
Abstract
Background:
The apolipoprotein E (APOE) ɛ4 allele is associated with dose-response effects on cognitive dysfunction and dementia risk in older adults. However, its effects on cognition in middle-aged adults remains unclear.
Objective:
We examined effects of ɛ4 heterozygosity and homozygosity on objective and subjective cognition in middle-aged adults enrolled in the Healthy Brain Project (HBP) and in older adults from the Australian Imaging, Biomarkers and Lifestyle (AIBL) study.
Methods:
HBP participants (1,000 non-carriers; 450 ɛ4 heterozygotes; 50 ɛ4 homozygotes) completed unsupervised assessments of the Cogstate Brief Battery (CBB), ratings of subjective cognitive function and provided a saliva sample. AIBL cognitively normal participants (650 non-carriers; 204 ɛ4 heterozygotes; 31 ɛ4 homozygotes) completed in-person assessments of the CBB, ratings of subjective cognitive function and provided a blood sample.
Results:
Greater memory impairment was observed in middle-aged ɛ4 homozygotes compared with ɛ4 heterozygotes and non-carriers. When data from middle-aged (HBP) and older (AIBL) adults were pooled, the effect of ɛ4 homozygosity and memory impairment increased with age. In both middle-aged and older adults, ɛ4 heterozygotes did not differ from non-carriers on any measure of objective or subjective cognition.
Conclusion:
Memory impairment in ɛ4 homozygotes is evident in adults aged 50-60 years, and this can be detected through unsupervised cognitive assessments. The effect of ɛ4 homozygosity increases with older age. APOE ɛ4 homozygosity has a negative impact on memory as early as midlife, but due to the subtle magnitude of effect, our findings support the necessity of online platforms in large cohorts to assess these complex relationships.
INTRODUCTION
In cognitively normal (CN) adults, carrying even one copy of the apolipoprotein E (APOE) ɛ4 allele is associated with increased risk of dementia and reduced age of dementia onset (by∼8 years) [1, 2]. In CN adults with abnormally high amyloid-β levels (Aβ+), ɛ4 is associated with faster memory loss [3, 4]. The importance of the ɛ4 allele as a risk factor for AD is also evident in CN older adults for whom Aβ levels remain below established thresholds for abnormality (Aβ-). In these groups, ɛ4 is associated with faster Aβ accumulation [5–7], which can be accompanied by subtle dysfunction in episodic memory [8]. Studies investigating the relationship between Aβ and age in midlife indicate that, in the absence of an autosomal dominant AD mutation, Aβ rarely meets established thresholds for abnormality [7, 9]. Therefore, studying the effects of ɛ4 on cognition in middle-aged adults, when Aβ levels are unlikely to have reached current thresholds of abnormality, could improve understanding of the preclinical stage of AD. However, as meta-analyses of the effects of ɛ4 on cognition in midlife indicate effect sizes are small (e.g., d = 0.1), large samples are required to provide the necessary statistical power [10, 11].
Online platforms provide a practical approach for collection of large amounts of data. Accordingly, we have developed methods to optimize digital assessments to validly and reliably measure cognitive domains relevant to early AD in unsupervised contexts [12–14]. We developed the Healthy Brain Project (HBP; healthybrainproject.org.au) as an online platform where participants complete unsupervised cognitive assessments and provide a saliva sample for genetic analysis. The advantage of this sampling method is its large-scale and ethnically and residentially diverse recruitment pool [14, 15]. To provide a methodological check and theoretical context for any relationships observed from unsupervised assessment of cognition in middle-aged adults, the same investigations can be repeated in a comprehensively-phenotyped CN cohort that has undertaken conventional, supervised assessments, such as in the Australian Imaging, Biomarkers and Lifestyle (AIBL) study.
The aim of this study was to examine the effect of APOE genotype on unsupervised assessments of objective and subjective measures of cognition in a very large cohort of middle-aged adults. We hypothesized that APOE ɛ4 would be associated with cognitive dysfunction as indicated by a visual memory composite in middle-aged adults. We also explored quantitative and qualitative similarities between any gene-cognition relationships detected in an unsupervised context against data collected in a separate cohort under a supervised context. Finally, given the breadth of age-range available across HBP and AIBL cohorts, we pooled data to explore the effect of APOE genotype on visual memory from middle to older age.
