
Abstract
Background:
Cerebral amyloid angiopathy with related inflammation (CAA-ri) is a rare age-associated disorder characterized by an inflammatory response to amyloid in cerebral blood vessels. CAA-ri is often treated with corticosteroids, but response to treatment is variable.
Objective:
To assess the relationship between clinical and paraclinical measures and outcomes in patients with CAA-ri treated with high doses of methylprednisolone.
Methods:
Longitudinal clinical course, and results from serum and cerebrospinal fluid (CSF) testing, electroencephalography, and neuroimaging were reviewed from 11 prospectively-accrued CAA-ri patients diagnosed, treated, and followed at Barnes Jewish Hospital (St. Louis, MO, USA). Magnetic resonance imaging (MRI) changes were quantified using a scoring system validated in cases of amyloid related imaging abnormality (ARIA-E). Clinical outcomes were assessed as change in modified Rankin Scale (ΔmRS) from baseline to final assessment (median 175 days from treatment with high doses of methylprednisolone; range, 31–513).
Results:
Worse outcomes following methylprednisolone treatment were associated with requirement for intensive care unit admission (median ΔmRS, 5 versus 1.5; p = 0.048), CSF pleocytosis (median ΔmRS 4.5 versus 1; p = 0.04), or lower CSF Aβ40 at presentation (rho = –0.83; p = 0.02), and diffusion restriction (median ΔmRS 4 versus 1.5; p = 0.03) or higher late ARIA-E scores (rho = 0.70; p = 0.02) on MRI, but not preexisting cognitive decline (median ΔmRS 2 versus 2; p = 0.66).
Conclusion:
Clinical and paraclinical measures associated with outcomes may inform clinical counseling and treatment decisions in patients with CAA-ri. Baseline cognitive status was not associated with treatment responsiveness.
Keywords
INTRODUCTION
Cerebral amyloid angiopathy (CAA) is an age-associated disorder characterized by deposition of amyloid-β (Aβ) in cerebral blood vessels with a meningocortical predilection [1]. There is substantial but incomplete overlap between CAA and Alzheimer’s disease (AD), with CAA present in 78%of elderly patients with frequent neuritic plaques, as opposed to 21%of patients without neuritic plaques [2]. Patients with CAA most often present with cerebral hemorrhage, with microinfarctions noted in severe cases [3]. Less often inflammatory responses against vascular amyloid may be observed, termed cerebral amyloid angiopathy with related inflammation (CAA-ri) [4–6]. Considerable overlap is observed between the clinical and radiological features of CAA-ri and amyloid related imaging abnormality (ARIA) observed in patients receiving experimental anti-amyloid antibody therapies [7–10]. Early symptoms of CAA-ri typically include cognitive decline, persisting over weeks to months, with accompanying focal neurologic signs localized to affected brain regions [11–13]. Patients may also manifest with seizures and psychoses, mimicking autoimmune encephalitis [14] and complicating the differential diagnosis. Identification of asymmetric white matter lesions, and microscopic or macroscopic hemorrhages or superficial siderosis on neuroimaging may support antemortem diagnoses [15]. However, brain biopsy may still be required to detect vascular amyloid and vascular or perivascular inflammation [6] and facilitate treatment in atypical patients [16].
Mirroring the clinical phenotype, the severity of CAA-ri and its long-term outcomes vary widely. Whereas some patients have mild symptoms or self-limited disease [9, 18], others progress to severe disability or death despite the appropriate use of immunosuppressant treatments [11, 19–21]. The factors that predict disease severity and responsiveness to first-line treatments, such as high-dose methylprednisolone, are unknown. To explore clinically-accessible associations of treat-ment-responsiveness, we assessed the relationship between clinical and paraclinical features and outcomes in consecutively accrued CAA-ri patients treated with high doses of methylprednisolone. We expected that factors associated with poorer baseline function (e.g., preexisting cognitive decline), a more severe inflammatory response (e.g., cerebrospinal fluid [CSF] pleocytosis, extent of neuroimaging abnormalities), and neuronal loss (e.g., CSF levels of neurofilament light chain [NfL], total-tau; and diffusion restriction on magnetic resonance imaging [MRI]) would associate with worse outcomes.
METHODS
Protocol approvals, registrations, and patient consent
Clinical and diagnostic data, including results of serum and CSF tests and brain MRI, were reviewed from 12 patients with CAA-ri consecutively-en-countered from September 2015 to February 2019 at our tertiary care hospital (Barnes-Jewish Hospital; Washington University School of Medicine; St. Louis, MO, USA). Patients were initially evaluated for rapidly progressive dementia, and enrolled within prospective research studies, permitting collection and evaluation of active clinical symptoms/signs and retrospective review of existing medical records. Study protocols were approved by the Washington University School of Medicine Human Research Protections Office. Patients or their delegates provided written informed consent prior to participation. Records were incomplete for one patient who was excluded from analyses. Thus, 11 patients were included in the study.
