
Abstract
Background:
Patients with Alzheimer’s disease (AD) have gut microbiome alterations compared with healthy controls. However, previous studies often assess AD patients who have been on medications or other interventions for the disease. Also, simultaneous determination of gut microbiome in patients with mild cognitive impairment (MCI) or AD in a study is rare.
Objective:
To determine whether there was a gut microbiome alteration in patients newly diagnosed with AD or MCI and whether the degree of gut microbiome alteration was more severe in patients with AD than patients with MCI.
Methods:
Fecal samples of 18 patients with AD, 20 patients with MCI, and 18 age-matched healthy controls were collected in the morning for 16S ribosomal RNA sequencing. No patient had medications or interventions for AD or MCI before the samples were collected.
Results:
Although there was no difference in the microbial α-diversity among the three groups, patients with AD or MCI had increased β-diversity compared with healthy controls. Patients with AD had decreased Bacteroides, Lachnospira, and Ruminiclostridium_9 and increased Prevotella at the genus level compared with healthy controls. The changing direction of these genera in patients with MCI was the same as patients with AD. However, Lachnospira was the only genus whose abundance in patients with MCI was statistically significantly lower than healthy controls. Bacteroides, Lachnospira, and Ruminiclostridium_9 were positively associated with better cognitive functions whereas Prevotella was on the contrary when subjects of all three groups were considered. The negative correlation of Prevotella with cognitive functions remained among patients with MCI.
Conclusion:
Patients newly diagnosed with AD or MCI have gut dysbiosis that includes the decrease of potentially protective microbiome, such as Bacteroides, and the increase of microbiome that can promote inflammation, such as Prevotella. Our results support a novel idea that the degree of gut dysbiosis is worsened with the disease stage from MCI to AD.
INTRODUCTION
The possible role of gut microbiome-brain axis in the development of Alzheimer’s disease (AD), the most common neurodegenerative disease in the elderly, has been proposed in recent years [1–3]. This proposal is supported by the findings that patients with AD have gut microbiome features that are different from mentally healthy people, gut microbiome that is linked to inflammation is increased in AD patients, and some bacteria that are amyloid generating are increased in those patients [4, 5]. Animals with AD-like brain changes have altered gut microbiome that increases inflammatory responses [6]. Replacing gut microbiome of AD-like mice with that of healthy mice attenuates AD-like brain and behavior changes [7].
The complex pathological changes including amy-loid-β peptide accumulation and deposition, activation of inflammatory responses and oxidative stress, which induce cell injury and dysfunction, ultimately lead to the presentation of AD [8]. Gut microbiome can alter gut mucosal permeability, activate gut immune cells, and potentially induce systemic and neural inflammation [4, 5]. These processes may be the pathological mechanisms for the involvement of gut microbiome in the development of AD.
One of the significant questions is whether gut microbiome alteration occurs before the presentation of AD symptoms. If so, this alteration may contribute to the development of AD symptoms. If the alteration occurs after the presentation of AD, gut microbiome may contribute to the worsening of AD presentation. Thus, it is necessary to determine whether there is a gut microbiome change at a stage before the full presentation of AD. Mild cognitive impairment (MCI) is considered as a prodromal stage of AD [9]. Although some patients with MCI may not progress to AD and MCI in some patients may not be the results of AD-like neuropathology, amnestic MCI has a conversion rate of 10 to 15% per year to probable AD [10]. Thus, determining the changes of gut microbiome in patients with MCI may provide an indication for the role of gut microbiome in MCI and AD presentation. Three studies published in 2019 have investigated the gut microbiome in patients with MCI. One study showed that patients with MCI had gut microbiome similar to that of patients with AD [4]. Another study showed that gut microbiome was different among healthy controls and patients with MCI or AD. It was possible to distinguish healthy controls from patients with MCI or AD or patients with AD from patients with MCI [11]. The third study showed that patients with MCI had increased Bacteroides [12]. These results suggest gut microbiome has changed already even in patients with MCI. However, two of these three studies clearly included patients on medications, such as acetylcholinesterase inhibitors, to improve symptoms [4, 12] and the other study did not provide this information [11]. Although the effects of these medications on gut microbiome are not known, the potential effects of these agents on gut microbiome through gut motility and neuro-endocrinal influence cannot be totally excluded. Thus, studying newly diagnosed patients is necessary to limit the effects of drugs and interventions physicians or the families of patients may have initiated.
We hypothesize that patients with newly diagnosed MCI or AD have similar gut microbiome that is different from that of healthy controls and that the gut dysbiosis in patients with MCI is less severe than patients with AD. To test these hypotheses, fecal microbiome of patients with newly diagnosed AD or MCI and age-matched healthy controls were determined.
MATERIALS AND METHODS
Participants
This study was conducted according to the principle of the Declaration of Helsinki. The protocol was approved by the Ethics Committee of Sun Yat-sen Memorial Hospital, Sun Yat-sen University [protocol number: SYSEC-KY-KS-2018-040]. A total of 60 participants who were 60 years old or older were recruited between August 14, 2018 to April 19, 2019 from the neurology and rehabilitation clinics of Sun Yat-sen Memorial Hospital. All participants were not diagnosed with AD or MCI before, and had never taken acetylcholinesterase inhibitors, such as donepezil, and/or memantine. Among them, there were 20 subjects in each group of cognitive normal control or patients with AD or MCI. All participants enrolled in the study signed the written informed consent.
