
Abstract
Background:
Alzheimer’s disease dementia (ADD) is an important health problem in the world.
Objective:
The present study investigated the validity and reliability of a new version of the Frontal Assessment Battery (FAB) named the FAB-phonemic (FAB-P).
Methods:
A total of 76 patients with ADD, 107 patients with amnestic mild cognitive impairment (aMCI), 37 patients with non-amnestic MCI (naMCI), and 123 healthy controls were included in this study. All participants were evaluated with the FAB-P and the cognitive assessments according to a standard procedure.
Results:
The global FAB-P scores in patients with ADD were lower than those of patients with aMCI, patients with naMCI, and healthy controls (p < 0.001). Patients with aMCI performed worse than healthy controls (p < 0.001). The interrater reliability, test-retest reliability, and Cronbach’s alpha coefficient for the FAB-P were 0.997, 0.819, and 0.736, respectively. The test could distinguish the patients with mild ADD, aMCI, and naMCI from healthy controls with classification accuracy of 89.4%, 70.9%, and 61.6%, respectively. It could also discriminate between the patients with ADD and aMCI, between those with ADD and naMCI, and between those with aMCI and naMCI with classification accuracy of 73.8%, 83.9%, and 58.0%, respectively. The regression analysis revealed that the Montreal Cognitive Assessment and the Stroop Color Word Test Part C had the greatest contribution to FAB-P score variance.
Conclusion:
The FAB-P is a valid and reliable tool for evaluating frontal lobe function and can effectively discriminate ADD, aMCI, and naMCI.
INTRODUCTION
Alzheimer’s disease dementia (ADD) has become an important health problem among the aging population in China. Mild cognitive impairment (MCI) is an intermediate state between dementia and normal cognitive aging. The prevalence of ADD and MCI is 3.21% and 20.8% [1, 2], respectively, among individuals aged 65 years and older. In addition to the domain for episodic memory, executive function is the cognitive domain affected in patients with MCI and early-stage ADD [3]. Previous screening tests mainly focused on the memory domain.
The Frontal Assessment Battery (FAB), develo-ped by Dubois et al., is a simple, reliable tool to assess frontal lobe dysfunction at bedside [4]. The original test includes six items: 1) similarities (con-ceptualization), which explores abstract reasoning by presenting pairs of objects from the same semantic category; 2) lexical fluency (mental flexibility), which assesses self-organization, strategy, and cha-nge, by requiring the person to generate as many words as possible that start with a given letter; 3) motor series, which explores motor programming and planning by carrying out Luria’s series (fist-side-palm); 4) conflicting instructions, which explores the person’s sensitivity to interference by giving the opposite response to that of the examiner; 5) go/no-go, which assesses inhibitory control and impulsivity; and 6) prehension behavior, which assesses the ability to spontaneously inhibit prehension. The FAB is widely used in Western countries, and only a few researchers have tried to administer the FAB for Chinese people. The Chinese version of the FAB had to be adapted because Chinese is different from English, Japanese, and Korean. The mental flexibility (verbal fluency) subtest is the main item affected by culture, which is often substituted with category fluency. The Chinese version of the FAB (CFAB) uses category fluency (animal) as the mental flexibility subtest, which is only moderately valid in evaluating executive dysfunction among Chinese stroke patients with small subcortical infarcts [5]. In the Taiwanese (Traditional Chinese) version of the FAB (TFAB), the verbal fluency subtest is modified as the orthographical fluency subtest, which is a useful screening procedure to differentiate MCI due to subcortical ischemic vascular disease (SIVD) from MCI due to ADD [6, 7]. Chinese Pinyin exists in mainland China with simplified Chinese characters that reflect the Chinese phonemic system and differ from traditional Chinese, making phonemic fluency possible. We used Chinese phonemic fluency as the verbal fluency subtest and developed a new version of the FAB called the FAB-phonemic (FAB-P)
The purpose of the present study was to investigate the validity and reliability of the FAB-P.