Clinical evaluation
Patients were admitted to the neurology inpatient service and evaluated by experienced clinicians. Information concerning presentation and past history was obtained from a reliable collateral source (commonly the patient’s spouse). Nine of the eleven patients met clinicoradiological criteria for probable CAA-ri [15]. The remaining two patients presented with rapid cognitive decline and strictly leptomeningeal findings on MRI. The diagnosis of CAA-ri was established on brain biopsy in these two cases (the details of one case were previously reported [16]) in accordance with established neuropathological criteria [22]. Investigations and treatments were directed by treating clinicians and were generally consistent across patients. All patients were treated with IV methylprednisolone (generally 1000 mg daily for 5 days, although one patient only received 1000 mg for two days). Two patients were treated with lower doses of steroids prior to evaluation at our center. Another two patients received additional immunomodulatory therapies late in their course (intravenous immunoglobulin 2 mg/kg divided over 5 days in one case and azathioprine 50 mg daily for 5 days in the other). Patients were followed for a median 175 days from treatment (range, 31–513).
Whereas some studies distinguish between CAA-ri as involving perivascular inflammation as opposed to amyloid-β related angiitis (ABRA) involving inflammatory infiltrates into the vessel wall [23–25], it is not clear whether these entities are truly distinct or if they exist along a spectrum with the same underlying pathophysiology and common clinical and radiological features. We use the term CAA-ri to encompass both vascular and perivascular inflammation, acknowledging that the majority of our patients were diagnosed based on clinicoradiological criteria, which does not distinguish between these entities.
Outcome assessment
The mRS was chosen as the primary outcome measure due to its ease of application (including the ability to reliably assign an mRS based on historical reports), high inter-rater reliability, and inclusion of death (mRS = 6) as an outcome [26]. The mRS has also been widely used as an outcome measure in the extant literature, including patients with autoimmune encephalitis [27, 28] and CAA-ri/ABRA [6]. For this study, the primary clinical outcome was defined as the change in modified Rankin Scale (ΔmRS), calculated by subtracting the premorbid mRS (i.e., mRS before the onset of CAA-ri symptoms) from the mRS at the last assessment. Change from premorbid baseline was chosen because a large proportion of patients with CAA-ri had at least some degree of preexisting impairment. In this context, a positive ΔmRS would reflect worsening from premorbid status following treatment, while a patient who returned to their previous level of function (i.e., the best possible outcome) would receive a ΔmRS of 0. The mRS was assigned by study clinicians integrating history and physical examination findings at each assessment, without consideration of neuroimaging or CSF findings. Premorbid mRS was inferred through interview of a knowledgeable collateral source familiar with the patient’s premorbid status, incorporating information from the medical record. Subsequent mRS were prospectively assigned by study investigators.
Biomarker measures
CSF biomarkers
Excess CSF was collected for research purposes from CAA-ri patients who underwent a clinically-indicated lumbar puncture at first presentation. Aliquots of CSF were obtained from 1:1 age- and sex-matched community dwelling cognitively normal (CN) individuals who were enrolled in longitudinal studies of memory and aging at the Washington University Knight Alzheimer Disease Research Center (St. Louis, MO) and underwent lumbar punctures for research purposes [29]. Aliquots of CSF from CAA-ri patients and CN participants were processed and stored according to established research protocols [30].
CSF levels of Aβ40, Aβ42, total tau, and phospho-tau181 were measured in cases and CN participants using a fully automated chemiluminescent enzyme immunoassay (LUMIPULSEG1200, Fujirebio). CSF NfL levels were measured using a plate-based enzyme-linked immunosorbent assay kit (UMAN Diagnostics). Insufficient CSF was available for research purposes from 4/11 patients (36%). Two of these four patients had CSF Aβ42, total tau, and phospho-tau measured via a commercial laboratory as part of clinical evaluation (ADmark® panel; Athena Diagnostics, MA).
