
Abstract
Background:
Lewy-related pathology (LRP), primarily comprised of α-synuclein, is a typical neuropathological change that has been identified in many neurodegenerative disorders such as Parkinson’s disease (PD), PD with dementia, and dementia with Lewy bodies.
Objective:
To investigate the distribution of LRP in the China Human Brain Bank, the co-occurrence of neuropathologic features of Alzheimer’s disease (AD) in LRP cases, and LRP-related cognitive dysfunction.
Methods:
LRP neuropathological diagnosis was performed in 180 postmortem brains. AD neuropathological diagnosis was then performed in the 21 neuropathologically-diagnosed LRP cases. Antemortem cognitive functioning evaluation (Everyday Cognitive, ECog) was assessed for brain donors by the immediate kin of the donor within 24 hours after death.
Results:
12% (21 in 180) postmortem brains were neuropathologically diagnosed as LRP cases. 86% (18 in 21) aged above 80, 81% (17 in 21) LRP cases combined with AD neuropathology, and 62% (13 in 21) combined with both the intermediate or high-level amyloid-β and phospho-tau pathologies. ECog scores showed significant differences between the groups of LRP brainstem-predominant type and LRP diffuse neocortical type, and between groups of AD and the combined LRP (diffuse neocortical type)-AD.
Conclusion:
The overlap of neocortical α-synuclein, amyloid-β, phospho-tau, and neuritic plaques in LRP suggested the potential interplay among the common characteristics of proteinopathies in the late stage of neuropathological development of LRP in human brains. The anatomic progression of LRP, the process of α-synuclein spreading from the brainstem to limbic and neocortical regions, might aggravate the deterioration of cognitive function in addition to that effect of AD.
Keywords
INTRODUCTION
In 1912, Frederick Lewy first described the abnormal intracytoplasm inclusions now known as Lewy bodies in a patient with what is now called Parkinson’s disease (PD) [1]. Lewy-related pathology (LRP) is characterized by α-synuclein that accumul-ates in cell bodies as Lewy bodies and in cell processes as Lewy neurites [2]. According to the Braak Stage, the deposition of α-synuclein in human brains follows a temporal pattern that first appears in the brainstem regions, and then gradually transfers to the limbic then diffuses to neocortical regions [3]. The Lewy body-related pathology is observed in dementia with Lewy bodies (DLB), idiopathic PD, PD with dementia, and multiple system atrophy [4]. Lewy bo-dies are a common neuropathologic finding in dementia, second to Alzheimer’s disease (AD) [4]. AD is the most prevalent age-related neurodegenerative disorder and its neuropathologic changes are characterized by the accumulation of amyloid-β (Aβ) plaques and tau-laden neurofibrillary tangles [5]. Interestingly, former studies found several AD cases exhibit significant α-synuclein aggregation in addition to Aβ plaques and neurofibrillary tangles [6]. Specifically, 40–60% AD cases display Lewy bodies that are most frequently localized to the amygdala [6–8]. That co-existence of Aβ plaques, phospho-tau, and α-syn-uclein in AD cases suggests Aβ plaques and phospho-tau might also be found in LRP cases, which has been confirmed by a longitudinal clinicopathologic study of aging and neurodegenerative disease, showing co-morbid AD in PD with dementia patients [9].
The neuropathologic comorbidities of LRP and AD will make the diagnosis of neurodegenerative diseases, pharmacologic treatments, and the development of novel therapeutics targeting proteinopathy difficult. Moreover, although China has been reported as facing an enormous challenge and disease burden of dementia, available information about LRP in China remains limited [10]. Particularly, few neurop-athological studies have been done in human LRP brains to check the presence and the level of Aβ and phospho-Ttau pathologies, as well as the impact of LRP on the cognitive dysfunction in the Chinese population. Hence, the knowledge gap may exist considering the under-recognized LRP cases and neuropathologic comorbidities. Furthermore, the risk factors underlying the pathogenesis of neurodegenerative diseases in China might be different from other countries of the world.
In this study, we want to investigate 1) the distribution and neuropathological change of LRP in the China Human Brain Bank, 2) the distribution and neuropathologic change of Aβ deposits, phospho-tau, and neuritic plaques in the neuropathologically identified LRP cases, and 3) the contribution of LRP in daily cognitive dysfunction, and in the daily cognitive dysfunction of the combined LRP-AD neuropat-hology.
MATERIALS AND METHODS
Human brain tissue samples
Postmortem human brain tissues (midbrain, pons, medulla, amygdala, cingulate, hippocampus, parie-tal, temporal, frontal cortex) were obtained from the National Human Brain Bank for Development and Function (http://anatomy.sbm.pumc.edu.cn/brainbank), located at Chinese Academy of Medical Sciences (CAMS)/Peking Union Medical College (PUMC) in Beijing, China, with written consents from both the brain donors and their next-of-kin. The brain tissue collection protocols were approved by the Instituti-onal Review Board of the Institute of Basic Medical Sciences of the CAMS/PUMC, Beijing, China (approval number: 009-2014), and a detailed proto-col describing the collection and processing of brain tissues was previously published [11]. The postmortem delay of brain tissues were within 24 hours. All samples were obtained in agreement with ethical standards and legislation defined by CAMS/PUMC.
