
Abstract
Background:
Vascular disease is a risk factor for Alzheimer’s disease (AD) and related dementia in older adults. Retinal artery/vein occlusion (RAVO) is an ophthalmic complication of systemic vascular pathology. Whether there are associations between RAVO and dementia risk is unknown.
Objective:
To determine whether RAVOs are associated with an increased risk of developing vascular dementia or AD.
Methods:
Data from Adult Changes in Thought (ACT) study participants were analyzed. This prospective, population-based cohort study followed older adults (age ≥65 years) who were dementia-free at enrollment for development of vascular dementia or AD based on research criteria. RAVO diagnoses were extracted from electronic medical records. Cox-regression survival analyses were stratified by APOE ɛ4 genotype and adjusted for demographic and clinical factors.
Results:
On review of 41,216 person-years (4,743 participants), 266 (5.6%) experienced RAVO. APOE ɛ4 carriers who developed RAVO had greater than four-fold higher risk for developing vascular dementia (Hazard Ratio [HR] 4.54, 95% Confidence Interval [CI] 1.86, 11.10, p = 0.001). When including other cerebrovascular disease (history of carotid endarterectomy or transient ischemic attack) in the model, the risk was three-fold higher (HR 3.06, 95% CI 1.23, 7.62). No other conditions evaluated in the secondary analyses were found to confound this relationship. There was no effect in non-APOE ɛ4 carriers (HR 1.03, 95% CI 0.37, 2.80). There were no significant associations between RAVO and AD in either APOE group.
Conclusion:
Older dementia-free patients who present with RAVO and carry the APOE ɛ4 allele appear to be at higher risk for vascular dementia.
Keywords
INTRODUCTION
Dementia affects an estimated 50 million people worldwide, with 10 million new cases per year [1], and is a leading cause of death globally [2]. Alzheimer’s disease (AD) dementia is the most common type of dementia accounting for approximately 60% of all dementia, followed by vascular dementia causing an estimated 20% of cases [3], and other less common types of dementia, such as dementia with Lewy bodies and frontotemporal dementia. The etiologies of the various types of dementia are complex and perhaps interconnected. Though the presence of specific neuropathological changes (amyloid-β [Aβ] and hyperphosphorylated tau [p-tau] tangles) is considered the definitive pathophysiologic mechanism of AD, vascular pathology has been shown to be an important independent risk factor for AD and related dementias [4]. Several studies have shown associations between vascular disease and decreased cognitive function and AD dementia [5, 6]. Even the most common condition, AD is usually accompanied by other neurodegenerative changes, especially in older adults, who constitute the bulk of people with dementia [7, 8].
Retinal vein/artery occlusion (RAVO), commonly referred to as retinal vascular occlusion, is the second most common retinal vascular disorder after diabetic retinopathy and affects an estimated 16 million people worldwide [9]. Like dementia, the incidence of RAVO increases with age. Retinal vein occlusion is more common than retinal artery occlusion, but both share common risk factors including hypertension and vascular disease. Both RAVO in general and retinal artery occlusion in particular are associated with a higher risk for stroke and myocardial infarction [10], which are both risk factors for vascular dementia [11].
The retina is an extension of the central nervous system, and retinal ganglion cells (RGCs), whose axons make up the optic nerve, are neuronal cells that transmit visual information to the brain. Certain retinal disorders have pathological features that overlap with AD specifically, including neurodegeneration and accumulation of Aβ and p-tau, while microvascular abnormalities in the retina have been associated with stroke [12]. We previously reported associations between AD dementia and age-related macular degeneration (AMD), glaucoma, and dia-betic retinopathy (DR) using data from Adult Ch-anges in Thought (ACT), a large, prospective, population-based cohort study [13, 14]. We hypothesized that shared physiological pathways may exist between these eye conditions and AD, providing potential clues into the etiology of AD and related dementias [13]. In this study, we investigated whether RAVOs are similarly associated with increased risks of developing vascular dementia or AD.
METHODS
Study population
Detailed study methods have been published previously [14, 15]. In brief, the Adult Changes in Thought (ACT) is a population-based, prospective cohort study of participants ≥65 years recruited from Kaiser Permanente Washington (KPW) membership rolls who are dementia-free at enrollment and are followed until development of any dementia [14]. Participants receive APOE genotyping at recruitment. At screening and each biennial visit [15, 16], participants receive cognitive screening tests and medical history and risk factor evaluations. KPW is an established Washington state health care delivery system. Comprehensive ophthalmic care was provided for all members, and care was not related to ACT enrollment or any study findings. This study was approved by the Institutional Review Boards of KPW and the University of Washington and conducted in accordance with the Declaration of Helsinki. All participants gave informed written consent. This report is based on the 2018 ACT data freeze.