MRI analysis
MRIs were initially reviewed by a board certified neuroradiologist, with subsequent review by study authors (A.S.P., G.S.D.). Diffusion restriction, contrast enhancement, and microhemorrhage were deemed ‘present’ if changes were detected on the MRI performed prior to treatment (baseline MRI). To quantify inflammatory changes, an ARIA-E rating scale described by Barkhof et al. [31] was applied by study authors who were aware of the clinical diagnosis, but not patient identity (thus, blinded to clinical features, mRS, and CSF findings at the time of imaging). Briefly, this scale assigns 0–5 points reflecting the size and number of T2/Fluid Attenuated Inversion Recovery (FLAIR) parenchymal and sulcal hyperintensities to each of 6 brain regions in each hemisphere. The highest scores for each region are then summed to yield a total score. A score for swelling was not assigned recognizing its poor interrater reliability [31]. ARIA-E scores were assigned for the last pre-treatment MRI (median 42 days after symptom onset, range 10–298), MRI obtained following first-line treatment (1-2 weeks post-treatment), and the first follow-up MRI obtained > 2 weeks post-treatment (median 68 days after symptom onset, range 17–200). All scans were obtained at our tertiary care center, with the exception of three pre-treatment scans that were performed at outside hospitals prior to transfer.
Statistical analysis
Data were analyzed using SPSS version 26 (IBM Corp., Armonk, NY). Continuous variables were compared to ΔmRS using nonparametric correlations (Spearman’s rho). For categorical variables, ΔmRS was compared across groups with and without the variable of interest using the Mann-Whitney U test. The Wilcoxon signed-rank test was used to compare biomarker levels in CSF from cases and matched CN participants. Statistical significance was defined as p < 0.05. Analyses were not corrected for multiple comparisons, recognizing the exploratory nature of this study.
Data availability
Anonymized data not published within the article will be shared upon request from qualified investigators.
RESULTS
Participant characteristics, clinical features, and results of investigations are summarized in Table 1. Findings for individual patients are detailed in Supplementary Table 1. Six patients had preexisting cognitive decline attributed to a neurodegenerative dementing illness, with symptomatic duration spanning 10 to 120 months (median premorbid mRS = 2, range 1–3). All patients had cognitive deficits at presentation; focal neurological deficits were detected in the majority. On the initial lumbar puncture, CSF protein was elevated in most cases; three patients had mild CSF pleocytosis (5–10 nucleated cells/μL). Only one patient had notably elevated CSF WBCs (46 cells/μL).
Demographic features, clinical characteristics and results of investigations in patients with CAA-ri
ARIA-E, amyloid related imaging abnormality (edema); CSF, cerebrospinal fluid; MRI, magnetic resonance neuroimaging. †Early post-treatment MRIs were obtained in 5 patients, a median duration of 6 days (range 5–12) following treatment for CAA-ri. ‡Late post-treatment MRIs were obtained in 10 patients, a median duration of 68 weeks (range 17–200) following treatment for CAA-ri.
Clinical outcomes and imaging findings are depicted in Fig. 1. The final mRS ranged broadly following treatment (Fig. 1A; median duration of follow-up = 175 days; range, 31–513). Three patients died of complications of CAA-ri within 3 months of treatment (mRS = 6). Of the remaining patients, 5 improved following treatment, with 3 patients recovering to within one point of their premorbid mRS, and 3 experienced no change in mRS across a median 320-day follow-up period (range, 52–513; Fig. 1B). Inflammatory changes on MRI, as measured by ARIA-E score, also varied widely among patients at presentation (Fig. 1C; median early ARIA-E score of 22, range 5–39). These abnormalities normalized in the majority of surviving patients who underwent follow-up MRI (median late ARIA-E score of 3, range 0–25; median 68 days from treatment initiation, range 17–200). A post-treatment MRI was not obtained in one patient who transitioned to hospice care prior to follow-up due to complications of CAA-ri and aspiration pneumonia. No patients experienced definite clinical or radiological recurrence across follow-up, although several patients experienced persistent waxing and waning symptoms.