The clinical assessment and diagnosis of AD dementia and MCI were made by experienced neuro-logists independent from the study, according to the 2018 National Institute of Aging and Alzhei-mer’s Association (NIA-AA) guidelines. Briefly, their cognitive and functional status was assessed based on a neuropsychological battery including the Chinese version of the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Instrumental Activities of Daily Living (ADL), Clinical Dementia Rating (CDR), and Alzheimer’s Disease Assessment Scale-Cognitive section (ADAS-Cog). Hachinski ischemic score and Hamilton depression rating scale were assessed to help exclude diseases of severe neural tissue ischemia, depression, or anxiety. If the neuropsycho-logical measurement results indicated the participants having MCI or probable AD, blood was obtained to test thyroid function, homocysteine, vitamin B-12, folic acid, blood glucose, glycosylated hemoglobin, blood lipid, and syphilis. Brain magnetic resonance spectroscopy was performed as well. These tests and examinations were used to exclude other diseases that may cause cognitive decline.
The exclusion criteria for participating in this study included: 1) a family history of dementia; 2) any other neurodegenerative diseases, such as Parkinson’s disease and amyotrophic lateral sclerosis; 3) enduring mental illness, such as schizophrenia; 4) severe cardiac, pulmonary, hepatic or renal diseases, or any tumor; 5) a history of taking antibiotics or glucocorticoid within six months, and 6) intestinal diseases, such as irritable bowel syndrome.
Fecal sample collection and DNA isolation
Fecal samples were collected in the morning from recruited subjects newly diagnosed with AD or MCI and age-matched healthy controls. Microbial genomic DNA was extracted from fecal pellets using the PowerSoil DNA Isolation Kit (MOBIO Laboratories) according to the manufacturer’s protocols and was stored at –80° for further testing. DNA quality and quantity were assessed by the ratios of 260 nm/280 nm and 260 nm/230 nm, respectively.
16S RNA gene sequencing and analysis
The V3-V4 sequenced regions of the 16S rRNA gene were amplified by PCR. The PCR amplified product was purified, quantified, and normalized to form a sequencing library. The constructed library was first subjected to library quality inspection. Two samples from the AD group and two samples from the healthy control group failed to pass the library quality inspection and were then excluded. Thus, a total of 56 quality-qualified libraries were sequenced using Illumina Miseq/Microseq (Illumina, San Diego, CA, USA). Afterwards, the raw image data files obtained by high-throughput sequencing were converted into the original sequenced reads by base calling analysis and the results were stored in the FASTQ file format that contained sequence information of reads and its corresponding sequencing quality information followed by data processing according to the overlapping relationship among paired-end (PE) reads and the PE sequence of Tags. The quality of reads and the effect of merge were filtered through three steps. Step 1) PE reads splicing: splicing the reads of each sample through overlap using FLASH v1.2.7 software, the obtained splicing sequence was the raw tags data; Step 2) Tags filtering: the raw tags obtained by splicing were filtered by Trimmomatic v0.33 software to get high quality tags data (i.e., clean tags); Step 3) Removal of chimeras: The chimeric sequences were identified and removed using UCHIME v4.2 software to obtain the effect tags. Clustering of Tags at 97% sequence similarity level using UCLUST in QIIME2 software to obtain operational taxonomic unit (OTU) and the OTU was taxonomically annotated based on the Greengene (Release 13.8). 0.005% of all sequence numbers as a threshold was used to filter OTU. The OTU representative sequence was compared with the microbial reference database to obtain the species classification information corresponding to each OTU and then the composition of each sample was counted at each level (i.e., phylum, class, order, family, genus and species). On this basis, the QIIME2 software was used to generate the species abundance table at different classification levels and R package was used to map the community structure plot under the taxonomic level of the sample. Species annotation was performed using the RDP Classifier (version 2.2) with a confidence threshold of 0.8. α-diversity of samples (evenness, faith pd and the Shannon index) and β-diversity [Bray Curtis, unweighted unifrac, weighted unifrac, and principal component analysis (PCA)] were investigated with QIIME2 and R software to compare the similarity of species diversity in different samples. Linear discriminant analysis with effect size (LEfSe) was performed online based on the taxonomic files obtained from the QIIME2 analysis.
Statistical analysis
Continuous parameters, including age, years of education, scores of cognitive tests, and relative abundance of taxa were presented as mean±standard deviation (S.D.). Categorical factors, such as gender and rates of participants with hypertension or diabetes, were presented as percentage (%). Differences among groups were tested with either Chi-square test for category variable or one-way analysis of variance (ANOVA) for continuous variables. One-way ANOVA was followed by post hoc Dunn’s multiple comparison tests for parametric data or Kruskal-Wallis sum-rank test was followed by Dunn’s multiple for non-parametric data. Spearman correlation coefficients were used to detect the relationships between the taxa and clinical data. The Chi-square test, ANOVA and Spearman correlation coefficient were performed by SPSS version 25.0 (SPSS Inc., Chicago, IL) with a p < 0.05 as the significance level.
RESULTS
Subject characteristics
The characteristics of AD, MCI patients and age- and gender-matched cognitively normal controls are shown in Table 1. AD patients had lower MMSE and MoCA scores than MCI patients and healthy controls. These scores of MCI group were also lower than those of the healthy control group. No significant difference was found in the duration of education and the number of patients with hypertension or diabetes among patients with AD or MCI and healthy controls. No subject in the three groups was obese (body mass index > 30).
General characteristics of participants
Results are means (S.D.) or number of individuals (%). *p < 0.05 compared with healthy control group; #p < 0.05 compared with the MCI group. AD, Alzheimer’s disease; BMI, body mass index; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; ADAS-Cog, Alzheimer’s Disease Assessment Scale-cognitive section.
