
Abstract
Background:
Increasing evidence supports an important role of vascular risk in cognitive decline and dementia.
Objective:
This study aimed to examine whether vascular risk was associated with cognitive decline, cerebral hypometabolism, and clinical progression in cognitively intact elders.
Methods:
Vascular risk was assessed by the Framingham Heart Study general Cardiovascular disease (FHS-CVD) risk score. The cross-sectional and longitudinal associations of FHS-CVD risk score with cognition and brain glucose metabolism were explored using multivariate linear regression and linear mixed effects models, respectively. The risk of clinical progression conversion was assessed using Kaplan-Meier survival curves and multivariate Cox proportional hazard models.
Results:
A total of 491 cognitively intact elders were included from Alzheimer’s Disease Neuroimaging Initiative (ADNI) database. Participants with high FHS-CVD risk scores had lower baseline Mini-Mental State Examination (MMSE) (p = 0.009), executive function (EF) (p < 0.001), memory function (MEM) (p < 0.001) scores, and F18-fluorodeoxyglucose positron emission tomography (FDG-PET) uptake (p < 0.001) than those with low FHS-CVD risk scores. In longitudinal analyses, individuals with higher FHS-CVD risk scores had greater longitudinal declines in MMSE (p = 0.043), EF (p = 0.029) scores, and FDG-PET uptake (p = 0.035). Besides, individuals with a higher vascular risk had an increased risk of clinical progression (p = 0.004).
Conclusion:
These findings indicated effects of vascular risk on cognitive decline, cerebral hypometabolism, and clinical progression. Early detection and management of vascular risk factors might be useful in the prevention of dementia.
INTRODUCTION
Dementia is one of the greatest global public health challenges in modern societies [1]. Alzheimer’s disease (AD) is the most common form of dementia which is characterized by a progressive decline in cognitive function. AD is driven by a constellation of genetic and environmental risk factors. Accumulating evidence has indicated a vascular contribution to AD [2–4], with multiple vascular risk factors associated with an increased risk of AD, including hypertension [5], diabetes [6], smoking [7], and hypercholestero-lemia [8]. Besides, it has been reported that only 24% of demented patients have pure AD pathology, whereas vascular alterations can be discovered in more than 50% of patients with clinically diagnosed AD, highlighting the importance of vascular risk factors in the mechanisms underlying AD and dementia [9, 10].
In the 2018 National Institute on Aging-Alzhei-mer’s Association (NIA-AA) Research Framework [11], cognitive decline was used in staging the severity of AD. Several vascular risk factors have been reported to be associated with cognitive function [12–15]. Available evidence supports that amyloid-β (Aβ) burden represents the earliest evidence of AD neuropathologic change [16, 17]. Besides, F18-fluorodeoxyglucose positron emission tomography (FDG-PET) brain metabolism is a biomarker of neurodegeneration [11]. Recently, FDG-PET has been reported to be an independent biomarker for AD biological diagnosis [18]. Studies on the associations of vascular risk with Aβ burden and FDG-PET could be useful for understanding the role of vascular factors in AD.
Considering that the effects of single vascular risk factors on AD are controversial, the Framingham Heart Study general Cardiovascular Disease (FHS-CVD) risk score was a multivariable measure of vascular risk [19]. It represents a quantifiable expression of the factors acting on functional and anatomical changes of macrovessels and microvessels. Therefore, the FHS-CVD risk score can be used to assess general vascular risk. Previous studies had investigated whether FHS-CVD risk score was related to brain atrophy and hypometabolism [20–22], and several studies investigated the association between FHS-CVD risk score and cognitive decline, but with controversial findings [14, 23]. Furthermore, there were inconsistent findings regarding the influence of Aβ burden on cognition or neurodegeneration [21, 25]. In addition, a previous study found that the FHS-CVD risk score could predict the conversion from mild cognitive impairment (MCI) to AD [26], but the association of the FHS-CVD risk score with clinical progression in cognitively intact elders is still unknown.
In this study, our first goal was to investigate the cross-sectional and longitudinal associations of general vascular risk assessed by the FHS-CVD risk score with cognition and brain glucose metabolism as well as whether these associations depended on Aβ burden, in a cohort of cognitively intact elders. Second, we aimed to test the predictive value of the FHS-CVD risk score for the development of clinical progression in cognitively intact elders.