Immunohistochemistry and neuropathological diagnosis
The optimized immunohistochemistry staining procedure for α-synuclein can be briefly summarized as: Formalin-fixed tissues are deparaffinized in xylenes, brought to distilled water through graded alcohols and treated with 1:100 proteinase K. After washing three times in 0.1 M PBS, tissues are im-mersed for 30 min in 1% hydrogen peroxide in 0.1 M PBS. Tissues are then washed three times in 0.1 M PBS and incubated at 4°C overnight in sheep antibody to α-synuclein (Biosensis, S-024-100) at 1:1000 dilution. After washing in PBS, tissues are incubated for 2 h at room temperature in biotinylated anti-sheep IgG (Vectastain BA-6000) diluted 1:500. After washing in PBS, slides are treated for 30 min with ABC (Vectastain PK-4000), with A and B components of the kit both at 1:1000 dilution. After three washes in PBS, slides are treated with DAB (5 mg/100 ml). Tissue are then washed in distilled water and counterstained with hematoxylin. Then slides are taken through 75% alcohol, 80%, 95%, 100% and into xylenes to be coverslipped.
The neuropathological assessment of LRP was conducted according to the Diagnosis and Management of Dementia with Lewy Bodies - Third Report of the DLB Consortium, and being tailored to the China Human Brain Bank for use in practice (Table 2) [12]. The pathologically diagnosed LRP type was classified into three categories (brainstem, limbic, neocortical) based upon the anatomic progression of α-synuclein [3]. In LRP diagnostic procedure, we selected the midbrain, pons, and medulla as the brainstem region; amygdala, cingulate, and hippocampus as the translational/limbic region; parietal, temporal, and frontal as the diffuse neocortical region (Table 1) [12]. Compared with the Third Report of the DLB Consortium criteria, we selected the hippocampus, rather than nucleus basalis and transentorhinal, as the translational/limbic region. In this study, the pathologically diagnosed LRP cases were classified based on our adapted LRP pathological diagnosis criteria but would also be able to get the same classification results from the Third Report of the DLB Consortium (Table 2) [12].
Neuropathological and Clinical Distribution of LRP in Postmortem Human Brains. The clinical diagnosis of LRP was made by neurologists in either PUMC hospital or other comprehensive hospitals in Beijing
0 = none; 1 = mild (sparse Lewy bodies (LBs) or Lewy neurites (LNs)); 2 = moderate (more than 1 LB per low-power field and sparse LNs); 3 = severe (4 or more LBs and scattered LNs per low-power field). PTB, postmortem brains; M, male; F, female; N, no; Y, yes; B, brainstem-predominant; T, transitional or limbic; D, diffuse neocortical; Mid, midbrain; Med, medulla; Amy, amygdala; Cing, cingulate; Hip, hippocampus; Par, parietal; Tem, temporal; Fro, frontal.
Diagnosis and management of dementia with Lewy bodies - Third report of the DLB consortium [12]
0 = none; 1 = mild (sparse Lewy bodies (LBs) or Lewy neurites (LNs)); 2 = moderate (more than 1 LB per low-power field and sparse LNs); 3 = severe (4 or more LBs and scattered LNs per low-power field). Mid, midbrain; Med, medulla; Amy, amygdala; Cing, cingulate; Hip, hippocampus; Par, parietal; Tem, temporal; Fro, frontal.
The neuropathological assessment of AD was conducted according to the National Institute on Aging–Alzheimer’s Association criteria and a det-ailed description was previously reported [13, 14]. Multiple AD neuropathological characteristics were examined in the pathological diagnosis, including Aβ deposits, neurofibrillary tangles (phosphorylated tau), and neuritic plaques. According to the Braak staging scheme, the accumulation of Aβ deposits and neurofibrillary tangles follows distinct regional progressions across brain regions as AD advances [15, 16]. Based on the neuropathologic advance level, the pathological staging of Aβ deposits (A Score), neurofibrillary tangles (B Score), and neuritic plaques (C Score) are adapted to the four-point score scale [13]. The score (0, 1, 2, 3) of each neuropathology feature represents its neuropathologic accumulation/aggregation level [13]. The combina-tion of A, B, and C scores is designated as “Not”, “Low”, “Intermediate”, or “High” AD neuropathologic change; the “Intermediate” or “High” AD neuropathologic change is considered sufficient explanation for dementia [13].
Everyday Cognitive (ECog) function evaluation
The ECog is an informant-rated questionnaire evaluation comprised of multiple subscales (memory, language, visuospatial abilities, planning, organiza-tion, and attention) for the early detection and systematic characterization of daily cognitive dysfunction [17]. That systematic assessment of daily cognitive function provides more information in understanding the determinants of functional impairment and may guide the development of new interventions in the elderly [17]. In this way, the estimation of an individual’s ability to cognitive function in daily life is an important aspect of neuropsychological and neurodegenerative evaluation [17].