METHODS
Subjects
Three hundred forty-three subjects were recruited from the outpatient memory clinics of China-Japan Friendship Hospital and Beijing Tiantan Hospital between 2015 and 2018. All participants underwent routine assessments, including standardized history taking, physical and neurological examinations, necessary laboratory tests, and a computed tomography (CT) or magnetic resonance imaging (MRI) scan. Of these patients, 76 (35 men and 41 women) met the consensus criteria of NIA-AA (the National Institute on Aging-Alzheimer’s Association workgroups) for probable ADD [8]. The Clinical Dementia Rating Scale (CDR) [9] of the patients with ADD was 1.0. One hundred forty-four of these patients were diagnosed with MCI and fulfilled the following criteria: 1) cognitive complaint, preferably corroborated by an informant; 2) objective cognitive impairment, quantified as a performance score more than 1.5 standard deviation (SD) below the appropriate mean on one cognitive test of any domain; 3) normal general cognitive functioning (scores of the Mini-Mental State Examination (MMSE) [10] equal to or above 26); 4) essentially intact activities of daily living (ADL); and 5) no dementia [11]. Subjects with a score less than 1.5 SD from the mean on a learning measure or delayed recall on the Rey Auditory Verbal Learning Test (RAVLT) [12] or the Rey-Osterrieth complex figure (ROCF) [13] were classified as having amnestic MCI (aMCI). Subjects with a score less than 1.5 SD from the mean on at least one test of attention, executive function, language facilities and visuospatial capacity, but no memory impairment, were classified as having non-amnestic (naMCI). A total of 107 aMCI (54 men and 52 women) and 37 naMCI (12 men and 25 women) patients were included in the study. The CDR score was 0.5 in all MCI patients. One hundred twenty-three subjects were considered as healthy controls, including 38 men and 85 women. The inclusion criteria for the controls were as follows: 1) almost normal cognitive functions verified by informants; 2) the MMSE scores equal to or above 26; 3) intact ADL; and 4) a CDR score of 0. The exclusion criteria for the patients and controls were: severe medical illness, neurological disorder, psychiatric disease, hearing or eyesight loss, and obvious abnormalities visible by cranial CT or MRI. Participants who had been prescribed psychiatric drugs were also excluded.
The objectives of the research were explained to the participants and their families, and written informed consent was obtained for each participant. The research was approved by the Ethics Committee of the China-Japan Friendship Hospital and Beijing Tiantan Hospital.
Clinical evaluations
Cognitive assessments
The cognitive assessments were administered by technicians according to a standard procedure and scored by a neuropsychologist. The time required for test administration was approximately 90 min.
The test battery included global cognitive screening, attention/processing speed, executive function, memory aptitude, language facilities, and visuospatial abilities. The MMSE and the Montreal Cognitive Assessment (MoCA) (Beijing version) were used for global cognitive screening [10, 14]. The Digit Span Forward subset of the Wechsler Adult Intelligence Test-Revised Chinese version (WAIS-RC) [15], the Trail Making Test A (TMT-A) [12], the Stroop Color Word Test (modified version) (SCWT) Part A [12], and the Digit Symbol subtest of the WAIS-RC [15] were used to assess processing speed/attention. Executive function was assessed using the Chinese Version of Trail Making Test B (TMT-B) [16] and the SCWT Part C [12]. The RAVLT included the sum of trials 1 to 5 and delayed recall to detect verbal memory [12]. The delayed recall (30 min) aspect of the ROCF [13] was also used to measure visual memory. The Semantic Category Verbal Fluency Test (animal) [12] and the Boston Naming Test (BNT) as modified by Cheung et al. [17] was employed to assess language ability. Visuospatial skills were verified by the ROCF [13], the Block Design of the WAIS-RC [15], and the Clock Drawing Test (CDT) [18] scored by the Rouleau system. The raw scores were documented in all cognitive tests.
The frontal assessment battery
The FAB-P was administered to all participants. The scorers rating the test were blinded to the cognitive test scores. The time required for test adm-inistration was approximately 5 minutes. The FAB consists of six items, and the score on each item ranges from 0 to 3 for a total score ranging from 0 to 18. A higher score means a better performance. The six subtests of the FAB explore 1) similarities (conceptualization), 2) lexical fluency (mental flexibility), 3) Luria motor sequences (programming), 4) conflicting instructions (sensitivity to interference), 5) go-no go test (inhibitory control), and 6) prehension behavior (environmental autonomy). In the new Chinese version of the FAB, the lexical fluency subtest is modified as a Chinese phonetic fluency task. “ ” was chosen to make words as the first, for example “
” was chosen to make words as the first, for example “ (making rich)”. The scoring system for this item was as follows: more than 6 words, 3; 5-6 words, 2; 3-4 words, 1; less than 3 words, 0.