METHODS
ADNI database
Data used in this study were obtained from Alz-heimer’s Disease Neuroimaging Initiative (ADNI) database. The ADNI database was established as an ongoing, longitudinal multicenter study launched in 2003, aiming at developing AD-related biomarkers for early detection and treatment of AD. ADNI was approved by institutional review boards of all participating institutions, and written informed consent was obtained from all participants or their guardians according to the Declaration of Helsinki. More details can be found in previous studies [27, 28] and at http://www.adni-info.org.
Participants
Cognitively intact elders who had available data to calculate the FHS-CVD risk score were included from ADNI-1/GO/2 cohorts at baseline. All participants had a Mini-Mental State Examination (MMSE) score from 24 to 30 and a global Clinical Dementia Rating (CDR) score of 0 at baseline. All participants received an MRI scan at 1.5 Tesla signal strength, among whom 50% received an FDG PET scan at bas-eline, and all the subjects had to be able to complete a 3-year imaging study [27]. The inclusive and exclusive criteria for participants in ADNI were described in a previous study [27]. A total of 491 ADNI participants were included in the present study, including 139 Apolipoprotein E (APOE) ɛ4 carriers and 352 non-carriers.
FHS-CVD risk score
FHS-CVD risk score is calculated based on age, gender, medicine for hypertension, systolic blood pr-essure (SBP), total cholesterol (Total-C), high-den-sity lipoprotein cholesterol (HDL-C), smoking status, and medical history of diabetes at baseline [19]. FHS-CVD risk score is a sex-specific risk score with different points in each variable for males and females. The score for age ranges from 0 to 12; SBP –3 to 7; Total-C 0 to 5; HDL-C –2 to 2; smoking 0 to 3; and diabetes 0 to 4 in females. And in males, the score for age ranges from 0 to 15; SBP –2 to 5; Total-C 0 to 4; HDL-C –2 to 2; smoking 0 to 4; and diabetes 0 to 3. The total FHS-CVD risk score ranged from –5 to 33 for females and ranged from –4 to 33 for males. The detailed method of calculating the FHS-CVD risk score has been described in a previous study [19].
FDG-PET image processing
Global brain glucose metabolism of participants was measured by FDG-PET. In ADNI database, the FDG-PET scans were obtained and the mean FDG-PET uptake was averaged over right and left angular gyri, right and left inferior temporal regions, and bilateral posterior cingulate as regions of interest (metaROIs) which were sensitive to AD-related cha-nges in metabolism [29, 30]. PET images were spatially normalized in statistical parametric mapping (SPM) to the MNI PET template. The mean counts were extracted from the 5 metaROIs for each subject’s FDG scans at each time point, computing the intensity values with SPM subroutines [30]. Then, each metaROI mean was intensity-normalized by dividing it by pons/vermis reference region mean. Preprocessing steps were performed to mitigate inter-scanner variability, including dynamic co-registrat-ion of images acquired in consecutive time frames, averaging, reorientation along the anterior-posterior commissure and filtering with a scanner specific filter function to produce images of a uniform isotropic resolution of 8 mm full width at half maximum Gaussian el [18, 30]. A detailed description of FDG-PET image acquisition and processing can be found at http://adni.loni.usc.edu/data-samples/pet/.
Cognitive measures and clinical progression
MMSE, executive function (EF), and memory function (MEM) scores were all included to assess cognition using the neuropsychological battery from the ADNI database. The MMSE score indicates the global cognitive function of participants. EF score in ADNI database was assessed using Category Fluency, WAIS-R Digit Symbol, Trails A & B, Digit Span Backwards, and clock drawing. MEM score in the ADNI database was assessed using relevant items of the Rey Auditory Verbal Learning Test (RAVLT), ADAS-Cog, Logical Memory, and MMSE. Participants were defined as having clinical progression if their clinical status (cognitive normals progressed to MCI or dementia) changed [31].
