
Abstract
Background:
Unawareness of disease is a common feature of Alzheimer’s disease (AD), but few studies explored its neural correlates. Additionally, neural correlates according to the object of awareness are unexplored.
Objective:
To investigate structural brain correlates in relation to different objects of awareness.
Methods:
27 people with AD underwent MRI scanning on a 3T Siemens Prisma. T1-MPRAGE was used to investigate cortical thickness and white matter microstructure was defined by DTI as fractional anisotropy, mean, axial, and radial diffusivity. Preprocessing used FreeSurfer6.0, ExploreDTI, and FSL-TBSS. Awareness of disease, cognitive deficits, emotional state, relationships, and functional capacity were assessed with the short version of the Assessment Scale of Psychosocial Impact of the Diagnosis of Dementia. Voxel-wise correlations between brain structure and awareness were determined by FSL-PALM. Analyses were corrected for multiple comparisons using Threshold Free Cluster Enhancement and FWE.
Results:
Lower left hemisphere cortical thickness was related to poorer disease awareness uncorrected and corrected for age, sex, and MMSE. In the uncorrected model, mainly right-sided, but also left temporal lower cortical thickness was related to decreased awareness of cognitive deficits. Correcting for age, sex, and MMSE eliminated correlations for the right hemisphere, but extensive correlations in the left hemisphere remained. For white matter integrity, higher right hemisphere MD was related to lower cognitive awareness deficits, and lower FA was related to lower functional capacity awareness.
Conclusion:
Findings suggest that extensive regions of the brain are linked to self-awareness, with particular frontal and temporal alterations leading to unawareness, in agreement with theoretical models indicating executive and mnemonic forms of anosognosia in AD.
Keywords
INTRODUCTION
Lack of awareness regarding the disease or its deficits, also called anosognosia, is a common feature of people with Alzheimer’s disease (AD) [1]. It is considered a multifaceted phenomenon, being influenced by neurocognitive [2] and psychosocial factors [3], and ranging from a slight minimization of difficulties to a complete denial of problems [4]. Anosognosia has been related to different negative consequences for individuals with AD, such as diminished treatment adherence [5], increased engagement in high-risk situations [6, 7], earlier institutionalization [8, 9], and for their caregivers, increased caregiver burden [6, 10–13].
Studies exploring the neuroanatomical correlates of anosognosia in individuals with AD have highlighted associations with various regions: frontal [14, 15], temporal, including the hippocampus [16, 17], and also midline structures such as the cingulate cortex [18–20]. One possible explanation for the discrepancy in results regarding the neural different objects (e.g., cognitive difficulties, emotional changes, behavioral symptoms). In fact, awareness is considered a multidimensional phenomenon [21]. It has been shown that patients with AD may present anosognosia for some deficits but preserved awareness of other difficulties [22–26].
In support of these findings, factorial analysis showed that instruments measuring unawareness can be divided into various factors [27–29]. For example, analyzing the Assessment Scale of Psychosocial Impact of the Diagnosis of Dementia (ASPIDD) [30], Dourado et al. [27] highlighted a four-factor division: awareness for activities of daily living, awareness of cognitive functioning and health condition, awareness of emotional state, and awareness of social functioning and relationships.
In addition, considering that awareness is a broad and multidimensional concept, it might rely not on single areas of the brain but on the connectivity between different regions. In fact, studies have shown that lack of awareness in patients with AD was related to functional disconnections between cortical midline regions [31], the medial prefrontal cortex and other regions of the prefrontal cortex [32], and between the posterior cingulate cortex and the orbitofrontal cortex [33]. Using diffusion tensor imaging (DTI) techniques, which provide information about white matter tracts, some recent studies in patients with schizophrenia highlighted that impaired awareness was also related to diminished structural connectivity [34, 35]. However, to date, no studies have explored the association between brain structural connectivity, especially using DTI, and awareness in dementia.