METHODS
Participants
The unsupervised sample consisted of CN adults (n = 1,500) enrolled in the HBP who had provided saliva samples and also completed cognitive assessments (Fig. 1) [15]. Cognitive normality was assumed as participants self-reported that they did not have a diagnosis of mild cognitive impairment (MCI), AD, or any other dementia. Details of the recruitment process have been outlined previously; notably, we sought to target recruitment to individuals with a family history of dementia [15]. Participants are eligible for enrolment if they are currently residing in Australia; are fluent in English; do not have a diagnosis of AD, Parkinson’s disease, dementia with Lewy bodies, or other known diagnosis of dementia; do not have a history of major traumatic brain injury or other neurological disease or insult; do not have a diagnosis of a major psychiatric condition (e.g., schizophrenia, uncontrolled major depressive disorder, or other psychiatric disorder); and do not use any of the Australian government’s Therapeutic Goods Administration approved medication for the treatment of AD (e.g., donepezil, rivastigmine, or other approved medication).
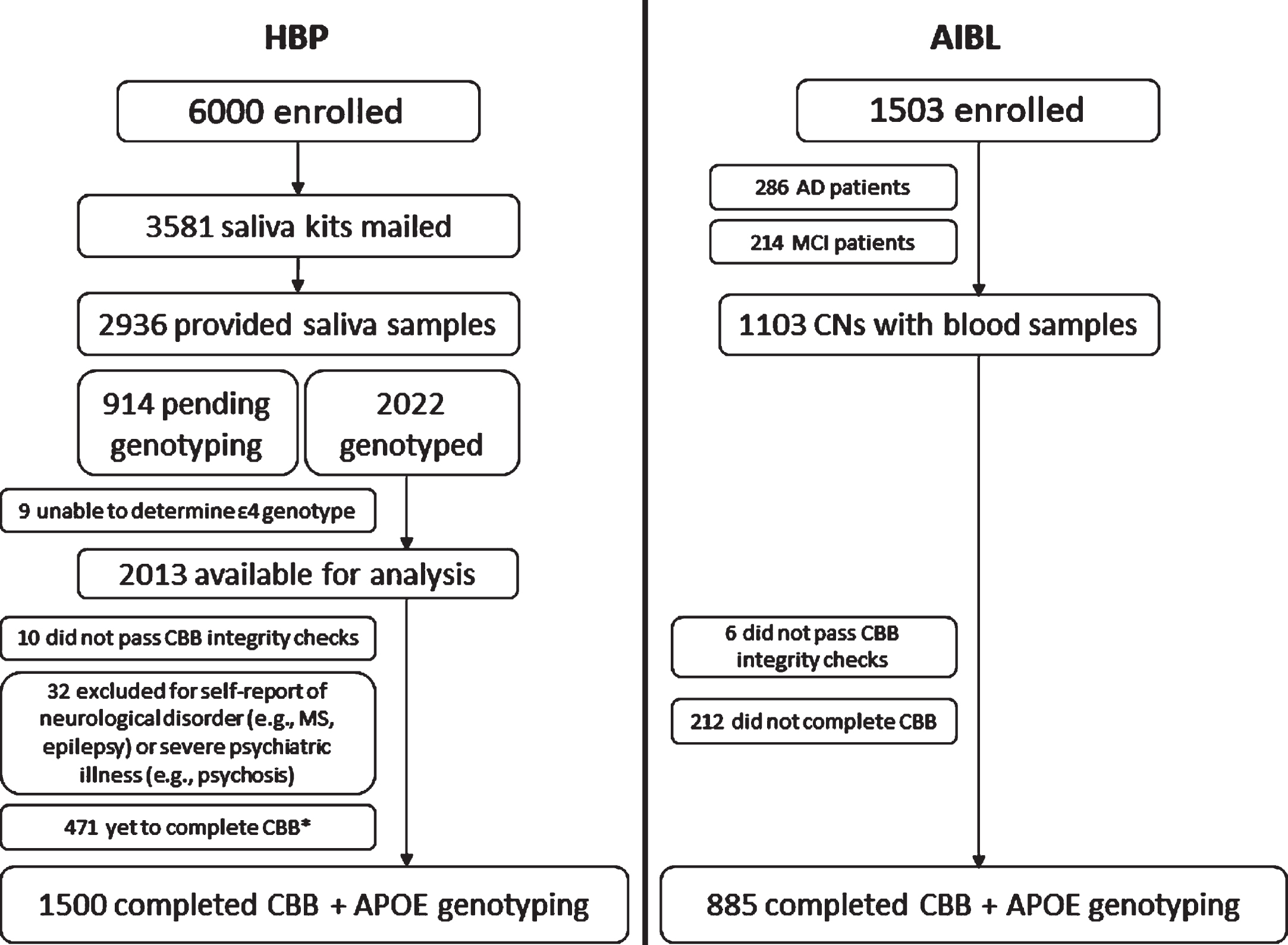
Number of participants enrolled in HBP and AIBL, and availability of genetic and cognitive data in each sample (*note: the HBP platform was designed such that participants can complete tests and questionnaires in their own time, and as such, while these participants may not have completed the CBB at the time of this report, they may complete it in the future).