Vascular dementia and AD evaluation
Participants were screened biennially with the Cognitive Abilities Screening Instrument (CASI), which ranges from 0–100 with higher scores indicating better cognition [17]. Participants with CASI scores ≤85 underwent a standardized diagnostic evaluation, including physical and neurologic examinations and a neuropsychological test battery [18]. Dementia diagnoses and vascular dementia diagnoses were determined at consensus conferences using Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) criteria [19], and probable and possible AD dementia diagnoses were determined using the National Institute of Neurological and Communicative Disorders and Stroke - Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria [20]. Our primary outcome was the development of vascular dementia and secondary outcomes as development of AD.
Study variable description
The diagnosis of RAVO was defined as a history of occlusion of a retinal artery or vein. The diagnosis of RAVO was extracted from diagnostic codes available in participants’ electronic records, which were available from 1993 (1 year prior to the first enrollment date of the original ACT cohort). RAVO diagnosis was based on the following International Classification of Diseases (ICD)-9-Clinical Modification (CM) and ICD-10-CM codes. Codes for RAVO included 362.30, 362.31, 362.32, 362.33, 362.35, 362.36, 362.37, and H34.1-H34.9999.
The following variables were based on enrollment and biennial self-reported medical history: smoking, hypertension, congestive heart failure, diabetes, coronary artery disease defined as any history of myocardial infarction, angina, coronary artery bypass grafting, or angioplasty, and cerebrovascular disease defined as any history of strokes, carotid endarterectomy, or transient ischemic attacks. The following ophthalmic covariates were based on ICD-9-CM and ICD-10-CM codes: glaucoma, DR, and AMD (Supplementary Table 1). We generated a “coronary artery disease” variable based on any myocardial infarction, angina, coronary artery bypass grafting, or angioplasty. Because strokes are directly related to the diagnosis of vascular dementia, we excluded strokes from the list of potential confounders for analyses of all dementia outcomes. We generated an “other cerebrovascular disease” variable based on a history of either carotid endarterectomy or transient ischemic attack and included this variable in the extended models.
Statistical analyses
The outcomes of vascular dementia and probable or possible AD were analyzed using Cox proportional hazards models. Age was the time axis. Censoring occurred at data freeze, death, or loss to follow-up, and, for the vascular dementia or AD outcome, diagnosis of other dementia. All models were stratified by any APOE ɛ4 allele status and adjusted for sex, self-reported non-Hispanic White race, education noted as with or without 4 years of additional education post high school, and smoking history. We refer to this primary model as the demographic covariates adjusted model. After the stratification by APOE genotype, model assumptions were tenable.
Secondary analyses
Demographic and clinical covariates adjusted models
The following were included in sensitivity analyses as potential confounders of the association between RAVO and dementia outcomes: diabetes, hypertension, congestive heart failure, smoking history, coronary artery disease, and other cerebro-vascular disease (excluding stroke). Only the covariates that changed the coefficient of RAVO noted from the demographic covariates adjusted model by greater than 10% were included in the demographic and clinical covariates adjusted models.
Eye disease adjusted models
Glaucoma, AMD, and DR were assessed as potential confounders of the association between RAVO and dementia outcomes in both the demographic covariates only models and the demographic and clinical covariates adjusted models.
RESULTS
Study population, RAVO
Data from 5,546 ACT participants were available. A total of 4,743 participants with follow-up data were included in the dataset (total person-years 41,216; average 8.7 years/person). A total of 58.6% of the cohort was female and the average age at baseline was 74.5 years. Of all participants, 89% were white, 3.6% Black, 3.5% Asian, 0.19% American Indian or Alaskan Native, and 3.12% were other. A total of 4,166 had APOE genotype data, of which 1,102 participants (26%) had at least 1 APOE ɛ4 allele. A total of 754 participants (16.0%) reported having diabetes, 2,830 (60%) reported having hypertension and 1,282 (27%) had a history of coronary artery disease (Table 1).
