
Abstract
Background:
Recent studies of photobiomodulation (PBM) in patients with cognitive or psychological disorders (including traumatic brain injury, stroke, and dementia) have yielded some encouraging results.
Objective:
In this study, we aimed to investigate the effect of a single stimulation on memory in older adults with mild cognitive impairment (MCI).
Methods:
After PBM, hemodynamic changes, as a measure of functional brain activity, were evaluated using functional near-infrared spectroscopy (fNIRS). Eighteen subjects who met the criteria of MCI were randomly assigned to control and experimental groups. A single real or sham PBM session was administered to the forehead of each patient in the experimental and control groups, respectively. All subjects performed a visual memory span test before and after the stimulation, and their hemodynamic responses during the tasks were measured using fNIRS.
Results:
The results showed that among the MCI subjects, only those who received PBM, but not those who received the sham stimulation, demonstrated significant improvement in the visual memory performance and a reduction in the hemodynamic response during the tasks.
Conclusion:
These findings suggest that PBM may reduce the cognitive efforts needed to complete tasks that require high memory loads, and thus improve the cognitive performance of individuals with MCI.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is considered an intermediate stage between normal aging and dementia, in which older adults with MCI demonstrate subtle cognitive impairment that differs from normal aging but does not meet the criteria of dementia. In these cases, the individuals or their families would note some changes to their cognitive function, such as increased forgetfulness, but the individuals remain capable of functioning independently in their daily lives [1]. The prevalence rate of MCI is approximate 15% –20% in people aged≥60 years. Individuals with signs of MCI have been shown to have a higher risk of developing dementia in the future, and the annual rate at which MCI progresses to dementia has been estimated to range between 8% and 15% [2]. Given that MCI is considered an intermediate stage between normal aging and dementia, early intervention is considered important to delay or even prevent the development of dementia. Several attempts have made to evaluate the effects of pharmacological treatments, including cholinesterase inhibitors [3] and vitamin E [4], on slowing the cognitive decline in subjects with MCI; however, none of them have showed significant effects.
Photobiomodulation (PBM) therapy uses the delivery of light in the visible (400–700 nm) or near-infrared (700–1100 nm) range to stimulate or inhibit biological cell and tissue function [5]. During PBM, the cytochrome c oxidase activities are increased due to near-infrared light absorption, which in turns increase electron transport, mitochondrial membrane potential, and adenosine triphosphate production, and thus boosting oxygen metabolism, utilization rate, and energy production in the cells [6]. In human studies, increased cerebral concentrations of oxidized cytochrome c oxidase, oxygenated hemoglobin, and total hemoglobin [7], and increased strength of electrophysiological oscillations [8] were observed during and after PBM. Together, these results suggested that PBM may improve cell metabolism. Recent studies have tested PBM to patients with cognitive or psychological disorders and have yielded some encouraging results. Early studies on PBM have shown positive effects on patients with traumatic brain injury [9], as indicated by improved executive function, verbal learning, and memory after 18 treatments over the course of 6 weeks. Improvements in cognitive or neurological functioning after PBM were also reported in stroke patients [10–12]. Significant effect has been found in patients with dementia as well. Following a 12-week course of PBM therapy, five patients with mild to moderately severe dementia showed improvements in cognitive performance according to the Mini-Mental State Examination and the Alzheimer’s Disease Assessment Scale [13]. In another study, 11 patients with Alzheimer’s disease showed improved cognitive function (i.e., executive function and memory) after 28 sessions of PBM [14]. Furthermore, a patient with Alzheimer’s disease showed significant improvement in the cognitive functions, as measured by the Montreal Cognitive Assessment and Working Memory Questionnaire, after applying PBM therapy twice daily for 4 weeks [15]. Given these encouraging results of PBM in terms of improving the cognitive functions of patients with traumatic brain injury, stroke, and dementia, the aim of this study was to examine the effect of a single stimulation on the visual memory of individuals with MCI. The hemodynamic response after a single stimulation was examined with the aim of establishing the functional neural changes associated with the improvement of cognitive function after the stimulation.