Measurements of Aβ burden
In our study, we used cerebrospinal fluid (CSF) Aβ42 levels to represent Aβ burden. In ADNI, CSF procedural protocols have been described in a previous study [28]. In brief, baseline CSF Aβ42 was measured at the ADNI Biomarker Core Laboratory by the INNOBIA AlzBio3 immunoassay (Fujirebio, Belgium) with a within-batch precision value of 5.1–7.8%.
Statistical analyses
Participants were classified into high and low FHS-CVD risk score groups according to a threshold of >20% for predicted risk in 10 years which required more aggressive risk factor modification (e.g., FHS-CVD risk score of 17 for women and FHS-CVD risk score of 14 for men) [19]. Baseline demographic factors of this study were compared by Chi-square tests for categorical variables and Kruskal-Wallis test for continuous variables. In case of skewed distribution (Kolmogorov-Smirnov test <0.05) for dependent variables, log10-transformed was performed to approximate a normal distribution. Data were missing for EF score (n = 15, 3.1%), MEM score (n = 15, 3.1%), FDG-PET (n = 128, 26.1%), and CSF Aβ42 (n = 135, 27.5%) at baseline. In our cross-sectional study, the associations of FHS-CVD risk score with cognitive scores, FDG-PET uptake and CSF Aβ42 were explored using multivariate linear regression analyses (using low FHS-CVD risk score group as a reference). The longitudinal associations of baseline FHS-CVD risk score with cognitive scores, FDG-PET uptake and CSF Aβ42 were explored using linear mixed effects models. The longitudinal study eventually included 476 participants for MMSE score, 475 participants for EF score, 476 participants for MEM score, 202 participants for FDG-PET, and 176 participants for CSF Aβ42 (at least one follow-up during 4 years). As age and gender had been incorporated into the FHS-CVD risk score model, the above analyses were adjusted for years of education and APOE ɛ4 status at baseline. All outcome variables in linear mixed-effects models were standardized to z scores to facilitate comparisons between modalities. To investigate the effects of Aβ burden on the associations of the FHS-CVD risk score with cognition and brain glucose met-abolism, we additionally adjusted for baseline CSF Aβ42. Finally, Kaplan-Meier survival curves were plotted with log-rank tests to compare the probabilities of conversion to clinical progression between low and high FHS-CVD risk score groups, and multivariate Cox proportional hazard models were further used to test the predictive ability of FHS-CVD risk score for clinical progression (adjusted for years of education and APOE ɛ4 status at baseline). As for the clinical progression cohort, 476 participants had finished follow-up exam over 4 years. R version 3.5.1 was used for statistical analyses and figure preparation. And p < 0.05 was considered significant in these analyses.
RESULTS
Characteristics of participants
The baseline demographic characteristics are shown in Table 1. In brief, 491 cognitively intact individuals were included from the ADNI with a mean age of 74.18±5.79 at baseline. Participants were divided into high and low vascular risk groups according to the FHS-CVD risk score, and there were 241 participants (49.08%) having high vascular risk. The longitudinal distributions of the samples were concluded in Supplementary Table 1. The average duration of follow-up for MMSE score cohort was 1.36±1.27 years, EF score cohort 1.41±1.31 years, MEM score cohort 1.41±1.31 years, FDG-PET imaging cohort 1.26±1.17 years, CSF Aβ42 cohort 1.16±1.20 years, and clinical progression cohort 1.35±1.26 years.
Demographic information
p values of between-group comparisons were obtained using the Chi-square tests for categorical variables and Kruskal-Wallis test for continuous variables. APOE, apolipoprotein E; MMSE, Mini-Mental State Examination; Total-C, total cholesterol; HDL-C, high-density lipoprotein cholesterol; SBP, systolic blood pressure; FHS-CVD, Framingham Heart Study general cardiovascular disease; EF, executive function; MEM, memory function; FDG-PET, F18-fluorodeoxyglucose positron emission tomography; CSF, cerebrospinal fluid; Aβ, amyloid-β. *Data were missing for EF (n = 15, 3.1%), MEM (n = 15, 3.1%), FDG-PET (n = 128, 26.1%), CSF Aβ42 (n = 135, 27.5%).