Demographic and health variables at baseline, stratified by retinal artery/vein occlusion (RAVO) diagnosis
Coronary artery disease: history of prevalent myocardial infarction, coronary artery bypass grafting, or angioplasty; other cerebrovascular disease: history of history of carotid endarterectomy or transient ischemic attack; SD, standard deviation.
There were 1,270 cases of any dementia during the follow-up period, including 1,034 incident cases of AD and 117 incident cases of vascular dementia. All diagnoses of RAVO occurred prior to incident dementia. A total of 266 participants had a diagnosis of RAVO before censoring (Fig. 1).

Diagram of study participant selection. ACT, Adult Changes in Thought study; RAVO, retinal artery/vein occlusion; AD, Alzheimer’s disease dementia.
Risks of vascular dementia and AD
Demographic covariates adjusted models
A) Vascular dementia outcome. Participants who were APOE ɛ4 carriers and had RAVO had a greater than four-fold higher risk for developing vascular dementia (Hazard Ratio [HR] 4.54, 95% Confidence Interval [CI] 1.86, 11.10, p = 0.001) compared to APOE ɛ4 carriers who did not have RAVO (Table 2, Fig. 2). There was no association between RAVO and vascular dementia in the non-APOE ɛ4 carrier group (HR 1.03, 95% CI 0.37, 2.80).
Hazard ratios (HR) and 95% confidence intervals (CI) for the association of retinal vascular occlusions and dementia (vascular dementia and Alzheimer’s disease [AD] dementia). Age was the time axis. The demographic covariates adjusted models are adjusted for sex, education, self-reported non-Hispanic White race, and smoking history. For the demographic and clinical covariates adjusted models, the following additional variables were evaluated: diabetes, hypertension, congestive heart failure, cardiovascular disease and other cerebrovascular disease and only the covariates that impacted the results of the demographic covariates adjusted model by greater than 10% were added: other cerebrovascular disease1, diabetes2, congestive heart failure3
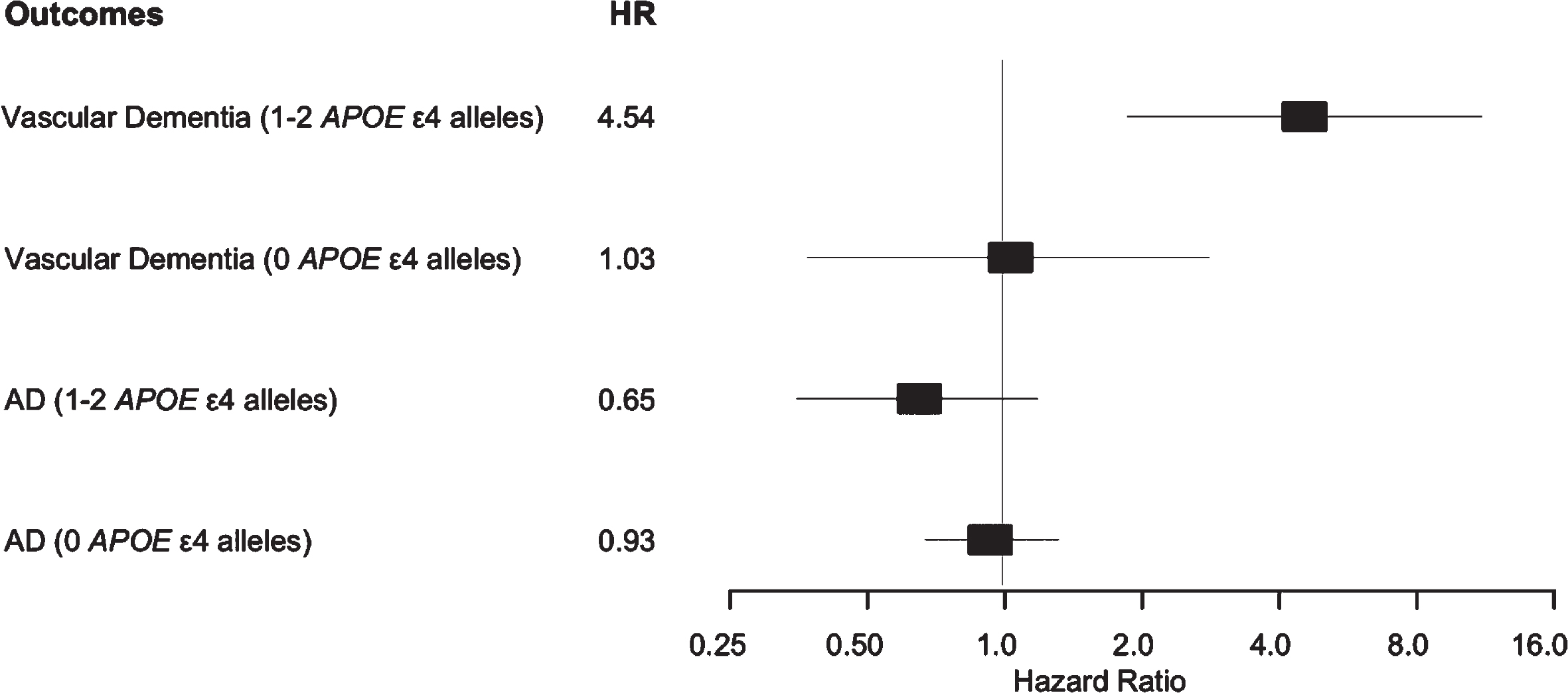
Forest plots showing hazard ratios (HR) and 95% confidence intervals for six independent models of associations of retinal artery/vein occlusions (RAVOs) and dementia (vascular dementia and Alzheimer’s disease [AD] dementia) stratified by APOE ɛ4 status. All models were adjusted for sex, education, Self-reported non-Hispanic White race, and smoking history.