The ECog questionnaire was performed to generate and assess the antemortem cognitive functioning evaluation of the neuropathologically diagnosed LRP cases in our study. All ECog evaluations were conducted within 24 h after death by in-person or phone interview with immediate kin of the brain donor. The global ECog score represented the average functional level considering all the cognitive subscales and would be marked as “unknown” if the immediate kin of the brain donor cannot recall or respond. In accordance with the criteria, the ECog scores can be categorized into three groups: cognitive normal (ECog score <1.0), mild cognitive impairment (ECog score between 1.0 and 2.0), and dementia (ECog score >2.0) [14, 17].
Statistical analysis
Results were expressed as mean±the standard error of the mean (SEM), with all of the original data displayed. The two-tailed unpaired t test was used to detect age differences between groups. Comparisons of the global ECog scores between groups were performed using Kruskal-Wallis test and Steel-Dwass-Critchlow-Fligner test. p < 0.05 was considered statistically significant. The controlling of false discovery rate (FDR) in multiple comparisons was performed by the Benjamini-Hochberg procedure. All statistical analysis was conducted using Statistical Analysis Software (SAS Studio) and Graphpad Prism 7.
RESULTS
21 neuropathological diagnosed LRP cases in 180 postmortem human brains
Among all the collected postmortem human brains at the China Human Brain Bank, 180 were fully qualified for conducting the neuropathological diagnosis of LRP, and we altogether identified 21 neuropathologically diagnosed LRP cases (Table 1). Based on the neuropathological criteria for LRP postmortem diagnosis, we found 15 cases of LRP brainstem-predominant type, 3 cases of LRP transitional/limbic type, and 3 cases of LRP diffuse neocortical type (Table 2) [12].
86% neuropathologically diagnosed LRP cases aged above eighty
Aging is acknowledged as one of the important risk factors in the development of neurodegenerative diseases. According to the age of death, we grouped the postmortem brain samples into four categories: younger than 70 (none), 70 to 79 (n = 3), 80 to 89 (n =10), and above 90 (n = 8). We found 100% of the neuropathologically diagnosed LRP cases aged above 70 and 86% (18/21) cases aged above 80 (Table 3). The average age of 21 neuropathologically diagnosed LRP cases was 88.
Demographic Distribution of 21 Neuropathologically Diagnosed LRP Cases. Results were displayed as the number of cases
Besides, we analyzed the distribution of sex differences in LRP diagnosis. In 180 brain donors, 101 (56%) cases were male, and 79 (44%) were female. In 21 neuropathologically diagnosed LRP cases, 12 (57%) were male, and 9 (43%) were female. We found that 47% (7/15) brainstem-predominant type cases were male, 100% (3/3) transitional/limbic type cases were male, and 67% (2/3) diffuse neocortical type cases were male (Table 3). Overall, in the middle and late stages (limbic and neocortical regions) of LRP anatomic progression, 83% (5/6) cases were male; in the early stage (brainstem regions) of LRP anatomic progression, 47% (7/15) cases were male.
81% neuropathologically diagnosed LRP cases with concomitant AD neuropathologic changes
We investigated the AD neuropathologic changes in the 21 neuropathologically diagnosed LRP cases and our findings showed 17 (81%) LRP cases combined with AD neuropathology (Table 4). In the study, we identified 4 (19%) LRP cases without AD neu-ropathology, 3 (14%) with low-level AD neuropathology, 10 (48%) with intermediate-level AD neuropathology, and 4 (19%) with high-level AD neuropathology (Table 4). According to the National Institute on Aging-Alzheimer’s Association guidelines for AD, the intermediate or high-level AD neuropathologic change is considered sufficient explanation for dementia and thus considered as the criteria for AD neuropathological diagnosis [13]. Among 14 LRP cases with the intermediate or high-level AD neuropathology (LRP-AD), 9 (64%) LRP-AD cases were LRP brainstem-predominant type, 2 (14%) were LRP transitional/limbic type, and 3 (22%) were LRP diffuse neocortical type (Table 4).