Associations of FHS-CVD risk score with cognitive scores and FDG-PET at baseline
After adjusting for educational level and APOE ɛ4 status, we found that participants with high FHS-CVD risk scores had lower MMSE (p = 0.009), EF (p < 0.001), and MEM (p < 0.001) scores at baseline than those with low FHS-CVD risk scores (Table 2). In addition, we found participants with high FHS-CVD risk scores had lower FDG-PET uptake than those with low FHS-CVD risk scores (p < 0.001) (Table 2).
Associations of FHS-CVD risk score with baseline cognitive scores and brain glucose metabolism
Cross-sectional associations of FHS-CVD risk score with cognitive scores and brain glucose metabolism at baseline were tested by multiple linear regression models. All models were adjusted for education and APOE ɛ4 status at baseline. FHS-CVD, Framingham Heart Study general cardiovascular disease; MMSE, Mini-Mental State Examination; EF, executive function; MEM, memory function; FDG-PET, F18-fluorodeoxyglucose positron emission tomography; APOE, apolipoprotein E.
Longitudinal associations of baseline FHS-CVD risk score with cognitive scores and FDG-PET
The longitudinal associations of FHS-CVD risk score with cognitive scores and FDG-PET uptake are shown in Fig. 1. We found that individuals with high FHS-CVD risk score showed faster decline in MMSE (p = 0.043) and EF (p = 0.029) scores than those with low FHS-CVD risk score (Fig. 1A, B). Besides, compared to low FHS-CVD risk score group, a higher FHS-CVD risk score was associated with a faster decline in FDG-PET uptake (p = 0.035) (Fig. 1D). But there was no significant association of FHS-CVD risk score with MEM score over 4 years (p = 0.372) (Fig. 1C).

Longitudinal associations of baseline FHS-CVD risk score with cognitive scores and FDG-PET. Compared to low FHS-CVD risk score group, individuals with higher FHS-CVD risk scores showed faster declines in MMSE score (A), EF score (B), and FDG-PET uptake (D). No significant association of the FHS-CVD risk score with MEM score (C) over time was found.
Effects of Aβ burden on associations of FHS-CVD risk score with FDG-PET and cognitive scores
We found no associations between the FHS-CVD risk score and CSF Aβ42 levels (p = 0.780) at baseline after comparing the high and low FHS-CVD risk score groups. Longitudinally, CSF Aβ42 levels were also not found to be associated with the baseline FHS-CVD risk score over 4 years (p = 0.567). Besides, we found that the cross-sectional and longitudinal associations between the FHS-CVD risk score with FDG-PET uptake and cognition scores were not affected after additionally adjusting for baseline CSF Aβ42 (Supplementary Tables 2 and 3).
FHS-CVD risk score and risk of clinical progression
In the clinical progression cohort, 57 participants eventually had clinical progression (only 2 progressed to dementia) with an average time to progression of 2.12±1.15 years, including 19 participants (average time to progression of 2.05±0.96 years) in the low risk group and 38 participants (average time to progression of 2.16±1.24 years) in the high risk group. Kaplan–Meier survival curves showed that individuals with high FHS-CVD risk scores had faster rates of progression than those with low FHS-CVD risk scores (p = 0.005) (Fig. 2). This result was further confirmed by multivariate cox proportional hazard models. Participants with higher FHS-CVD risk scores were at an increased risk of clinical progression compared to those with lower risk scores (HR = 2.28, 95% CI: 1.31–3.99, p = 0.004) (Supplementary Table 4) after adjustment for education and APOE ɛ4 status at baseline.