CN adults (n = 885) enrolled in the AIBL study underwent APOE genotyping and completed a series of computerized cognitive assessments. The AIBL recruitment process has been detailed previously [16]. Participants were excluded from AIBL if they had a previous confirmed diagnosis of any of the following: schizophrenia; Parkinson’s disease; untreated sleep apnea; depression (Geriatric Depression Score [GDS]≥6); cancer (except basal cell skin carcinoma) in the last two years; symptomatic stroke; or uncontrolled diabetes. Participants were excluded if their current alcohol use exceeded four standard drinks per day for men or two per day for women. All available neuropsychological, psychiatric, and medical information were reviewed by a clinical panel to determine the cognitive health of each participant. The clinical panel was blind to APOE genotype.
Standard protocol approvals, registrations, and patient consents
The HBP was approved by the human research ethics committee (HREC) of Melbourne Health [15]. Participants viewed the consent form through a web browser and downloaded a portable document format (PDF) of the form. Participants indicated their willingness to join the study by clicking on a box and entering their full name (in lieu of a signature). The AIBL study was approved by the HRECs of Austin Health, St. Vincent’s Health, Hollywood Private Hospital and Edith Cowan University [16]. Informed consent was provided in writing prior to participation.
APOE genotyping
Genotek Oragene (OG-500) 2 ml saliva kits (including instructions on saliva collection) were mailed to HBP participants who had completed at least 80% of assessments [15]. Saliva samples were forwarded, in batches of 1,000 samples, to GenoFIND Services laboratory (Salt Lake City, UT, USA), where they were processed to extract targeted SNPs including APOE (rs429358, rs7412). A blood sample from each AIBL participant was forwarded for DNA extraction using either QIAamp DNA blood Midi or Maxi kits (Qiagen), applying manufacturer’s protocol. APOE genotype was determined through TaqMan genotyping assays (Life Technologies) for rs7412 (Assay ID: C____904973_10) and rs429358 (Assay ID: C___3084793_20) on a QuantStudio 12K-Flex real-time PCR system (Applied Biosystems) using the TaqMan GTXpress Master Mix (Life Technologies) methodology per manufacturer’s instructions.
Cognitive assessment
HBP participants completed the Cogstate Brief Battery (CBB) using an unsupervised, online platform [14], and AIBL participants completed the same battery but were supervised in-person by trained raters [17]. The CBB consists of four tasks: Detection (DET), Identification (IDN), One Card Learning (OCL), and One-Back (OBK) [17, 18]. DET is a simple reaction time test shown to measure psychomotor function. IDN is a choice reaction time test shown to measure visual attention. The primary outcome for DET and IDN was reaction time in milliseconds (speed), normalized using a log10 transformation. OCL is a continuous visual recognition learning task that assesses visual learning within a pattern separation model. OBK is a task of working memory and attention. The primary outcome for OCL and OBK was the proportion of correct answers (accuracy), normalized using an arcsine square-root transformation. The Attention Composite was computed by standardizing and averaging the DET and IDN tasks. As DET and IDN are speeded measures, they were reverse scored such that negative values reflected poorer performance. The Visual Memory Composite was computed by standardizing and averaging the OCL and OBK tasks. Tests were standardized using the baseline mean and standard deviation of the entire CN sample in each cohort.
Subjective ratings of cognition
Subjective ratings of cognitive function in the HBP was assessed using the Cognitive Function Instrument (CFI) [19]. However, as the CFI was designed for use in older adults, some items were modified to include ecologically valid questions about subjective experiences of memory and thinking at work, and other aspects relevant to middle-aged individuals’ lives [15]. The primary outcome was total CFI score, with higher scores indicating higher levels of concern. In AIBL, the measure of subjective cognitive function was the Memory Complaints Questionnaires (MAC-Q), which was administered in-person as a paper form [20]. The primary outcome was total MAC-Q score, with higher scores indicating higher levels of concern.
Demographic and clinical assessments
HBP participants self-reported date of birth, sex, race, years of education, residential address (from which we determined whether they resided in a metropolitan or rural/regional area), height and weight (to compute body mass index), blood pressure (derived from self-report systolic and diastolic blood pressure reading and/or self-report history of hypertension), and history of hypercholesterolemia, diabetes mellitus, and current cigarette smoking. HBP participants also completed the Hospital Anxiety and Depression Scale (HADS) via our online platform [15]. For AIBL participants, all assessments were conducted in person [16].
Data analysis
All analyses were conducted in the statistical program R (v 3.5). Figure 1 illustrates the number of HBP and AIBL participants who provided a saliva or blood sample and who also completed computerized cognitive assessments. Only baseline assessments for both cohorts were included.