Despite the consensus in the literature regarding the multifaceted characteristic of anosognosia, to our knowledge, no previous studies examined the neural correlates of awareness according to its object. Additionally, DTI has not been used in relation to awareness in AD. Finally, studies on neural correlates of awareness in AD were almost exclusively conducted in developed regions, with more homogeneous educational level. Accordingly, the aim of the present study was to investigate the neuroanatomic substrates of awareness in AD patients using DTI in a sample with a heterogeneous educational level. The ASPIDD, used in the current study, allows us to examine the neuroanatomic associations of different objects of awareness. Considering both previous findings regarding neural substrates of anosognosia and the multidimensional nature of awareness, we expected to find an association between awareness and white matter integrity and, additionally, we hypothesized this association to differ according to the object of awareness.
MATERIALS AND METHODS
Participants
Twenty-seven participants with mild to moderate AD were included in the study, recruited from the Center for Alzheimer’s disease and Related Disorders (CDA) of the Institute of Psychiatry of the Federal University of Rio de Janeiro (IPUB/UFRJ), Brazil. The clinical diagnosis of AD was made by a psychiatrist using clinical interviews with the patients and caregivers, cognitive screening tests, laboratory tests, and imaging. The participants were diagnosed with possible or probable AD according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR) [36] and National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria [37, 38]. Exclusion criteria were history of other neurological disorder (also excluding cases with mixed AD and vascular dementia); history of head injury resulting in loss of consciousness for more than an hour; history of alcohol or substance abuse (based on ICD-10 criteria); and history of diagnosed major psychiatric illness or current psychological comorbidity (for example, mood disorder).
Instruments
Background variables
In addition to sociodemographic variables, global cognitive functioning was assessed with the Mini-Mental State Examination (MMSE) [39, 40]. Short-term and working memory were measured, respectively, with the forward and backward digit span test [41, 42].
Awareness measure
The short version of the Assessment Scale of Psychosocial Impact of the Diagnosis of Dementia (ASPIDD-s) [43] was applied to assess awareness of disease, cognitive deficits, emotional state, relationships, and functional capacity. People with AD and their caregivers answered the same questions separately and the number of discrepant responses was calculated, generating scores for the full scale and each domain (cognitive, affective, social, and activities of daily living [ADL]). The ASPIDD-s is composed of 12 items (3 for each domain), with scores in each item ranging from 0 to 3 (0 to 36 for the full scale), with higher scores indicating more impaired awareness. No cut-offs were used to categorize participants as anosognosic or not, considering that anosognosia is a graded, and not a binary phenomenon [1].
Neuroimaging
All participants underwent MRI-scanning on a 3T Siemens MAGNETOM Prisma, using a 64-channel head coil. For this study, a high-resolution 3D T1 Magnetization Prepared Rapid Gradient Echo (T1-MPRAGE; repetition time: 2,300 ms; echo time: 2,27 ms; flip angle: 8°; field of view: 250 mm; 1mm isotropic voxels) was used to investigate cortical thickness. A 3D Echo Planar Imaging (EPI) Diffusion Tensor Imaging (DTI) sequence (repetition time: 6,800 ms; echo time: 61 ms; field of view: 220 mm; 5 b = 0 s/mm2 (1 at the beginning and 4 at the end of acquisition) with 30 collinear directions at b = 1000 s/mm2; 64 slices; EPI factor: 110; 2 mm isotropic voxels) was used to measure white matter microstructure.
Cortical thickness
Cortical thickness was analyzed using FreeSurfer version 6.0 (http://surfer.nmr.mgh.harvard.edu). The pipeline has been described extensively before [44, 45]. In short, T1 images were first linearly registered to Talairach space to compute seed points. Then a correction was applied for bias field inhomogeneity, the skull was stripped and an initial white matter surface was generated using volumetric classification. From Talairach space, cutting planes to separate the hemispheres were obtained. The initial white matter surfaces were nudged into the direction of the gradient to find the white and gray matter and pial surface. Lastly, the cortical surfaces were automatically labeled by nonlinear surface-based registration of the Desikan-Killiany atlas [46]. The resulting surfaces and segmentations were manually checked and corrected if necessary. In 13 patients leftover skull was manually removed and surfaces were recalculated. In 3 patients the white matter was manually corrected and control points were added to recalculate white matter and surface information.
