
Abstract
Background:
Identifying modifiable risk factors for cognitive decline can reduce burden of dementia.
Objective:
We examined whether homocysteine was associated with memory performance, mediated by entorhinal volume, hippocampal volume, total gray matter volume, or white matter lesions, and moderated by APOE ɛ4 allele, B vitamins, creatinine, total cholesterol, or triglycerides.
Methods:
All 204 members of the Czech Brain Aging Study with subjective cognitive decline (SCD; n = 60) or amnestic mild cognitive impairment (aMCI; n = 144) who had valid data were included. Linear regression was used, followed by conditional process modeling to examine mediation and moderation.
Results:
Controlling for age, sex, and education, higher homocysteine was related to poorer memory performance overall (b = –0.03, SE = 0.01, p = 0.017) and in participants with SCD (b = –0.06, SE = 0.03, p = 0.029), but less so in aMCI (b = –0.03, SE = 0.02, p = 0.074); though sensitivity analyses revealed a significant association when sample was reduced to aMCI patients with more complete cognitive data (who were also better functioning; b = –0.04, SE = 0.02, p = 0.022). Results were unchanged in fully adjusted models. Neither mediation by markers of brain integrity nor moderation by APOE ɛ4, B vitamins, creatinine, and cardiovascular factors were significant. Memory sub-analyses revealed that results for SCD were likely driven by non-verbal memory. The homocysteine-memory relationship was significant when hippocampal volume was below the median (b = –0.04, SE = 0.02, p = 0.046), but not at/above the median (p = 0.247).
Conclusion:
Higher homocysteine levels may adversely influence memory performance, which appears particularly apparent in those without cognitive impairment. Results appear to be independent of brain health, suggesting that homocysteine may represent a good target for intervention.
INTRODUCTION
Alzheimer’s disease (AD) is the most prevalent cause of dementia affecting older adults [1]. The underlying biological mechanisms of AD include the accumulation of amyloid-β plaques, neurofibrillary tau tangles, and neurodegeneration which is reflected in latest research (AT(N) criteria [2]). However, other factors may also be important for progression from subjective cognitive decline (SCD) and mild cognitive impairment (MCI) towards AD dementia [3]. Memory deficit in individuals with MCI is associated with a substantially higher risk of conversion to AD dementia [4]. Therefore, identifying factors associated with memory performance may better explain upstream processes important for pathological cognitive aging. Identifying such factors that both affect the rate of progression toward dementia syndrome and are modifiable is doubly important in the efforts to modify disease risk through intervention and thus reduce the burden of dementia on society. In this context, homocysteine may represent one such opportunity.
Homocysteine is a sulfur amino acid, a product of methionine metabolism [5]. At high concentrations, homocysteine is neuro- and vasotoxic [6]. Elevated homocysteine blood level has been identified as a risk factor for MCI [7, 8] and AD dementia [5, 9–11]. However, what underlies the association between homocysteine and cognition remains unclear. Historically, the link between higher levels of homocysteine and lower levels of B vitamins and folate, which may suppress cognitive function, was one proposed mechanism [12], but this link may not explain fully the homocysteine-cognition relationship [10]. Evidently, other potential pathways for this relationship may exist [5, 13].
Previous research has reported a negative associ-ation between homocysteine and memory performance in healthy older adults as well as adults with MCI or AD dementia [14–19]. Others have suggested a relationship between a higher homocysteine level and less structural integrity or greater brain atrophy [10, 20–26]. However, few have examined homocysteine in relation to memory and brain health mar-kers simultaneously to test whether brain health may underlie the association between homocysteine and cognitive functioning, in particular memory functioning. Studies testing this mediation found that white matter lesions (WMLs) did not mediate the association between homocysteine and cognitive functioning when assessed with attention, psychomotor speed, and global cognition [27], or when assessed with spatial navigation performance [28]. Another study [18] found no changes in the relationship between homocysteine and memory after controlling for WMLs and brain atrophy, but they did not directly assess the mediating relationship, leaving the possibility of mediation by brain health unclear.
Also notable is the role of the ɛ4 allele of the apolipoprotein E (APOE) gene in the presumed association between homocysteine levels and memory, which remains unclear. While some have found more elevated homocysteine in carriers of the APOE ɛ4 allele than non-carriers [11, 19], others have found that APOE ɛ4 carriers are at a lower risk for hyperhomocysteinemia [29]. There is also mixed evidence for whether APOE ɛ4 status moderates the association between homocysteine and cognition, with some suggesting that APOE ɛ4 magnifies the link between homocysteine and cognition [30] and others reporting null results for moderation by APOE ɛ4 [27, 31].