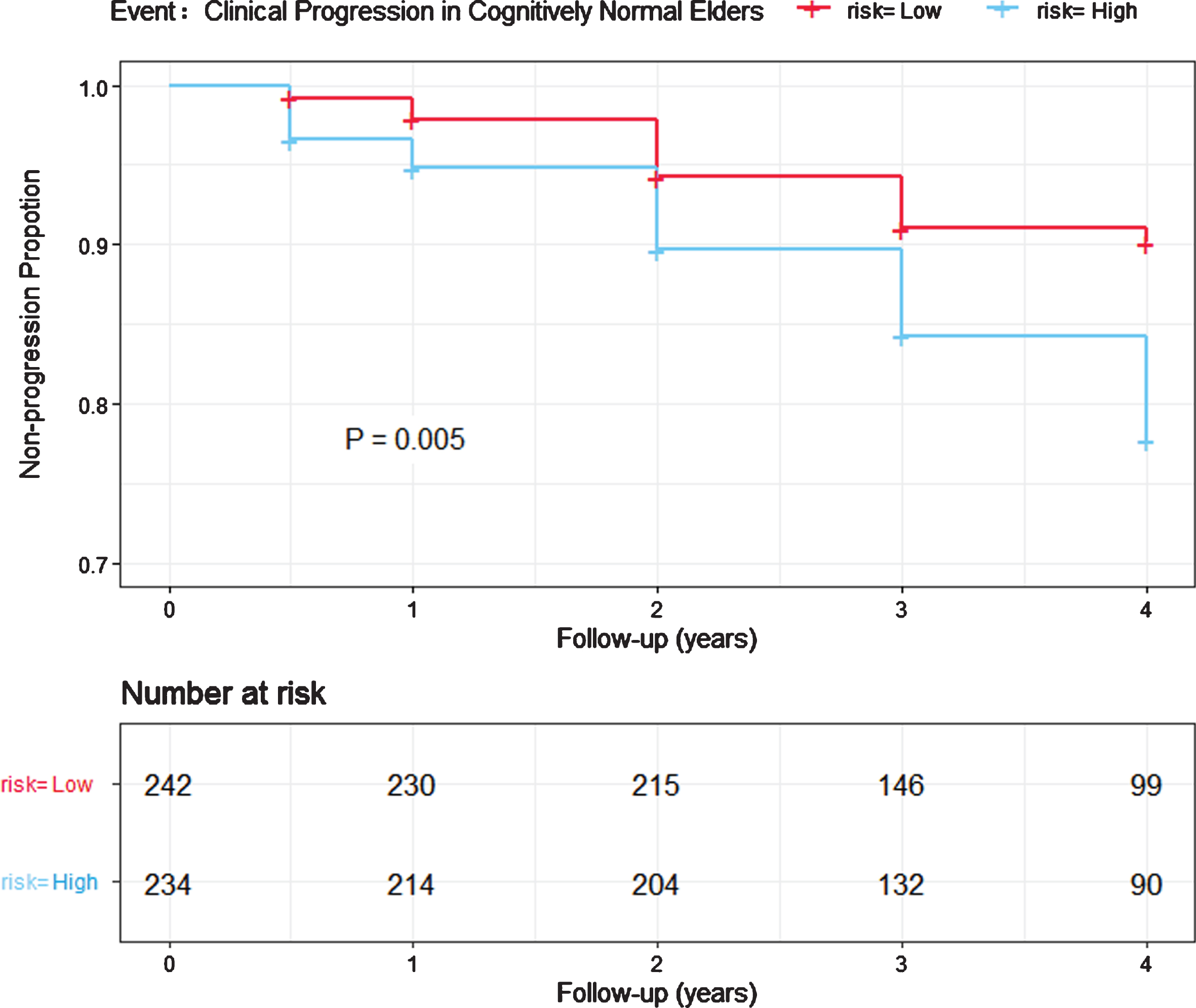
Association between baseline FHS-CVD risk score and clinical progression. The progression rate of individuals with high FHS-CVD risk scores was much higher than that of individuals with low FHS-CVD risk scores (p = 0.005).
DISCUSSION
In cognitively normal older individuals, our main findings are as follows: 1) increased FHS-CVD risk scores were associated with cognitive decline and cerebral hypometabolism both cross-sectionally and longitudinally; 2) patients with higher FHS-CVD risk scores were at an increased risk of clinical progression in cognitively intact elders.
Previous studies have demonstrated that single vascular risk factors could contribute to cognitive decline [32]. Higher general vascular risk assessed by the FHS-CVD risk score was associated with memory impairment and deterioration of executive function [14, 21]. In the Framingham Offspring Study, the associations between similar multivariable vascular risk algorithms and the risk of cognitive decline in healthy adults were also reported [33, 34]. Our results indicated that vascular burden could impair cognitive function, which was consistent with the above studies. In longitudinal analysis, higher vascular risk was found to be associated with a faster decline in EF score. However, we did not find any association between vascular risk and MEM score. This is consistent with previous studies showing that many patients with vascular cognitive impairment or vascular dementia might exhibit impaired executive functions but not memory deficits especially in early stage [35, 36]. Neuroimaging studies also showed that new lacunes could cause a steeper decline in cognitive functions, especially in executive function [37]. Additionally, our study was the first to find that cognitively intact elders with increased FHS-CVD risk scores were more likely to have clinical progression to MCI or dementia, further indicating an important role of vascular risk in cognitive decline and dementia development.