α-diversity and β-diversity
All indices of α-diversity (evenness, faith pd, and Shannon diversity based on OTU levels) were similar among the three groups (Fig. 1A–C). Significant differences in β-diversity were observed based on the Bray curitis and weighted Unifrac analyses. The patients with AD or MCI had a higher β-diversity than healthy controls (Fig. 1D, E). PCA analysis showed that the healthy controls had microbial components different from those of patients with AD or MCI (Fig. 1F).
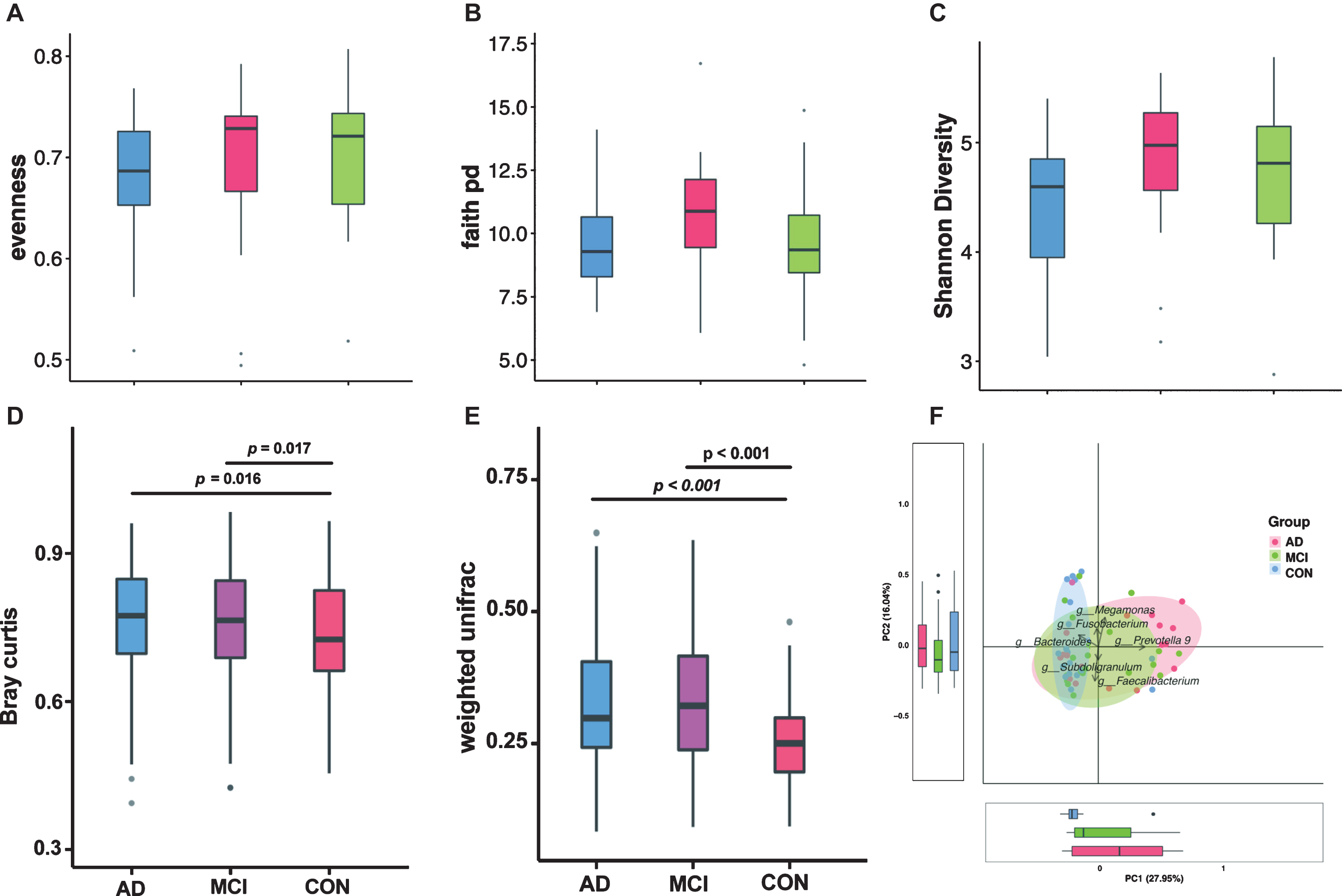
The α-diversity and β-diversity analysis of the gut microbiota in patients with AD (n = 18) or MCI (n = 20), and the healthy controls (n = 18). The evenness (A), faith pd (B), and Shannon diversity (C) of α-diversity and Bray curtis (D), weighted unifrac (E), and PCA (F) of β-diversity analysis are presented. AD, Alzheimer’s disease; MCI, mild cognitive impairment; CON, healthy controls; PCA, principal component analysis.
Composition of gut microbiota at the phylum and genus levels
At the phylum level, Firmicutes, Bacteroidetes, Proteobacteria, Verrucomicrobia, and Fusobacteria were the dominant bacteria (Fig. 2A). There was a difference in the abundance of Protobacteria among the three groups (p = 0.04), while Firmicutes, Bacteroidetes, Verrucomicrobia, and Fusobacteria were not different among the three groups. At the genus level, Bacteroides, Faecalibacterium, Prevotella_9, Megamonas, and Phascolarctobacterium were the dominant genera. There were differences in the relative abundance of Bacteroides (p = 0.037), Blautia (p = 0.041), Lachnospira (p = 0.01), and Prevotella_9 (p = 0.0095) among the groups (Fig. 2B).