We built on previous research by examining the association between homocysteine and memory in participants with SCD and amnestic MCI (aMCI). A previous study from the same cohort investigated the association between homocysteine and spatial nav-igation [28], finding higher levels of homocysteine were related to poorer spatial navigation performa-nce. We focused on the memory domain specifically because of its central role in progression towards AD dementia. Specific memory subdomains—immediate recall, delayed recall, verbal memory, and non-ver-bal memory—were also considered. To help better understand any homocysteine-memory link, we also tested potential mediation by structural integrity associated with dementia (i.e., entorhinal volume, hippocampal volume, and total gray matter volume) or WMLs and moderation by APOE ɛ4 status, B vitamins, creatinine, and cardiovascular risk factors. We hypothesized that higher levels of homocysteine would be associated with poorer memory performance. Based on the limited previous research including both cognitive tests and brain health markers, we also expected measures of structural integrity to only partially mediate the association between homocysteine and memory performance. We expected the results to be particularly pronounced for tests of delayed recall.
MATERIALS AND METHODS
Participants
Participants were members of the Czech Brain Aging Study [32] who were diagnosed with either SCD or aMCI. Participants were volunteers referred to the clinic by general practitioners, neurologists, psychiatrists, and geriatricians based on cognitive complaints reported by themselves and/or by their informants. For this study, participants were incl-uded if (a) they completed comprehensive neuropsychological testing, blood profile, had diagnostic information indicating SCD or aMCI, and magnetic resonance imaging (MRI) and (b) there were 60 days or fewer between their blood collection, their neuropsychological testing, and their MRI acquisition (n = 355). Participants with missing diagnosis information (n = 6), less than 50%of memory tests available (n = 31), with elevated depressive symptoms (n = 82; Geriatric Depression Scale 15-item version [GDS-15]; cutoff ≥6 [33]), missing data on the homocysteine variable (n = 14), or who were outliers (>2.5 SD above the mean per diagnosis group) on variables with excessive (positive) skewness (i.e., homocysteine, vitamin B12, triglycerides; n = 18) were dropped. The final sample (n = 204) included participants with SCD (n = 60, M age = 66.92, SD = 8.46; M education = 16.08, SD = 3.37; 19 men, 41 women) or aMCI (n = 144, M age = 71.80, SD = 8.04; M education = 14.56, SD = 3.61; 76 men, 67 women). See Fig. 1 for a flow chart of inclusion and exclusion criteria used to create the analytic sample.
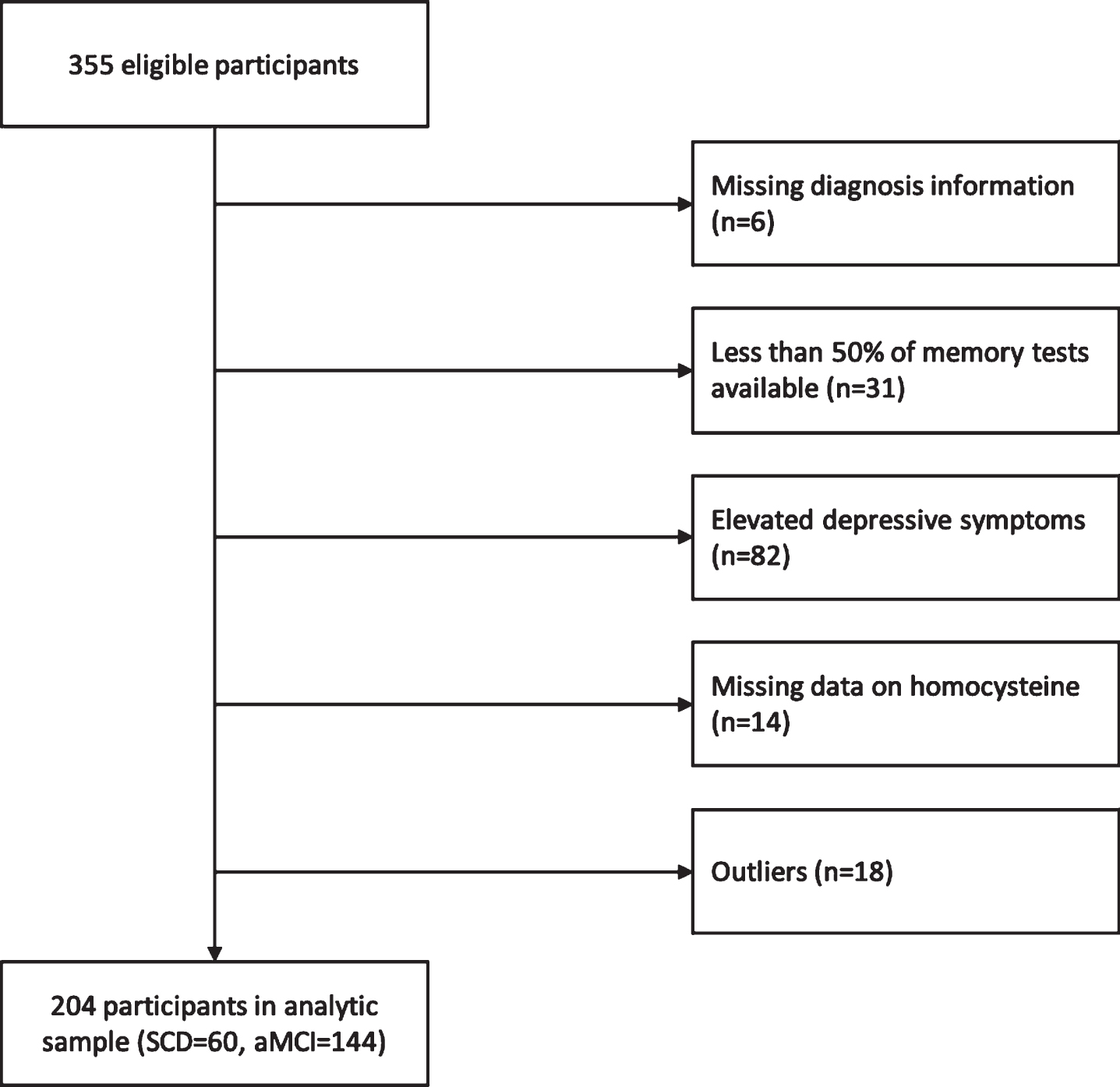
Flow chart illustrating inclusion and exclusion of participants in the analytic sample. Participants were initially eligible if (a) they completed comprehensive neuropsychological testing, blood profile, had diagnostic information indicating SCD or aMCI, and magnetic resonance imaging (MRI) and (b) there were 60 days or fewer between their blood collection, their neuropsychological testing, and their MRI acquisition.