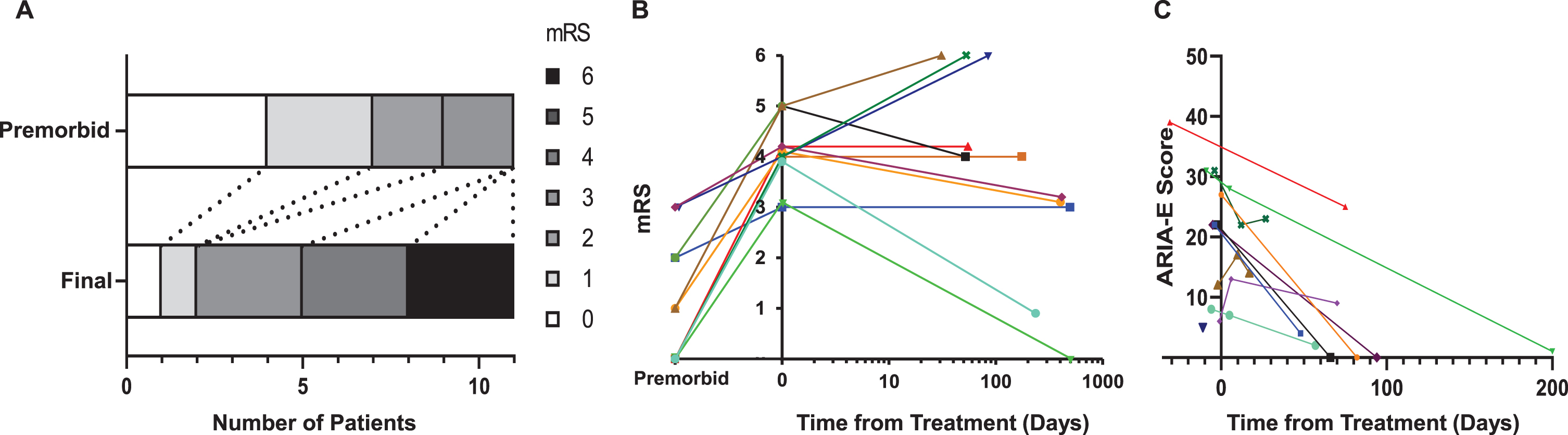
Outcomes following treatment for CAA-ri. Bar graphs (A) depict overall shifts in modified Rankin Scale (mRS) before (premorbid) the onset of symptoms attributable to CAA-ri onset and after treatment (final). The relationship between time from treatment, and mRS (B: logarithmic time scale) and amyloid related imaging abnormality (ARIA-E; C) scores are shown for individual patients with CAA-ri.
As shown in Table 2, the only clinical/demographic variable that was associated with ΔmRS was intensive care unit (ICU) admission (U = 2.0, p = 0.048). This relationship was driven by the close association between ICU admission and mortality: all three patients who required ICU admission succumbed to their illness. Increasing age was associated with worse outcome (rho = 0.55, p = 0.08), although this did not achieve pre-defined levels of statistical significance. No associations were observed between outcome and sex (U = 12.5, p = 0.79), prior cognitive decline (U = 12, p = 0.66), or time from symptom onset to treatment (rho = 0.40, p = 0.23).
Association between candidate variables and clinical outcomes (ΔmRS) following treatment
For categorical variables, median ΔmRS for each group is shown along with results of the Mann-Whitney U test. For continuous variables, rho is the rank correlation coefficient between that variable and ΔmRS. ΔmRS, change in modified Rankin Scale (from premorbid mRS); ICU, intensive care unit; ARIA-E, amyloid related imaging abnormality (edema); CSF, cerebrospinal fluid; WBC, white blood cells; Aβ, amyloid-β; pTau181, phosphorylated tau181; NfL, neurofilament light chain.
Considering common paraclinical tests, CSF WBC > 5 (U = 3.0, p = 0.042) but not protein levels (rho = –0.27, p = 0.43) associated with worse outcomes (Fig. 2). Additionally, diffusion restriction on MRI (U = 3.5, p = 0.03), but not contrast enhancement (U = 14.0, p = >0.99), was associated with worse outcomes. Microhemorrhages were present in 10 of 11 patients and were not considered as putative outcome associations. Pre-treatment ARIA-E scores were not correlated with median ΔmRS (rho = –0.02, p = 0.95). However, late post-treatment ARIA-E scores associated with ΔmRS (rho = 0.70, p = 0.02), with higher scores—corresponding to greater severity and broader distribution of inflammatory changes—associated with worse outcomes (Fig. 3). The observed relationships between variables of interest and outcomes appeared to reflect the degree of treatment responsiveness, as no clear associations were observed between clinical/demographic or paraclinical variables and mRS at the time of treatment or final mRS (Supplementary Table 2). ICU admission was the lone exception, as all three patients who required ICU admission experienced the worst possible outcomes (final mRS = 6.0; i.e., death).