AD Neuropathological Distribution and Change in 21 Neuropathologically Diagnosed LRP Cases. Results were displayed as the number of cases
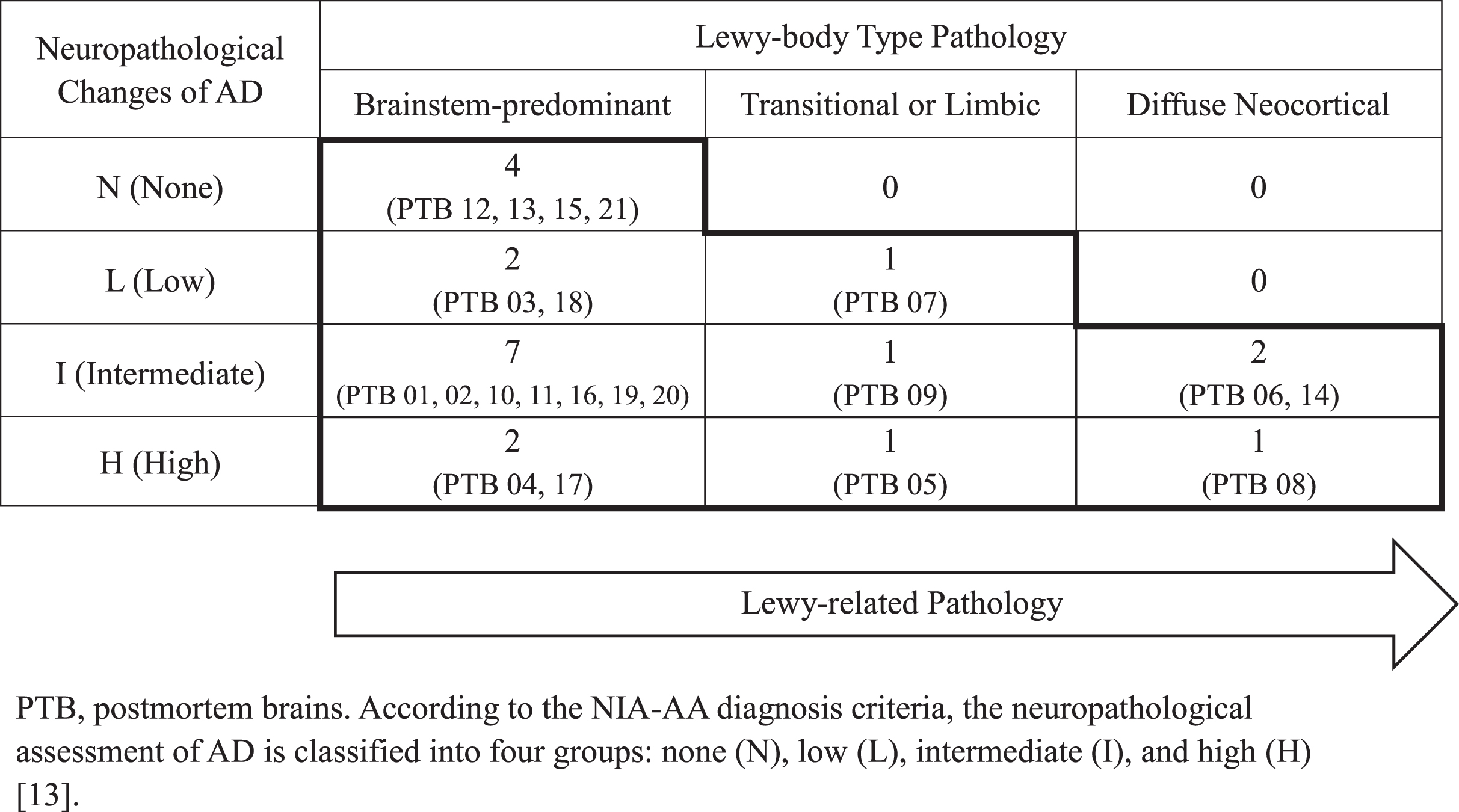
Furthermore, in the 21 neuropathological diagnosed LRP cases, we found 60% (9/15) LRP brainstem-predominant type combined with the intermediate or high-level AD neuropathology, 67% (2/3) LRP transitional/limbic type combined with intermediate or high-level AD neuropathology, and 100% (3/3) LRP diffuse neocortical type combined with intermediate or high level AD neuropathology (Table 4). Considering altogether 81% (17/21) of the diagnosed LRP cases, regardless of types, concurred with either low, intermediate or high-level AD neuropathology, it would be vital to check AD neuropathologic alterations in the LRP etiology study, and vice versa, in the future (Table 4).
Besides, the antemortem diagnostic accuracy of LRP needed to be improved. In our study, we found only the diffuse neocortical type cases (14%, 3/21) were being clinically diagnosed as PD during life (Table 1). Neither brainstem-predominant nor transitional/limbic type case was being clinically identified as PD/Lewy body disease (LBD) during life (Table 1).
In order to further investigate the correlation among the common characteristics of proteinopath-ies, we staged and scored the neuropathological change of Aβ deposits, neurofibrillary tangles, and neuritic plaques in each of the 21 pathologically diagnosed LRP cases (Table 5). We found that there was a positive correlation between α-synuclein pathology and Aβ pathology: 76% (16/21) of LRP cases had an intermediate or high-level Aβ pathology, equivalent to A score 2 or 3 (Table 5). Meanwhile, we found the positive correlation existed between α-synuclein pathology and tau pathology: 71% (15/21) of LRP cases had an intermediate or high-level tau pathological staging level, equivalent to B score 2 or 3 (Table 5). Besides, we identified 62% (13/21) of LRP cases had an intermediate or high-level staging of neuritic plaques, equivalent to C score 2 or 3 (Table 5).