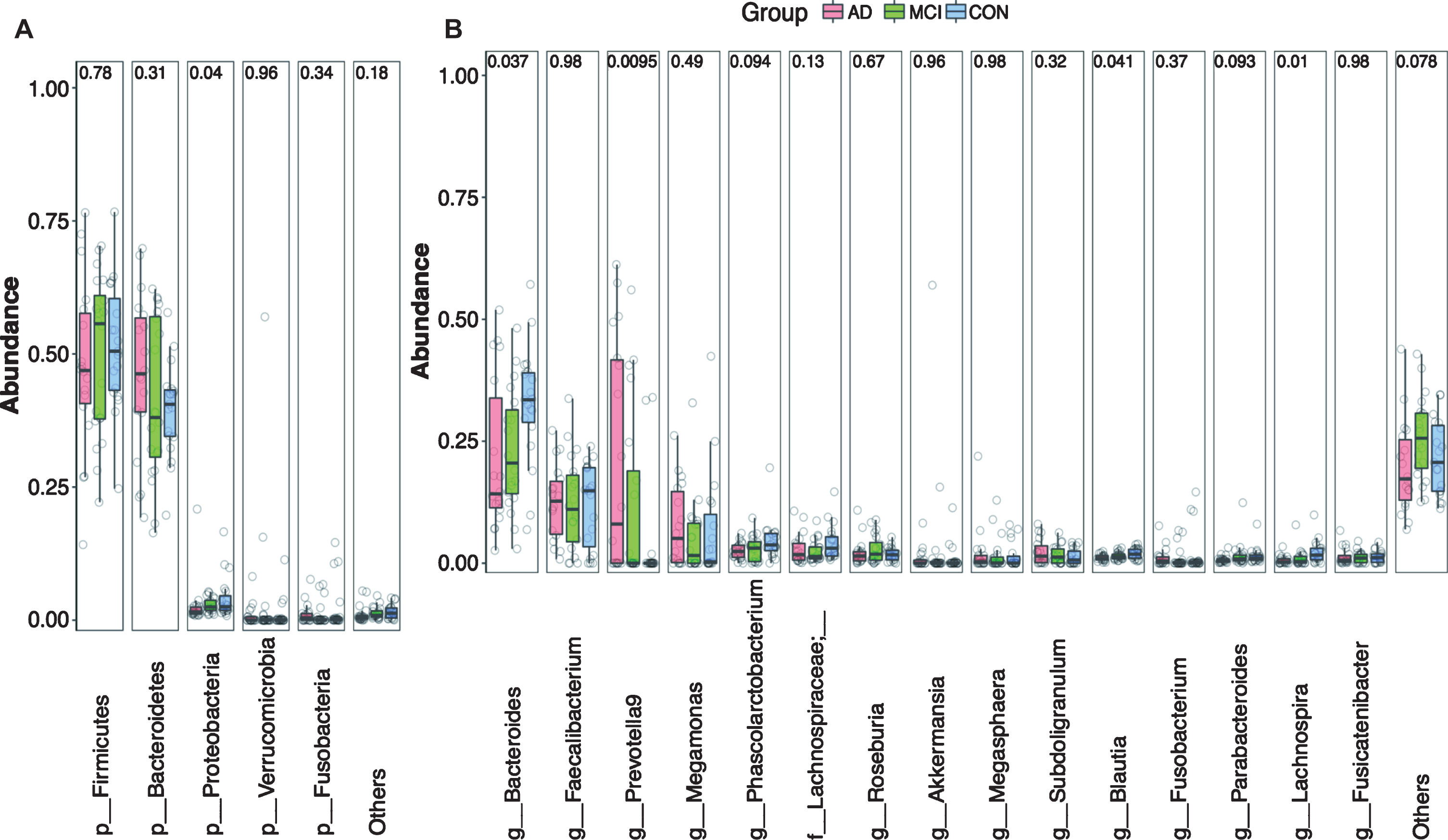
Relative abundance of gut microbial taxa at phylum-level (A) and genus-level (B) in patients with AD (n = 18) or MCI (n = 20) and the normal controls (n = 18). AD, Alzheimer’s disease; MCI, mild cognitive impairment, CON, healthy controls.
Differences in microbiome of patients with MCI or AD
The LEfSe method was used to perform comparison among the AD, MCI, and healthy control groups. Considering the differences in the taxa at all levels with a logarithmic linear discriminant analysis score > 2.0 and a p value < 0.01, we found that the abundance of 39 taxa between AD and control group (Fig. 3A), 26 taxa between MCI and control group (Fig. 3B), and 48 taxa between AD and MCI group (Fig. 3C) were significantly different. Using the Venn diagram, 10 taxa were common in the result of AD versus control and MCI versus control, 14 taxa were common in the result of AD versus control and AD versus MCI and 9 taxa were common in the result of AD versus MCI and MCI versus control. These 10, 14 and 9 taxa belonged to 4, 3 and 2 genera, respectively (Fig. 3D).