White matter microstructure
DTI images were processed using ExploreDTI version 4.8.6 [47]. First, all images were corrected for signal drift using the b = 0 s/mm2 images as a reference [48], Gibbs ringing artifacts were corrected [49], and if present Venetian Blinds were closed [50]. Both DTI and T1 images were then cropped to remove non-brain data, and DTI-images and b-matrix were ordered so that all b = 0 volumes were at the beginning. Lastly, DTI images were corrected for subject motion and eddy currents, the b-matrix was rotated [51], and images were non-linearly warped to the participant’s T1-scan to correct for EPI deformations [52].
After preprocessing every participant’s fractional anisotropy (FA), axial diffusivity (AxD; λ1), radial diffusivity (RD; mean λ2 and λ3), and mean diffusivity (MD; mean λ1, λ2, and λ3) were extracted. FSL’s 6.0.1 Tract-Based Spatial Statistics (TBSS) was used for further analysis (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/) [53]. All FA-images were non-linearly registered to a common space template. Then a mean FA image was created and thinned to create the mean FA skeleton. This skeleton was based on group-specific and represented the center of all tracts common to this group. The subjects-specific FA-image was then projected onto this skeleton and thresholded at FA > 0.20. The nonlinear registrations and FA-skeleton were used to warp AxD, RD, and MD images onto the group-specific skeleton.
Data analysis
Descriptive statistics were generated to illustrate the sample characteristics. Voxel-wise correlations between gray and white matter structure and awareness were determined by FSL-PALM version alpha108 [54], using a non-parametric permutation testing approach. The correlations between the full and subscale scores of awareness and MRI-parameters were calculated both uncorrected and corrected for age, sex, and MMSE score, using 5000 permutations and the PALM acceleration option. The acceleration option allows for the use of a lower amount of permutation with a confidence interval around the p-value that is similar to that of much higher numbers of permutations [55]. Analyses were corrected for voxel-wise multiple comparisons using Threshold Free Cluster Enhancement (TFCE) and Family-Wise Error (FWE). A pFWE < 0.05 was considered statistically significant. Statistical analyses were conducted using SPSS v. 26 [56].
Ethical issues
All participants and their caregivers signed consent forms before taking part in the project. The project was approved by the Federal University of Rio de Janeiro (UFRJ)/Institute of Psychiatry Ethics Committee (Research Ethics Committee number 536.634) and all individuals provided informed consent prior to participation.
RESULTS
Sample characteristics
The sociodemographic and clinical characteristics of the participants can be seen in Table 1. The sample had a fairly well-balanced gender distribution, with an age range within typical values found in the literature. Educational level reflected the heterogeneity found in developing regions. Regarding clinical variables, participants ranged from mild to moderate dementia, accounting for lower educational achievement, and had scores indicative of memory impairment in the digit span test. ASPIDD-s scores were suggestive of unawareness (positive scores, indicating overestimation of abilities), regardless of the object.
Demographic and clinical profile of the sample
* # female/male; mv, missing values.
Cortical thickness
Awareness of disease
First, the correlation was tested between awareness of disease (ASPIDD-s total score) and cortical thickness. In the model uncorrected for age, sex, and MMSE score, lower awareness of disease was related to lower cortical thickness in the left postcentral, superior, middle, and inferior temporal and parahippocampal and fusiform, superior and inferior parietal and supramarginal, insula regions (all pFWE < 0.05, Fig. 1). The correlation strength ranged between r = –0.33 and r = –0.73. In the right hemisphere cortical thinning of the superior, middle, and inferior temporal regions was also related to lower disease awareness (all pFWE < 0.05, [min –max: r = –0.38 ––0.61], Fig. 1). After correction for age, sex, and MMSE score, the correlation between lower disease awareness and cortical thinning was found in the same regions as in the uncorrected analysis, and further extended into the left precentral gyrus, and the left lingual, superior, middle, and orbitofrontal, and rostral anterior cingulate cortices (all pFWE < 0.05, min-max: r = –0.28 –r = –0.75], Fig. 1). The right temporal correlations were no longer statistically significant (pFWE > 0.05). In summary, although widespread correlations were found in both hemispheres, those in the left hemisphere were most robust and survived adjustments for age, sex, and MMSE score.