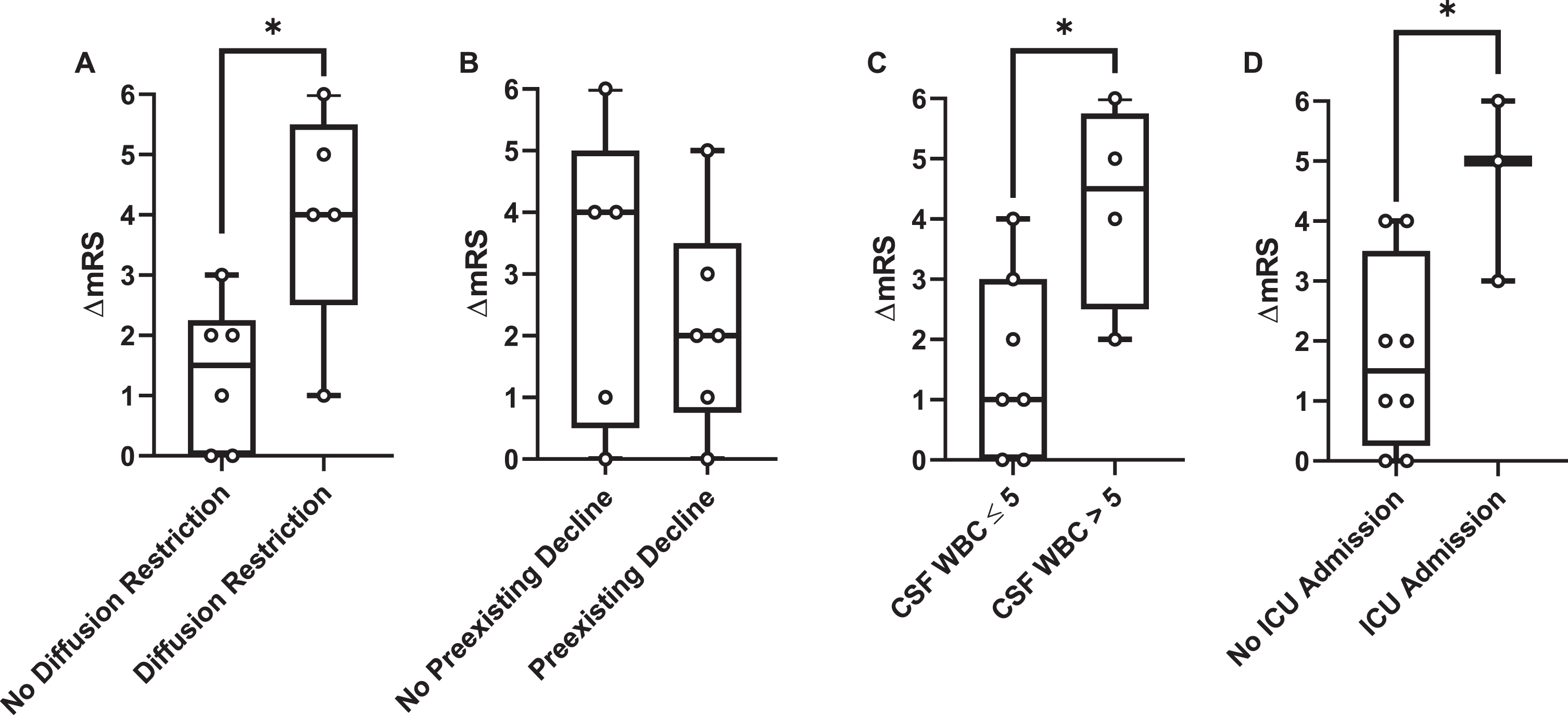
Relationships between common paraclinical tests and outcomes. Box-and-whisker diagrams depict the relationship between measured factors and change in modified Rankin Scale (ΔmRS) for (A) presence/absence of diffusion restriction on magnetic resonance neuroimaging during the index admission, (B) presence/absence of preexisting cognitive decline, (C) presence/absence of CSF pleocytosis and (D) requirement for intensive care unit (ICU) admission. *p < 0.05.
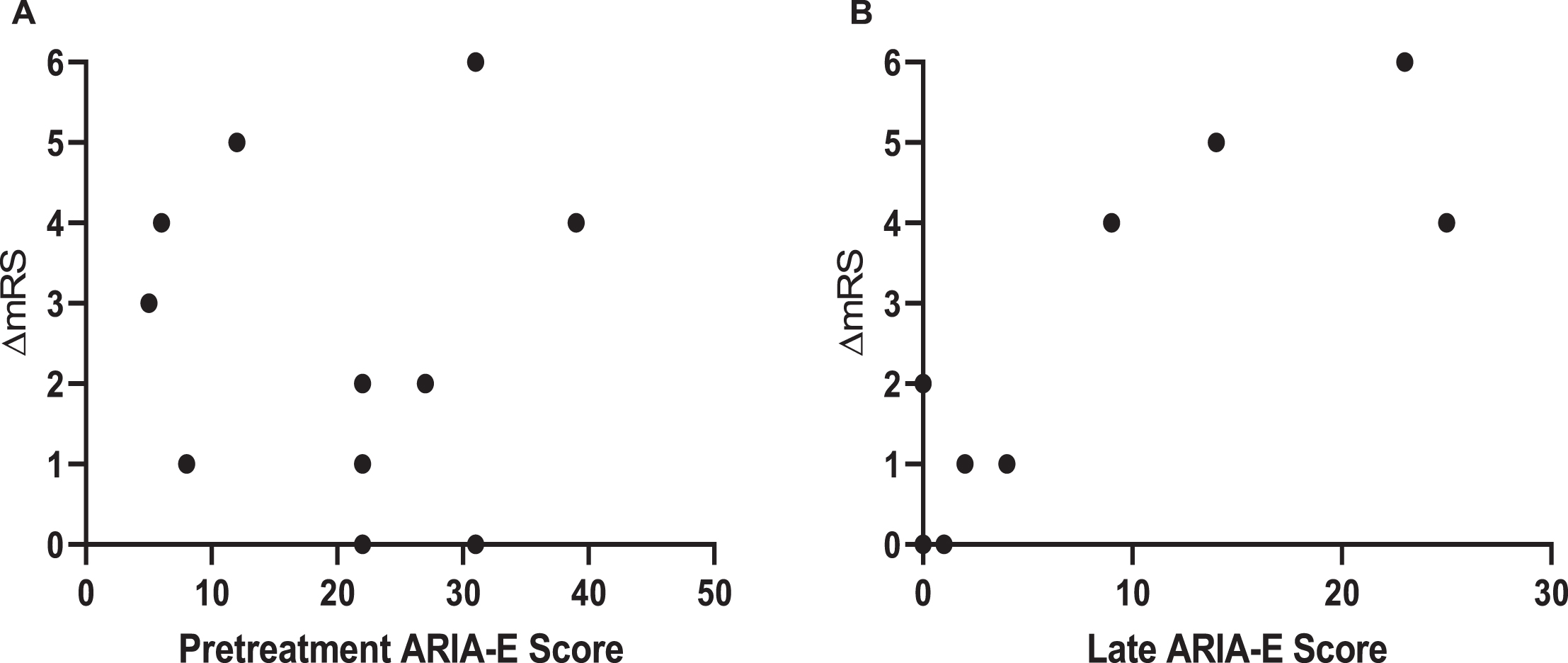
Relationship between ARIA-E scores and outcomes. Scatterplots depict the relationship between early (pre-treatment; A) and late (B) ARIA-E scores, and the change in modified Rankin Scale (ΔmRS). Only late ARIA-E scores were associated with ΔmRS (rho = 0.70; p = 0.02; early ARIA-E: rho = –0.02, p = 0.95).
Biomarkers of AD (Aβ40, Aβ42, total tau, phosphorylated tau181) and neurodegeneration (total-tau, NfL) were measured in the subset of patients from whom CSF was available for research purposes (n = 7), and two additional patients who underwent clinical testing for Aβ42, total tau and phosphorylated tau181. Biomarker values were compared to those observed in 1:1 age- and sex-matched CN community dwelling participants enrolled in prospective studies of memory and aging at the Knight Alzheimer Disease Research Center (n = 9). CSF levels of Aβ40 (p = 0.02) and Aβ42 (p = 0.01) were lower in CAA-ri patients compared to CN research participants, while CSF levels of phosphorylated tau181 (p = 0.04) and NfL (p = 0.03) were higher in CAA-ri patients versus CN individuals (Fig. 4). CSF levels of total tau were higher in patients compared to CN controls, but this did not meet the predefined threshold for statistical significance (p = 0.11), owing to inclusion of one CN individual with higher-than-expected total tau (p = 0.02 when excluding this patient).
