
Abstract
Background:
Central arterial stiffness and brain hypoperfusion are emerging risk factors of Alzheimer’s disease (AD). Aerobic exercise training (AET) may improve central arterial stiffness and brain perfusion.
Objective:
To investigate the effects of AET on central arterial stiffness and cerebral blood flow (CBF) in patients with amnestic mild cognitive impairment (MCI), a prodromal stage of AD.
Methods:
This is a proof-of-concept, randomized controlled trial that assigned 70 amnestic MCI patients into a 12-month program of moderate-to-vigorous AET or stretching-and-toning (SAT) intervention. Carotid β-stiffness index and CBF were measured by color-coded duplex ultrasonography and applanation tonometry. Total CBF was measured as the sum of CBF from both the internal carotid and vertebral arteries, and divided by total brain tissue mass assessed with MRI to obtain normalized CBF (nCBF). Episodic memory and executive function were assessed using standard neuropsychological tests (CVLT-II and D-KEFS). Changes in cardiorespiratory fitness were measured by peak oxygen uptake (VO2peak).
Results:
Total 48 patients (29 in SAT and 19 in AET) were completed one-year training. AET improved VO2peak, decreased carotid β-stiffness index and CBF pulsatility, and increased nCBF. Changes in VO2peak were associated positively with changes in nCBF (r = 0.388, p = 0.034) and negatively with carotid β-stiffness index (r = –0.418, p = 0.007) and CBF pulsatility (r = –0.400, p = 0.014). Decreases in carotid β-stiffness were associated with increases in cerebral perfusion (r = –0.494, p = 0.003). AET effects on cognitive performance were minimal compared with SAT.
Conclusion:
AET reduced central arterial stiffness and increased CBF which may precede its effects on neurocognitive function in patients with MCI.
Keywords
INTRODUCTION
Reduced cerebral blood flow (CBF) and elevated central arterial stiffness are emerging risk factors for age-related cognitive decline, mild cognitive impairment (MCI), and dementia including Alzheimer’s disease (AD) [1–6]. As a consequence of central arterial stiffening, cerebral blood vessels, particularly the arterioles and capillary vascular beds, are exposed to augmented arterial pulsations (i.e., increases in arterial pressure and blood flow pulsatility), which may lead to cerebral endothelial dysfunction, vasoconstriction, and brain hypoperfusion [6–8]. Chronic brain hypoperfusion and high arterial pulsation have also been linked to the brain tissue damage (e.g., brain atrophy and white matter hyperintensities) as well as cognitive impairment [2, 9]. Therefore, interventions to decrease central arterial stiffness may lead to increase in CBF, which could prevent or delay the onset and progression of age-related cognitive decline and dementia [3, 8].
There is some evidence that aerobic exercise train-ing (AET) may decrease central arterial stiffness [10–12], increase regional brain perfusion [13–15], and improve cognitive performance [16] in cognitively normal older adults. Moreover, higher cardio-respiratory fitness has been associated with lower central arterial stiffness [12] and higher CBF [17]. In a recent study, we also showed that AET may increase regional CBF in patients with amnestic MCI, a prodromal stage of AD, but had minimal effects on neurocognitive function when compared to stretching-and-toning (SAT) intervention [18, 19]. However, at present, the effects of AET on central arterial stiffness and CBF are inconclusive, and the relationship between changes in central arterial stiffness and CBF remains unknown [6, 20].
Amnestic MCI may represent a critical time window for implementing lifestyle interventions for preventing further cognitive decline [21]. Understanding the effects of AET on central arterial stiff-ness and CBF in amnestic MCI is crucial in that we currently lack effective interventions to prevent or treat AD [22]. The purpose of this study was to investigate the effects of one-year AET on central arterial stiffness and CBF as well as their relationship to cognitive performance in patients with amnestic MCI. We hypothesized that AET would reduce central arterial stiffness and increase CBF and that these hemodynamic changes would be associated with cognitive performance in previously sedentary MCI patients.
MATERIALS AND METHODS
The present study was a sub-study of a one-year, single-blinded, proof-of concept, parallel randomized controlled trial (RCT) comparing effects of moderate-to-vigorous AET versus SAT programs on neurocognitive function in amnestic MCI patients (ClinicalTrials.gov: NCT01146717) [18]. In the parent study, measurements of cardio- and cerebro-vascular hemodynamics, cardiorespiratory fitness, and neurocognitive function were conducted at baseline, midpoint (6-month), and trial completion (12-month). Magnetic resonance imaging (MRI) was performed at baseline and trial completion (12-month). The randomization procedures and trial design were explained in detail in a previous report [18] and are presented briefly in Supplementary Figure 1. During the study, participants were instructed not to disclose their group assignment or to discuss their interventions during measurements or meeting with blinded investigators or other participants. All the collected data were de-identified prior to analysis. Investigators conducting data analysis were blinded to the randomization codes. The intervention programs and the procedures for data collection and analysis related to this study are presented below.