Functional near-infrared spectroscopy (fNIRS), an optical imaging method that uses light in the near-infrared spectrum (650–950 nm), is a non-invasive means used to monitor the hemodynamic responses evoked by brain activity. fNIRS measures quantitative changes in the concentrations of oxygenated hemoglobin [oxy-Hb] and deoxygenated hemoglobin [deoxy-Hb] in cerebral blood. fNIRS signals have been shown to correlate with the blood oxygenation level-dependent signal, as measured by fMRI. Studies have shown that the hemodynamic level increases as tasks become more difficult [16], indicating that the tasks may require more neural effort from the subjects to perform. Our recent study showed that young adults exhibited a significant reduction in frontal hemodynamic levels during difficult tasks after a single PBM stimulation (Chan et al., unpublished data). Therefore, we hypothesized that PBM could have a positive effect on neural processing and could reduce the amount of effort required to complete cognitive task. A reduction in the hemodynamic response, as measured by fNIRS, needed to complete a difficult task would be anticipated after PBM stimulation, as compared to the baseline measurement.
MATERIALS AND METHODS
Subjects
Twenty-two subjects were recruited through an online advertisement and on campus promotion. The inclusion criteria were no known history of head injury or epilepsy, psychological and/or neuropsychological disorders, or memory and/or other cognitive problem(s). In addition, only subjects who had a score of≥3 on the short memory questionnaire [17], which indicated significant subjective memory complaints, were eligible for participation. All subjects had normal or corrected-to-normal vision during the experiment. The study was conducted in accordance with the Declaration of Helsinki of the World Medical Association Assembly and was approved by the Joint Chinese University of Hong Kong - New Territories East Cluster Clinical Research Ethics Committee. Informed consent was obtained from all individuals included in the study.
The subjects were classified with MCI according to the criteria proposed by the National Institute of Aging-Alzheimer’s Association workgroups [1]; that is, the subjects had self- or informant-reported cognitive complaints, objective cognitive impairment (as measured by neuropsychological assessments), essentially preserved general cognitive functioning, preserved independence in functional abilities, and no known history of dementia. Eighteen of the recruited subjects met these criteria.
The various cognitive functions of the subjects, including verbal memory, visual memory, executive function, and attention, were measured by standardized neuropsychological tests, including the Hong Kong List Learning Test 2nd Edition [18–20], the Rey–Osterrieth Complex Figure Test [21], the Five-Point Test [22], the Chinese Category Fluency Test [23], and the Digit Span [24] and Shape Trail Tests [25].
Materials
Hemodynamic measure
A 16-channel fNIRS system (OEG-SpO2 system; Spectratech Inc., Tokyo, Japan) was used to measure the relative [oxy-Hb] and [deoxy-Hb] changes during visual memory span tasks. Using near-infrared light wavelengths of 770 and 840 nm, the device calculates subjects’ task-related hemodynamic responses based on the modified Beer–Lambert Law [26]. Six pairs of emission and detector probes were arranged in a 2-row×6-column matrix on the forehead of each subject (Fig. 1), with the center of the matrix on Fpz according to the international 10/20 system. The distance between the emission and detector probes was 3 cm, and the sampling rate was 12.21 Hz. The [oxy-Hb] signal was the primary dependent variable because its signal has a stronger relationship with cerebral blood flow than the [deoxy-Hb] signal [27]. To avoid estimation of differential pathlength factor for optical pathlength, we labeled or quantified our results as changes in [oxy-Hb] / (optical pathlength).

Headset of the fNIRS device with 16 probe distribution locations. The fNIRS probes were removed and reset each time.
Photobiomodulation
PBM was applied using a Wisefori 5–3800 model (Wisefor Ltd. Hong Kong). The device contained nine LEDs, which were placed to F7, AF7, Fp1, FpZ, Fp2, AF8, F8, Fz, and Cz according to the international 10/10 system, and emitted 810 nm continuous wave light at an irradiance of 20 mW/cm2. Using a patented design, the device temperature was maintained between 36 and 38°C during stimulation, and the protocol could be adjusted using a smart phone. This device was granted a CE certificate and is registered by the FDA as a Class 1 device. The duration of stimulation was 350 s, which generated a fluence of 7 J/cm2. The subjects in the control group wore the PBM headset, but the device was turned off and had no energy supply. The subjects were blinded to the group assignment.
Procedure
Informed consent was collected from the subjects prior to initiating the experiment. All subjects received the same baseline assessment. During the experiment, the subjects were randomly assigned into two groups: an experimental group (n = 9) and a control group (n = 9). The experimental subjects underwent real PBM stimulation, and the control group underwent sham stimulation. During the experiment, the subjects performed visual memory span tests, followed by a 350 s real or sham stimulation and immediately followed by a repeat of the visual memory span tests. The experimental procedure is illustrated in Fig. 2.