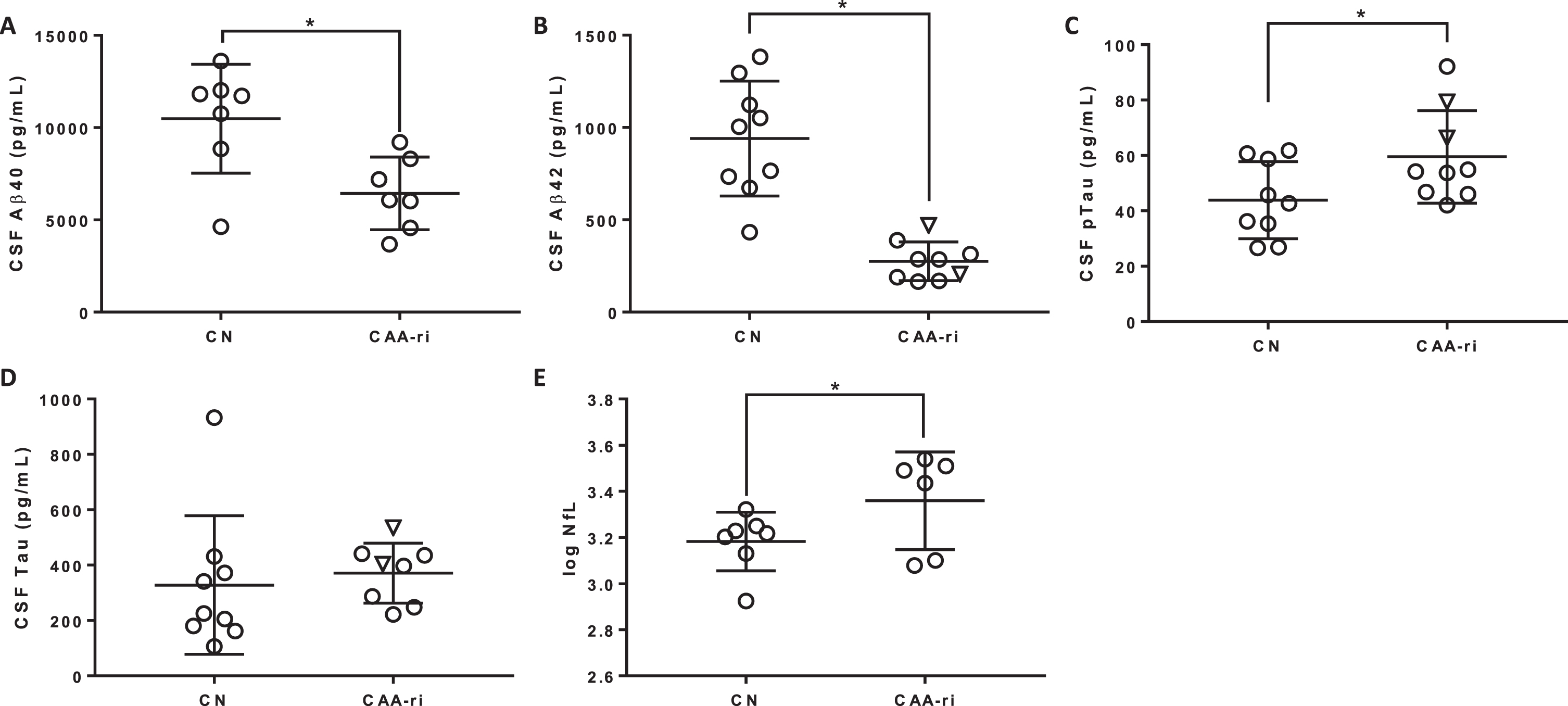
Biomarkers of Alzheimer’s disease and neurodegeneration. CSF levels of amyloid-β40 (Aβ40; A), amyloidβ42 (Aβ42; B), phosphorylated tau181 (pTau; C), total Tau (D) and neurofilament light (NfL, log-transformed; E) are shown in cognitively normal participants (CN) and CAA-ri patients. Outlying data from one CAA-ri patient was omitted from the figures for total Tau (1427 pg/mL) and log NfL (4.6) but was included in statistical analyses. Circles and inverted triangles depict biomarkers measured in research and clinical laboratories, respectively. *p < 0.05 (Wilcoxon signed-rank test).
The relationship between changes in ARIA-E scores (pre-treatment and late) and clinical and paraclinical measures were considered via post-hoc analyses. The absence of diffusion restriction on MRI was associated with greater improvement in post-treatment ARIA-E scores (median improvement of 22 points in patients without diffusion restriction, versus 8 points in those with diffusion restriction; U = 3.0, p = 0.047); no other associations were observed (Supplementary Table 3).
DISCUSSION
The requirement for ICU admission, emergence of diffusion restricting lesions on brain MRI, presence of CSF pleocytosis and lower CSF Aβ40 at presentation, and higher late ARIA-E scores (i.e., failure of T2/FLAIR hyperintensities to normalize with treatment) were associated with worse outcomes in patients with CAA-ri in this series. These markers may identify patients who are at the highest risk of negative outcomes, with implications for clinical counseling and treatment. While the need for ICU admission represents