Neuropathological Changes of Amyloid β, Phospho-Tau and Neuritic Plaques in 21 Neuropathologically Diagnosed LRP Cases. Results were displayed as the number of cases

After analyzing AD neuropathological changes of each LRP case, we found that 62% (13/21) of LRP cases had an intermediate or high-level score for tau pathology and Aβ pathology. 52% (11/21) of LRP cases had all three neuropathologies, the intermediate or high-level staging of Aβ deposits, phospho-tau and neuritic plaques (Table 5). Meanwhile, we found the co-occurrence of neocortical α-synuclein, Aβ deposits, phospho-tau, and neuritic plaques pathologies in the neuropathologically diagnosed LRP cases. In our work, we identified three LRP diffuse neocortical type cases, PTB 06, PTB 08, and PTB 14, with the highest neuropathology level of α-synuclein spread and aggregation in the brain. Interestingly in these donors, we also identified the intermediate or high-level neuropathology of Aβ deposits (A score 2 or 3), phospho-tau (B score 2 or 3), and neuritic plaques (C score 2 or 3) in addition to the neocortical α-synuclein pathology (Table 5).
Progression of LRP deteriorated Everyday Cognitive function and triggered dementia
The Everyday Cognitive (ECog) function evaluation was performed for each LRP case within 24 h after death by in person or phone interview with immediate kin of the brain donor (Table 6). Overall, global ECog scores increased along with LRP anatomic progression, the process of α-synuclein spreading from the brainstem (ECog Mean±SD, 1.25±0.63), limbic (ECog Mean±SD, 2.87±2.14) to neocortical (ECog Mean±SD, 3.90±0.10) reg-ions (Fig. 2). After comparing the differences of global ECog scores among LRP brainstem-predo-minant type, LRP transitional/limbic type, and LRP diffuse neocortical type, we found ECog scores showed significant difference between the groups of LRP brainstem-predominant type and LRP diffuse neocortical type, which indicated the everyday cognitive function might be deteriorated along with the LRP anatomic progression (Fig. 2). Taken 2.0 as the cut-off score of dementia, we found the mean and median scores of LRP transitional/limbic type (2.87, 2.40) and LRP diffuse neocortical type (3.90, 3.90) were above the dementia cut-off score (Fig. 2) [14, 17]. Our data suggested the LRP impairment of cognitive domains including transitional/limbic and diffuse neocortical areas were more likely to develop dementia and deteriorated the cognitive dysfunction compared with the brainstem-predominant region.
Comparation of Global ECog Scores between Groups of LRP Brainstem-predominant Type and LRP Diffuse Neocortical Type. The ECog score of PTB 04 was “unknown” and excluded from the table
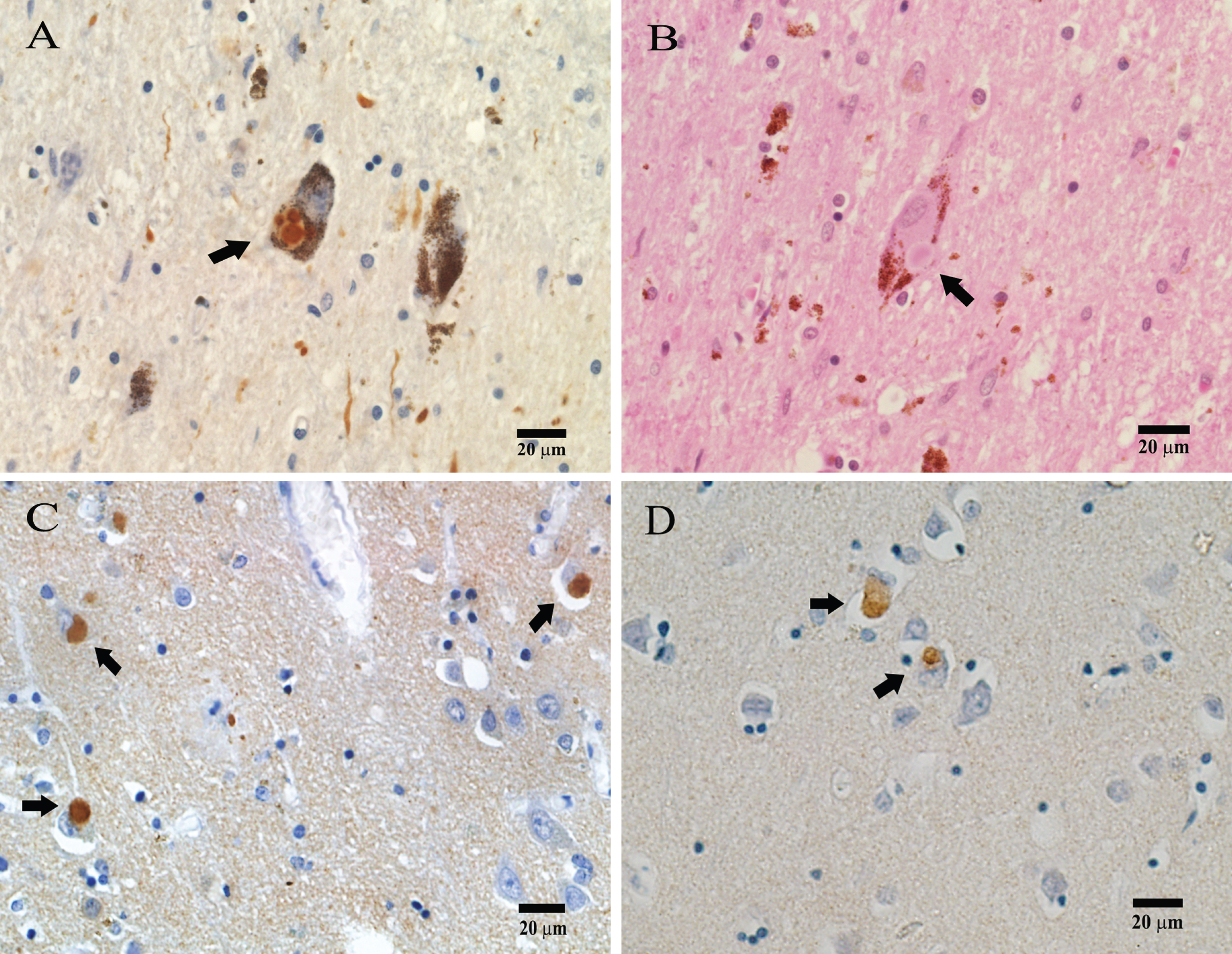
LRP Positive Pathology Diagnosis. Immunohistochemical detection of Lewy body deposit (indicated with arrow) using α-synuclein antibody in midbrain (A), hippocampus (C), and temporal (D). B) Hematoxylin & Eosin (HE) Staining for midbrain.