SCD was diagnosed based on the presence of subjective cognitive complaints without deficits in objective cognitive performance (i.e., scoring within normal limits [not greater than 1.5 standard deviations below] on age- and education-adjusted norms for neuropsychological tests) and was not associated with any acute event [34]. Participants with aMCI met published clinical criteria for aMCI [35], including memory complaints reported by themselves and/or their informants, evidence of memory dysfunction on neuropsychological testing, generally intact activities of daily living, and absence of dementia. Memory impairment was established when the patient scored more than 1.5 standard deviations below the mean of age- and education-adjusted norms on any memory test. Participants meeting the Diagnostic and Statistical Manual of Mental Disorders IV-TR criteria for dementia were not included.
Procedures
The Czech Brain Aging Study (CBAS) is a clinic-based longitudinal study of brain and cognitive aging conducted across two university hospitals—Motol University Hospital in Prague and St. Anne’s University Hospital in Brno [32]. The current study included cross-sectional data only from Motol University Hospital in Prague. Participants are eligible if they are at least 55 years old and do not have dementia at their baseline assessment. Participants complete neurological and neuropsychological assessments, laboratory procedures, brain CT or MRI, and provide sociodemographic information. CBAS is approved by an ethical committee and all subjects sign informed consent.
Measures
Memory
Memory was calculated as a composite score for all participants who had at least 50%of the tests available. Memory was assessed with four tests wh-ich included seven separate scores (Cronbach’s alpha = 0.93). Immediate memory was assessed with the Rey Auditory Verbal Learning Test (RAVLT –Immediate –Sum of Trials 1–5 [36]), the Brief Visuospatial Memory Test –Revised (BVMT-R Immediate –Sum of Trials 1–3 [37]), and the Uniform Data Set Logical Memory (Logical Memory –Immediate [38]); delayed memory with the RAVLT –Delayed [36], the BVMT-R –Delayed [37], and Logical Memory –Delayed [38]; verbal memory with the RAVLT [36] and Logical Memory [38]; and non-verbal memory with the BVMT-R [37] and the Rey-Osterrieth Complex Figure Test Recall (ROCFT; recall after three minutes [39]). In addition to assessing the overall memory domain, we also considered each of the four memory subdomains separately. Most participants had full data for the memory tests (75.49%), with 14.71%missing one test, 3.92%missing two tests, and 5.88%missing three tests. The individual tests were standardized using group-specific (SCD, aMCI, full sample) z-scores and then averaged.
Biological measures
The collection of biological samples has been previously described [28]. Briefly, venous blood samples were collected following a 12-h fast. The blood samples were maintained on ice immediately following collection and were centrifuged at 4–8°C within 2 h, with sodium heparin added as the anticoagulant. Although other blood measures are collected, the current study focused on homocysteine, with total cholesterol, triglycerides, vitamin B12, folate, and creatinine included as covariates. We chose to focus specifically on total cholesterol because of the high correlation between total cholesterol and low-density lipoprotein (LDL) cholesterol (r = 0.90) and our focus on cholesterol as a risk factor for poor mem-ory performance. Further, APOE genotyping was determined by a procedure using leukocyte DNA samples [40]. APOE status was dichotomized with carriers of at least one ɛ4 allele vs. not. Homocysteine was included as a continuous variable and as a dichotomous variable with the commonly used cutoff of ≥12μmol/L. We chose to include the dichotomous variable because some have suggested that homocysteine may not be detrimental to cognitive functioning until a threshold of 12μmol/L has been met [10, 41].
MRI acquisition
MRI was acquired on a 1.5T scanner (Avanto; Siemens, Erlangen, Germany) using T1-weighted 3-dimensional high-resolution magnetization-prepa-red rapid acquisition with gradient echo (MPRAGE) sequence with the following parameters: TR/TE/TI = 2000/3.08/1100 ms, flip angle 15°, 192 continuous partitions, slice thickness 1.0 mm, and in-plane resolution 1 mm. Scans were visually examined by a single neuroradiologist, blinded to the diagnosis, for sufficient technical quality and the absence of structural findings contradicting eligibility [42]. MRI volumetry was processed using Freesurfer (v5.0; http://surfer.nmr.mgh.harvard.edu; [43]).