an obvious proxy measure of disease severity or treatment failure (i.e., sicker patients are more likely to require ICU admission), the relationship between other markers and treatment responsiveness remains unclear. Areas of restricted diffusion, when present, were generally punctate or very small, suggesting that the presence of acute infarction—not the volume of infarcted tissue—associated with outcome. In this context, infarction may identify patients with immune-mediated vascular and perivascular infiltrates predisposing to occlusion of small vessels and hypoperfusion of corresponding vascular territories. In the same way, increased CSF cell count at presentation may mark patients with more robust immune responses leading to increased blood brain permeability. Caution is advised, however, before extending findings observed in subsets of patients to clinical practice.
A recent study considered the relationship between several of the same variables and clinical and radiographic outcomes in 48 patients accrued over two decades [21]. In this study, 32/34 (94%) patients who received immunosuppressive agents improved clinically from presentation; radiological improvement was reported in 24/28 (86%) treated patients. Although radiological outcomes were similar to those reported in the present study (improvement was noted in 10/10 patients with longitudinal neuroimaging), clinical outcomes in our series were considerably more variable. Following treatment, 5 patients improved clinically, 3 remained unchanged, and 3 died (Fig. 1). Several factors may have contributed to this difference, including the older age of participants in our series, shorter follow-up period, and the reliance on an outcome measure that over-represents motor outcomes (mRS).