(making rich)”. The scoring system for this item was as follows: more than 6 words, 3; 5-6 words, 2; 3-4 words, 1; less than 3 words, 0.
Statistical analysis
Statistical analyses were performed using SPSS, version 17.0 (SPSS Inc., USA). Data are expressed as the mean±SD unless otherwise specified. One-way analysis of variance (ANOVA) was applied for quantitative demographic variables among the control, aMCI, naMCI, and ADD groups. We compared the re-sults of the cognitive tests and the scores of the FAB-P using analysis of covariance (ANCOVA) adjusted for age, education, and gender. The Chi-square test was used to compare the differences between the qualitative variables among four groups, including the sex ratio and handedness. Because multiple cognitive tests were administered, Bonferroni correction for multiple tests was also applied.
The interrater reliability of the FAB-P was determined by rating 20 randomly selected participants. One examiner tested and scored the participant, and the other examiner scored the participant simultaneously. Test-retest reliability was assessed for 23 subjects for the FAB-P. To avoid a learning effect, the second rating was performed six months after the first rating. The Pearson correlation coefficient was calculated to analyze the interrater reliability and test-retest reliability. Internal consistency was examined using a Cronbach’s alpha coefficient.
To examine discriminant validity, we used a stepwise discriminant analysis among different groups. A receiver operating characteristic (ROC) analysis was also conducted to determine the optimal cut-off scores between healthy controls and different MCI or ADD groups. The sensitivity and specificity of the FAB were also assessed.
To investigate the concurrent validity, the Pearson correlation coefficient (r) was used to evaluate the correlations between the FAB scores and age, education, and cognitive test scores. Stepwise multivariate regression analysis was further used to find independent contributions to the variance of the FAB-P.
All statistical tests were 2 tailed, and p < 0.05 was considered to indicate statistical significance.
RESULTS
Comparison among groups
The demographic and clinical data of the patients with ADD, aMCI, and naMCI and the healthy controls are summarized in Table 1.
Demographic, neuropsychological data and FAB-P performance of the patients with ADD, aMCI, naMCI, and the healthy controls
ADD, Alzheimer’s disease dementia; aMCI, amnestic mild cognitive impairment; FAB-P, Frontal Assessment Battery-phonemic; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; n, number; naMCI, non-amnestic mild cognitive impairment; ND, no data.
The healthy controls (mean age 66.26±9.96 years) were younger than patients with aMCI (mean age 74.24±8.05 years), naMCI (mean age 71.46±9.63 years), and ADD (mean age 78.21±7.43 years) (p < 0.001, p = 0.011, and p < 0.001), whereas ADD patients were older than aMCI and naMCI patients (p = 0.018, p = 0.001). There were no differences in age between patients with aMCI and naMCI (p > 0.05). Patients with ADD had lower education levels than patients with MCI and healthy controls (p < 0.001, p = 0.001, and p < 0.001), but there were no differences in education among patients with aMCI, patients with naMCI and healthy controls (p > 0.05). There were more male patients with aMCI than male patients with naMCI and male healthy controls (p = 0.046, p = 0.002), while there were no sex differences among the other groups (p > 0.05). The percentages of patients who were right-handed were similar among the three groups (p > 0.05). There were also no differences in duration of disease among the three patient groups (p > 0.05).
After adjusting age, gender, and education, patients with ADD performed worse than patients with aMCI, patients with naMCI, and healthy controls on the MMSE and the MoCA (p < 0.001) (Bonferroni correction was applied and level of significance set at 0.017). The scores of the MoCA in patients with aMCI were lower than those of patients with naMCI (p = 0.009) and healthy controls (p < 0.001), whereas patients with naMCI also had worse scores than healthy controls (p = 0.001). Only patients with aMCI had lower scores than healthy controls on the MMSE (p < 0.001), and there were no difference between patients with aMCI and naMCI, patients with naMCI and healthy controls (p > 0.05).