Bilateral entorhinal volume was computed as the sum between the right and left entorhinal volumes. Bilateral hippocampal volume was computed as the sum between the right and left hippocampal volumes. Entorhinal volume, hippocampal volume, and total gray matter volume were corrected for estimated intracranial volume (ICV) to account for differences in head size [44]. In analyses, these variables were presented as %ICV. Presence of WMLs was assessed based on visual inspection of MRI scans, as previously described [28]. Based on this assessment, participants received a score on the Fazekas scale [45]. Possible scores range from 0 (absence of WMLs) to 3 (severe WMLs). Entorhinal volume, hippocampal volume, total gray matter volume, and WMLs served as mediators in the analyses.
Statistical analyses
Basic descriptive statistics were calculated to describe the sample and differences between participants with SCD and aMCI were assessed with t-tests or chi-square tests where applicable. Next separate hierarchical regressions were conducted relating homocysteine to memory scores. Regression models were estimated for the entire group and separately by diagnosis. Model 1 was adjusted for age, sex, and years of education. Model 2 additionally controlled for vitamin B12 and folate, which are known factors associated with homocysteine and cognition. Model 3 added a measure of renal function which is associated with homocysteine levels—creatinine—and cardiovascular risk factors—total cholesterol and triglycerides. Mediation analyses were conducted to assess the association between homocysteine and memory with entorhinal volume, hippocampal volume, total gray matter volume, and WMLs serving as mediators. These analyses were adjusted for age, sex, and education to create parsimonious models, after we observed that additional covariates did not influence the main results. Finally, we assessed the effects of APOE status (coded as the presence or abs-ence of an ɛ4 allele), B vitamins, creatinine, and cardiovascular risk factors on the association between homocysteine and memory through moderation ana-lyses. All analyses were conducted using SAS software (SAS Institute, Cary, NC) Version 9.4. Mediation and moderation analyses were conducted with the PROCESS Macro Version 3.4.1 in SAS [46]. For mediation analyses, we used the bootstrapping method to test for significance of the indirect effect with 10,000 bootstrap samples with a 95%confidence interval (CI). In the mediation analyses, the “a path” represents the relationship between the independent variable and the mediator, the “b path” represents the relationship between the mediator and the dependent variable, the “c path” (total effect) represents the effect of the independent variable on the dependent variable, and the “c’ path” (direct effect) represents the effect of the independent variable on the dependent variable while accounting for the mediator. See Fig. 2 for an illustration of the mediation pathways in our study. Significance was assessed according to p < 0.05 criteria.
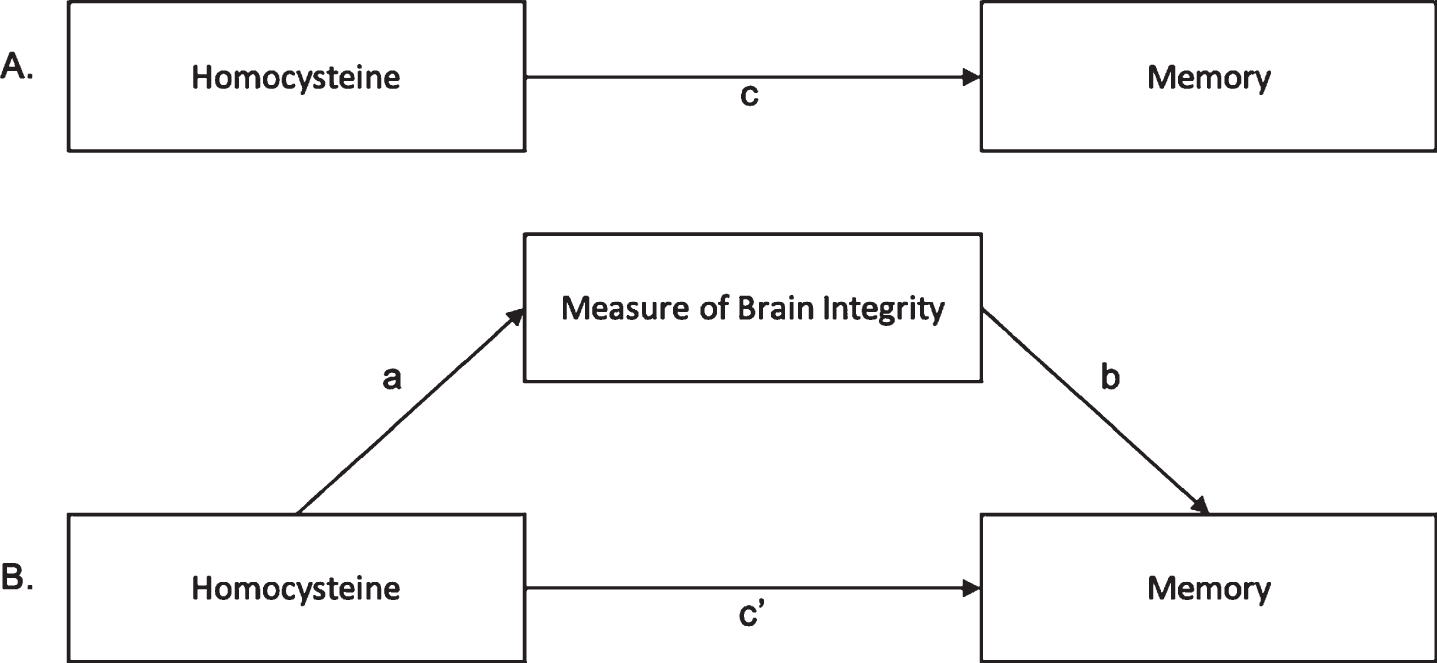
Illustration of Mediation Pathways. Panel A illustrates the total effect, i.e., the relationship between homocysteine and memory without the mediator. Panel B illustrates the mediation relationship, including path a (relationship between homocysteine and the mediator), path b (relationship between the mediator and memory), and path c’ (the relationship between homocysteine and memory accounting for the mediator). The measures of brain integrity that served as the mediator included bilateral entorhinal volume, bilateral hippocampal volume, total gray matter volume, and white matter hyperintensities.