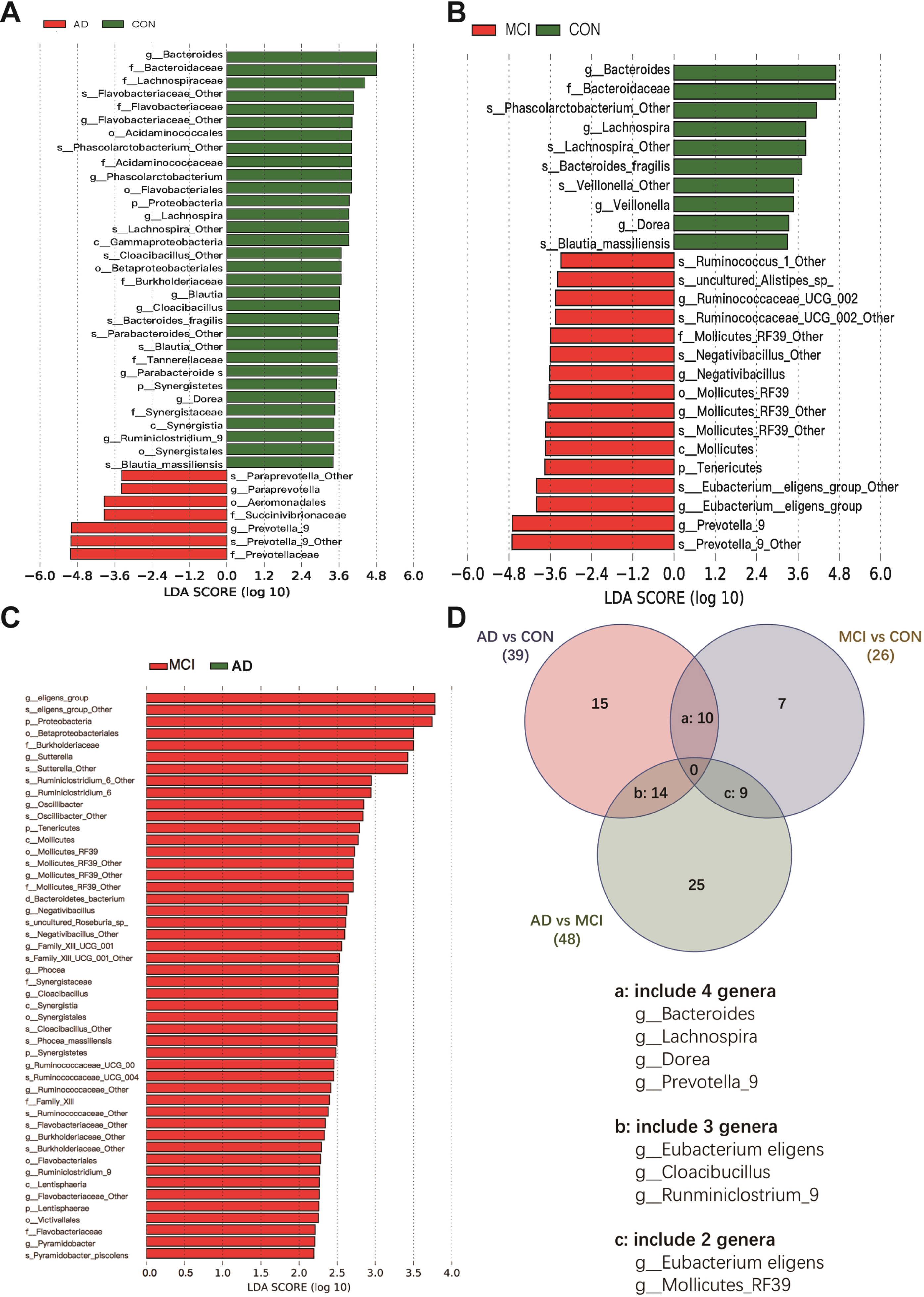
Bacterial taxa with different abundances among three groups. A, B, and C panels are histogram of the LDA scores for genera that were different between the two comparing groups. Panel D is a Venn diagram showing the genera that were different among three groups. AD, Alzheimer’s disease; MCI, mild cognitive impairment; CON, healthy controls; LDA, Linear discriminant analysis.
As described above, Firmicutes and Bacteroidetes at the phylum level were not different among AD, MCI, and control groups (Fig. 4A, B). The ratio of Firmicutes to Bacteroidetes was not different among the three groups (Fig. 4C). We then focused on the taxa at the genus level. The abundance of Prevotella_9 was significantly increased (Fig. 4D) and the abundance of Bacteroides was significantly decreased in the AD group (Fig. 4E) compared with healthy controls. However, the abundance of these two genera in the MCI group was not different from those in the AD group or healthy controls. Interestingly, the ratio of Prevotalla_9 to Bacteroides of the healthy controls was significantly lower than that of MCI group (p = 0.04) or AD group (p = 0.006) (Fig. 4F), indicating that it may be worthwhile to determine whether this ratio has a potential to discriminate individuals with AD or MCI from healthy controls before the intervention for AD or MCI has started. Compared to the healthy controls, the abundance of Lachnospira was significantly decreased in the MCI (p = 0.006) and AD (p = 0.002) group (Fig. 4G). Patients with AD but not those with MCI had a lower abundance of Ruminiclostridium_9 than healthy controls (Fig. 4H). The abundance of Eubacterium eligens group of MCI group was significantly higher than that of AD group (p = 0.0003) or healthy controls (p = 0.024) (Fig. 4I). Further analysis at the species level showed that patients with MCI and AD had a lower abundance of Bacteroides fragilis than control group (Fig. 4J) and that patients with AD had increased Prevotella_9; s_uncultured bacterium compared with control group and patients with MCI (Fig. 4K).