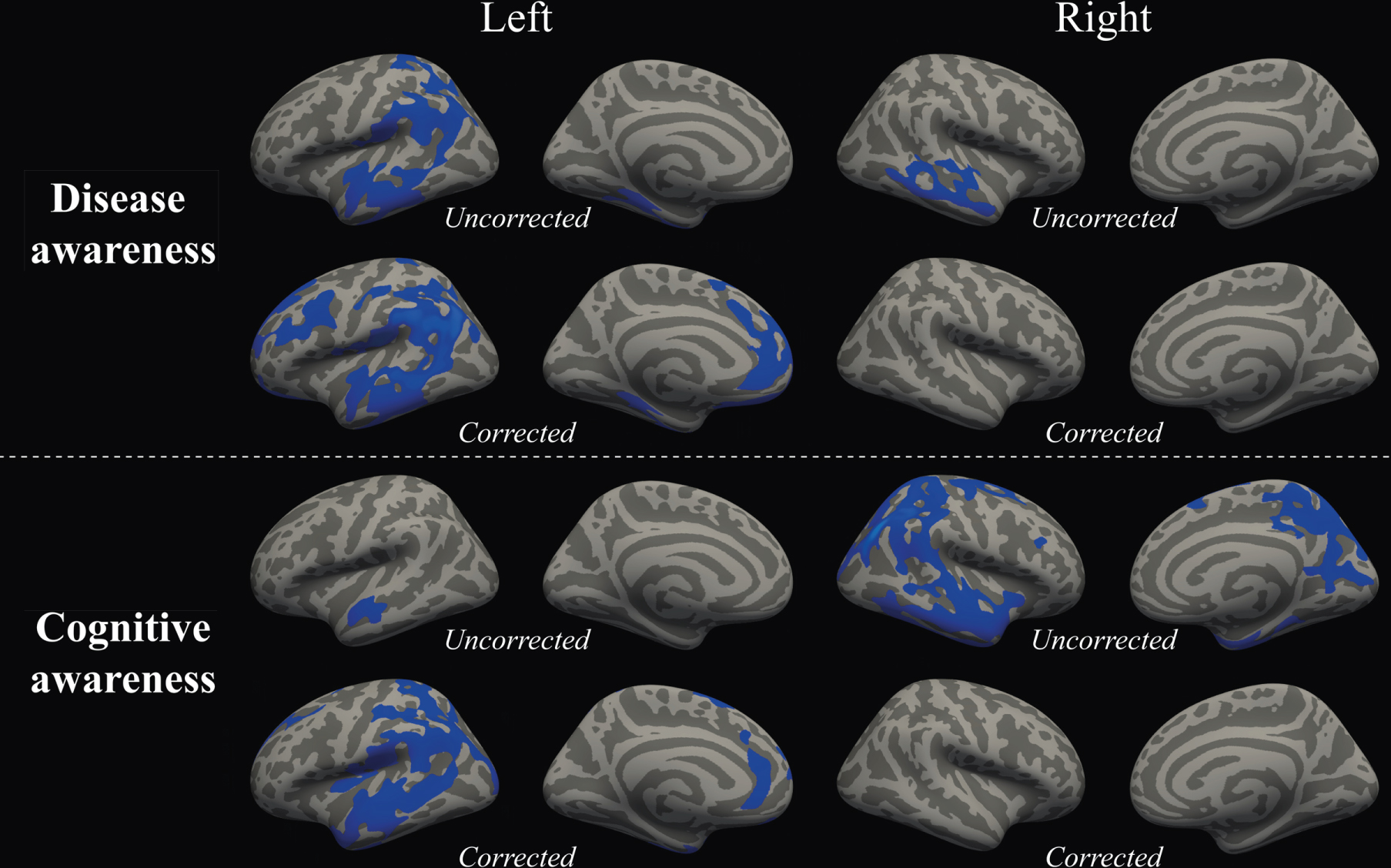
Schematic overview of the cerebral areas showing a statistically significant correlation between cortical thinning (blue regions) lower awareness of disease (top row) and cognitive awareness (bottom row) at pFWE < 0.05. Results can be seen for the analyses without confounding factors (uncorrected) and with age, sex, and MMSE scores (corrected).