RESULTS
The overall sample had an average age of 70.36 years (SD = 8.44; range: 49 to 91) and an average of 15.01 years (SD = 3.60) of education. Slightly over half of the sample were women (53.20%). The average score on the GDS-15 was 2.40 (SD = 1.62) indicating absence of depressive symptoms. Just over a half of the sample were non-carriers of the APOE ɛ4 allele (62.15%), 34.46%were heterozygotic carriers and 3.39%were homozygotic carriers. The average Fazekas score was 1.40 (SD = 0.96), indicating a low level of WMLs. Participants with aMCI were significantly older (M = 71.80, SD = 8.04, t = –3.86, p < 0.001) and had significantly higher homocysteine (M = 13.60, SD = 4.40, t[160.0] = –3.75, p < 0.001) compared to participants with SCD (M = 66.92, SD = 8.46; M = 11.60, SD = 2.99, respectively), See Table 1 for descriptive statistics for all study variables for the full sample and separately for participants with SCD and aMCI. See Table 2 for intercorrelations among study variables.
Descriptive statistics for all participants and by diagnosis
N = 204; for SCD: n = 60 and for aMCI: n = 144. p-value for t-tests or chi-square assessed differences between participants with SCD and aMCI. aMCI, amnestic mild cognitive impairment; APOE, apolipoprotein E; AVLT, Rey Auditory Verbal Learning Test; BVMT-R, Brief Visuospatial Memory Test –Revised; Logical, Uniform Data Set Logical Memory Test –Revised; M, mean; MMSE, Mini-Mental State Exam; ROCFT, Rey-Osterrieth Complex Figure Test; SCD, subjective cognitive decline; SD, standard deviation. aAssessed with the Geriatric Depression Scale 15-item version. bAssessed with the Fazekas scale (range 0 to 3). cIncludes the sum of trials 1 to 5. dIncludes the sum of trials 1 to 3.
Intercorrelations among variables
Bolded values indicate significant correlations at p < 0.05. Sex was coded as male = 0, female = 1. APOE status was coded 0 = non-carrier, 1 = carrier of the ɛ4 allele. Entorhinal volume, hippocampal volume, and total gray matter volume were adjusted for estimated intracranial volume. Memory represents the standardized memory domain calculated as a composite score from each of the memory tests for the full group. APOE, apolipoprotein E; MMSE, Mini-Mental State Exam. aWhite matter lesions assessed with the Fazekas scale (range 0 to 3).
Main results are presented in Table 3. Controlling for age, sex, and education, higher levels of homo-cysteine were significantly related to poorer memory performance for the full sample (b = –0.03, SE = 0.01, p = 0.017) and for participants with SCD (b = –0.06, SE = 0.03, p = 0.029). The association only approached significance for participants with aMCI (b = –0.03, SE = 0.02, p = 0.074). The pattern of results was similar when homocysteine was included as a dichotomous variable, although the association did not reach statistical significance for the full sample (full sample: b = –0.18, SE = 0.11, p = 0.111; SCD: b = –0.45, SE = 0.16, p = 0.008; aMCI: b = –0.17, SE = 0.14, p = 0.207). In SCD, high homocysteine was associated with almost a half SD lower memory score. The results were not explained by further adjustment for vitamin B12 and folate, or for creatinine, total cholesterol, and triglycerides.
Results from the regression analyses for the association between homocysteine and memory performance
Model 1 controlled for age, sex, and education. Model 2 additionally controlled for vitamin B12 and folate. Model 3 additionally controlled for creatinine, total cholesterol, and triglycerides. Dichotomous homocysteine was dummy coded as 0 = normal (<12μmol/L) and 1 = elevated (≥ 12μmol/L). Bolded values indicate significant results. aMCI, amnestic mild cognitive impairment; b, unstandardized regression coefficient; SCD, subjective cognitive decline; SE, standard error. an = 201, 172, and 167 for Models 1, 2, and 3, respectively. bn = 59, 52, and 50 for Models 1, 2, and 3, respectively. cn = 142, 120, and 117 for Models 1, 2, and 3, respectively.