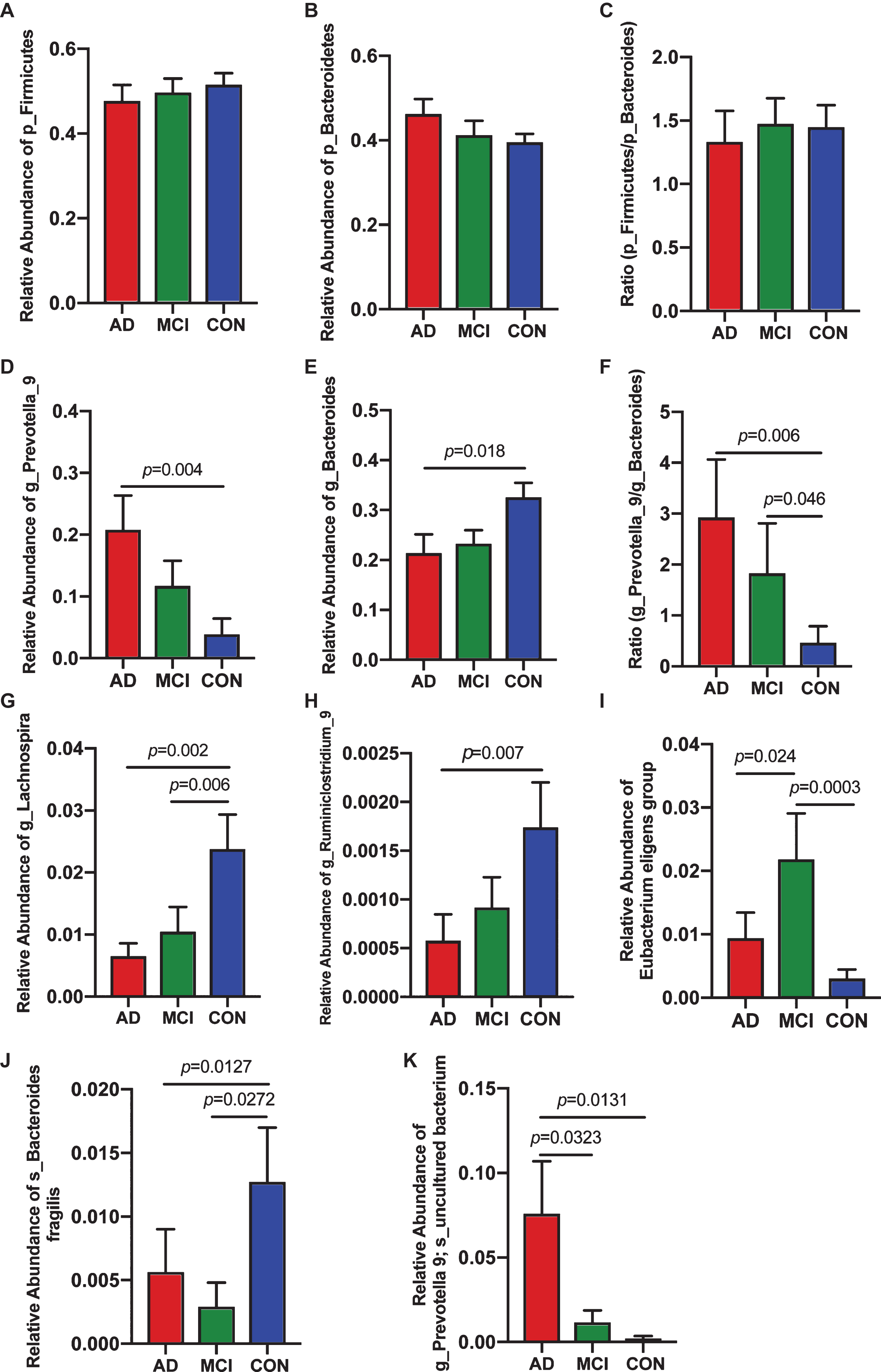
Bacterial genera with different abundances among three groups. A-C) Relative abundance of Firmicutes and Bacteroidetes at the phylum level. C-H) Relative abundance of genera at genus level that were different among three groups. I, J) Relative abundance of genera at species level from g_Bacteroides and g_Prevotella that were different among three groups. AD, Alzheimer’s disease; MCI, mild cognitive impairment; CON, healthy controls; LDA, Linear discriminant analysis.
Correlation between bacterial genera and clinical data
When all subjects from three groups were considered, the abundance of Bacteroides, Lachnospira, and Ruminiclostridium_9 were positively correlated with MMSE and MoCA. The abundance of Prevotella_9 and the ratio of Prevotella_9 to Bacteroides were negatively correlated with MMSE and MoCA scores and positively correlated with ADAS-Cog scores (Fig. 5). Our results showed no significant correlation between the above taxa and age or duration of education when all studied subjects were included (Fig. 5A). However, the abundance of Ruminiclostridium_9 was positively correlated with age in patients with AD (Fig. 5B). The abundance of Prevotella_9 and the ratio of Prevotella_9 to Bacteroides were negatively correlated with MoCA scores in patients with MCI (Fig. 5C). Finally, the abundance of Lachnospira was positively correlated with MMSE in healthy controls (Fig. 5D).