Participants
Seventy patients with amnestic MCI were recruited from the University of Texas Southwestern Medical Center Alzheimer’s Disease Center, senior centers in the Dallas-Fort Worth metropolitan area, and local newspaper advertisements. Inclusion criteria were men and women aged between 55 and 80 years who were diagnosed with amnestic MCI. The diagnosis of amnestic MCI was based on Petersen criteria [23] as modified by the Alzheimer’s Disease Neuroimaging Initiative (http://adni-info.org/). Specifically, we used a global Clinical Dementia Rating scale of 0.5 with a score of 0.5 in the memory category, an objective memory loss as indicated by education-adjusted scores of approximately one standard deviation below the normative mean on the Logical Memory subtest of the Wechsler Memory Scale-Revised (WMS-R), and a Mini-Mental State Exam (MMSE) score between 24 and 30. Participants who were obese (BMI ≥35 kg/m2) and had uncontrolled hypertension and diabetes were excluded because these conditions may have significant impact on central arterial stiffness [24] and CBF [25]. Individuals who participated in moderate to vigorous intensity AET more than 3 times per week with each session lasting >30 min over the past two years were also excluded. Screening procedures included a detailed medical history and medication questionnaire, a comprehensive physical examination, 12-lead electrocardiogram, echocardiography, and carotid artery ultrasonography to excluded severe carotid stenosis (>50%) and overt cardiovascular disease. Detailed inclusion and exclusion criteria are provided in our previous study [18].
This study was approved by the Institutional Review Board of the University of Texas Southwestern Medical Center and Texas Health Presbyterian Hospital Dallas, and was performed in accordance with the guidelines of the Declaration of Helsinki and Belmont Report. All participants provided informed written consent prior to participation. This trial was registered at ClinicalTrials.gov (NCT01146717: Aerobic Exercise Training in Mild Cognitive Impairment Study).
Intervention
AET program
The moderate-to-vigorous AET program was based on each individual’s fitness level evaluated with peak oxygen uptake (VO2peak) treadmill testing. Exercise intensity, duration, and frequency were gradually progressed as participants adapted to their previous exercise level. Specifically, the program began with 3 exercise sessions per week for 25–30 min per session at the intensity of 75–85% of maximal heart rate (HR) which was measured during VO2peak treadmill testing at baseline. At week 11, 3 or 4 aerobic exercise sessions per week for 30–35 min per session were performed. In the week participants performed 3 exercise sessions per week, a high intensity exercise session was introduced which consists of 30 min of exercise at the intensity of 85–90% of maximal HR (e.g., brisk uphill walking). After week 26, participants performed 4 or 5 exercise sessions per week for 30–40 min, including two high intensity sessions. Each exercise session included a 5 min warm-up and a 5 min cool-down.
SAT program
The SAT program was used as an active control group to maintain participants’ attention at a similar level as the AET program. The frequency and duration of SAT program were same as the AET program. This program focused on the upper and lower limb stretching exercises. During each session, participants were asked to keep their HR below 50% of maximal HR. At week 19, a second set of full body stretching exercise that is more advanced than the previous set was prescribed. At week 26, a set of low resistance TheraBand exercise that focuses on strengthening the upper and lower body was prescribed.
In both programs, each participant was closely supervised by an exercise physiologist for the first 4–6 weeks to make sure that the participant understood and became familiar with AET or SAT instruc-tions and could perform exercise safely by themselves either at a fitness center or home. During the study period, all participants were asked to perform the assigned interventions on top of their regular physical activities. To ensure adherence to AET and SAT interventions, participants were required to keep a detailed training log in addition to HR monitoring during each of exercise sessions and to meet with an exercise physiologist monthly or as needed to review and resolve training related issues. The average compliance to exercise training was ∼ 69%, which is calculated as a ratio of the prescribed exercise sessions over the actually completed sessions in which participants achieved the target heart rate [18].
Measurements
Cardiovascular hemodynamics
All hemodynamic data were collected in an environmentally controlled laboratory with an ambient temperature of about 22C. After participants were instrumented and rested in the supine position for > 15 min, brachial cuff blood pressure was measured intermittently at least three times using an electrocardiography (ECG)-gated electro-sphygmo-manometer (Suntech, Morrisville, NC, USA) and averaged to obtain systolic (SBP), diastolic (DBP), and mean blood pressure (MBP). Applanation tono-metry (SphygmoCor 80, AtCor Medical) was used to obtain continuous arterial pressure waveforms from the carotid, brachial, and femoral arteries. Carotid pressure waveform was calibrated to the brachial MBP and DBP using a procedure described previously [26]. The carotid-femoral pulse wave velocity (cfPWV) was measured by the standard procedure [27]. The common carotid artery (CCA) images were obtained by a 3-to–12 MHz linear array transducer with duplex ultrasonography (CX50, Philips Ultrasound, Bothell, WA, USA). The systolic and diastolic CCA diameters were measured using an edge-detection software (Vascular Tool 5; Medical Imaging Applications, Coralville, IA, USA) [12]. Carotid β-stiffness index was calculated as a measure of the local carotid arterial stiffness adjusted for the distending pressure [28]. Carotid intima-media thickness (CIMT) was assessed as a surrogate measure of carotid atherosclerotic severity [29].