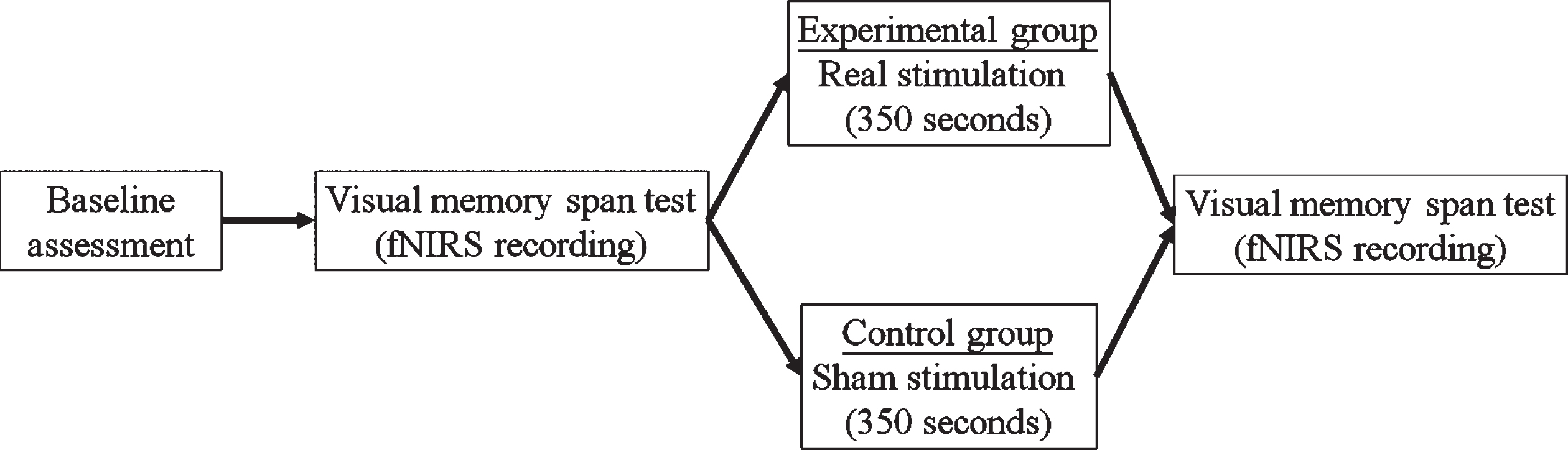
Experimental procedures.
A computerized Corsi block test [28] was used to assess the visual memory of the subjects. The details of this task were described in Claessen, Van Der Ham, & Van Zandvoort’s paper [29]. In this task, each trial started with 9 blue square blocks on the monitor for 1 s. After that, a sequence of blocks turned into yellow with one at each time for 1 s, during which the subjects were required to memorize and then repeat the sequences in the same order as presented by tapping the corresponding blocks with the computer mouse. The task starts with short sequences (i.e., 2 blocks), which then gradually increase in length. That is, in the 2-block condition, there were only 2 blue blocks changed into yellow, whereas 7 blue blocks changed into yellow in the 7-block condition. Each block included two trials, and all subjects underwent all of the trials until a span of 7 blocks was attempted, even if they answered incorrectly in previous trials. The average visual span for a normal individual is approximately 5 blocks [30], whereas patients with brain disorders have been shown to have shorter visual span [31]. The performance was determined by the longest span remembered and the total score (i.e., the longest span remembered×total number of correct trials).
Data analysis
First, independent sample t-tests and chi-square tests were performed to compare two groups at baseline in terms of demographic variables and performance baseline assessment. For the behavioral performance, paired t-tests and chi-square tests were performed to detect within-group improvements. Besides, Pearson’s correlation coefficients were calculated to evaluate the relationship between performance of neuropsychological tests and behavioral improvement of the visual memory test.
For the hemodynamic response, when collecting the fNIRS data, a 0.10 Hz low-pass filter with a slope of 60 dB/octave, was applied to remove high-frequency noise during the task. A correlation-based signal improvement was used to reduce noise based on the negative correlation between [oxy-Hb] and [deoxy-Hb] [32]. The baseline correction was performed by subtracting the overall [oxy-Hb] response from the average [oxy-Hb] before the start of the visual memory task, which lasted for 10 s. The corrected fNIRS response was averaged across spans and subjects. MANOVA was carried out to detect the main effect of the span. A two-way ANOVA was performed to evaluate the group×time interaction. Paired t-tests were performed to investigate the pre-post difference after real/sham stimulation.