HBP and AIBL participants were classified into three APOE groups: ɛ4 non-carriers (ɛ2/ɛ2, ɛ2/ɛ3, ɛ3/ɛ3), ɛ4 heterozygotes (ɛ2/ɛ4, ɛ3/ɛ4), and ɛ4 homozygotes (ɛ4/ɛ4). We then conducted a series of analyses of co-variance (ANCOVA) models to examine the effect of APOE group on each outcome measure. Analyses were conducted separately in each cohort. While age, sex, and education did not differ significantly between APOE groups in either the HBP or AIBL cohorts, we included these variables as covariates in all analyses given their potential effects on cognition. Means and standard deviations of each outcome measure were computed for each APOE group, and a series of planned comparisons were conducted. These planned comparisons were between (a) ɛ4 non-carriers and ɛ4 heterozygotes, and (b) ɛ4 non-carriers and ɛ4 homozygotes.
To explore the effect of APOE genotype and older age on cognitive function, we pooled data across both the HBP and AIBL cohorts. Four separate ANCOVA models were conducted to compare ɛ4 non-carriers and ɛ4 homozygotes at each of the following age strata: (a) 40–50, (b) 51–60, (c) 61–70, and (d) 71–80 years of age.
The statistical significance for all comparisons was set at p < 0.05. Analyses were not adjusted for multiple comparisons because this is a novel area of research that reports one of the first outcomes of remote and unsupervised assessment of cognitive function, because the sample sizes studied were large and because hypotheses were tested with only three dependent variables. However, we did compute effect sizes (Cohen’s d) to quantify the magnitude of difference between groups as it provides context for the meaningfulness of findings [21].
RESULTS
Demographic and clinical characteristics
Of those who were provided a saliva sampling kit in the HBP cohort (i.e., met our pre-specified criteria of completing 80% of HBP assessments),∼81% returned a sample of their saliva (Fig. 1). Of the 2013 participants for whom APOE genotyping has been completed to date, ∼30% (n = 602) were ɛ4 heterozygotes, and ∼3% (n = 63) were ɛ4 homozygotes. APOE ɛ4 carriage was associated significantly with a family history of dementia (Table 1). The proportion of ɛ4 carriers was significantly higher among participants with (∼38%) as compared to without (∼24%) a first or second-degree family history of dementia, χ2 = 42.05, p < 0.001.
Relationship between APOE genotype and family history of dementia in the HBP cohort
Of the 2013 HBP participants for whom APOE genotype was available, 1,500 also completed cognitive assessments on the CBB (Fig. 1). The demographic characteristics of this group are summarized in Table 2. In the HBP cohort, ɛ4 homozygotes had significantly lower years of education than non-carriers. A significantly higher proportion of ɛ4 homozygotes in the AIBL cohort also reported a first-degree family history of dementia (Table 2). No other demographic or clinical characteristics differed between APOE groups in the HBP and AIBL cohorts, although, by design, the HBP cohort was, on average, ∼15 years younger than the AIBL cohort. Additionally, in a subset of participants who provided details about their medications at the time of analysis (n = 1,300), 25% of ɛ4 homozygotes, 24.7% of ɛ4 heterozygotes, and 22% of ɛ4 non-carriers reported taking statins or other lipid-modifying medications, although there were no significant differences between groups, χ2 = 0.534, p = 0.766.
Demographic characteristics of the HBP and AIBL cohorts
BP, blood pressure; BMI, body mass index; CDR, Clinical Dementia Rating Scale; HADS, Hospital Anxiety and Depression Scale.
Effect of APOE genotype on cognitive function
Performance of each APOE group on the Attention and Visual Memory composites is summarized in Table 3. In the HBP cohort, ɛ4 non-carriers performed significantly better than ɛ4 homozygotes on the Visual Memory Composite (Table 3), with a moderate magnitude of difference (Fig. 2). APOE ɛ4 non-carriers and ɛ4 heterozygotes performed equivalently on the Visual Memory Composite, with the magnitude of this difference very small (d < 0.10) (Fig. 2). No differences were observed between APOE groups on the Attention Composite.