Cerebrovascular hemodynamics
Cerebrovascular hemodynamics in both steady-state and pulsatile components were obtained by duplex ultrasonography (CX50, Philips Ultrasound, Bothell, WA, USA) and transcranial Doppler (TCD: Multi-Dop X2: Compumedics/DWL, Singen, Germany) [30]. The former was used to obtain total CBF as a sum of blood flow measured from the bilateral internal carotid (ICA) and vertebral arteries (VA) [31, 32] (i.e., the detailed methodology for CBF measurement is presented in the Supplementary Material). Cerebrovascular resistance (CVR) was calculated by MBP/total CBF; normalized CBF (nCBF) was obtained by total CBF/brain tissue mass which was obtained based on MRI measurement of total brain tissue volume and an estimate of brain tissue density of 1.06 g/mL [33]. To assess pulsatile components of CBF, CBF velocity (CBFV) was measured from the middle cerebral artery (MCA) using TCD. The normalized systolic and diastolic CBFV as well as pulsatility index (PI) were calculated by dividing their absolute values by mean CBFV (CBFV %) [34]. End-tidal carbon dioxide (EtCO2) was measured using capnography (Carpnograd, Novamatrix, Wallingford, CT, USA) during CBF assessment.
MRI measurement of brain tissue volume and white matter hyperintensity (WMH)
T1-weighted magnetization-prepared rapid acquisition gradient-echo (MPRAGE) sequence was im-plemented using a 3-tesla scanner (Achieva 3.0T, Philips Medical System, the Netherlands) to obtain high-resolution brain structural images. The FreeSurfer software (version 6.0, https://surfer.nmr.mgh.harvard.edu) was used for tissue segmentation to measure brain gray matter and white matter volume. The total brain tissue volume was calculated as a sum of the volumes of the cerebrum, cerebellum, and brainstem. WMH was measured from FLAIR images using a lesion prediction algorithm implemented in the LST toolbox for Statistical Parametric Mapping (SPM12) (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/). Detailed MRI data collection and processing methods are provided in the Supplementary Material.
Neuropsychological function
Standardized total and delayed free recall scores from the California Verbal Learning Test-second edition (CVLT-II) [35], along with scores from the Trail Making, Color-Word inhibition, and Letter and Category Fluency scores from the Delis-Kaplan Executive Function System (D-KEFS) [36] were used to assess episodic memory and executive function. These tests are widely used, are sensitive for detecting cognitive decline in older adults, and have been used to reveal the effects of AET and cardiorespiratory fitness on neurocognitive function [14, 37].
Cardiorespiratory fitness
The VO2peak was assessed by a modified Astrand-Saltin protocol on a treadmill [38]. During testing, participants walked or jogged at a fixed speed, which was determined by individual fitness level [39]. The treadmill grade was subsequently increased by 2% every 2 min until volitional exhaustion. VO2 was measured during the 2nd minute of each stage using the Douglas bag method. Gas fractions were analyzed by mass spectrometry (Marquette MGA 1100), and ventilatory volume was measured by a Tissot spirometer. HR was monitored continuously via ECG. The VO2peak was defined as the highest VO2 measured during the last stage of testing from at least a 40 second Douglas bag collection [39]. The criteria used to suggest that VO2peak was achieved included an increase in VO2 < 150 ml despite increasing work rate 2% grade, a respiratory exchange ratio > 1.1, and HR < 5 beats/min of age-predicted maximal values (220-age). In all cases, at least two of these criteria were achieved, confirming the identification of VO2peak based on the American College of Sports Medicine guideline [40]. Our previous studies have shown that by using these methods, VO2peak can be measured reliably in sedentary older adults [39, 41].
Statistical analysis
Independent t-test and chi-square test were used to compare group differences at baseline for continuous and categorical variables, respectively. The primary analysis was performed using linear mixed model (LMM) with all available data (i.e., the intent-to-treat principle) from the randomized participants who had baseline and either 6- or 12-month data or both (Supplementary Figure 1) with an assumption of missing data at random [42]. Both the main and the interaction effects of group (AET versus SAT) and time (baseline, 6-month, versus 12-month) on central arterial stiffness, CBF, and other outcome measures were included in the LMM. Individual intercepts and slopes were specified as random effects. An unstructured covariance matrix was used to account for within-subject correlations. Model parameters were estimated using the restricted maximum likelihood method [42]. Post-hoc multiple pairwise comparisons were corrected by the Bonferroni methods in case of significant main effects or group-by-time interactions. Pearson’s correlation was performed to examine linear associations between variables.
Secondary data analyses were performed by using a serial mediation analysis to explore the effects of exercise-related changes in VO2peak, central arterial stiffness, and arterial pulsation on CBF. We used bootstrapping (5000 samples) to calculate bias-corrected 95% confidence intervals (CI) of the explained associations using the PROCESS statistical package [43]. Indirect effects were interpreted as significant if zero was not included in the 95% CI [43]. Statistical significance was set a priori at p < 0.05. Data normality was checked by the Shapiro-Wilk test and the visual inspection of histogram and Q-Q plots. All analyses were performed using SPSS 20.0 (IBM Corporation, Armonk, NY, 2011).