B) AD outcome. There were no significant associations between RAVO and AD in either APOE group (Table 2, Fig. 2).
Secondary analyses
Demographic and clinical covariates adjusted models
A) Vascular dementia outcome. The only vascular risk factor that impacted the RAVO coefficient by more than 10% in the demographic covariates adjusted model was other cerebrovascular disease. The association between RAVO and vascular dementia among people with at least one APOE ɛ4 allele remained significant after controlling for other cerebrovascular disease (HR 3.06, 95% CI 1.23, 7.62, p = 0.016). None of the other conditions evaluated in secondary analyses were found to confound this relationship. Results from the full model are shown in Supplementary Table 2.
B) AD outcome. There were still no significant associations between RAVO and AD in either the group with at least one APOE ɛ4 allele or the group with no APOE ɛ4 alleles after adding additional covariates that affected the RAVO coefficient by more than 10% (Supplementary Table 3).
Eye disease adjusted models
Adjusting for AMD, DR, and glaucoma, the risk of vascular dementia associated with RAVO among people with at least one APOE ɛ4 allele was very similar in the demographic covariates adjusted model (HR 4.14, 95% CI 1.58, 10.84, p = 0.004). Including terms for the eye diseases in the model that included other cerebrovascular disease led to an attenuated but still significantly elevated risk of vascular dementia associated with RAVO (HR 2.77, 95% CI 1.05, 7.36, p = 0.04) (Supplementary Table 4). We did not perform analogous analyses for the AD dementia outcome since there were no associations between RAVO and AD.
DISCUSSION
On an analysis of 4,166 participants with 41,216 person-years of follow-up, we found that RAVO is significantly associated with vascular dementia among people with at least one APOE ɛ4 allele, but there was no association of RAVO with AD dementia among people with or without an APOE ɛ4 allele. These findings were not impacted by adjustment for demographic characteristics, clinical characteristics, or other eye conditions.
Our study considered people with a history of either retinal vein occlusion or retinal artery occlusion. Retinal vein occlusion is typically caused by localized thrombus formation in the retinal vein, often due to compression from a thickened retinal artery within the shared adventitia, when atherosclerosis is present. In contrast, retinal artery occlusion is usually caused by an embolism originating elsewhere in the body, such as from the carotid or coronary arteries, or a heart valve [21]. Many of the systemic risk factors for RAVO (age, hypertension, diabetes mellitus, obesity, hyperlipidemia, cigarette smoking, hypercoagulable states) [22, 23] are also risk factors for stroke and cardiovascular disease, suggesting that people with RAVO may be at higher risk for stroke or myocardial infarction [10]. Stroke is an established risk factor for dementia; a 2018 meta-analysis reported that an incident stroke doubles the risk for any dementia in older adults [24]. Given stroke is a strong risk factor for vascular dementia, we excluded self-reported history of stroke as a covariate in our model. Non-stroke cardiovascular disease, especially peripheral artery disease, has also been associated with AD and dementia [25, 26].