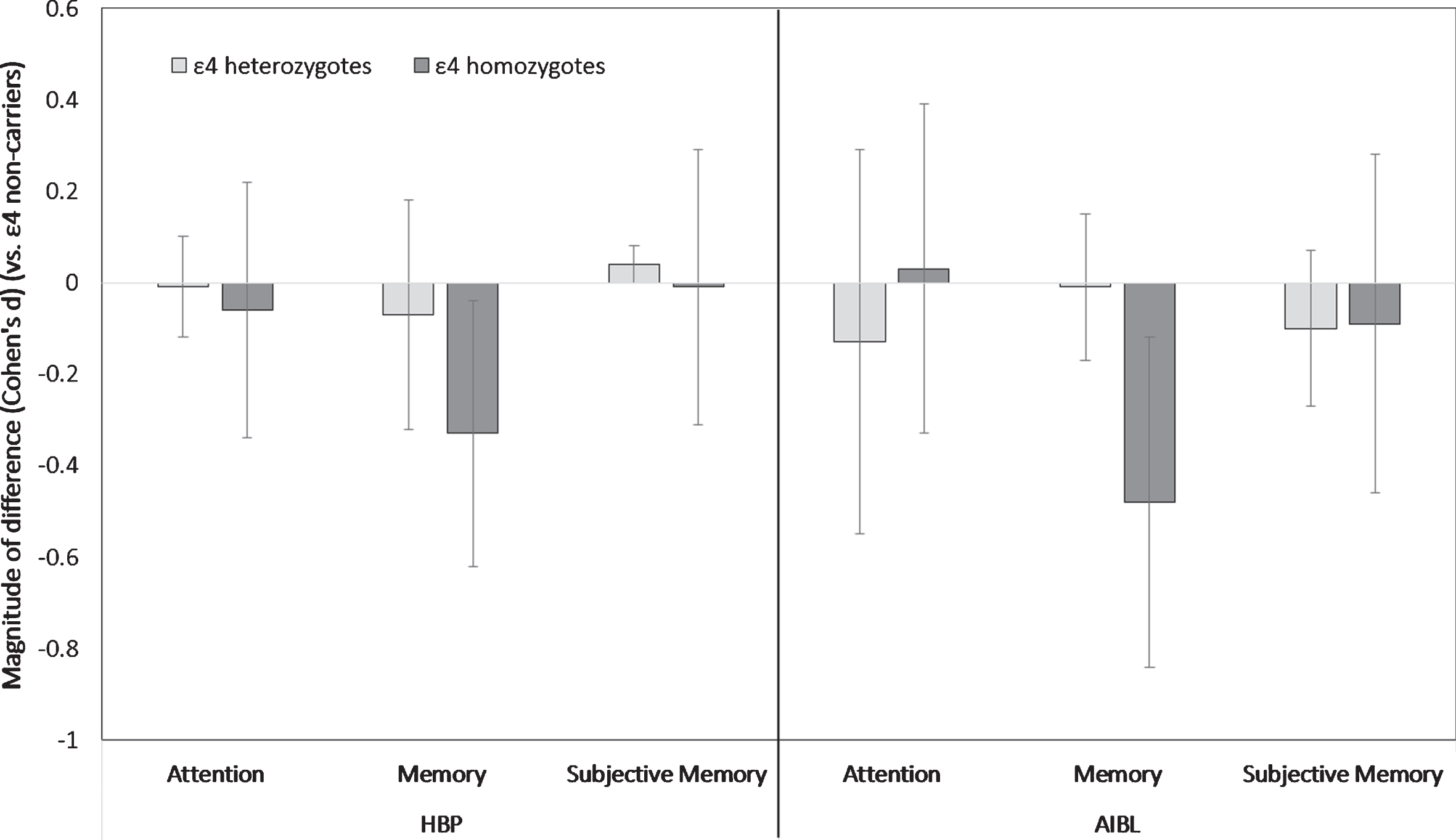
Magnitude of difference relative to ɛ4 non-carriers (represented by the “0” line) of ɛ4 heterozygotes (light grey bars), and ɛ4 homozygotes (dark grey bars) on the Attention composite, the Visual Memory composite, and a measure of subjective memory concern (CFI total score in HBP; MAC-Q total score in AIBL). Negative values indicate poorer performance. Error bars represent 95% confidence intervals.
Effects of APOE group on each objective and subjective memory outcome measure
Subjective memory concern was measured used the CFI total score in the HBP cohort and the MAC-Q total score in the AIBL cohort.
In the AIBL cohort, ɛ4 non-carriers performed significantly better than ɛ4 homozygotes on the Visual Memory Composite (Table 3), with the magnitude of difference moderate (Fig. 2). APOE ɛ4 non-carriers and ɛ4 heterozygotes performed equivalently on the Visual Memory Composite (Fig. 2). No differences were observed between any APOE groups on the Attention Composite.
Effect of APOE genotype on subjective ratings of cognition
No statistically significant differences were observed between any APOE groups on subjective ratings of cognitive function in the HBP and AIBL cohorts. The magnitude of difference between groups for measures of subjective cognitive function were very small (d < 0.10) (Fig. 2).
Exploration of the effect of APOE genotype and increasing age on memory
We sought to explore the influence of age, from mid- to later-life, on the difference in performance between ɛ4 non-carriers and ɛ4 homozygotes on memory. For parsimony, this exploratory analysis was not conducted for attention or subjective ratings of cognition because our main analysis indicated no effects of ɛ4 homozygotes on these outcomes. Similarly, we did not conduct this exploratory analysis on ɛ4 heterozygotes.