RESULTS
Participant characteristics were similar between the SAT and AET groups, including age, sex, education, and the scores on the MMSE and Logical Memory tests (Table 1).
Participants’ demographics by randomization groups
Values represent mean±standard deviation. SAT, stretching and toning; AET, aerobic exercise training.
Intervention effect
AET significantly improved VO2peak at 6- and 12-month when compared with the SAT group (Supplementary Table 1). Carotid β-stiffness index and CBF PI decreased and nCBF increased in the AET compared with SAT groups (Fig. 1 and Table 2 and 3). Of note, ICA blood flow volume and normalized diastolic CBFV (%) increased after AET (Table 3). Systemic and carotid blood pressures, CVR, and cfPWV decreased in both groups, but CIMT did not change. As reported in our previous studies [18, 44], WMH volume increased whereas total gray matter and hippocampal volumes decreased in both groups (Supplementary Table 2). The AET group showed a small but statistically significant improvement on letter fluency performance compared with the SAT group, but no other cognitive differences were seen between groups over time (Table 4).
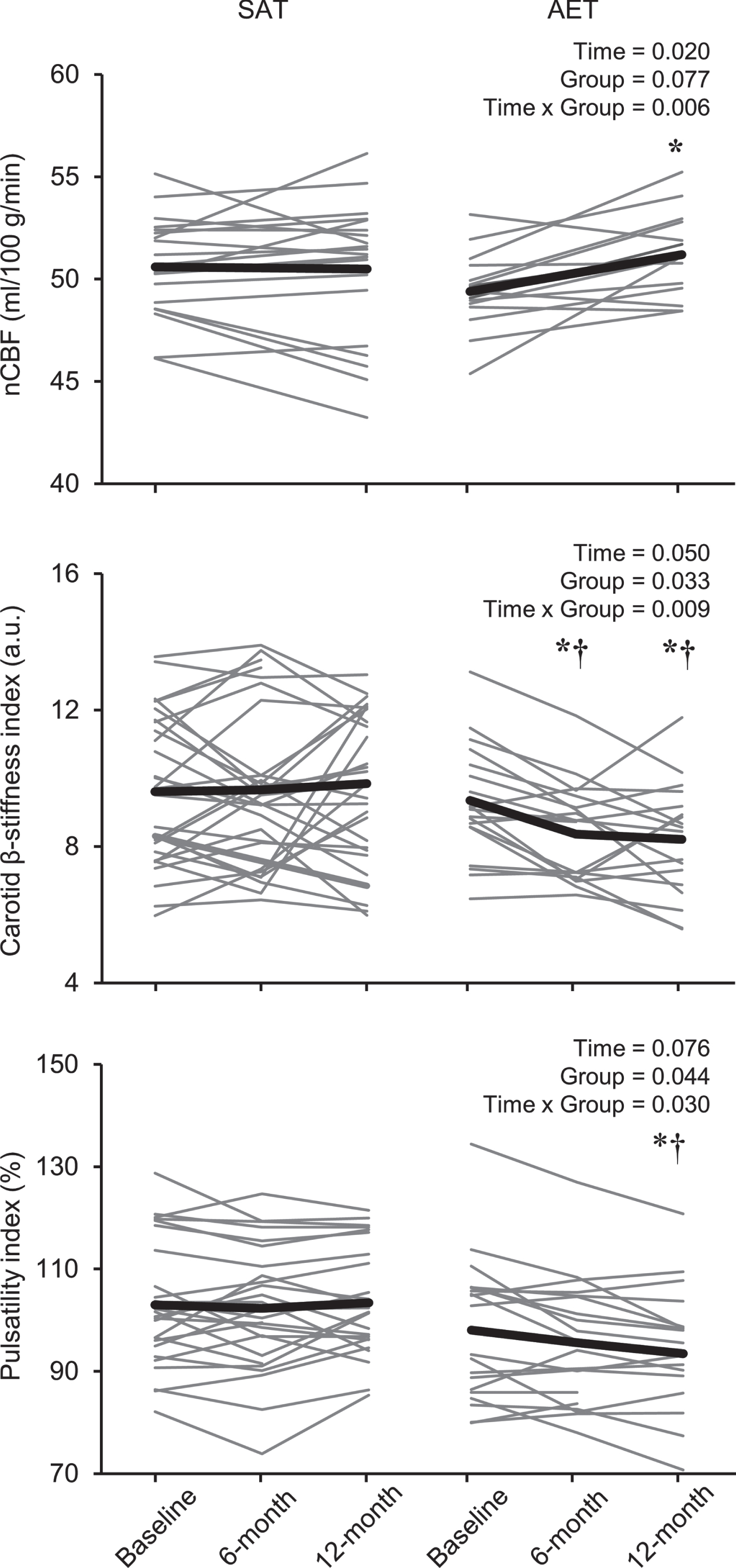
One-year changes in normalized cerebral blood flow (nCBF) (upper panel), carotid β-stiffness index (middle panel), and cerebral blood flow velocity pulsatility index measured at the middle cerebral artery (lower panel) in the stretching-and-toning (SAT) and aerobic exercise training (AET) groups. Thin lines show individual changes and the thick line represents the estimated marginal means with linear mixed model analysis (LMM). *versus baseline within the same group. †versus SAT.