RESULTS
Baseline assessment and demographic variables
Independent sample t-tests and chi-square tests were performed to detect any group differences at baseline. There were no significant differences between the groups in terms of demographic variables (p-values = 0.16–0.95), including age, gender, and years of education. Concerning their neuropsychological test performance, both groups performed comparatively (p-values = 0.061–0.95) (Table 1).
Demographic information and neuropsychological test performance of the experimental and control groups
aChi-squared test was performed in evaluating group difference.
Behavioral results
The total scores were calculated by multiplying the longest correct span and the total number of correct trials, and the scores were analyzed using independent and paired t-tests. As shown in Fig. 3, the baseline scores of the two groups were not significantly different (t (16) = 1.0, p > 0.05, d = 0.45). The total scores of the experimental group improved significantly by 29.3% (from 49.0 to 63.3; t (8) = 2.3, p = 0.05, d = 0.75). However, the total scores of the control group only improved by 3.7% (from 57.2 to 59.3), and the difference was not significant (t (8) = 0.3, p > 0.05, d = 0.09). In addition, the number of subjects who showed improvement was significantly different between the two groups; that is, 66.7% of the subjects in the experimental group and only 22.2% of subjects in the control group showed improvement (χ 2 (1) = 3.6, p = 0.05). Consistent results were observed with regard to the longest correct span; that is, the improvement in the experimental group (from 5.1 to 5.9) was significant (t (8) = 2.8, p = 0.02, d = 0.93), but that in the control group (from 5.4 to 5.4; no change) was not (t (8) = 0, p = 1, d = 0).
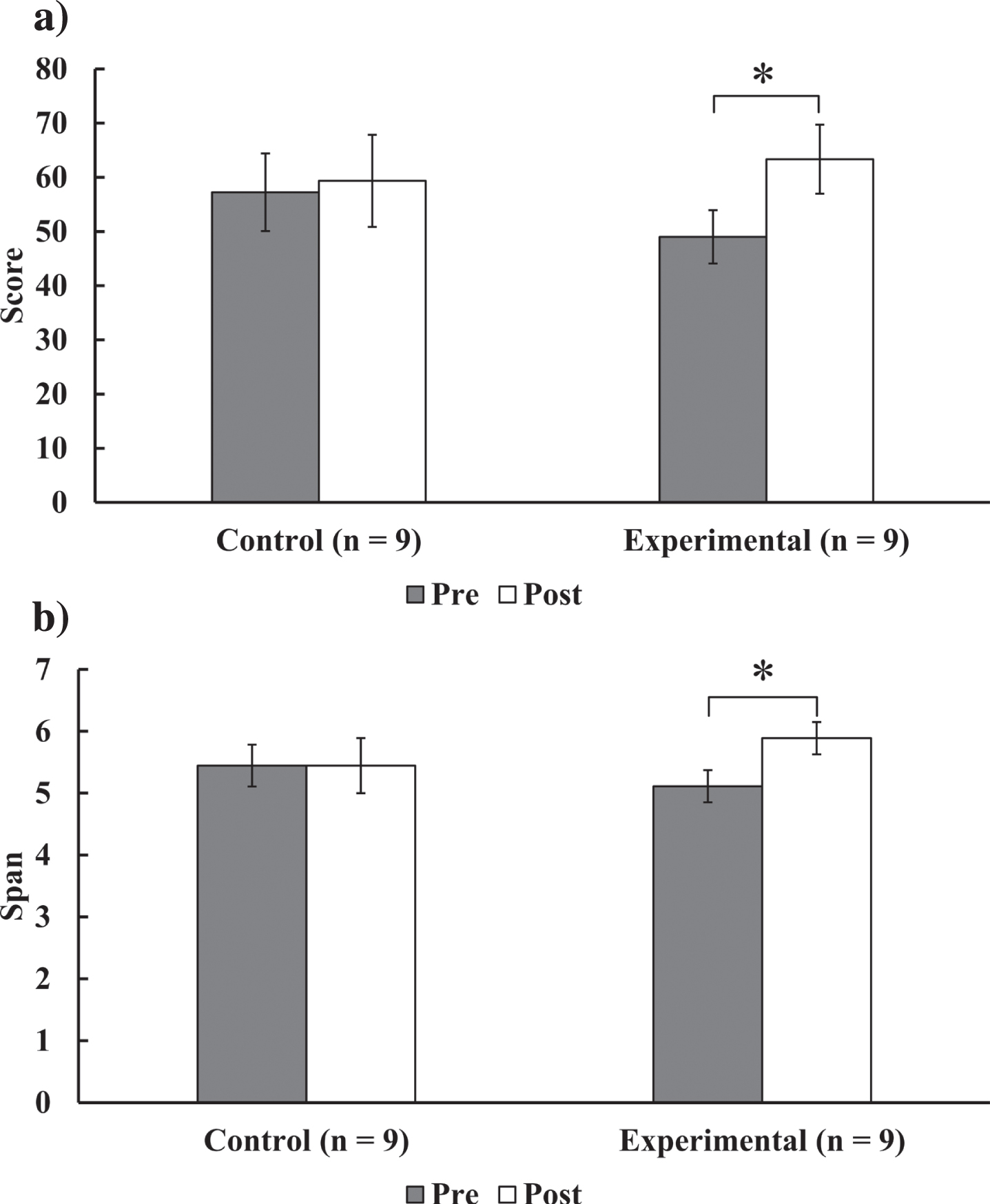
The a) score and b) longest correct span of the computerized visual memory test. Error bars represent one standard error of the mean. *p < 0.05.