Given the qualitative similarity in the effects of APOE on cognition and subjective ratings of cognition in both HBP and AIBL cohorts, individual-participant level data from both cohorts were pooled for this analysis. We observed a statistically significant difference between ɛ4 non-carriers and ɛ4 homozygotes on the Visual Memory Composite at ages 51–60 years, 61–70 years, and 71–80 years, with the magnitude of difference moderate (Table 4, Fig. 3). No significant differences were observed between ɛ4 non-carriers and ɛ4 homozygotes on the Visual Memory Composite who were aged 40–50 years, though this difference was moderate in magnitude (Fig. 3).
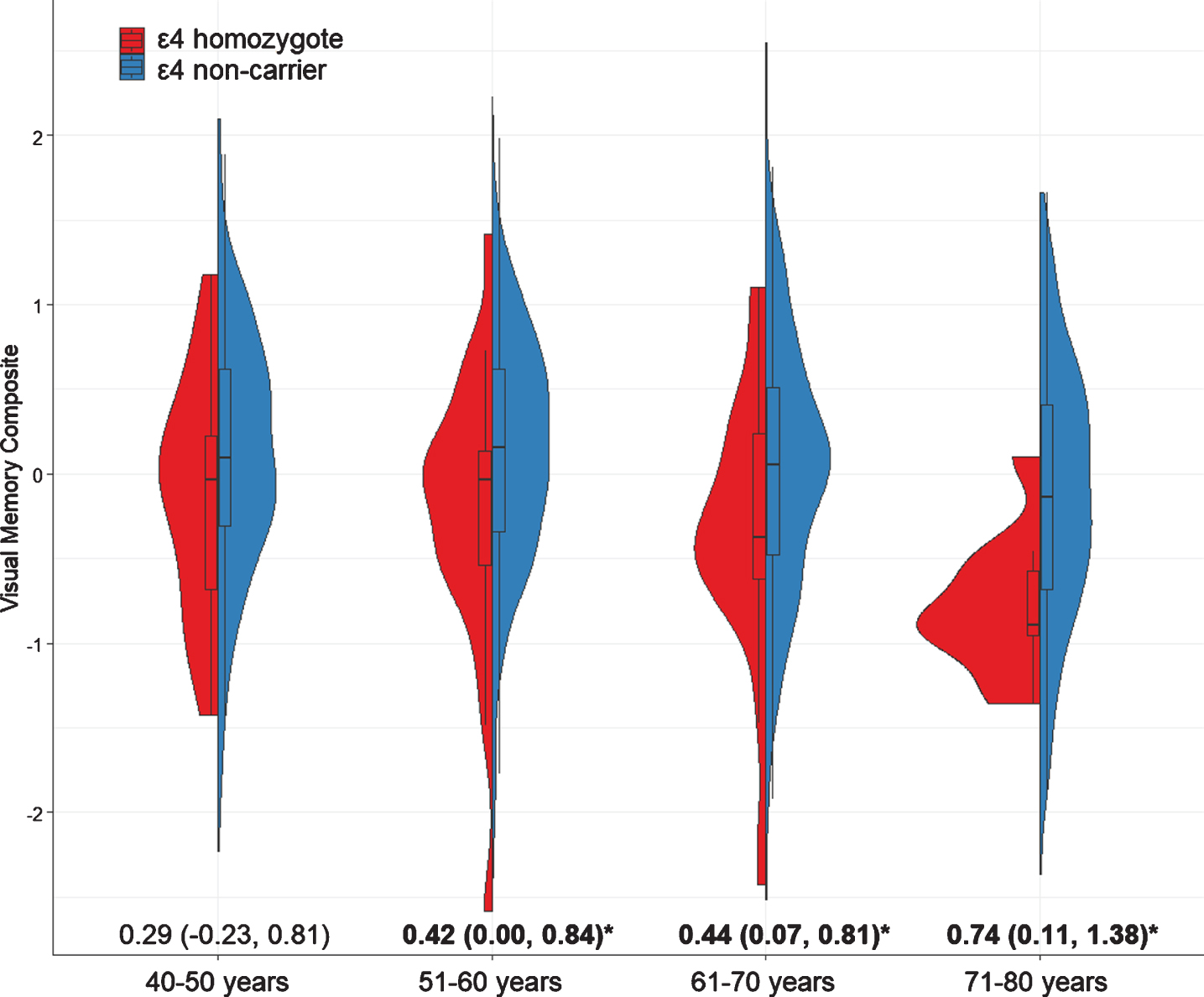
Performance of ɛ4 non-carriers (light grey bars) and ɛ4 homozygotes (dark grey bars) on the Visual Memory composites at each age-group. Values indicate magnitude of difference between groups (i.e., Cohen’s d and 95% CIs). Error bars represent 95% confidence intervals.