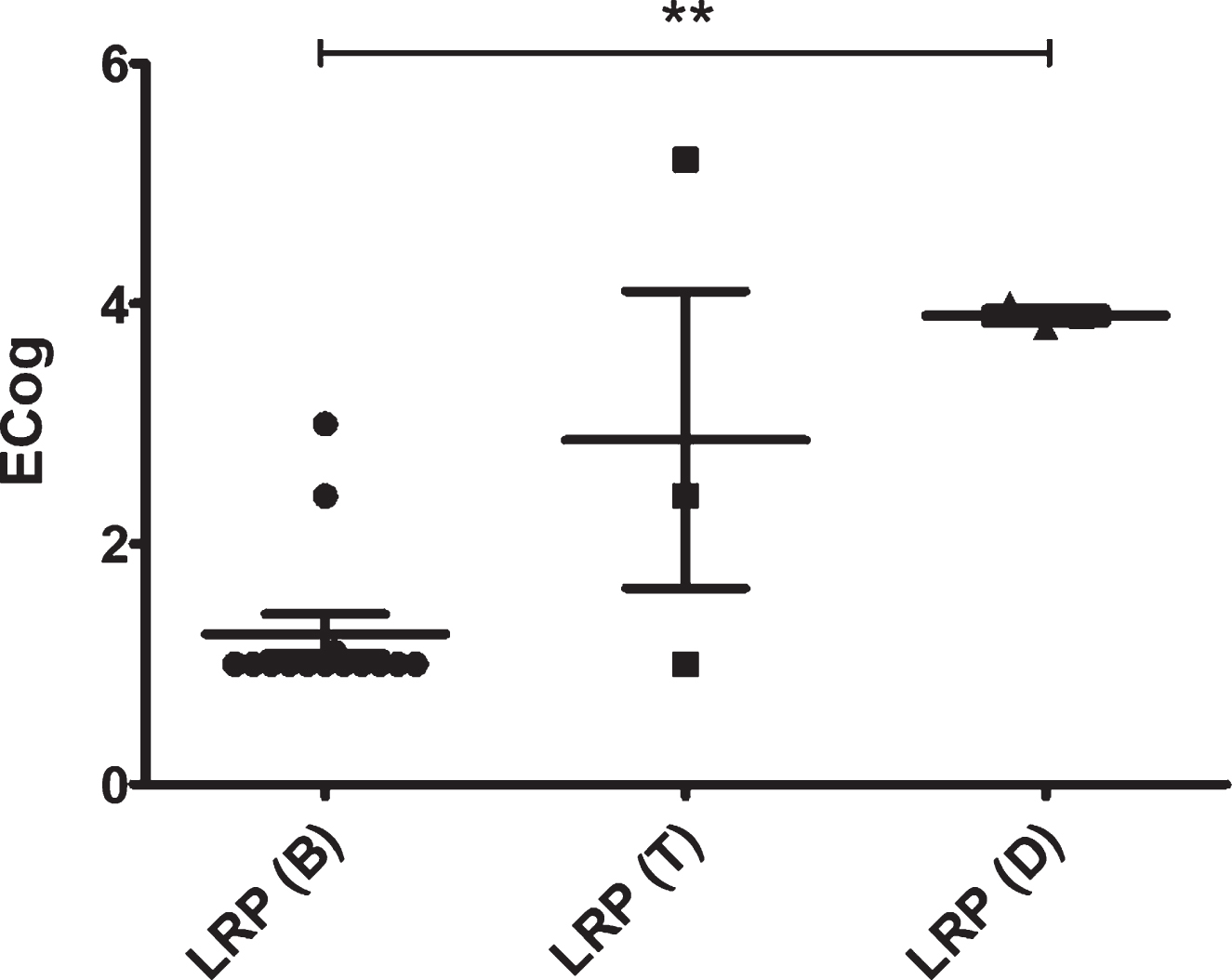
Comparation of Global ECog Scores among LRP Brainstem-predominant, Transitional or Limbic, and Diffuse Neocortical Types. LRP (B), LRP brainstem-predominant type (n = 14). LRP (T), LRP transitional or limbic type (n = 3). LRP (D), LRP diffuse neocortical type (n = 3). The ECog score of PTB 04 was “unknown” and excluded from the figure.