Sub-domain analysis
Testing the 4 sub-domains, a correlation uncorrected for confounding factors was found between lower cognitive awareness and cortical thinning in the left superior and middle temporal gyri (pFWE < 0.05, min-max: r = –0.20 –r = –0.78), and in the right pre-, post- and paracentral, posterior cingulate, precuneus, supramarginal, superior and inferior parietal, cuneus, lingual, lateral occipital and pericalcarine, entorhinal, parahippocampal, fusiform, and superior, middle and inferior temporal, insula, and superior and middle frontal regions (pFWE < 0.05, min-max: r = –0.29 –r = –0.74). Correcting for age, sex, and MMSE score, a correlation between lower cognitive awareness and cortical thinning in the left hemisphere was found in the entorhinal, fusiform, superior, middle, and inferior temporal, in the supramarginal, inferior and superior parietal, in the lateral occipital, in the anterior cingulate, in the postcentral, and superior, middle, and orbitofrontal, and the insula regions (pFWE < 0.05, min-max: r = –0.28 –r = –0.78). All correlations in the right hemisphere lost statistical significance (pFWE > 0.05). Summarizing, when correcting for common factors related to brain alterations, corrections in the left hemisphere gained strength, whereas those in the right hemisphere lost significance.
White matter integrity
Awareness of disease
There were no correlations between disease awareness (i.e., ASPIDD-s total score) and any of the white matter integrity parameters (all pFWE > 0.05).
Sub-domain analysis
Testing the sub-domains, lower cognitive awareness was related to higher indices of mean diffusivity (i.e., poorer white matter integrity) in the right anterior thalamic radiation, in the right forceps minor and anterior cingulum bundles, and the right inferior fronto-occipital and superior longitudinal tracts (all pFWE < 0.05, min-max: r = 0.39 –r = 0.79, Fig. 2). This correlation lost statistical significance after correction for age, sex, and MMSE. Lower awareness of functional capacity was related to lower fractional anisotropy (i.e., poorer white matter integrity) in the bilateral anterior cingulum bundle and the forceps minor (all pFWE < 0.05, min-max: r = –0.44–r = –0.65, Fig. 2). This correlation remained after correction for age, sex, and MMSE score (Fig. 2). To conclude, the correlations with functional capacity awareness survived correction for age, sex and MMSE score, whereas associations with cognitive awareness did not. This indicates that functional capacity awareness correlations depend to a lesser extent on age, sex, and MMSE score than cognitive awareness correlations do.
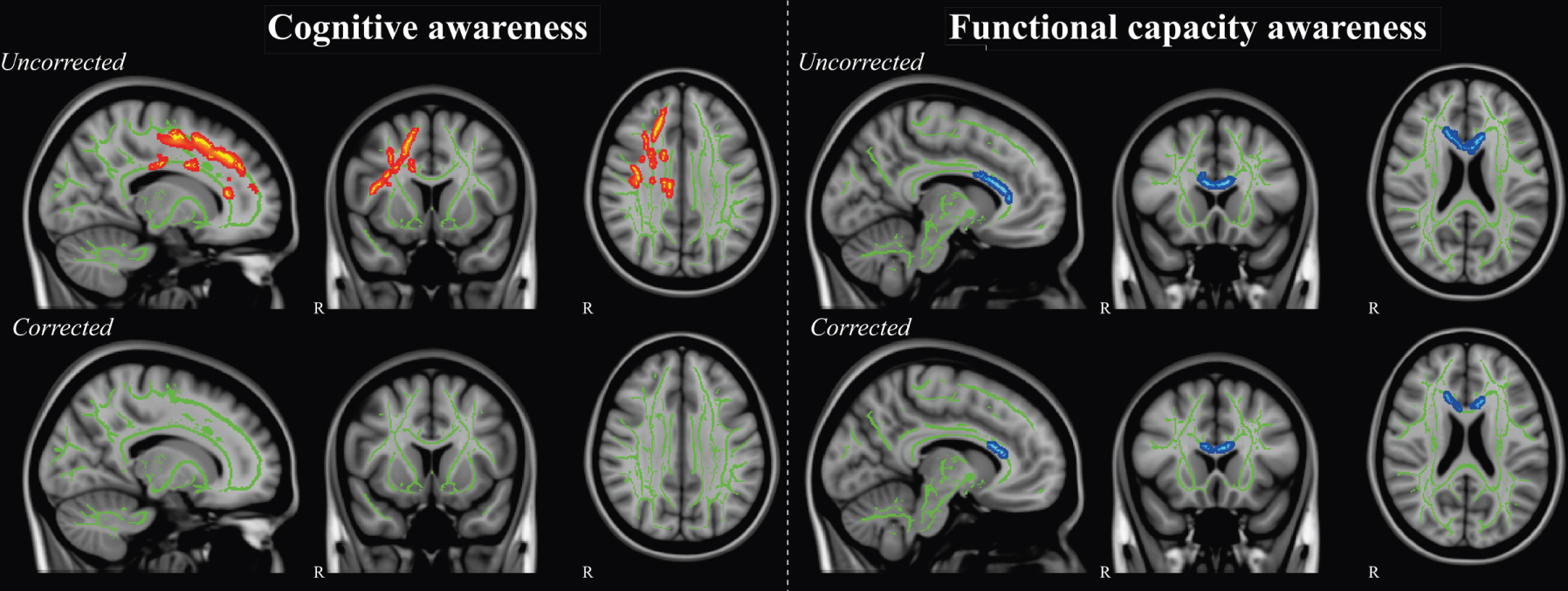
Schematic overview of the cortical white matter tracts where higher mean diffusivity (red) was related to lower awareness of cognitive deficits scores, and where lower fractional anisotropy (blue) was associated with lower functional capacity awareness scores at pFWE < 0.05. Data are presented in radiological orientation and superimposed on the TBSS-generated white matter skeleton (green) and the MNI152 1mm standard space brain. Shown are the results for the analyses without confounding factors (uncorrected) and with age, sex, and MMSE score (corrected).