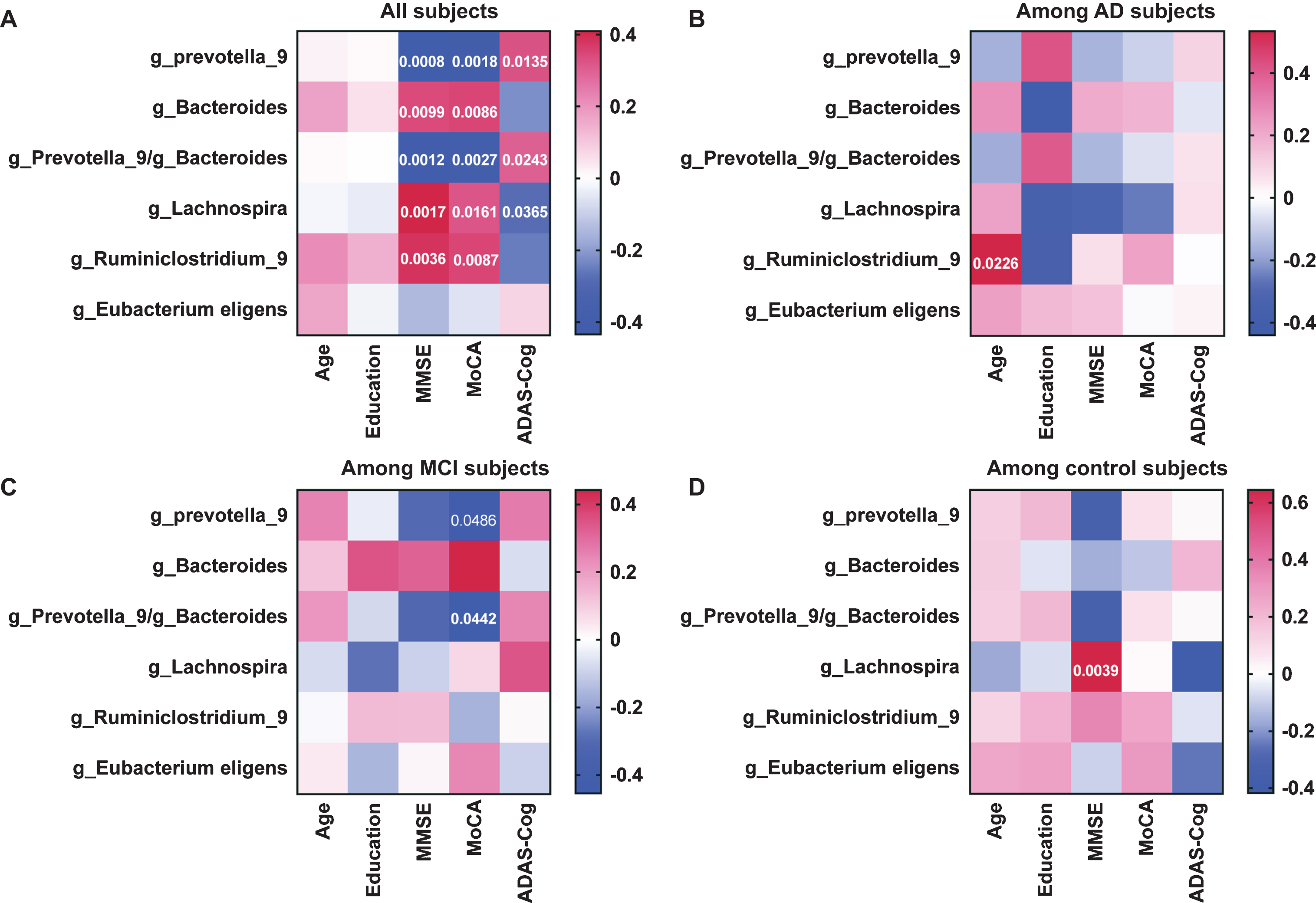
Heatmaps showing correlations between microbiota genera and clinical characteristics. The scale bar showed the Spearman r value. The p values were shown in the blocks. A) All subjects from three groups were included. B) Subjects with AD were analyzed. C) Subjects with MCI were analyzed. D) Subjects of control group were analyzed. MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognitive subscale.
DISCUSSION
We found that patients with MCI or AD had an increased β-diversity compared with healthy controls. Multiple genera including Bacteroides, Prevotella_9, and Ruminiclostridium_9 had a similar direction of changes in patients with AD or MCI when compared with healthy controls. However, the changes in these genera reached significance only in patients with AD but not in patients with MCI. One genus, Lachnospira, was low in patients with AD or MCI compared with healthy controls. The third change pattern is that Eubacterium eligens group was increased in patients with MCI compared with healthy controls and patients with AD. These patterns of changes suggest that patients with MCI and AD have similar changes in gut microbiome but the gut dysbiosis in patients with MCI is less severe than that in patients with AD. Consistent with our findings, a previous study has shown a similar gut microbiome change in patients with AD or MCI [4]. Another study showed significant changes of gut microbiome in patients with MCI compared with healthy controls, but this change was distinguishable from patients with AD [11]. Results of these two previous studies and our study clearly indicate that gut dysbiosis occurs in patients with MCI, a disease stage before the full presentation of AD.
We propose that gut dysbiosis may interact with brain pathological process to form a viscous cycle to facilitate the presentation of AD. The occurrence of gut dysbiosis in patients with MCI cannot be used as evidence to support that gut dysbiosis works as an initiator for AD brain changes. It is known that AD neuropathological changes, such as amyloid-β accumulation, occur years before MCI [9]. Animal studies have shown AD-like mice have gut microbiome changes [6, 13]. Thus, it is likely that the pre-symptomatic AD brain changes can alter gut microbiome. These lines of evidence would suggest that gut dysbiosis is a change subsequent to the AD neuropathology. However, transplantation of healthy mouse feces to AD-like mice improves the neuropathological and behavioral presentation of the AD-like mice [7]. Probiotics improve symptoms of AD patients [14]. These lines of evidence suggest that gut microbiome is important in modulating the pathological processes of AD. Those bacterial genera that have an altered abundance in patients with AD or MCI may be candidates that play a role in modulating the pathological processes of AD or whose change in abundance is simply caused by AD pathology. Although a previous study has attempted to link AD biomarkers, such as amyloid-β concentrations in the cerebrospinal fluid, to gut microbiome [15], there is not enough information in the literature to help us distinguish which role of the four genera whose abundances were altered in AD patients plays. Nevertheless, in our study, Bacteroides abundance was positively correlated with MMSE and MoCA. Similarly, Lachnospira was positively correlated with MMSE and MoCA and negatively correlated with ADAS-Cog. On the other hand, Prevotella_9 was negatively correlated with MMSE and MoCA and positively correlated with ADAS-Cog. These results suggest a potential of using these genera as biomarkers for cognitive functions. Consistent with the findings when data from all subjects of three groups were analyzed, Prevotella_9 was negatively correlated with MoCA in patients with MCI and Lachnospira was positively correlated with MMSE in control group. These results further suggest a role of these two genera in cognitive functions.