Although vascular disease and mixed-type dementia (both AD and vascular dementia) are increasingly considered to be independent but convergent disease processes [5, 27], few studies have investigated RAVO and risk for dementia. Several studies have reported associations between RAVO and cerebrovascular disease. One study assessed retinal vein occlusion as a marker of premature brain aging, comparing MRI findings of 125 people with retinal vein occlusion to age-matched people without retinal vein occlusion and finding a higher prevalence of cerebral small vessel disease in the retinal vein occlusion group. This finding was most notable in the youngest group (38% [15/39] of those with a retinal vein occlusion who were younger than age 60 versus 4% [47/1105] in people without a retinal vein occlusion who were younger than age 60, p < 0.001). The suggested mechanism is that the retinal artery may be undergoing the same disease process as the cerebral vessels and compressing the retinal vein, so retinal vein occlusion may act as a marker for cerebrovascular disease [28]. Patients with non-embolic branch retinal artery occlusion have a higher prevalence of cerebrovascular disease [29], and the Rotterdam study found an association between wider retinal venules and vascular dementia [30]. Structural differences in the retinal vasculature, including differences in vessel stiffness similar to differences associated with RAVO, have been associated with higher neocortical Aβ scores, which are relevant in AD [31]. Other differences in the microvasculature of the retina (sparser vasculature with decreased retinal fractal dimensions) have been noted in people with AD compared to cognitively normal elderly controls, and it is postulated that these differences may reflect similar differences in the cerebral microvasculature associated with AD [32, 33]. We also included AMD, DR, and glaucoma as potential confounders that were chosen a priori because we had previously shown that these diseases are associated with increased risk for both AD and all-cause dementia, which includes vascular dementia [13]. The association between RAVO and vascular dementia still remained significant after controlling for these conditions. Interestingly, we did not find any association between RAVO and AD and this may have been due to different study populations or methods.
A recent study evaluated the association between retinal vein occlusion and dementia risk using data from the South Korean National Health Insurance Service [34]. This retrospective study evaluated 46,259 people with retinal vein occlusion and matched controls over a follow-up period of 6.6 years and found that retinal vein occlusion was associated with an increased risk of all cause dementia diagnoses based on ICD-10-CM codes (HR, 1.16; 95% CI, 1.12–1.21), AD (HR, 1.15; 95% CI, 1.11–1.20), and vascular dementia (HR, 1.24; 95% CI, 1.12–1.37). The risk of dementia was found in patients with and without hypertension, though the combination of retinal vein occlusion and hypertension was associated with a higher risk for vascular dementia (HR 1.88; 95% CI: 1.63–2.18). These results differ from our study in that we found a stronger association between RAVO and vascular dementia determined using a prospective design with consensus conference-based research criteria among people with at least one APOE ɛ4 allele but did not find any association between RAVO and AD. Unlike our study, this study relied on diagnostic codes from a national insurance database to identify dementia cases, which may have led to imprecision due to unrecognized cases and/or misclassification by dementia type such as AD or vascular dementia. The authors only evaluated retinal vein occlusion and not retinal artery occlusion. Similar to our results, the South Korean study found that the associations between retinal vein occlusion and dementia risk persisted when controlling for risk factors such as diabetes, hypertension, and smoking history. A key difference in our study was the availability of APOE genotype data from ACT participants which allowed us to detect an APOE ɛ4 specific association between RAVO and vascular dementia.
We found a strong association between RAVO and vascular dementia among people with at least one APOE ɛ4 allele in our study. The fact that this association was only noted among people with at least one APOE ɛ4 allele was unexpected. We chose to stratify by APOE genotype because proportional hazards assumptions were found to be untenable. APOE ɛ4 is a strong genetic risk factor for late onset AD. The prevalence of the APOE ɛ4 allele in our study is comparable to what is known in the literature; prevalence varies significantly by ethnicity, and studies have found prevalence rates ranging from as low as 5% to as high as 40% [35–37]. The APOE protein is involved with lipid transport and cholesterol regulation [38]. People with at least one APOE ɛ4 allele have a higher risk for atherosclerosis and higher levels of low-density lipoproteins (LDL) in plasma [39] and have been shown to be at higher risk for ischemic cerebrovascular disease [40, 41]. People with at least one APOE ɛ4 allele are also at higher risk of RAVO, suggesting that APOE genotype may play a role in retinal microvascular disease [42], although other studies have reported inconsistent findings about the relationship between APOE genotype and retinopathy [43, 44]. Our finding that only APOE ɛ4 carriers with RAVO had increased risk of vascular dementia while APOE ɛ4 carriers without RAVO did not have any increased risk suggests a specific relationship between APOE ɛ4, RAVO, and vascular dementia. APOE-related retinal microvascular dysfunction may play a role in the pathogenesis of vascular dementia. Another possibility is that RAVO events may be markers of more severe generalized APOE-related microvascular disease, resulting in vascular dementia. Mouse models have demonstrated variations in the phenotypic expression of APOE ɛ4 [45], and it is possible that the degree of APOE-related microvascular dysfunction varies among individuals with this allele. We considered that there might be a stronger association between RAVO and vascular dementia in people who had two APOE ɛ4 alleles compared to those who had one APOE ɛ4 allele; however, we did not have sufficient power to assess a dose-dependent effect.
