-known and commercially available, such as the Sniffin’ Sticks [28, 53], the UPSIT [30], and the CC-SIT [31]. The Sniffin’ Sticks Identification test scores correlate with the UPSIT [54], and the CC-SIT scores are similar and do not differ from those of the UPSIT [31]. One study used the OPID test, which has shown similar results to the UPSIT in the classification of MCI of AD patients [29]. However, although these different tests measure the same construct and are comparable, they are not identical. Thus, the results of this meta-analysis should be interpreted with having this in mind. Second, this meta-analysis evaluated bias risks from each included study using the NOS. Considering the lack of gold standard tools to assess quality of case-control studies (e.g., SCD versus healthy older adults) [55, 56], especially for non-randomized studies, we followed the recommendations of Zeng et al. (2015) and used the NOS to evaluate studies included in the meta-analysis, even though the NOS has not yet been fully validated [33, 55]. Although the majority of the included studies demonstrated a low to moderate risk of bias, no studies were excluded based on this assessment. Results at the NOS scale revealed that the main shortcomings in terms of quality were found in the method used for participants’ recruitment and the non-inclusion of variables such as age or sex in the analysis. Rigorous recruitment methods help avoid the risk of bias regarding the representativeness of the sampling. It is also important to include factors such as age or sex as covariates when analyzing olfactory scores since these variables are known to influence olfactory performance [53]. A common strength of the selected studies was the assessment of olfactory identification by valid olfactory tests and the use of valid cognitive tests to qualify the lack of difference between SCD and control groups on the cognitive level. However, in most of the selected studies, confounding variables such as depression or anxiety symptoms were not accounted for in the analyses. Considering that these symptoms might lead the person to express an SCD, there is a need that future studies control for the influence of these variables [6]. Third, when analyzing publication bias, we were unable to performed regression-based analysis due to the small number of included studies. It highlights the dearth of studies on the sense of smell within individuals with SCD. Indeed, this meta-analysis included a low number of five different samples, which is the minimal number of studies required for random-effects models [57]. Thus, more studies with rigorous methodologies and larger samples of individuals with SCD are needed to conclude that olfactory identification is indeed a biomarker of AD at the SCD stage.
Following these limitations, we recommend that future studies include larger groups that are well-matched for sociodemographic characteristics. Furthermore, we recommend that a rigorous neuropsychological evaluation be conducted when selecting SCD participants. Future studies should also control for psychological variables that are susceptible to influence cognitive complaints such as anxiety or depression levels. Cognition should also be rigorously evaluated with more than a rapid screening test (i.e., The MMSE or the MoCA) when recruiting and differentiating healthy participants and SCD participants from MCI patients.
CONCLUSION
Olfactory identification is slightly impaired in individuals with SCD compared to healthy older adults. This first meta-analysis also highlights the limited literature on this topic and thus the need for more studies in order to better characterize individuals with SCD on olfactory capacities. To conclude, our results suggest that olfactory dysfunction may be a potential early marker of AD.
Footnotes
ACKNOWLEDGMENTS
We would like to thank AnnyPier Roof for her research assistance, Gabrielle Ciquier Sell for English editing and Dr Suurmond for his generous help with Meta-essentials. We would also like to thank the reviewers for their generous recommendations.
This work was supported by grants from NSERC (Natural Sciences and Engineering Research Council of Canada) [2015-04597] (JF), FRQS (Fonds de Recherche du Québec - Santé) [#32618] (JF) and UQTR (Université du Québec à Trois-Rivières) research funds (BB). BJ is supported by scholarships from the CIHR (Canadian Institutes of Health Research), the FRQS (Fonds de recherche Québec santé), and the Fondation J.A. DeSève (CIUSSS du Nord-de-l’île-de-Montréal).