A correlation analysis was performed to investigate factors affecting the behavioral improvement after PBM. Pearson’s correlation coefficients were calculated for the correlations between the change in the total scores, the longest correct span of the visual memory test, and the performance on the neuropsychological tests. However, there were no significant correlations between the changes in the total scores and the longest correct span of the visual memory test, and the total learning trials and delayed recall trials of the Hong Kong List Learning Test (p-values = 0.70–0.90), and the copy, immediate, and delayed recall trials of the Rey–Osterrieth Complex Figure Test (p-values = 0.27–0.95).
Hemodynamic response
The fNIRS device was used to measure the hemodynamic responses during the visual memory task. It is known that the more difficult the task, the higher the hemodynamic level required [16], and the latter has been proposed as a measure of mental effort. Consistent with previous studies, individuals with MCI also showed a similar pattern, in which a longer memory span was associated with a higher hemodynamic response in the baseline measure (Fig. 4). There was a significant main effect of the span (F (5, 13) = 10.8, p < 0.001, η p 2 = 0.81), with the [oxy-Hb] during a span of 7 blocks significantly higher than a span of 2 to 6 blocks (p < 0.003, Bonferroni-adjusted).
The mean hemodynamic response across the 16 channels of the baseline and post stimulation (sham/real stimulation) was analyzed using a two-way ANOVA, with the group (experimental, control) entered as the between-subjects factor, and time (pre, post) entered as the within-subjects factor. As shown in Fig. 5, there was a significant group×time interaction (F (1, 16) = 7.1, p = 0.02, η p 2 = 0.31) in a span of 2 blocks. Specifically, the reduction in the hemodynamic response (experimental: –73.8%, control: + 33.2%) was only significant in the experimental group (t (8) = 3.5, p = 0.008, d = 1.18) but not in the control group (t (8) = 0.7, p > 0.05, d = 0.24). Similar results were observed in a span of 7 blocks, in that the reduction in the hemodynamic response (experimental: –31.8%, control: –4.9%) was only significant in the experimental group (t (8) = 3.2, p = 0.01, d = 1.07) but not in the control group (t (8) = 0.4, p > 0.05, d = 0.15). The results were observed across all 16 channels, as shown in Fig. 6. Particularly significant decreases in [oxy-Hb] were observed in 11 channels for a span of 2 blocks (t (8) = 2.4–3.3, p = 0.02–0.04, d = 0.81–1.11), and significant decreases were observed in 6 channels for a span of 7 blocks (t (8) = 2.7–3.6, p = 0.007–0.04, d = 0.84–1.19).