Cardiovascular measurements by randomization groups
Values represent estimated marginal means [95% confidence interval (CI)] and p-values calculated from the linear mixed model (LMM). n is the number of observations. p < 0.05 are bolded. The Bonferroni correction was applied for multiple pairwise comparisons. *versus baseline within the same group. †versus SAT. SAT, stretching-and-toning; AET, aerobic exercise training.
Cerebral hemodynamic measurements by randomization groups
Values represent estimated marginal means [95% confidence interval (CI)] and p-values calculated from the linear mixed model (LMM). n is the number of observations. p < 0.05 are bolded. *versus baseline within the same group. †versus SAT. The Bonferroni correction was applied for multiple pairwise comparisons. SAT, stretching-and-toning; AET, aerobic exercise training; CBF, cerebral blood flow; TCD, transcranial Doppler; CO2, carbon dioxide.
Cognitive performance by randomization groups
Values represent estimated marginal means [95% confidence interval (CI)] and p-values calculated from the linear mixed model (LMM). Higher cognitive test scores mean better cognitive performance. n is the number of observations. p < 0.05 are bolded. *versus baseline within the same group. The Bonferroni correction was applied for multiple pairwise comparisons. SAT, stretching-and-toning; AET, aerobic exercise training.
Associations and mediation analyses
Correlation analyses revealed that increases in VO2peak across the groups after one-year AET or SAT were associated with increased nCBF and decreased CBF PI, carotid β-stiffness index (Fig. 2), and cfPWV (r = –0.350, p < 0.025). Furthermore, correlation analyses between individual