The global FAB-P scores in patients with ADD were lower than those of patients with aMCI, patients with naMCI and healthy controls (p < 0.001). Patients with aMCI performed worse on the FAB-P than those with healthy controls (p < 0.001), while there were no difference between patients with aMCI and naMCI, patients with naMCI and healthy controls. Patients with ADD had lower scores for similarity, the Luria motor sequences, conflicting instructions and go-no go subtests than patients with aMCI (p = 0.002, <0.001, <0.001, <0.001), patients with naMCI (p = 0.001, p < 0.001, = 0.001,<0.001) and healthy controls (p < 0.001, <0.001, <0.001, <0.001), whereas patients with ADD also performed worse than healthy controls in the lexical fluency (p <0.001). The scores of similarity and go-no go test in patients with aMCI were lower than healthy controls (p = 0.009, <0.001). There were no differences in prehension behavior among all patients (p > 0.05).
Reliability
The Pearson correlation coefficient for the FAB-P was 0.997 (p < 0.001), which revealed good interrater reliability. Test-retest reliability for the FAB-P was also good (r = 0.819, p < 0.001). The Cronbach’s alpha coefficient was 0.736 on the six items of the FAB-P, showing good internal consistency.
Concurrent validity
After Bonferroni correction for multiple tests was applied (level of significance set at 0.003), the FAB-P had a strong correlation with age (r = –0.352, p < 0.001) and education (r = 0.398, p < 0.001). After controlling for age and education, the FAB-P was positively correlated with the scores of the MMSE (r = 0.445, p < 0.001), the MoCA (r = 0.550, p < 0.001), the sum of trials 1 to 5 (r = 0.363, p < 0.001) and delayed recall (r = 0.341, p < 0.001) of the RAVLT, the delayed recall of the ROCF (r = 0.425, p < 0.001), the Digit Span Forward (r = 0.235, p = 0.003), the Digit Symbol (r = 0.233, p = 0.003), the verbal fluency test, (r = 0.434, p < 0.001), the BNT (r = 0.336, p < 0.001), and the Block Design (r = 0.307, p < 0.001). The FAB-P was negatively correlated with the scores of the TMT-A (r = –0.332, p < 0.001), TMT-B (r = –0.270, p = 0.001), the SCWT Part A (r = –0.273, p < 0.001) and Part C (r = –0.393, p < 0.001) (Table 2). Stepwise multiple regression analysis revealed that the MoCA (R2 = 0.308, p < 0.001) and the SCWT Part C (R2 = 0.345, p = 0.002) had the greatest contribution to variations in FAB-P scores. The FAB-P had a negative correlation with the ADL (r = –0.214, p = 0.006) and the CDR (r = –0.471, p < 0.001), whereas there was no relationship between the FAB-P and the NPI. (p > 0.05).
Correlation between the FAB-P and other cognitive tests
BNT, the Boston Naming Test; CDT, the Clock Drawing Test; FAB-P, Frontal Assessment Battery-phonemic; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; RAVLT, the Rey Auditory Verbal Learning Test; ROCF, the Rey-Osterrieth complex figure; SCWT, the Stroop Color Word Test; TMT-A, the Trail Making Test A; TMT-B, Trail Making Test B. ap < 0.05; bp≦0.003.
Discriminant validity
The stepwise discriminant analysis between the ADD patients and healthy controls yielded a canonical discriminant function for the FAB-P (r = 0.783, Wilks’λ= 0.387, p < 0.001). The overall classification accuracy was 89.4% with sensitivity of 93.5% and specificity of 82.9%. The analysis between the aMCI and control groups and the naMCI and control groups also yielded a canonical discriminant function for the FAB-P (r = 0.462, Wilks’λ= 0.786, p < 0.001; r = 0.251, Wilks’λ= 0.937, p = 0.001) with classification accuracy of 70.9% and 61.6%. The discriminant function for the FAB-P were achieved between the ADD and aMCI (r = 0.536, Wilks’λ= 0.713, p < 0.001), the ADD and naMCI (r = 0.643, Wilks’λ= 0.586, p < 0.001), and the aMCI and naMCI groups (r = 0.203, Wilks’λ= 0.959, p = 0.015) with classification accuracy of 73.8%, 83.9%, and 58.0%.