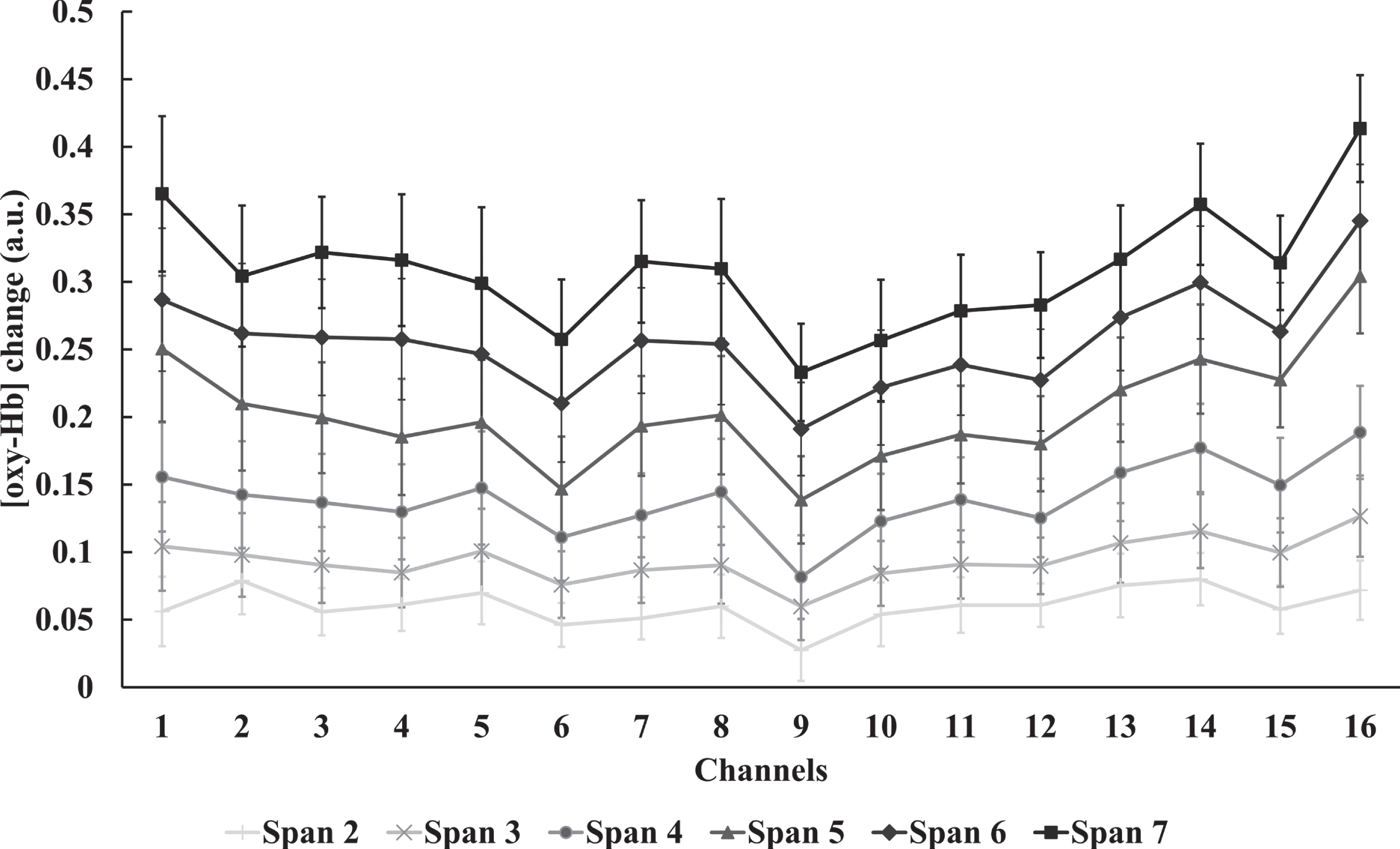
Changes in [oxy-Hb] in different visual memory spans across 16 channels before sham/real stimulation (n = 18). Error bars represent one standard error of the mean.
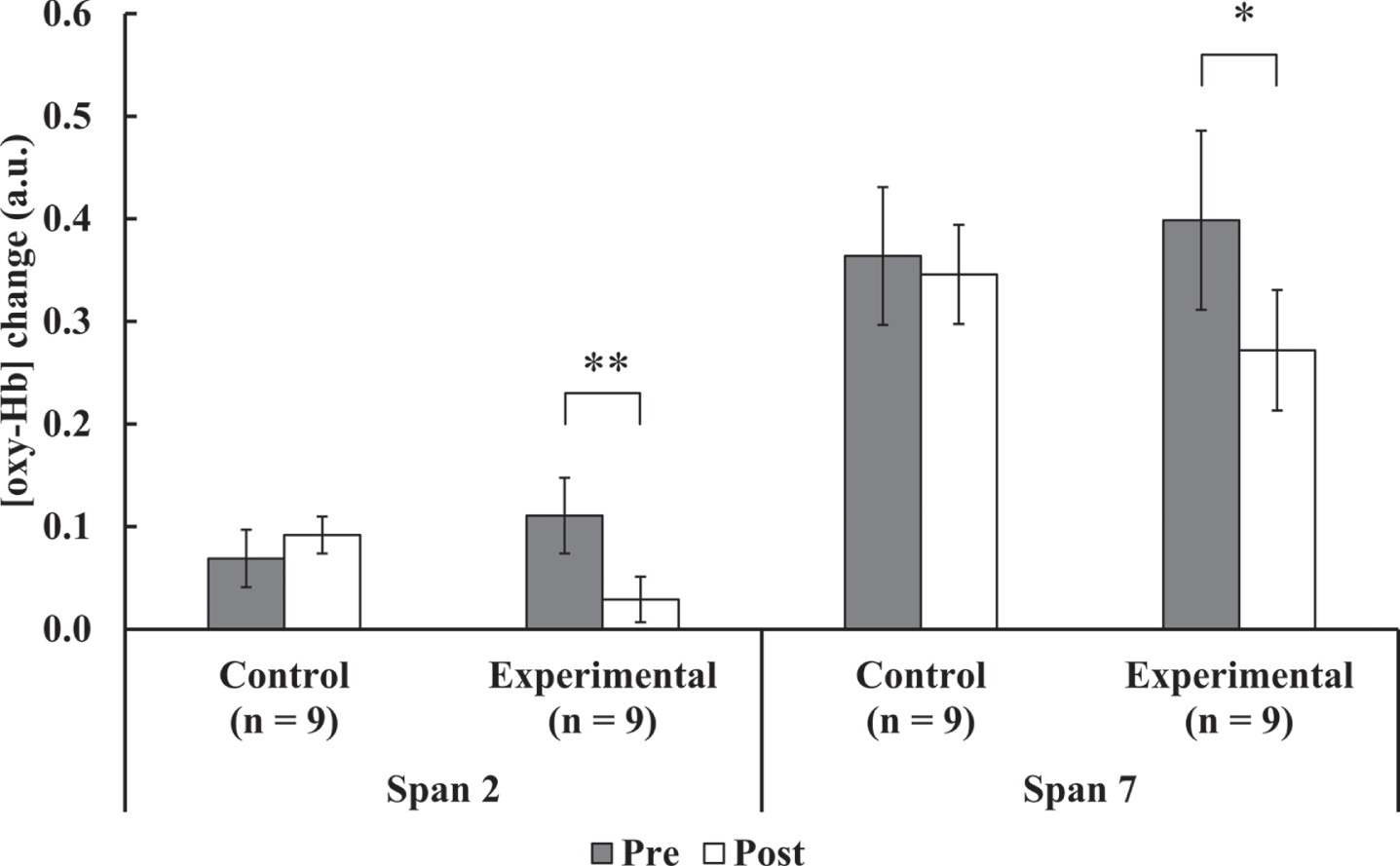
16-channel averaged changes of [oxy-Hb] in a span of 2 (easier) and 7 (harder) blocks before and after sham/real stimulation. Error bars represent one standard error of the mean. *p < 0.05, **p < 0.01.

Changes in [oxy-Hb] in a span of 2 (easier) and 7 (harder) blocks across 16 channels. Error bars represent one standard error of the mean. Asterisks indicate the significance levels of paired t-tests in each group across 16 channels. No correction for multiple comparisons was made. *p < 0.05, **p < 0.01.
DISCUSSION
The findings of this study show that older adults with MCI demonstrated improved visual memory immediately after one PBM stimulation, which led to a reduction in the hemodynamic response associated with the visual memory task. This reduction in the hemodynamic level was observed across all 16 channels over the frontal lobe region. These results suggest that PBM may enhance the efficiency of functional neural activity and may be an underlying mechanism related to the improvement in cognitive/behavioral performance. Given that the study subjects reported memory complaints and demonstrated some signs of mild cognitive impairment, PBM may be a potential intervention for older adults with early signs of cognitive decline. However, further long-term studies are necessary in order to confirm this observation and draw further conclusions.