Several potential mechanisms in which vascular burden leads to cognitive decline have been identified. Diminished cerebral glucose metabolism was proved to occur before neurodegenerative changes and cerebral atrophy [38], and it could predict cognitive decline years before clinical diagnosis of AD [39]. Decreased FDG-PET uptake was considered as a biomarker of brain hypometabolism. The Harvard Aging Brain Study found that higher FHS-CVD risk scores were associated with widespread cerebral hypometabolism [21]. Our study also found that FHS-CVD risk score was associated with a faster decline in FDG-PET uptake, which was consistent with previous studies. This also suggested that an increased FHS-CVD risk score might play an important role in the early stages of AD. In addition, impaired FDG-PET uptake could also reflect dysfunction in blood-brain barrier (BBB) transport systems [40, 41]. BBB breakdown has been proved to be an early biomarker of human cognitive dysfunction, independent of Aβ and tau [42]. Studies indicated a significant association of cerebrovascular abnormalities (especially BBB dysfunction) with the onset and progression of AD [43]. Moreover, a higher FHS-CVD risk score also reflected accelerated vascular aging, which would damage intracranial vessels and further lead to reduced cerebral blood flow (CBF). Previous studies showed that reduced CBF would cause cognitive decline [44]. Besides, we found no association between FHS-CVD risk scores and CSF Aβ42 levels, which was in line with previous studies [14], suggesting separate pathophysiological amyloid and vascular pathways to enhance neurodegeneration and cognitive decline [24, 25]. Vascular burden leading to cognitive decline is not affected by Aβ burden, which is consistent with previous longitudinal studies showing that amyloid-positive individuals did not show clear evidence of cognitive decline [45, 46]. To sum up, an increased FHS-CVD risk score played an important part in cognitive decline and dementia.
Previous studies on single vascular risk factors failed to demonstrate a clear and reliable association with cognitive impairment [47]. FHS-CVD risk score is an easy and reliable tool for a global assessment of vascular burden. Most of the items considered in the scale are potentially treatable. Findings from this work have potential implications for early detection and integrated management of vascular risk factors as well as for developing primary and secondary prevention strategies. Although promising, our findings should be considered preliminary, and further independent evaluation is necessary.
Several limitations should be mentioned. Firstly, vascular risk interventions may modify the associations, but it is challenging to collect data on vascular risk factors in longitudinal observational studies and therefore we did not investigate vascular risk interventions. Secondly, ethnic homogeneity of our mainly Caucasian sample limits the generalizability of these results to other populations with different ethnic backgrounds. Moreover, after multiple corrections, the longitudinal associations of baseline FHS-CVD risk score with cognitive scores and FDG-PET became non-significant. Considering that there was loss to follow-up to a certain extent in the longitudinal data which might reduce the trend of the longitudinal associations, our results were still of certain suggestive value. Further validation should be performed in large-scale cohort studies with adequate follow-up. Lastly, the role of FHS-CVD risk score in the cognitive function of middle-aged or elderly people is still controversial, but most subjects in our study were elderly people. Thus, more young and multiracial participants should be involved in future studies and further stratified analyses should be conducted. Moreover, further studies are required to investigate whether a reduction in the FHS-CVD risk score is a new therapeutic target for decreasing the risk of cognitive deterioration and dementia.
In summary, we found that a higher FHS-CVD risk score was associated with poorer cognitive performance, lower brain glucose metabolism as well as an increased risk of clinical progression in cognitively normal elders. This finding indicates that early detection and integrated management of vascular burden might be effective in combating cognitive decline and protecting brain health.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the Nat-ional Natural Science Foundation of China (8101274) and Qingdao Applied Basic Research Project (18-2-2-43-jch).
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Gr-ant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Assoc-iation; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Ins-titutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.