The area under the curve (AUC) for the global scores of the FAB-P when comparing the ADD and control groups was 0.958 (CI = 0.934–0.982) (p < 0.001). The optimal cut-off score of the FAB-P was determined as 12/13, whereas the sensitivity and specificity were 0.934 and 0.829. The AUC values when comparing the aMCI or naMCI and control groups were 0.761 (CI = 0.697–0.825) (p < 0.001) and 0.668 (CI = 0.573–0.764) (p = 0.002). If the cut-off scores for aMCI or naMCI were selected as 14/15 or 15/16, the sensitivity and specificity were 0.770 and 0.642, or 0.623 and 0.583, respectively. When comparing the ADD and naMCI, the ADD and aMCI, the aMCI and naMCI groups, the AUC were 0.906 (CI = 0.849–0.963) (p < 0.001), 0.805 (CI = 0.742–0.868) (p < 0.001), and 0.640 (CI = 0.542–0.737) (p = 0.012). The sensitivity and specificity for different comparisons were 0.861 and 0.827, 0.775 and 0.707, and 0.566 and 0.642, when the cut-off scores were considered as 12/13, 11/12, and 14/15, respectively (Fig. 1).
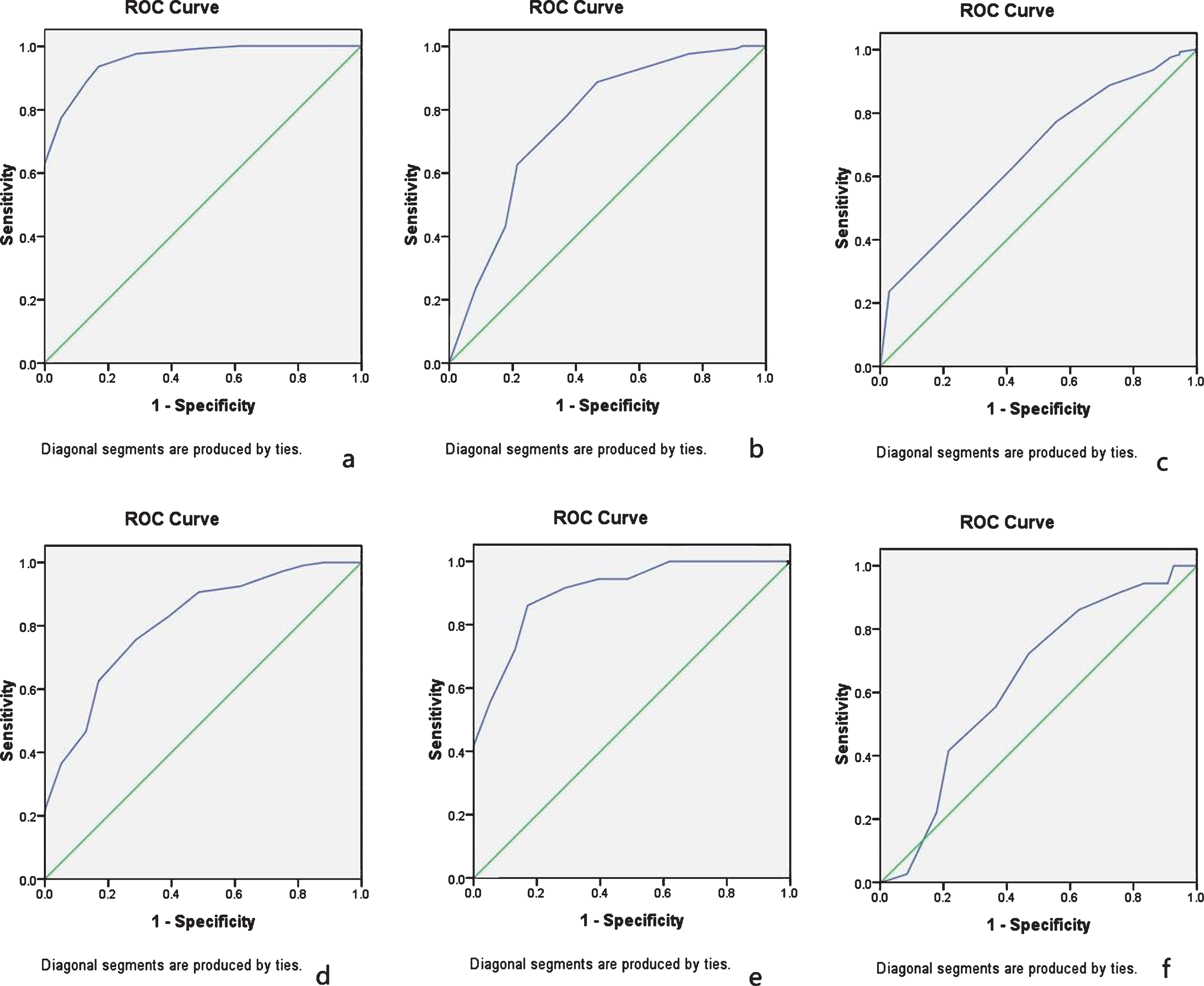
The area under the curve (AUC) for the global scores of the FAB-P when comparing different groups. a) The AUC between ADD and control groups; b) the AUC between aMCI and control groups; c) the AUC between naMCI and control groups; d) the AUC between aMCI and ADD groups; e) the AUC between naMCI and ADD groups; f) the AUC between aMCI and naMCI groups.
DISCUSSION
We developed a new version of the FAB administering the Chinese phonemic fluency task. The present study investigated the validity and reliability of the FAB-P. We found that the FAB-P had good interrater reliability, test-retest reliability, and internal consistency. The test could distinguish the patients with mild ADD, aMCI, and naMCI from healthy controls with classification accuracy of 89.4%, 70.9%, and 61.6%, respectively. It could also discriminate between the patients with ADD and aMCI, between those with ADD and naMCI, and between those with aMCI and naMCI with classification accuracy of 73.8%, 83.9%, and 58.0%, respectively. The FAB-P correlated with the scores of cognitive tests involving executive function, attention, memory and language, and the MoCA and the Stroop Color Word Test Part C had the greatest contribution, signifying that executive function had a close relationship with the FAB-P. All of those reflected the test had a good discriminant validity and concurrent validity.