We next examined whether WMLs, entorhinal vol-ume, hippocampal volume, or total gray matter vol-ume mediated the relationship between homocysteine and memory (Table 4). For the full sample and for participants with SCD and aMCI, neither WMLs, entorhinal volume, hippocampal volume, nor total gray matter volume mediated the relationship bet-ween homocysteine and memory performance. Using the full sample as an example, WMLs, entorhinal volume, hippocampal volume, and total gray matter volume accounted for less than 27%(0%, 6.47%, 10.59%, and 26.18%, respectively) of the significant associations between homocysteine and memory.
Mediation analyses testing effect of entorhinal volume, hippocampal volume, total gray matter volume, and white matter lesions on the relationship between homocysteine and memory performance
Analyses controlled for age, sex, and education. Bolded values indicate significant results at p < 0.05. X, homocysteine; M, entorhinal volume, hippocampal volume, total gray matter volume, or white matter lesions; Y, memory. Entorhinal volume, hippocampal volume, and total gray matter volume were corrected for estimated intracranial volume. White matter lesions were assessed with the Fazekas scale. aMCI, amnestic mild cognitive impairment; b, unstandardized regression coefficient; LLCI, lower limit confidence interval; SCD, subjective cognitive decline; ULCI, upper limit confidence interval. an = 197, 58, and 139 for full sample, SCD, and aMCI, respectively. bn = 108, 33, and 75 for full sample, SCD, and aMCI, respectively. cIndirect effect based on bootstrapping method with 10,000 bootstrap samples and a 95%confidence interval.
Finally, controlling for age, sex, and education, we did not find that the association between homocysteine and memory was moderated by APOE status, vitamin B12, folate, creatinine, total cholesterol, or triglycerides for the full sample or for those with SCD or aMCI only, whether homocysteine was entered as a continuous or a dichotomous variable (ps > 0.10).
Memory subdomains
Since our memory domain included subdomains (i.e., immediate/delayed and verbal/non-verbal), we also assessed whether patterns were different for the distinct subdomains (Table 5). The results for the full sample showed significant contributions to the memory effect through immediate and delayed memory, as well as verbal and non-verbal memory. The results for SCD seemed to be primarily driven by non-verbal memory with a smaller effect for immediate and delayed memory.
Results from the regression analyses for the association between homocysteine and memory subdomain performance
The models controlled for age, sex, education, vitamin B12, folate, creatinine, total cholesterol, and triglycerides. Dichotomous homocysteine was dummy coded as 0 = normal (<12μmol/L) and 1 = elevated (≥12μmol/L). The top 25th percentile of homocysteine was dummy coded based on the values for SCD of 13.58μmol/L and for aMCI of 16.19μmol/L. Bolded values indicate significant results. aMCI, amnestic mild cognitive impairment; b, unstandardized regression coefficient; SCD, subjective cognitive decline; SE, standard error. an = 167. bn = 50. cn = 117.
Sensitivity analyses
We also conducted sensitivity analyses to test whether the amount of missing data on the memory tests was influencing results. Thus, we reduced the sample to include only participants who had at least 80%of the included tests (n = 184; SCD = 60, aMCI = 124). Most participants had full data on the memory tests (83.70%) while the remaining participants were missing one test (16.30%). Cronbach’s alpha remained virtually the same at 0.92. Since the sample was the same for participants with SCD, we only ran analyses for the full group and for the participants with aMCI.
Results were consistent for Models 1–3 for the full sample, such that higher levels of homocysteine were associated with worse memory performance when homocysteine was included as a continuous variable, but also when included as a dichotomous variable (data not shown). For the aMCI group, higher levels of homocysteine were associated with worse memory performance in Model 1 (b = –0.04, SE = 0.02, p = 0.022), Model 2 (b = –0.04, SE = 0.02, p = 0.008), and Model 3 (b = –0.04, SE = 0.02, p = 0.0499) when homocysteine was a continuous variable. As in main analyses, homocysteine as a dichotomous variable was not associated with memory (data not shown). In order to examine whether those who were excluded from the analyses seemed to be more advanced in their clinical impairment, we conducted a post hoc t-test to test differences in memory performance for participants with aMCI who were included versus dropped from the sensitivity analyses. The group with fewer tests available performed significantly worse on the memory domain compared to participants with more tests available (M = –0.82, SD = 0.26 versus M = 0.13, SD = 0.73, respectively), t(76.5) = 10.76, p < 0.001. The groups were similar regarding age, sex, and education (ps > 0.18).
We examined whether our threshold for homocys-teine was extreme enough to detect negative associations with memory. We categorized presence or absence of elevated homocysteine corresponding to the top 25th percentile of homocysteine for each diagnosis (SCD = 13.58, aMCI = 16.19). The magnitude of the effect was similar to the 12μmol/L threshold (and attenuated to the point of only a trend towards significance for SCD in Model 2).