To study the contribution of LRP in daily cognitive dysfunction of the combined LRP-AD neuropathology, we selected another 20 neuropathologically diagnosed AD cases, meanwhile without any Lewy-related neuropathological change, as the control group. The average age of these 20 AD cases was 83 and 45% were male. The same ECog function evaluation was performed on the AD control group as well. Taken 2.0 as the cut-off score of dementia, we found 1) the mean and median scores (3.10, 3.10) of the combined LRP (transitional/limbic type)-AD group were above the mean and median scores (2.26, 2.20) of the AD control group, 2) the mean and median scores (3.90, 3.90) of the combined LRP (diffuse neocortical type)-AD group were above the mean and median scores (2.26, 2.20) of the AD control group, 3) the mean and median scores (3.90, 3.90) of the combined LRP (diffuse neocortical type)-AD were above the mean and median scores (3.10, 3.10) of the combined LRP (transitional/limbic type)-AD group, and 4) ECog scores showed the significant difference between the AD control group and the combined LRP (diffuse neocortical type)-AD group (Table 7, Fig. 3). Taken together, our findings indicated the progression of LRP might aggravate the deterioration of cognitive function in addition to that effect of AD.
Comparation of Global ECog Scores between Groups of AD and the Combined LRP (Diffuse Neocortical Type)-AD
AD, the intermediate or high-level AD neuropathology, meanwhile without any Lewy-related neuropathological change. LRP (diffuse neocortical type)-AD, the combined LRP (diffuse neocortical type) with the intermediate or high-level AD neuropathology.

Comparation of Global ECog Scores among AD, the Combined LRP (T)-AD, and the Combined LRP (D)-AD. AD, the intermediate or high-level AD neuropathology, meanwhile without any Lewy-related neuropathological change (n = 20). LRP (T)-AD, the combined LRP (transitional or limbic type) with the intermediate or high-level AD neuropathology (n = 2). LRP (D)-AD, the combined LRP (diffuse neocortical type) with the intermediate or high-level AD neuropathology (n = 3).
DISCUSSION
The significant overlap of α-synuclein, Aβ, and phospho-tau pathologies in neuropathologically diagnosed LRP human brains
A-synuclein is a 14-kDa protein that forms the major component of abnormal neuronal aggregates, Lewy bodies [18]. In AD patients, the hyperphosphorylated tau accumulates into intracellular tangles, whereas Aβ accumulates into extracellular plaques [19]. The common characteristics of proteinopathies suggest α-synuclein, Aβ, and phospho-tau may work in concord in the pathological development of neurodegeneration diseases. In our study, we found that 81% neuropathologically diagnosed LRP cases combined with AD neuropathology, and significant (intermediate or high-level) neuropathologic changes of both Aβ deposits and phospho-tau were observed in 62% LRP cases at the China Human Brain Bank. Furthermore, our intriguing findings revealed the overlap of neocortical α-synuclein, Aβ deposits, phospho-tau, and neuritic plaques pathologies in LRP cases, which suggested the potential interplay among the common characteristics of proteinopathies in the late stage of neuropathological development of LRP in human brains.
Our findings were in keeping with experimental evidence around the world where investigations in different countries also reported the distribution of AD neuropathology in LRP cases: In Japan, resea-rchers found that 4 of 11 (36%) DLB cases had an intermediate or high likelihood for AD after imm-unostaining diagnosis with postmortem brains [20]. In the United Kingdom, the co-existence of α-syn-uclein, Aβ, and tau neurofibrillary tangles were found at the Queen Square Brain Bank, and the three pat-hologies almost perfectly discriminated demented from non-demented cases [21]. In the Lewy body spectrum disorders patient cohort study from five academic institutions in five cities in the United States, 21% combined with intermediate-level AD neuropathology and 30% with high-level AD neuropathology [22]. In the State of Florida Brain Bank, the concomitant of AD was present in 66% of LBD patients [23]. Also, with brain tissues from Sun Health Research Institute in Arizona, another study identified 27 of 66 (41%) PD subjects combined with AD neuropathological changes [24].
The higher clinical prevalence of neurodegenerative diseases in China may lead to the higher ratio and level of AD neuropathological changes in LRP cases, compared with data from other countries. However, future investigations may need to revisit this difference after having collected much more samples, considering the potential significant under-diagnosed rate of LBD. For example, we in this study found the low antemortem diagnostic accuracy, especially for LRP at the early and middle stages of neuropathological progression. Besides, the genetic and/or epigenetic factors that contributed to the co-existence of α-synuclein, phosphorylated tau, and Aβ plaques may be the crucial concern in understanding the phenotype variance between different population groups.