Executive function is considered to be associated with the frontal lobe structure and/or function. Alth-ough there are many tests that assess it, some of these require long administration times, and some only inv-estigate one domain of executive function. The FAB is a brief and simple tool that includes six items that can assess executive function and differentiate 89.1% of patients from healthy participants [4]. A Korean study reported that the usefulness of education-ad-justment and supplementation with a frontal lobe fun-ction assessment (the FAB) improving the screening performance of the MMSE for dementia and its subtypes, especially non-ADD [19]. The FAB also had a role in the differential diagnosis of ADD and frontotemporal dementia (FTD) [20], although a study showed that the FAB was not a useful tool to distinguish successfully between behavioral variant FTD (bvFTD) and non-bvFTD [21]. Some subtests of the FAB, such as mental flexibility, motor programming, disinhibition and environmental autonomy, might be useful in differential diagnoses [20, 22]. When comparing ADD with vascular cognitive impairment or dementia with Lewy bodies, there were also disagreements among different studies [23, 24]. There was higher impairment indicated by the FAB total score and the subtests (conceptualization, sensitivity to interference, inhibitory control, and environmental autonomy) only in moderate to severe ADD compared to vascular dementia patients [25]. FAB could also provide a differential diagnosis for progressive supranuclear palsy (PSP), multiple system atrophy (MSA), and Parkinson’s disease (PD) patients [26].
The CFAB was first evaluated among Chinese stroke patients with small subcortical infarcts using the category fluency (animal) subtest because of the difference of the culture. They found that it had good internal consistency, test-retest reliability, interrater reliability, and low to good correlation with various executive measures with a classification accuracy of 80.6% [5]. The education-adjusted CFAB was considered a screening instrument in detecting MCI and early dementia. A combination of the CFAB and MMSE had a better screening performance compared to either test in isolation [27]. The CFAB was also used to evaluate executive function in the patients with PD, MSA, PSP, or amyotrophic lateral sclerosis. The patients with PD performed poorly on the CFAB, especially older patients, those with longer disease duration, and those with more severe motor disability [28]. A total of 41.6% of the patients with MSA had frontal lobe dysfunction assessed by the CFAB, with inhibitory control (60.9%) as the most impaired domain. The MSA-C subtype, disease severity, and a low education level are potential predictors of CFAB scores [29]. A total of 76.9% of PSP patients were impaired in the CFAB, which denoted executive dysfunction and correlated with the severity of the PSP severity [30]. Amyotrophic lateral sclerosis patients with an onset age > 45 years or a lower educational level performed worse in the CFAB [31].