changes in central and cerebral hemodynamics revealed that: 1) decreased carotid β-stiffness index was associated with increased nCBF and diastolic CBFV (%) and decreased CBF PI, and 2) increased nCBF was associated with the decreased CBF PI and increased diastolic CBFV (%) (Supplementary Table 3).
Based on these observations, we examined if changes in carotid β-stiffness index and CBF PI would mediate the association between changes in VO2peak and nCBF (Fig. 3). Inclusion of both carotid β-stiffness index and CBF PI in the mediation path attenuated the positive association between VO2peak and nCBF. This result was further confirmed by a bootstrapping assessment, which demonstrated significant indirect effects of carotid β-stiffness index and CBF PI on nCBF (95% CI: –0.001 to –0.207) (Fig. 3).
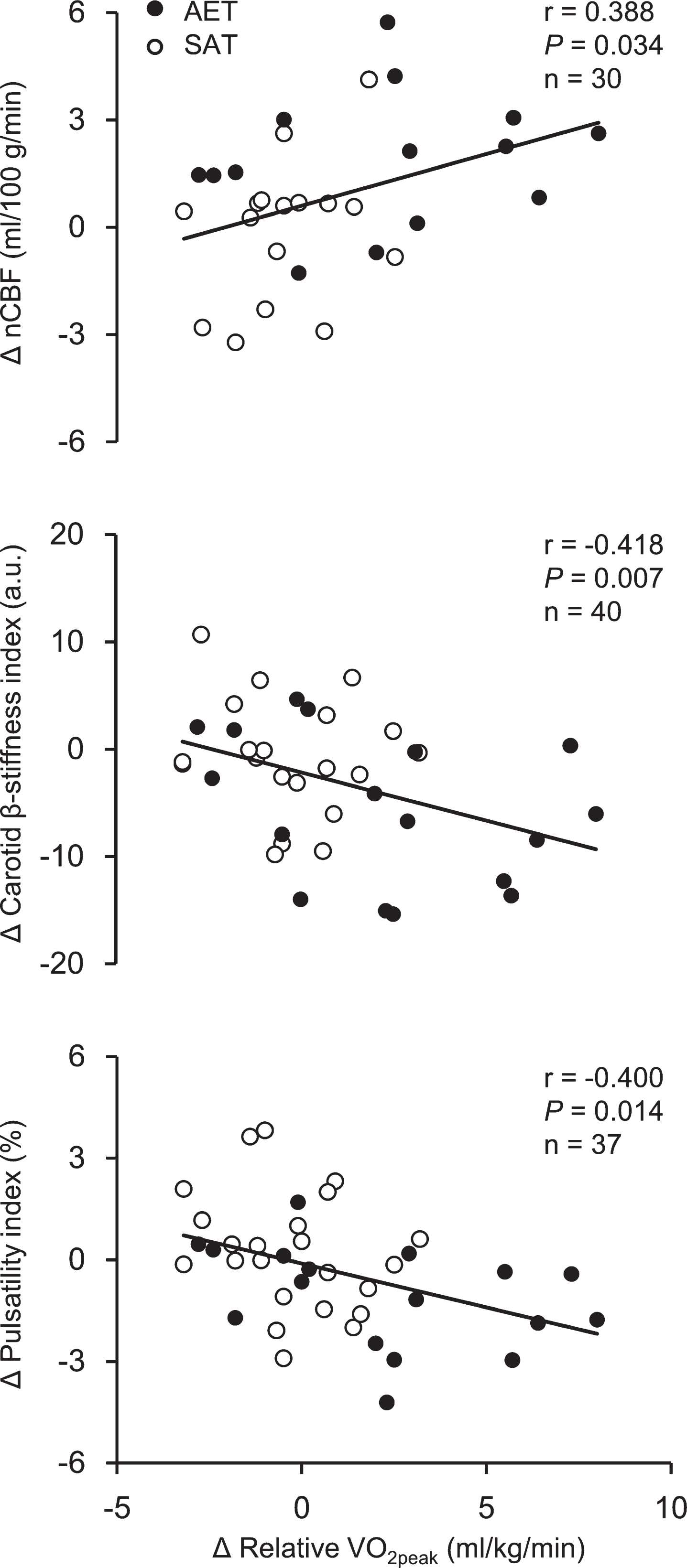
Correlations of one-year changes in peak oxygen uptake (VO2peak) with cerebral blood flow (upper panel), carotid β-stiffness index (middle panel), and cerebral blood flow velocity pulsatility measured at the middle cerebral artery (lower panel) across the stretching-and-toning (SAT) and aerobic exercise training (AET) groups. Note that the differences in the subjects numbers in the figure panels were due to the differences in the available measurements pre and post one-year interventions.
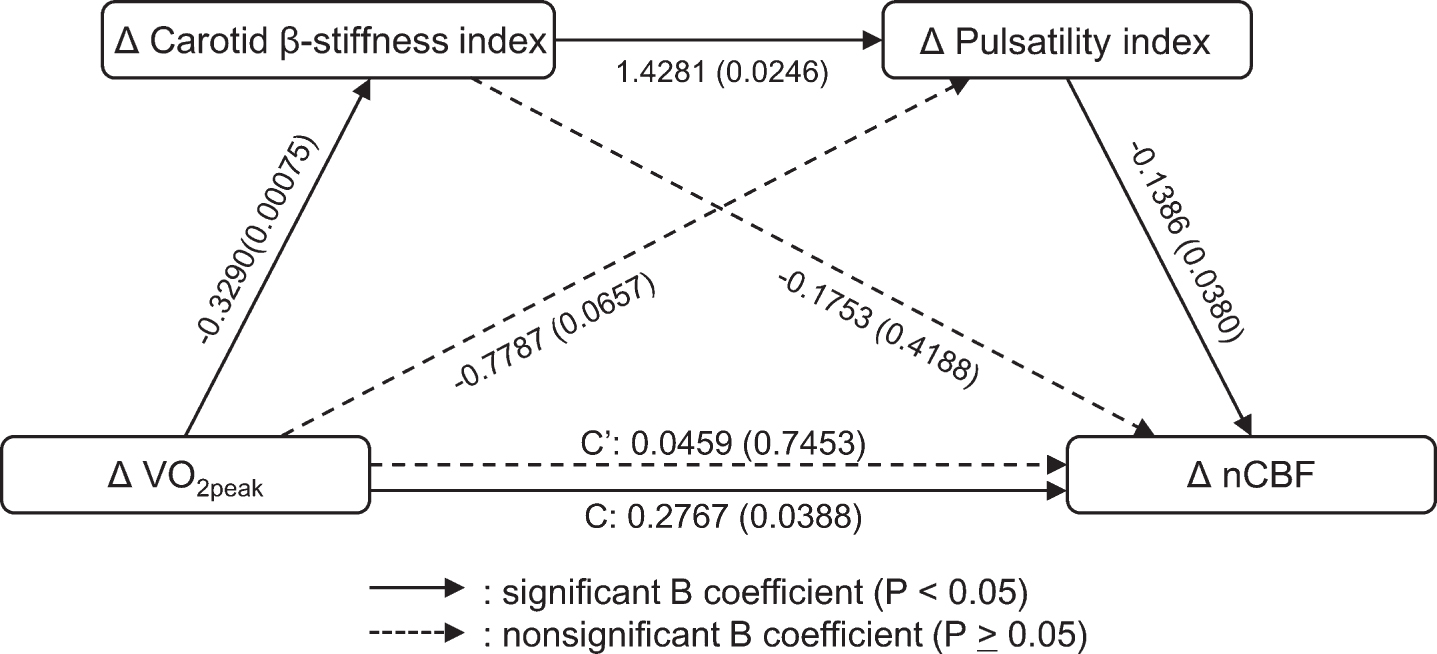
A serial mediation model to assess the relationship between changes in carotid arterial stiffness, CBF pulsatility index, peak oxygen uptake (VO2peak), and CBF across the groups after one-year aerobic exercise training or stretching-and-toning. B, unstandardized regression coefficients. A data set of n = 30 was used for modeling.