Difference in performance on the Visual Memory Composite between ɛ4 non-carriers and ɛ4 homozygotes at each decade
Effect of cohort not estimated in the 40–50 and 71–80 age groups because no AIBL participants were aged 40-50 years, and no HBP participants were aged 71-80 years.
DISCUSSION
The hypothesis that carriage of APOE ɛ4 would be associated with poorer visual memory in middle-aged CN adults was supported partially. Compared to middle-aged ɛ4 non-carriers, middle-aged ɛ4 homozygotes showed worse visual memory, but equivalent attention and subjective ratings of cognitive function. No visual memory impairment was observed in middle-aged ɛ4 heterozygotes. This pattern of visual memory impairment with normal attention and normal subjective ratings of cognition, specific to ɛ4 homozygotes, was also evident in the older CN adults from the AIBL cohort. The effect of ɛ4 on elevated Aβ, cognitive decline and clinical disease progression has been well demonstrated in the older AIBL group [3, 6]. Pooling of data from the middle- and older-aged cohorts made apparent that the association between ɛ4 homozygosity and visual memory impairment was evident even in adults aged 50–60 years and that the magnitude of this effect increased with age (Fig. 3). Given the low prevalence of elevated Aβ in middle-aged adults [7, 9], the observation of visual memory impairment in middle-aged ɛ4 homozygotes, and its qualitative similarity to that in older adults, suggests that this midlife visual memory impairment is a manifestation of AD processes which have begun in ɛ4 homozygotes as early as in the fifth decade of life.
In middle-aged and older adults, we observed that ɛ4 heterozygotes and ɛ4 non-carriers showed equivalent visual memory, attention, and subjective cognitive function. This absence of any effect on cognition is consistent with a recent meta-analysis and review which concluded there was no strong evidence for cognitive impairments associated with ɛ4 in middle-aged adults [10, 11]. In older adults, we and others have shown that while ɛ4 heterozygotes do show higher levels of Aβ and tau, and smaller brain volumes, these manifestations are less severe than in ɛ4 homozygotes [22–25]. Despite this strong link between ɛ4 carriage and AD pathology, cross-sectional comparisons of ɛ4 heterozygotes and ɛ4 non-carriers in studies of preclinical AD also fail to identify any visual memory impairments [22], with the effects becoming evident only through prospective study [3, 4]. Similarly, in middle-aged adults, cognitive dysfunction in ɛ4 carriers has only been evident from analyses of prospective data and were only discernible in ɛ4 homozygotes [26, 27]. Thus, the effects of APOE ɛ4 on cognitive function in very early AD are small and therefore seen more reliably in ɛ4 homozygotes. This is consistent with AD pathophysiological models which show that the accumulation of Aβ and tau can remain clinically silent for many decades [28, 29], and with estimates that indicate that ɛ4 homozygotes are diagnosed with AD dementia ∼8 years earlier than ɛ4 heterozygotes (68 years versus 76 years).
In older adults, Aβ- ɛ4 carriers showed subtle but faster rates of Aβ accumulation when compared to Aβ- ɛ4 non-carriers [5, 6], and this rate of Aβ accumulation was related to faster memory decline [8]. Small studies using CSF biomarker measures have observed that middle-aged ɛ4 carriers show lower levels of CSF Aβ42 (indicative of higher cerebral Aβ load) when compared to ɛ4 non-carriers [7], and that structural and functional imaging brain changes can be detected even in young to middle-aged ɛ4 carriers [30]. These data, and the similarity of cognitive impairment between middle-aged and older ɛ4 homozygotes, suggests that the visual memory impairment observed in the HBP middle-aged ɛ4 homozygotes reflects the early consequences of accumulating Aβ and/or tau in this group. Biomarker measures are not yet available in the HBP cohort due to the large sample size and highly distributed location of participants. While the role of APOE ɛ4 in increasing AD risk is thought to be most strongly through its effects on Aβ and tau accumulation, ɛ4 also has important associations with cerebrovascular disease, neuroinflammatory processes, and dysregulation of the blood-brain barrier [31, 32]. Inclusion criteria for both the HBP and AIBL cohorts render the prevalence of cardiovascular disease very low and equivalent across APOE genotype groups, reducing the likelihood that the effect of ɛ4 carriage on cognition is cerebrovascular in nature (Table 2). However, detailed biomarker studies will be required to enable better understanding of the biological correlates of memory impairment in middle-aged ɛ4 homozygotes. One benefit of the HBP is we now have a large group of committed participants who are likely to volunteer for more detailed investigations [15].