Cognitive dysfunction deteriorated along with LRP anatomic progression
Cognitive impairment represents an important co-mponent of the clinical syndromes of LRP and can occur in one or more domains, vary in severity, and present differently at various stages of the disease [25]. Taken global ECog score 2.0 as the divi-ding point between mild cognitive impairment and dementia, our data indicated the ECog score in-creased along with LRP anatomic progression, from the brainstem (ECog Mean±SD, 1.25±0.63), lim-bic (ECog Mean±SD, 2.87±2.14) to neocortical (ECog Mean±SD, 3.90±0.10) regions, in human brains, and the progression of LRP might aggravate the deterioration of cognitive function in addition to that effect of AD (ECog Mean±SD, 2.26±1.08) (Figs. 2 and 3). Furthermore, the mean and median ECog scores were above the dementia cut-off score when LRP developed into transitional/limbic and neocortical regions rather than the brainstem, and that LRP-associated dementia may work in concord with the AD-associated dementia in deteriorating cognitive function (Figs. 2 and 3).
A better understanding of the progression of cognitive deficits and LRP is essential for the development of therapeutic strategies. The inter-individual variability of cognitive evaluation findings, such as LRP brainstem-predominant type cases with high global ECog score in the setting of relatively low levels of neocortical and limbic α-synuclein pathology is perhaps due to the presence of neuropathologic co-morbid AD, while other cases sustaining relatively high levels of such neuropathology before exhibiting cognitive impairment may be because of neocortical plasticity, cognitive reserve or other unknown factors [26]. Considering the patient differences in the progression of cognitive dysfunction and in the risk factors for LRP development, more studies and sample cases are being needed to elucidate the relationship regarding the progression of LRP and cognitive deficits. Besides, another limitation in our study is that our ECog data is generated postmortem from immediate kin of the brain donor, which may not directly reflect the donor’s cognitive status compared with the antemortem data.
Conclusions and future direction
Our work was the first investigation that summarized LRP neuropathological findings from Chinese postmortem brains. We identified 81% neuropathologically diagnosed LRP cases combined with AD neuropathology, and significant (intermediate or high-level) neuropathologic changes of both Aβ deposits and phospho-tau were observed in 62% LRP cases. Furthermore, we found the anatomic progression of LRP deteriorated cognitive function and the LRP-associated dementia may work in concord with AD-associated dementia in aggravating cognitive dysfunction.
The significant overlap of α-synuclein, Aβ, and phospho-tau pathologies in LRP and AD indicates the potential interplay of those three proteins in the pathological development of neurodegenerative disorders. However, the precise role of the interplay among α-synuclein, phospho-tau, and Aβ in the downstream cellular and molecular dysfunction in neurodegenerative disorders is still unclear and remains to be further investigated. Furthermore, rather than gene mutations, epigenetic modifications play an important role in the etiopathology of protein aggregation in neurodegenerative changes. The striking overlap of the epigenetically disrupted human DNA methylome patterns between AD, PD, DLB, and Down syndr-ome suggested these neurodegenerative diseases mi-ght share similar epigenetic pathomechanisms that subsequently evolve into different protein aggregations as well as clinical entities [27]. Hence, the com-binatory role of environmental stimuli and aging in the remodeling of human epigenome and neuropathological development need to be revisited. Future neuroepigenetic studies focusing on the pathomechanism of α-synuclein, phospho-tau, and Aβ plaques would be vital for understanding the pathogenesis of neurodegenerative diseases as well as the dev-elopment of therapeutic strategies. In particular, neuroepigenetic modifications, especially DNA met-hylation, may play a crucial role in human neurodegenerative dysfunctions such as the combined LRP-AD neuropathology. Therefore, future studies at the China Human Bank focusing on investigating DNA methylome and comparing those critical genes, including SNCA, APP, MAPT, DUSP22, and DUSP6, will help to elucidate the underlying downstream cellular and molecular dysfunction in the combined LRP-AD neuropathology (Fig. 4). Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-1548).

The Hypothesized Model of Epigenetic Pathomechanism in LRP-AD Neuropathology. Rather than gene mutations, epigenetic modifications play an important role in the etiopathology of protein aggregation in neurodegenerative changes. The cause of this epigenetic change might be derived from the outer environmental stimuli and/or the aging process.
Footnotes
ACKNOWLEDGMENTS
Tissue provided by: National Human Brain Bank for Development and Function, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China. This study was supported by the Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences, Neuroscience Center, and the China Human Brain Banking Consortium. The authors would like to thank Ms. Yunli Ling, Ms. Yuanyuan Xu, Dr. Qian Yang and Mr. Qin Zhang for technical assistance.
This study was supported by grants from the National Natural Science Foundation of China (NSFC #91632113, #81771205), the Natural Science Foundation and Major Basic Research Program of Shanghai (16JC1420500, 16JC1420502), and the CAMS Innovation Fund for Medical Sciences (CIFMS #2017-I2M-3-008).