We did not find a difference in the abundance in Firmicutes and Bacteroidetes at the phylum level among the three groups of subjects. The ratio of Firmicutes to Bacteroidetes was also not different. Two previous studies have shown that patients with AD have decreased Firmicutes. One of these two studies also showed that patients with AD had increased Bacteroidetes [16] and the other one showed no change in Bacteroidetes in patients with AD [11]. Although the ratio of Firmicutes to Bacteroidetes was not calculated, this ratio shall be decreased in patients with AD in the study showing that these patients had reduced Firmicutes and increased Bacteroidetes. However, another study showed an increased ratio of Firmicutes to Bacteroidetes in patients with dementia compared with non-dementia subjects [17]. It appears that the majority of these non-dementia subjects in the study were MCI sufferers who had increased Bacteroidetes [12] and, therefore, had a decreased ratio of Firmicutes to Bacteroidetes. Thus, the ratio of Firmicutes to Bacteroidetes in patients with dementia may not be different from those in healthy controls in that study, a finding that is similar to ours.
Our results showed at the genus level that Bacteroides was decreased in AD patients, which is similar to a previous study [4]. However, Bacteroides was found to be increased in patients with AD or MCI in other studies [12, 18]. Our study also showed that Bacteroides fragilis was decreased in patients with AD. This bacterial species is a protective bacterial species in one study [19]. However, this bacterium was associated with increased amyloid-β deposition in AD mouse brain in another study [20]. It has been recognized that Bacteroides fragilis can be beneficial or detrimental, depending on the environment [21]. Similar to the complex situation of Bacteroides, Lachnospira of Firmicutes was increased in patients with AD in a previous study [4], but we observed a decrease in Lachnospira in AD patients. The reason for these different findings is not known but our patients are newly diagnosed and have not been on any interventions for AD, which is different from the previous study [4]. Similar to our study, an earlier study showed that patients with AD had reduced Lachnospira [22]. Additional factors, such as dietary and age differences among the subject populations, may also have contributed to the different findings on gut microbiome from various studies.
We showed that the ratio of Prevotella_9 to Bacteroides was increased in patients with AD and MCI. If this finding is validated by future studies, this ratio may be an indicator to discriminate patients with AD or MCI from healthy controls and may suggest that a balance between Prevotella_9 and Bacteroides is important for maintaining a healthy status. This ratio has been used as an indicator of improved glucose metabolism but Prevotella can be pathobiontic for promoting inflammatory responses [23, 24]. Thus, the increase of Prevotella may contribute to the development of neuroinflammation in patients with AD. However, different species of Prevotella may have pro-inflammatory and anti-inflammatory effects [25, 26]. Our results showed that Prevotella_9; s_uncultured bacterium was increased in patients with AD. The functions of these bacteria have not been reported.
Patients with AD had decreased Ruminiclostridium_9 that is a species of Firmicutes and a short-chain fatty acid producer [4]. Short chain fatty acids have been shown to be neuroprotective [27–29]. Thus, the decrease in Ruminiclostridium_9 may increase the susceptibility of patients to various insults. Finally, patients with MCI had increased Eubacterium eligens group. The significance of this increase is not known. However, the Eubacterium eligens group is considered to be probiotic [30]. The increase of Eubacterium eligens group in patients with MCI may be protective and this protective strategy disappears in patients with AD, which may participate in worsening the progress of AD pathology.
Since metabolic disorders, such as diabetes, interact with gut microbiome and may be linked to AD [31, 32], the presence of these disorders can be confounding factors for the interpretation of our findings. However, only one or two subjects in each group had diabetes and none of the subjects had obesity. Thus, the influence of these metabolic disorders in our findings may be small.
One limitation of our study is that we do not know how long patients had suffered from AD before they came to our hospital for care. It is possible that the severity of gut dysbiosis may be different at different stages of AD. All of our patients were newly diagnosed but their duration with AD is difficult to estimate. Staging them based on their signs and symptoms may reduce the power of our study due to a relatively small sample size. Future studies are needed to determine whether gut dysbiosis is worsened with increased severity of AD. Also, all of our subjects in this study are Chinese. The other three studies on the gut microbiome in patients with MCI have subjects in China or Japan [4, 12]. Since diet, geographic location and genetics can affect gut microbiome [33, 34], it is not appropriate to extrapolate our findings or the findings from the other three studies to patients of other origins or locations.
CONCLUSIONS
We have shown that patients newly diagnosed with AD or MCI have gut microbiome changes that include a decrease of potentially protective microbiome and an increase of microbiome that can promote inflammation. Our results support a novel idea that the degree of gut dysbiosis is worsened with the disease stage from MCI to AD.