In the HBP, we have utilized a web-based platform to recruit a large group of ɛ4 carriers, which enabled a more detailed analysis of the effect of ɛ4 homozygosity on cognitive function in middle-aged adults. We enriched the HBP sample with ɛ4 carriers by targeting our recruitment towards individuals with a first- or second-degree family history of dementia, and as such, it is likely that there may be over-representation of individuals concerned about their future risk of cognitive decline or dementia in the HBP cohort. We and others have shown that unsupervised cognitive tests, designed carefully with interactive instructions and practice sessions can have high usability and acceptability in middle-aged and older adults and thereby provide valid indices of cognition [12, 14]. The qualitatively similar effects of APOE ɛ4 in the HBP and AIBL cohorts lend more support to the contention that web-based platforms can be used effectively for remote, unsupervised assessment and characterization of at-risk individuals. Additionally, we have recently shown that cognitive dysfunction as measured using a web-based visual paired associate learning test is four times larger than traditional tests of episodic memory in Aβ+cognitively normal older adults [33]. This learning dysfunction is similarly observed, albeit at a smaller magnitude, in Aβ- cognitively normal ɛ4 carriers [34]. The results of our current study thus present an important context within which we can now seek to further challenge the utility of novel unsupervised cognitive tests to understand cognitive dysfunction in early AD.
There are several important caveats for generalization of our results. First, memory impairment was observed in ɛ4 homozygotes aged 40–50 years, but the magnitude of this impairment was not sufficient to reach statistical significance, likely due to the small sample size (n = 15). Given the moderate magnitude of this impairment and the qualitative similarity of that observed in older ɛ4 homozygotes in the study (Fig. 2), it is likely that this impairment will become significant with larger sample sizes. This suggests that it may be possible to observe clinical manifestations of AD biological processes even earlier than concluded here. Second, this is a cross-sectional study. While we have shown previously that APOE ɛ4 increases the rate of cognitive decline in older adults [35–37], future investigations are needed to determine the gene-dose effects of APOE ɛ4 on cognitive decline in middle-aged adults. The HBP platform will also serve as a convenient method for prospective data collection. Additionally, the impairment in memory observed in middle-aged ɛ4 homozygotes observed in this study informs brain behavior models of early AD by suggesting that AD pathophysiological processes can manifest cognitively in individuals known to be at increased risk for AD despite their relatively young age. However, these impairments were very subtle (d = 0.42) and evident only from comparison of large groups of individuals. Therefore, while important experimentally, the clinical significance of these impairments will need to be established in future studies. Finally, measures of Aβ and tau were not available in the HBP cohort. It is thus likely that a proportion of middle-aged ɛ4 homozygotes enrolled in HBP have abnormal Aβ or tau levels or are on the threshold of abnormality. This would be an important group of individuals to enroll into future biomarker studies, particularly using methods that do not require invasive procedures such as PET or CSF sampling [38, 39].
These caveats notwithstanding, the results of this study are the first to demonstrate that memory impairments are evident in middle-aged ɛ4 homozygotes, even when assessed via an unsupervised web-based platform. The magnitude of this effect increases with age, and further demonstrates the added risk of ɛ4 homozygosity on cognitive function. Our results have important implications for understanding clinicopathological relationships between putative risk factors for AD (e.g., ɛ4) and cognition in middle-aged adults, and for the use of unsupervised web-based platforms for large-scale screening of at-risk individuals.
Footnotes
ACKNOWLEDGMENTS
Dementia Australia and Alzheimer’s Association (Western Australia) assisted with promotion of the AIBL study and the screening of telephone calls from volunteers. We thank all HBP and AIBL participants for their commitment and dedication to helping advance research into the early detection and causation of AD.
The Healthy Brain Project (healthybrainproject.org.au) is funded by the National Health and Medical Research Council (GNT1158384, GNT1147465, GNT1111603, GNT1105576, GNT1104273, GNT1158384, GNT1171816), the Alzheimer’s Association (AARG-17-591424, AARG-18-591358, AARG-19-643133), the Dementia Australia Research Foundation, the Bethlehem Griffiths Research Foundation, the Yulgilbar Alzheimer’s Research Program, the National Heart Foundation of Australia (102052), and the Charleston Conference for Alzheimer’s Disease. We thank our study partners (PearlArc, SRC Innovations, Cogstate Ltd and Cambridge Cognition) for their ongoing support.
Funding for the AIBL study was provided in part by the study partners [Australian Commonwealth Scientific Industrial and Research Organization (CSIRO), Edith Cowan University (ECU), Florey Institute, University of Melbourne), Dementia Australia (DA), Austin Health, CogState Ltd., Sarich Institute]. The study also received support from the National Health and Medical Research Council (NHMRC).
YY Lim is supported by an NHMRC Career Development Fellowship (GNT1162645). MP Pase is supported by a Heart Foundation Future Leader Fellowship (GNT102052). RF Buckley is supported by a National Institutes of Health K99-R00 award (K99AG061238). L Bransby is supported by a Dementia Australia Research Foundation PhD Scholarship.