Since the analyses for the memory subdomains revealed that results for SCD were primarily driven by non-verbal memory, we also tested whether mediation by right and left hippocampal volume was present, since the right hippocampus has been associated with spatial memory previously [42]. Results were consistent with results using bilateral hippocampal volume as the mediator, such that for the full sample, SCD, and aMCI there was no evidence of mediation by either the left or right hippocampus. See Supplementary Table 1 for full results.
Finally, since the results seemed to be driven by participants who have yet to experience impairment (i.e., participants with SCD), we examined whether the association between homocysteine and memory differed for individuals with varying levels of brain integrity, defined by high versus low hippocampal volume based on median split. Results from the fully adjusted model indicated that higher homocysteine was related to poorer memory performance in those with hippocampal volume below the sample median (b = –0.04, SE = 0.02, p = 0.046). The association was not significant in those with hippocampal volume at or above the sample median (p = 0.247).
DISCUSSION
We examined the association between homocyst-eine and memory performance, and we tested mediation by markers of brain health in an attempt to identify potential mechanisms of any homocysteine-memory link. We found that higher levels of homo-cysteine were associated with worse memory performance. Memory subdomains—immediate, de-layed, verbal, non-verbal—contributed about evenly to the overall results. We also found that controlling for vitamin B12 and folate did not explain the associations. In fact, it even slightly (non-significantly) strengthened them, suggesting that the negative correlation between homocysteine and vitamin B12 and folate contributed to the link between homocysteine and memory performance. Results were stronger for participants with SCD than those with aMCI. We did not find evidence that either WMLs, entorhinal volume, hippocampal volume, or total gray matter volume mediated the relationship between homocysteine and memory. These measures explained only 0%, 6.47%, 10.59%, and 26.18%of the associations, respectively, suggesting that the link between homocysteine and memory may not be driven by underlying neurostructural changes. Finally, APOE status, B vitamins, creatinine, and cardiovascular risk factors did not moderate the results.
By being able to assess the associations in participants with SCD and aMCI within one study, we were able to observe that the link between homocysteine and memory may potentially diminish along the cognitive continuum, decreasing in magnitude from SCD to aMCI. This finding was underscored by results excluding those with more significant clinical impairment, whereby the association between higher homocysteine and poorer memory among patients with aMCI was strengthened when the more impaired patients were excluded in the sensitivity analyses (due to having less complete cognitive information). These results may be interpreted along the lines of a previous study where homocysteine was a significant risk factor for transition from cognitively unimpaired to aMCI, but not from aMCI to AD [7]; however, others have found that homocysteine was a risk factor for transition to dementia from normal cognition [47] and that participants with multidomain MCI who converted to dementia had higher baseline levels of homocysteine compared to non-converters [48]. The relationship between homocysteine and memory may be evident only very early on the cognitive decline trajectory, in SCD or early MCI stages, and tapers off when other factors contributing to impaired memory performance (e.g., more downstream AD pathology) may become more important.
We also tested to see whether the relationship between homocysteine and memory depended on the extent of regional brain atrophy and found a significant relationship only for participants who had less than the median hippocampal volume. This suggests that homocysteine may exacerbate memory performance in individuals who are not cognitively impaired but who have an increased risk of developing impairment based on hippocampal volume. The interrelation between homocysteine, hippocampal volume, and memory performance and decline may deserve additional attention. Based on this evidence and trials indicating positive effects of lowering homocysteine on subsequent cognitive performance [49, 50], intervention targeting homocysteine may be worthwhile. Longitudinal research, which points to the possibility that reducing homocysteine levels with vitamin B supplementation can slow age-related brain atrophy as well as reduce age-related cognitive decline [51], further underscores the potential utility of lowering homocysteine levels. Although we did not find brain markers as relevant, it may be that the cross-sectional design we used cannot fully capture the underlying mechanism of the homocysteine-memory link.
A recent systematic review and meta-analysis identified treating hyperhomocysteinemia as a promising clinical target for AD dementia prevention [52]. However, initial research assessing whether reducing homocysteine levels by supplementing B vitamins produces gains in memory performance has resulted in mixed findings, with some suggesting memory gains are unrelated to lowered homocysteine levels [53] and other suggesting reductions in homocysteine are related to reductions in gray matter atrophy and subsequently better cognitive performance [51]. Evidently, the underlying mechanisms of the role of homocysteine in memory performance in older adults are still poorly understood and may deserve more attention.
Our analyses with memory subdomains illustrated that the results for SCD were more closely related to non-verbal memory than verbal memory, and that the magnitude of the association for non-verbal memory was greater than for both immediate and delayed memory. The finding that the results for the full sample were not driven by delayed memory, which is most aligned with progression toward AD dementia, suggests that the homocysteine-memory link is not indicative of incipient AD, a notion also supported by the lack of mediation of this relationship by structural AD pathology. Both tests belonging to the non-verbal memory domain, the BVMT-R and the ROCFT, are measures of visuospatial memory. Therefore, this finding aligns well with the previous finding by our group whereby higher homocysteine was related to poorer spatial navigation performance [28]. The reasons for the presumed association between homocysteine and spatial abilities may deserve additional attention.