Correlation with caregivers’ scores
As described in the Methods section, the ASPIDD-s scores used here are calculated as the difference between the score given by the participants and by their respective informant. Thus, the above-described correlations could, in part, be driven by the variance of the magnitude of the deficits reported by the informant. To test this hypothesis, the scores given by the informants was correlated to thickness and white matter integrity measures of the participants. These analyses did not show any statistically significant associations, therewith suggesting that the magnitude of the deficits reported specifically by the informant did not drive our results.
DISCUSSION
Awareness of disease was correlated with thinning in extensive regions of the brain, in line with the notion that there is no single awareness center in the brain [57]. Nevertheless, there was particular involvement of frontal, temporal, and parietal regions, consistent with previous studies (for reviews, [58, 59]). Findings related to white matter integrity were restricted to a few domains of awareness, with damage to long-distance fibers connecting the cortical regions indicated above.
Broadly, the relationship between cortical thinning and awareness includes regions related to language processing and monitoring behavior (lateral frontal), insight and awareness (mesial frontal and parietal), and memory (temporal). This may reflect the varied cognitive functions recruited in the generation of self-awareness, including monitoring of responses, evaluation of self-information, and autobiographical recollection, respectively. Left-sided regions correlating with awareness follow, albeit a little more extensive spatially, the patterns of the default mode network (DMN), which is compromised early in the course of AD [60]. These findings may be indicative of impaired self-related processing and self-generated thought in this condition [61]. Unawareness in AD has been linked to DMN impairment [58] and it has been shown that anosognosia predicts hypometabolism in the DMN in AD [18].
Results are in line with theoretical models of unawareness, such as the Cognitive Awareness Model (CAM), which suggests a role for both frontal and temporal regions in the etiology of executive and mnemonic forms of unawareness, respectively [2]. In executive anosognosia, damage to mechanisms that compare current performance with records of ability prevents proper monitoring of ability. According to the CAM, comparator mechanisms operate both locally, leading to domain-specific unawareness, such as in anosognosia for hemiplegia, and centrally, with a lack of awareness across different abilities. The pattern of results of the current study, with thinning being associated with unawareness of different objects, supports the latter explanation. Additionally, according to the CAM, mnemonic anosognosia occurs when temporal lobe structures are affected, leading both to lack of updating of personal ability and a graded loss of remote memory, what has been termed, metaphorically, a petrified self.