Unique to this study, we adapted a visual scoring system validated in ARIA-E to grade imaging changes in CAA-ri [31]. As this score ostensibly measured the distribution and severity of T2-hyperintensities—a correlate for inflammation—higher scores identified those patients in whom imaging lesions failed to resolve with treatment. While pre-treatment ARIA-E scores did not correlate with outcomes, higher late ARIA-E scores were associated with worse outcomes. These findings suggest that longitudinal neuroimaging measures may inform treatment-responsiveness, with potential applications in clinical trials of disease-modifying therapies for CAA-ri.
CSF Aβ40 and Aβ42 were lower in CAA-ri patients than age- and sex-matched CN individuals in this series. This is consistent with the findings of a prior study assessing biomarkers in CAA-ri [32], but at odds with an earlier study that found that CSF Aβ40 and Aβ42 levels were similar in patients and controls at presentation, but lower in CAA-ri patients in the remission phase [9]. Differences across studies may reflect variability in the timing of CSF sampling, recognizing that the phase during which Aβ levels are elevated may not correspond to the period during which patients are most clinically symptomatic, i.e., biochemical remission may precede symptomatic improvement. Studies including longitudinal sampling of CSF are required to determine the timing and order of changes in CSF amyloid species over the course of the disease, and the relationships between amyloid measures and clinical outcomes.
Surprisingly, preexisting cognitive impairment did not influence treatment responsiveness, noting that patients with cognitive impairment were as likely to return to their premorbid mRS following treatment as patients without impairment. Similarly, neither CSF biomarkers associated with cerebral amyloid deposition (Aβ42) [33], neurofibrillary tangle burden (e.g., phosphorylated tau [34]) nor neuroaxonal loss (e.g., CSF levels of NfL [35] and total-tau [36]) associated with worse outcomes following treatment. These findings suggest that treatment responsiveness in CAA-ri patients was independent of baseline cognitive status and the severity of underlying AD neuropathological change. Thus, patients with CAA-ri may benefit from acute treatment with intravenous methylprednisolone, regardless of baseline cognitive status. This point is worth emphasizing in light of research suggesting that prevalent biases and treatment preferences may influence neurologists’ willingness to offer potentially life-saving treatments (e.g., tissue plasminogen activator) to patients with dementia presenting with acute neurologic decline [37].
Limitations
The majority of CAA-ri cases were diagnosed in accordance with clinicoradiological criteria [15], without pathologic confirmation. Although diagnostic accuracy cannot be assured in all cases, this approach increasingly mirrors clinical practice, favoring the generalizability of our findings. Additionally, the small sample size limited our ability to make strong inferences or to perform multivariable analyses required to consider the relationship between variables and outcomes. There is a clear need to confirm the direction and magnitude of associations between clinical and paraclinical markers and treatment-responsiveness in CAA-ri through future well-powered studies. This is especially pertinent for associations between outcomes, and CSF and neuroimaging biomarkers, which were obtained at variable times following presentation, and may have influenced clinicians’ selection of therapies, decisions concerning withdrawal of care, and outcomes. Future studies should also consider the influence of other factors implicated in the pathogenesis of CAA-ri (e.g., APOE genotype [24] and anti-amyloid antibodies [9, 20]) on meaningful outcomes, including measures of cognitive function and quality of life. Such outcomes are likely to be overlooked by simple measures of disability, including the mRS [38], compromising our ability to appreciate clinically meaningful changes in recovering patients. Concerning generalizability, all patients were treated with high doses of methylprednisolone, with two patients receiving additional therapies before transitioning to supportive care. As a result, our findings are best applied to evaluating outcomes following treatment with corticosteroids. Similarly, as no patients experienced definite disease recurrence, study results cannot be extended to inform the determinants of relapse in CAA-ri.
CONCLUSIONS
The requirement for ICU admission, emergence of diffusion restricting lesions on brain MRI, CSF pleocytosis and lower CSF Aβ40 at presentation, and failure of inflammatory changes on MRI to normalize with treatment were associated with worse outcomes in CAA-ri patients treated with corticosteroids. Routine assessment of these factors may identify patients with CAA-ri who may benefit from additional immunosuppressant therapy or treatment approaches.
Footnotes
ACKNOWLEDGMENTS
Study conduct was made possible by support from the NIH via grants K23AG064029, P50AG005681, P01AG003991, and P01AG026276, and through philanthropic contributions to promote research and education in autoimmune encephalitis (GSD). Study funders did not contribute to the design or conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.