Further correlation analyses revealed that individual changes in cfPWV and CIMT across the groups after one-year AET or SAT were associated negatively with changes in the D-KEFS letter fluency and the D-KEFS color-word inhibition scores, respectively (Supplementary Table 4). Notably, a negative correlation between the changes in cfPWV and D-KEFS letter fluency score was observed only in the AET group (r = –0.682, p = 0.003), but not in the SAT group (r = –0.049, p = 0.819). None of changes in VO2peak, systemic and cerebral hemodynamics, and volumes of WMH and brain tissue were associated with changes in cognitive performance (Supplementary Table 4). No significant associations were observed between changes in central arterial stiffness and changes in WMH volume and brain tissue volume (data not shown).
DISCUSSION
The main findings from this study are as follows. First, compared with the SAT group, one-year moderate-to-vigorous AET reduced carotid arterial stiffness and CBF pulsatility while increasing global CBF in patients with amnestic MCI. Of note, AET-related increase in CBF is due mainly to the increased ICA blood flow and is associated with the increases in diastolic CBF velocity measured at the MCA. Second, improved cardiorespiratory fitness, as measured by VO2peak, was associated with reduced central arterial stiffness and pulsatile CBF and increased CBF across the groups after one-year of AET or SAT, suggesting the presence of a potential “dose-response” relationship between changes in cardiorespiratory fitness, arterial stiffness, and CBF. Furthermore, mediation analysis showed that the positive association between changes in cardiorespiratory fitness and CBF was mediated by reductions in carotid stiffness and CBF pulsatility. Third, AET improved the D-KEFS letter fluency score when compared with SAT, suggesting improved executive function performance. In addition, individually reduced cfPWV and CIMT across the groups after one-year of AET or SAT were associated with improved D-KEFS letter fluency and the D-KEFS color-word inhibition score. Collectively, these findings demonstrated the benefits of moderate-to-vigorous AET on reducing cardiovascular risk factors and improvement in CBF in patients with amnestic MCI, which may improve neurocognitive function.
AET effects on CBF and central arterial stiffness
There is a significant knowledge gap in our understanding of the influence of AET on CBF regulation and its potential relation to age-related cognitive decline or dementia prevention [20]. Previous studies have reported that regular aerobic exercise may increase regional brain perfusion in cognitively normal subjects [13–15]. For example, aerobically trained athletes have greater brain perfusion in the posterior cingulate and precuneus [15] and the occipital area [14] when compared with age-matched sedentary individuals. Three months of AET also increased brain perfusion in the anterior cingulate region in previously sedentary older adults [13]. More recently, we found, in a subgroup of this same cohort of patients with amnestic MCI, that AET increased brain perfusion in the anterior cingulate-cortex while reducing perfusion in the posterior-cingulate-cortex when compared with SAT, which suggested a redistribution of brain perfusion associated with exercise training [19]. The findings of this study that AET increased global CBF measured from bilateral ICAs and VAs using color-coded duplex ultrasonography is new. The finding that the increases in global CBF can be attributed mainly to the ICA suggests that AET increased CBF mainly in the anterior and middle parts of the brain [45], which are often affected in patients with MCI or AD [1, 32].
To our knowledge, this is the first study to show a reduction of carotid arterial stiffness by AET in patients with amnestic MCI. Arterial stiffening is determined mainly by the elastin and collagen contents as well as the smooth muscle tone of the arterial wall [24]. Several previous studies of 3-4 months of AET suggested that reduced vascular smooth muscle tone, related to the improved endothelial function, decreased sympathetic neural activity or enhanced sympatholysis mediated by nitric oxide (NO), may be the underlying mechanism of exercise-related reduction of central arterial stiffness in older adults [10, 11]. Alternatively, there is increasing recognition of contributions of amyloid-β on vascular function [46]. Activation of amyloidogenic pathway leads to impairment of vasodilating properties of artery by reduction of NO activity and endothelium dependent vasodilation [46]. AET may reduce vascular amyloid-β deposition leading to a reduction of carotid arterial stiffness [46–48].
This study suggests that the AET increased CBF is related to the reduced central arterial stiffness. The large central elastic arteries expand during systole which attenuates the transmission of systolic pressure energy into the peripheral circulation [49]. During diastole, the arterial wall recoils to maintain DBP and generates a continuous blood flow into the peripheral vascular beds. This cyclic central arterial wall motion and its impacts on end-organ perfusion have been referred as the Windkessel effects [49]. It has been speculated that impaired Windkessel function and elevated arterial pulsations may cause cerebral endothelial dysfunction, increased cerebrovascular tone (i.e., increased CVR), and reduced CBF [8]. In this respect, serial mediation analysis supports our hypothesis that AET-induced improvements of CBF are related to the reductions in carotid β-stiffness and CBF pulsatility (Table 3, Fig. 2).