The TFAB used orthographical fluency as the verbal fluency subtest that could differentiate MCI due to SIVD from MCI due to ADD. Orthographical fluency had a classification accuracy of 73.2% by discriminative analysis, which significantly correlated with frontal periventricular, frontal deep, and basal ganglia white matter [6, 7].
We introduced the Chinese phonemic fluency task as the verbal fluency subtest to develop a new version of the FAB that was more similar to the traditional version. The results demonstrated the test have a sat-isfactory validity and reliability, and was able to accurately discriminate mild ADD, aMCI and naMCI. The aMCI is said to have a high likelihood of progr-essing to ADD, while naMCI is assumed to have a higher likelihood of progressing to a non-AD dementia [11]. We also found that the FAB-P had a role on discriminating aMCI from naMCI, which was the first attempt.
Episodic memory and executive function deficits are often considered to precede impairments in constructional praxis, language, and sustained attention in patients with ADD. In addition to memory impairments, subjects with aMCI also exhibit executive dysfunction [3]. Executive function deficits appear predominantly in tasks requiring the resolution of competing response tendencies, cognitive flexibility and self-monitoring [32, 33].
Another cross-sectional study found a significant difference in the total FAB and subtest scores between the aMCI and ADD groups. There were also significant differences in the MMSE total and subtest scores reflecting attention and memory function between the two groups. Moreover, the two FAB subtest scores (conflicting instructions and go/no-go) were significantly influenced only by the diagnosis and not by the interaction with memory impairment or disorientation [34].
Some executive function measures, including inhibition and switching, could predict subsequent global cognitive decline independent of episodic memory in initially non-demented older adults, including those with MCI and cognitively normal [35]. Impaired exe-cutive function and reduced parietotemporal met-abolism could predict the clinical progression to MCI and ADD in elderly healthy subjects [36]. The FAB total and subtest scores (similarities, motor series, and conflicting instructions) were significantly lower in ADD patients with delusional thoughts than in those without delusional thoughts [37]. A multiple regression analysis showed that delusional thoughts were significantly associated with the FAB total score. Frontal lobe dysfunction might be related to delusional ideation or misidentifications in patients with ADD. The meta-analysis suggests a consistent moderate association between ADL and executive function in patients with ADD [38]. Executive dysfunction was also a key contributor to impairment in instrumental ADL, whereas the relationship existed even after accounting the memory deficit degree in either ADD or MCI subjects [39]. In ADD patients, good performance in executive function, such as the verbal fluency test and the Stroop test, at baseline was associated with longer survival [40].
The MoCA and the SCWT Part C had the greatest contribution to variations in FAB-P scores in our study, which demonstrated the close relationship between the FAB-P and executive function. Abnormalities of the FAB-P in patients also showed the early changes of executive function in patients with mild ADD, aMCI, and naMCI. The present study also certified the correlation between the FAB-P and the ADL or the CDR, but it found no relationship between the test and behavioral and psychiatric symptom of dementia.
Abnormalities of cerebrospinal fluid or positron emission tomography (PET) on amyloid-β (Aβ) and tau were diagnostic biomarkers of ADD according to the AT(N) system. Cognitively normal people with Aβ and tau abnormalities are considered preclinical ADD. Some data suggested that altered Aβ42 levels in cerebrospinal fluid with decreased executive performance preceded memory impairment from hippocampal intraneuronal neurofibrillary pathology, which matched extracellular amyloid deposits that appeared in the basal isocortex first and only later involved the hippocampus. Stroop interference may be an additional important screen for early pathology during research [41].