Our study has several limitations. Despite the large number of study participants, RAVO and vascular dementia are both relatively infrequent, although the prevalence of RAVO was higher than we had expected based on current literature, possibly due to the large number of very old participants (age > 85 years) in the ACT cohort [9, 46]. The retinal diagnoses of retinal vein occlusion or retinal artery occlusion were based on ICD-9-CM and ICD-10-CM codes rather than by clinical examination and we were not able to distinguish between retinal vein occlusion and retinal artery occlusion based on the ICD-9-CM and ICD-10-CM codes as many of them were coded as unspecified. As many of these records predate the era of electronic health records, the review of individual charts was outside the scope of this study. Additionally, we were unable to analyze the retinal vein and artery occlusions separately due to our limited sample size; there were 7 cases of retinal vein occlusion and 8 cases of retinal artery occlusion in the APOE ɛ4 positive group. Retinal vein and retinal artery occlusions have different pathologic mechanisms, but both etiologies are associated with vascular disease and thus may be related to dementia risk. We therefore combined them into an overarching RAVO indicator and found a novel relationship that suggests an important role of APOE ɛ4 in the associations between RAVO and vascular dementia. RAVO, especially RAO, is a relatively infrequent event, and additional analysis of the individual associations between RVO and RAO in a larger study with sufficient cases for comparison is warranted. One concern may be the possibility of underdiagnosis of RAVO in participants who were not seen by eye care providers. However, our previous analysis found that 98.6% of the entire ACT study cohort was seen at least once by eye care providers in our system and an average of 26.7 times during their membership in KPW [13]. Importantly, our cohort is well-characterized in terms of dementia diagnosis, as the study includes prospective case identification and research criteria for the diagnosis of dementia and dementia subtype based on consensus conference consideration of all relevant data [19, 20]. This allowed us to better distinguish between vascular dementia and AD dementia, which have different but possibly convergent etiologies. We also enrolled people who were dementia-free and followed them prospectively over a long period of time (> 41,000 person-years), during which we identified over 1,100 incident cases of dementia. The number of people with RAVO in our data was insufficient for formal mediation analysis to evaluate the role of systemic vascular risk factors in the association between RAVO and vascular dementia, which would be important in future studies. In addition, the ACT population is predominantly white and the low number of other races limited our ability to perform a meaningful analysis of outcomes by race.
Unlike AMD, glaucoma, and DR, which are neuro-degenerative ophthalmic diseases that showed positive associations with AD in our previous study [11], we did not find an association between RAVO and vascular dementia or AD, except in the group of people with vascular dementia at least one APOE ɛ4 allele. The relationship between RAVO and vascular dementia risk among people with at least one APOE ɛ4 allele remained significant after we controlled for demographic factors, systemic vascular risk factors, and confounding neurodegenerative ophthalmic diseases. Our results suggest that older dementia-free individuals who present with RAVO may be at risk for developing vascular dementia, particularly if they have at least one APOE ɛ4 allele. These individuals may also be at risk for other vascular diseases, even if they do not already have known risk factors. Further studies are needed to investigate the relationship between retinal vascular changes, APOE genotype, vascular dementia, and AD.
Footnotes
AcknowledGMENTS
We thank Michael Brush, MD, and Michael Lee, MD, for their generous assistance with analyses of ophthalmic data from Kaiser Permanente Washington.
This work is supported by the NIH/NEI K23EY029246, NIH/NIA R01AG060942, NIH/NIP50 AG05136, and NIH/NIA U01AG006781, Latham Vision Innovation Award, and by an unrestricted grant from Research to Prevent Blindness. The sponsors / funding organizations had no role in the design or conduct of this research.