Some of the specific regions found to be associated with unawareness in this study have been reported previously, such as middle temporal regions [17], linked to memory function, frontal medial regions (e.g., [64]), in particular the anterior cingulate, which has been linked to self-appraisal and error monitoring [65, 66], and the insular cortex [19], a region that may be critical for self-awareness in general. There was considerable overlap between these correlates and those found for awareness of cognitive ability, which may suggest either that total scores were driven by scores in the cognitive domain (which provided the largest contribution among domains to the total scores), or that awareness of disease and cognitive ability rely on similar brain networks.
The associations were mostly lateralized to the left hemisphere. Although some studies found an association between unawareness and left hemisphere impairment (e.g., [67]), the right hemisphere has been more consistently linked to unawareness, both in dementia (e.g., [17, 19]) and in other conditions (e.g., anosognosia for hemiplegia; [68]). Considering that the current study is one of the first to investigate neural correlates of awareness in a sample with heterogeneous levels of educational achievement, the use of language-based cognitive resources could be a potential explanation; this is unlikely, however, given that the left hemisphere associations survived adjustments for educational level, unlike right hemisphere correlates. Also, regarding the sample characteristics, the laterality of the participants might be another factor to consider. However, this possibility must be considered carefully, as this information is not disclosed in most of the previous studies, also not being available for the present sample. Another possibility is that this refers to the measure of awareness employed, based on verbal reporting of difficulties, with stronger recruitment of language in response to the awareness questionnaire, as opposed to tasks [19]. Nevertheless, right-hemisphere recruitment has been seen across different measures of awareness (e.g., [17]; with right medial regions being linked to unawareness measured by questionnaire discrepancies, clinical assessment, or task performance), so it is unlikely this is a complete explanation.
There were no white matter correlate for total ASPIDD-s scores, in keeping with the notion that awareness is a more cortical than subcortical function, relying more heavily on grey than white matter [69]. Nevertheless, correlations with long-distance connecting fibers were observed for awareness of cognitive and ADL ability. Notably, these fibers connect frontal regions with parietal and temporal parts, mirroring the cortical findings reported in this study. Poorer integrity of the cingulum bundle was associated with unawareness for both domains. This white matter tract connects the frontal, parietal, and medial temporal lobe sites, being implicated in executive control and episodic memory [70]. The findings of the current study are in agreement with previous research that has indicated that disconnection between frontal and temporal regions may be linked to unawareness in dementia [31]. The involvement of the forceps minor suggests the importance of connectivity within the frontal lobes, as shown previously [32], reinforcing the notion that integration of information is an essential feature to develop awareness [62].
The current study has a few important limitations. In particular, although the assessment of awareness tapped into different objects, the questionnaire relied on patient-informant discrepancy. The questionnaire approach might not accurately reflect the patients’ awareness, as the responses might be influenced by other factors, such as social-desirability or defensive denial [71]. It has also been suggested that informant-based measurements of awareness may be prone to the influence of caregiver burden and depression [72], and these variables were not measured in the current study. Nevertheless, for certain objects of awareness (e.g., mood alterations, functional capacity), that cannot be readily measured by objective testing, questionnaires may be the best alternative. Future research should not only investigate different objects of awareness but rely on complementary methods (e.g., comparison of patient reports with both informant-reports and objective testing) to fully explore the multidimensionality of awareness. Additionally, considering that the focus of the present study was on the neural substrates of anosognosia in relation to the multidimensional nature of awareness, limited cognitive measures were used. Therefore, future studies should include a more comprehensive neuropsychological assessment. Finally, as shown by previous studies [73, 74], the reduced sample may have impacted on findings. Nevertheless, this has likely led to less pernicious Type II error, and the sample had a very typical clinical and cognitive profile, not limiting the ability to generalize findings. Also, further studies are necessary in order to replicate these findings.
In conclusion, results reinforce the notion that awareness in AD is generated by wide cortical networks, with particular involvement of regions dedicated to memory processing, self-reference, and self-awareness in general. This was accompanied by the involvement of long-distance connecting fibers between these regions in awareness. Stronger involvement of the left hemisphere may be linked to stronger language demands in questionnaire-based measures or reflect heterogeneity in educational level in the sample, suggesting the need for further studies from developing regions. The profile of gray and white matter correlates indicated here, together with previous findings, may allow predictive diagnosis in relation to lack of awareness, improving clinical management of the condition.