The present findings are also consistent with those of previous studies that demonstrated the beneficial effect of PBM in improving cognitive function following a single dose of stimulation. Specifically, a group of young adults showed a significant improvement in the learning task category after a single stimulation of 8 min [33], as well as improvements in sustained attention and short-term memory [34]. In our recent studies, young adults showed significant improvements in memory performance (Chan et al., unpublished data) and older adults showed significant improvements in inhibition and verbal fluency after a single dose of PBM [35]. fNIRS was used to compare the hemodynamic change from before to after sham/real stimulation to explore the neural mechanism induced by a single dose of PBM. Our results suggest that young adults exhibit significantly reduced frontal hemodynamic responses during difficult tasks after a single dose of PBM stimulation but not after sham stimulation (Chan et al., unpublished data). This finding is consistent with previous study that older adults exhibited lowered 2-back-related BOLD-fMRI responses after laser stimulation for 5 weeks [36]. Thus, the findings of the present study further improve our understanding of the beneficial effect of single PBM stimulation on cognitive performance. Similar to younger adults, older adults with MCI also demonstrate improvements in visual memory performance after a single dose of PBM stimulation. The significant results of the present and previous studies suggested that lower scalp fluences in the range of around 20 J/cm2 were already effective in case studies for treating patients with traumatic brain injuries and stroke [9, 38].