In addition, we observed that changes in carotid β-stiffness are associated negatively with changes in diastolic CBFV% which was increased in the AET group. Finally, changes in both carotid pulse pressure and CBF pulsatility are associated positively with CVR suggesting increases in cerebrovascular tone associated with elevated arterial pulsation [7, 8]. Collectively, these findings provide a mechanistic insight into the role of carotid arterial stiffness and arterial pulsation in the AET-induced increase in CBF.
Cognitive performance, brain volume, WMH
Increases in central arterial stiffness [3–5], brain hypoperfusion [1], elevated CVR [50], and increased arterial pressure and CBF pulsatility [2] all have been associated with age-related cognitive decline, MCI, and dementia. In the present study, we observed that the AET group improved slightly on the D-KEFS Letter Fluency task when compared to SAT, and that reductions in cfPWV and CIMT across the groups after one-year of AET or SAT were associated with improvements in the D-KEFS Letter Fluency and the D-KEFS Color-Word inhibition score. Particularly, we observed that reductions in cfPWV were associated with increases in the D-KEFS letter fluency score only in the AET group, not in the SAT group. These findings are consistent with a previous observational studies which suggested that exercise-related reductions in central arterial stiffness may improve executive function [14], though we did not see any effects of AET on episodic memory.
However, a few questions remain to be answered. First, in the present study, we did not find correlations between the AET-induced reductions in carotid arterial stiffness and changes in cognitive performance. Second, there were no correlations between changes in CBF and cognitive performance. Third, one-year AET did not prevent reductions in total brain and hippocampal volume and increases in WMH volume despite its demonstrated benefits for reducing carotid arterial stiffness and increasing global CBF. The answers to these questions are complicated by the limitations of this study as discussed below. We speculate it is possible that the effects of AET on brain structure and function may be related to the presence of brain pathophysiological changes in patients with MCI [1, 50] as well as a potential “dose-response” relationship between exercise training and its benefits on the brain [16, 45]. In addition, AET-induced improvements in arterial stiffness and CBF may precede changes in brain structure and function in patients with amnestic MCI.
Study strengths and limitations
There are several strengths of our study. First, this is the first randomized controlled study in patients with amnestic MCI that investigated the effects of one-year moderate-to-vigorous AET on central arterial stiffness and cerebral hemodynamics and their potential relationship with cognitive performance, brain tissue volume, and WMH. Second, the test-retest reproducibility of our systemic hemodynamics and cerebrovascular measurements exhibited strong intra-class correlations, which indicates the reliability of our data (Supplementary Table 5). Lastly, a comprehensive assessment of central arterial stiffness, carotid arterial and CBF pulsation, and global changes in CBF together with objective measurement of VO2peak allowed us to investigate the relationship between cardiopulmonary fitness, systemic, and cerebral hemodynamics.
The findings from this study should be interpreted in the context of following limitations. First, the sample size was relatively small and potential group differences in the baseline hemodynamics may influence study outcome measures (Table 2), though it was designed as a proof-of-concept study. Also, the attrition rate was relatively high (∼31%) and MRI measurements were performed only in a subset of participants, which may bias our results. Therefore, our findings need to be confirmed in future studies with lager sample size Second, although we observed that AET improved the D-KEFS letter fluency test score when compared to SAT, this change was minimal, which may limit clinical relevance of our findings. Third, the finding of the present study and its potential implication for AD should be interpreted in a clinical context since neuroimaging biomarkers of AD pathology (such as brain amyloid and tau) were not used to define MCI due to AD in the present study [51]. Finally, we must acknowledge that the findings of the present study were obtained mainly from white caucasian individuals and future studies in racially and ethnically diversified populations are needed to confirm the findings of this study. This is particularly important in AD due to existing ethnoracial disparities in AD prevalence and access to healthcare [22].
CONCLUSIONS
In patients with amnestic MCI, this study demonstrated that 1) one-year moderate-to-vigorous AET increased global CBF and reduced central arterial stiffness and arterial pulsation when compared with SAT; 2) the positive association between changes in cardiorespiratory fitness and CBF was mediated by the reductions in carotid stiffness and CBF pulsatility; and 3) AET was associated with slightly improved cognitive performance as measured by the D-KEFS letter fluency score which was associated with reduction in central arterial stiffness measured by cfPWV. These findings provide evidence that aerobic exercise reduces central arterial stiffness and increases CBF in patients with amnestic MCI which may benefits cognitive performance.
Clinical perspectives
At present, there are no effective treatment strategies to prevent or slow age-related cognitive decline or AD [22]. Mounting evidence indicates that elevated central arterial stiffness and reduced CBF are risk factors for age-related cognitive decline and AD [1–6]. In this regard, AET may improve brain structure and function by reducing vascular risk factors [20]. In this study of patients with amnestic MCI, one-year AET increased physical fitness, reduced carotid arterial stiffness, and improved global CBF, while its effects on cognitive performance were minimal when compared to the SAT control intervention. These findings demonstrated the benefits of AET on reducing vascular risk factors in older adults who have high risks of AD and suggest that these benefits may precede improvement in neurocognitive function.