Some strengths of the current study include contro-lling for variables that are highly related to cogni-tive performance (age, sex, education), and assessing the influence of B vitamins, creatinine, and cardiovascular risk factors on the association between homocysteine and memory. Although we did not find evidence of a mediating role for entorhinal volume, hippocampal volume, total gray matter volume, or WMLs, our study allowed for examination of these cerebrovascular and structural measures as potential mechanisms through which homocysteine is associated with memory. Further, by including participants with both SCD and aMCI, our study allowed for investigation of whether patterns between homocysteine and cognition differ for diagnostic groups.
There are also some limitations. Unavailability of data on certain vascular risk factors (e.g., hypertension) and other potential mechanisms through which homocysteine may interfere with memory precluded a full examination of alternative pathways explaining the relationship between homocysteine and memory. We also focused on only four measures of structural integrity, which could have limited our ability to detect associations between homocysteine, brain structure, and memory in other regional brain areas associated with AD and memory (e.g., parahippocampal gyrus and retrosplenial cortex). SCD and aMCI were defined based on complaints and cognitive performance rather than including biomarkers, which could contribute to notable heterogeneity within the groups. The current study had a cross-sectional design, preventing investigation of how homocysteine levels may influence changes in memory performance. Finally, the study was limited to participants with SCD or aMCI from a particular memory clinic in the Czech Republic, which could limit generalizability of findings.
Identifying pathways leading to cognitive decline is important in order to reduce the burden of imp-airment on older adults and modifiable risk factors may be especially salient in terms of interventions. Research has shown that contributions to elevated homocysteine include genetic factors—polymorphi-sms on genes related to homocysteine metabolism—as well as lifestyle factors—vitamin intake, sedentary lifestyle, smoking, and drinking behavior [6]. Given that homocysteine has been found to be modifiable through lifestyle intervention [10], our results indicating that higher homocysteine is related to poorer memory provide a promising direction for intervention into cognitive aging, especially when applying before the onset of cognitive impairment. Further, since indicators of brain volume and WMLs did not mediate the association between homocysteine and memory, it may be higher homocysteine is associated with poorer memory via a different, such as cardiovascular, pathway. Specifically, research has found that elevated homocysteine is related to endothelial dysfunction through oxidative stress, may influence vascular functioning by eliciting an inflammatory response, and could be directly neurotoxic by inducing excitotoxicity or compromising the blood-brain barrier [13]. Alternatively, homocysteine may be associated with the build-up of amyloid-β and the hyperphosphorylation of tau, indicating potential interaction with AD biomarkers as the pathway through which homocysteine may be related to impaired memory performance [13]. The lack of an interconnection with brain health markers may mean that targeting homocysteine early in impairment may be an effective intervention strategy.
Future research should include other variables representative of vascular impairment in order to more clearly delineate whether homocysteine is associated with cognition through vascular mechanisms. Investigating additional pathways such as oxidative stress or interaction with biomarkers of AD pathology (amyloid-β and tau) would also provide more evidence for the mechanisms through which homocysteine influences cognition. Future research should also include a longitudinal investigation to determine if homocysteine is related to changes in memory and conversion to MCI and dementia. Relatedly, inclusion of other study populations (cognitively normal, AD dementia) could help inform whether associations between homocysteine and memory depend on level of clinical impairment or study setting (e.g., population-based vs. memory clinic-based cohorts), which was partly indicated through our results.
Conclusion
We found that elevated homocysteine was related to poorer memory performance for the full sample and for participants with SCD and aMCI, although the results were clearly more pronounced with SCD compared to aMCI, suggesting diminishing strength of the relationship with increasing memory impairment. The relationship was not mediated by entorhinal volume, hippocampal volume, total gray matter volume, or WMLs, suggesting that the homocysteine-memory link is driven by another mechanism. The association was not greater in magnitude for delayed memory but rather was represented by immediate, delayed, verbal and non-verbal memory. In participants with SCD, the results were particularly strong for non-verbal memory, which was represented by tests of visuospatial skills. Together, this information seems to highlight that lowering homocysteine levels may be worthwhile in efforts to facilitate cognition in older adults.
Footnotes
ACKNOWLEDGMENTS
This work was supported in part by funds from the University of South Florida Nexus Ini-tiative (UNI) Award, the European Regional Deve-lopment Fund –Project ENOCH (#CZ.02.1.01/0.0/0.0/16_019/0000868), the Ministry of Health, Czech Republic–conceptual development of research organization, University Hospital Motol, Prague, Czech Republic grant 00064203, the Czech Ministry of Health grant NV 18-04-00455, the Institutional Support of Excellence 2. LF UK (#6990332), and the Charles University Grant Agency (GA UK) projects no. 436119, 327821 and 693018 at Charles University, Second Faculty of Medicine. Dr. Nedelska was supported by the International Brain Research Organization –International Society for Neurochemistry (IBRO-ISN) Fellowship, the Czech Alzheimer Foundation, The Ministry of Health of The Czech Republic grant number NV 18-04-00346.