Volumetric MRI, PET, and single photon emission computed tomography (SPECT) reflect neural structural and functional impairments in dementia. The FAB score correlated positively with the regional grey matter volume in the right precentral gyrus (Brodmann area 6), the left lateral frontal lobe (Brodmann area 9) and the right lateral frontal lobe (Brodmann area 46), and both latter regions were associated with other tests measuring executive function, such as the Executive Interview and the clock-drawing task [42]. The left rostral middle frontal cortex, which is mostly related to the dorsolateral prefrontal cortex (DLPFC), and the left cerebellar cortex, were associated with executive performance examined by the FAB in alcoholic subjects [43]. In addition to the frontal lobe alterations, another study also reported that the atrophy of the entorhinal cortex and parahippocampal gyrus in patients with early ADD or aMCI might influence one of the executive functions, such as the go/no-go task of the FAB, independently of the diagnosis [3]. Compared with patients with high scores on the FAB, ADD patients with low scores showed significant hypoperfusion in the left middle frontal gyrus and the right superior frontal gyrus extending to the left superior frontal gyrus, as indicated by SPECT data [44]. In dementia patients, FAB scores had a moderately positive correlation with the left callosomarginal and precentral regional cerebral blood flow [45]. All the studies verified that executive dysfunction mainly measured by the FAB correlated mostly with the frontal areas of the brain, although other brain areas may be involved.
Functional imaging was used to evaluate the relationship with the FAB in addition to the biomarkers, such as diffusion tensor imaging, resting-state functional MRI (rs-fMRI). Fractional anisotropy (FA) and mean diffusivity (MD) in frontal and parietal lobe WM structures were associated with executive function scores in MCI and only frontal lobe struct-ures in ADD. Executive function was more strongly associated with FA than MD. The relationship bet-ween executive function, FA and MD was strongest in MCI [46]. In the combined analysis of the patients with SIVD and ADD, the total FAB score was positively correlated with FA within the bilateral forceps minor, genu of the corpus callosum, left forceps major, left uncinate fasciculus, and right inferior longitudinal fasciculus and inversely correlated with MD within the right superior longitudinal fasciculus, genu and body of the corpus callosum, bilateral forceps minor, right uncinate fasciculus, and right inferior longitudinal fasciculus [47]. An rs-fMRI study found that the scores of episodic memory were significantly negatively correlated with the scores of executive function in both healthy controls and aMCI patients. There were increases in the intrinsic executive function network and decreases in the episodic memory network in aMCI patients, suggesting that the neural activity between executive function and episodic memory networks was not balanced. The connectivity between the right DLPFC and bilateral middle cingulate cortex mediated the association between executive function and episodic memory performance in aMCI patients. These findings provide direct evidence supporting the suggestion that executive function mediate episodic memory performance at the network level in a non-demented elderly population [48]. Low default mode network (DMN) deactivation, high executive control network (ECN) activation and high white matter hyperintensity burden were the main predictors of executive function scores at baseline. In contrast, poor DMN and ECN white matter microstructure and higher AD pathology predicted a greater annual decline in executive function scores. Subsequent mediation analysis demonstrated that DMN white matter microstructure uniquely mediated the relationship between AD pathology and changes in executive function [49]. We need further evaluate the relationship between the FAB-P and the biomarkers in AD patients.
The present study has some limitations. First, the participants were selected from our memory clinics, not from the community, which may lead to bias. Second, the healthy controls were more young, the aMCI patients had more males than other groups, and the ADD group had less education than other groups, but we analyzed the results after adjusting the age, education and gender.
In conclusion, the new version of the FAB (FBA-P) had good interrater reliability, test-retest reliability and internal consistency. The test also had a good discriminant validity and concurrent validity. The test could discriminate patients with mild ADD, aMCI, and naMCI from healthy controls, whereas it could also differentiate between patients with ADD and aMCI, between patients with ADD and naMCI, and between patients with aMCI and naMCI. The FAB-P was a valid and reliable tool for evaluating executive function. Undoubtedly, the test should be performed with a larger population to further determine its usefulness.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the China-Japan Fri-endship Hospital (2014-4-QN-32), Personnel development funding projects of Beijing Dongcheng District (DCQYYRC-791-01-DR) and Key Projects of Strategic International Cooperation in Scientific and Technological Innovation in National Key Research and Development Program (2018YFE0203600).