These results provide further insight into the functional neural processing associated with behavior performance and provide a possible explanation of the neural mechanism by which PBM leads to improved cognitive function. fNIRS was adopted to measure quantitative changes in the concentrations of [oxy-Hb] and [deoxy-Hb] in the cerebral blood, which is an indicator of functional brain activity [16]. Previous fNIRS studies showed an increased [oxy-Hb] and a decreased [deoxy-Hb] in both sides of prefrontal cortex [39] during and after PBM. Apart from increased [oxy-Hb], improvement in functional connectivity in the frontal-parietal network was reported [40]. These findings provided evidence that PBM is able to enhance the metabolic and hemodynamic activity of the brain, which results in increased cerebral blood flow. This process triggers an over-supply of cerebral blood flow to handle the increased oxygen demand, and this change in metabolic activity can be measured by the changes in [oxy-Hb] in the affected brain regions. Therefore, it is conceivable that PBM increases the metabolic activity in the brain, resulting in a decrease in [oxy-Hb] that makes the difficult cognitive task mediated by that region less effortful. Further investigation is warranted to provide additional evidence for this speculation. Biochemical studies such as investigating the production of aldehydes may also help to provide molecular evidence for possible underlying mechanism.
During the experiment, the participants in the experimental group did not verbally report any significant warm sensation, whereas the participants in the control group did not realize that they had a sham stimulation. Therefore, subjects in both groups may not have significant sensational difference perceptually. However, the sham stimulation may not be identical compared to the real stimulation because warm sensation was inevitably generated during the real stimulation process, but the thermal stimulation should not be accounted as the source of behavioral improvement in the experimental group. Since the behavioral improvements were majorly due to the photo-oxidation of cytochrome c oxidase, and thermal stimulation does not alter the concentration of cytochrome c oxidase [41], the behavioral improvements in the present study was less likely due to the temperature increase induced by the PBM, but the real PBM treatment effect itself. However, future PBM studies should be done by carefully controlling the warm sensation of the control group, such as warming the skull slightly but without PBM.
Although the fNIRS system also used near-infrared lights, which has a similar wavelength with respect to the PBM, the reported PBM effects was not likely due to the fNIRS system. According to the technical manual of the fNIRS system, the maximum output power of the six light sources (around 1.27 cm2 each) is 3.8 mW for 770 nm light and 3.4 mW for 840 nm on the surface of the emitters. In addition, each fNIRS recording lasted for around 390 s on average. Therefore, the fNIRS recording delivered a dosage of PBM at around 0.2 J/cm2 for both wavelengths (for 770 nm: 3.8 mW÷6 light sources÷1.27 cm2 each×390 s = 0.19 J/cm2, for 840 nm: 3.4 mW÷6 light sources÷1.27 cm2 each×390 s = 0.17 J/cm2), which was nearly negligible compared to the PBM device in the present study (i.e., 7 J/cm2). Therefore, the possibility of brain stimulation by fNIRS is minimum given the much smaller fluence by fNIRS light versus those used for PBM.
The present study has the following limitations. First, the current recruited sample was relatively small. Future study may investigate whether the results are consistent with a larger sample. Second, since the device was not turned on in the control group, the heat sensation was not comparable between the experimental group and the control group. Third, the long-term effect is still unknow as the present study did only one stimulation section. Apart from the limitations, it is noted that future studies should be cautious in deciding the amount of light energy delivered to ameliorate neurodegenerative diseases as there may be deleterious effects if the light energy is given at high level, although previous PBM studies did not report any sign effects from now.
In conclusion, the present findings provide evidence that PBM improves visual memory and reduces cognitive efforts in completing tasks with higher memory loads, which suggest the use of PBM in treating older adults with MCI.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Samantha Mui, Sophia Sze, Quin Chan, Christy Cheung, and Weltor Hui for their assistance in collecting data for this study. Further, we extend our appreciation to all of the study participants for their assistance in the experiments. This study was supported by funding from the General Research Fund of the Research Grants Council in Hong Kong, granted to the Chinese University of Hong Kong (ASC, 14606519). MRH was supported by US NIH Grants R01AI050875 and R21AI121700.