
Abstract
To assess the predictive value of neuropsychological tests for severe dependency in Alzheimer’s disease as defined by the Equivalent Institutional Care Rating Scale, in a multiethnic, community cohort. The sample included 146 elders from the Predictors 3 cohort. Cox proportional hazard models tested the predictive value of each neuropsychological test at baseline on relative risk of meeting severe dependency. Higher semantic processing and memory test scores at baseline were associated with lower risk of meeting severe dependency in the adjusted Cox models. The integrity of semantic processing and memory abilities in dementia appears to predict time to severe functional dependency.
INTRODUCTION
Neuropsychological tests are a key component of diagnosing Alzheimer’s disease (AD) dementia, teasing apart typical age-related changes from those associated with degenerative disease [1]. It is well established that impairment in episodic memory is a prominent and early indicator of AD [2], evident at both immediate and delayed intervals on memory testing, as well as on recognition testing requiring individuals to discriminate between learned and novel words [1, 3]. These deficits reflect the classic distribution of early AD neuropathology which encroaches upon the medial temporal lobe and hippocampus [2]. Episodic memory loss in early AD is classically accompanied by early degradation of semantic knowledge evident on measures of naming [1, 4] and category fluency [1, 5]. These deficits reflect the degeneration of temporal, but also parietal and frontal cortices associated with the storage of semantic knowledge [1]. As a reflection of the underlying neuropathology, individual neuropsychological tests may hold prognostic value for disease progression, including time to specific disease outcomes.
Functional and cognitive decline, and psychiatric features have been established as defining features of AD, which eventually lead to the dependence of the patient on a formal caregiver or family member [3, 6]. Clinic-based studies have demonstrated the value of assessing AD progression using the Dependence Scale (DS) [2, 6–8], a validated tool representing a wide range of care items required by a patient [8]. Patient dependence measured by the DS has been significantly associated with an increase in informal caregiving time and higher medical costs [7, 8]. The DS has demonstrated comparable associations with markers of disease severity across both clinic and community-based cohorts [2, 9]. One component of the DS in particular, the Equivalent Institutional Care (EIC) rating, appears to offer an unbiased assessment of severe dependency in multiethnic and community-based cohorts [9]. The EIC is divided into categories including limited home care, adult home (supervised setting with frequent assistance in activities of daily living), and health-related facility [10].
Previous work in a highly educated, predominantly Non-Hispanic White, clinic-based cohort has shown that global cognition, orientation, and memory scores derived from the Modified Mini-Mental State Examination (mMMSE) were robust predictors of severe dependency as defined by the EIC [2]. Little is known about whether such predictive value of neuropsychological tests for dependency holds in other ethnic groups, such as Hispanic/Latinos, who are disproportionately affected and exhibit a great amount of disabilities and comorbidities once diagnosed with AD [11]. The current study aims to assess the predictive value of neuropsychological tests for severe dependency in AD as defined by the EIC, in a multiethnic, community-based cohort.
METHODS
Participants were members of the Predictors 3 (P3) Study Cohort, a multi-ethnic, community-based cohort of elders residing in the Northern Manhattan area of New York [10]. The source of community-based participants was from the Washington Heights-Hamilton Heights-Inwood Columbia Aging Project (WHICAP), an ongoing prospective study of aging and AD [10]. Recruitment of the P3 cohort began in 2011 and the follow-up is ongoing. P3 is a subset of WHICAP and recruits elders diagnosed with incident AD, prevalent AD, and those who are at risk for AD, such as those with mild cognitive impairment (MCI). The base population for this study consisted of 292 P3 participants recruited from 2011 to 2019. Eligible participants included those with a baseline diagnosis of incident or prevalent dementia, at least one follow-up visit, and without missing data in the predictors, outcome, and covariates of interest. The covariates used in the adjusted models included: age, gender, ethnicity, education, as well as the Clinical Dementia Rating Scale (CDR) and presence of extrapyramidal signs (EPS). EPS was included as it has been demonstrated to be a robust predictor of dependency [12]. CDR was included as a broad representation of disease stage (mild versus moderate) to be certain that individuals were “matched” for level of disease severity when examining the utility of each neuropsychological predictor; CDR is a predictor of dependency in AD [6, 9]. These selection criteria led to an analytical sample of 146 participants (see Fig. 1).
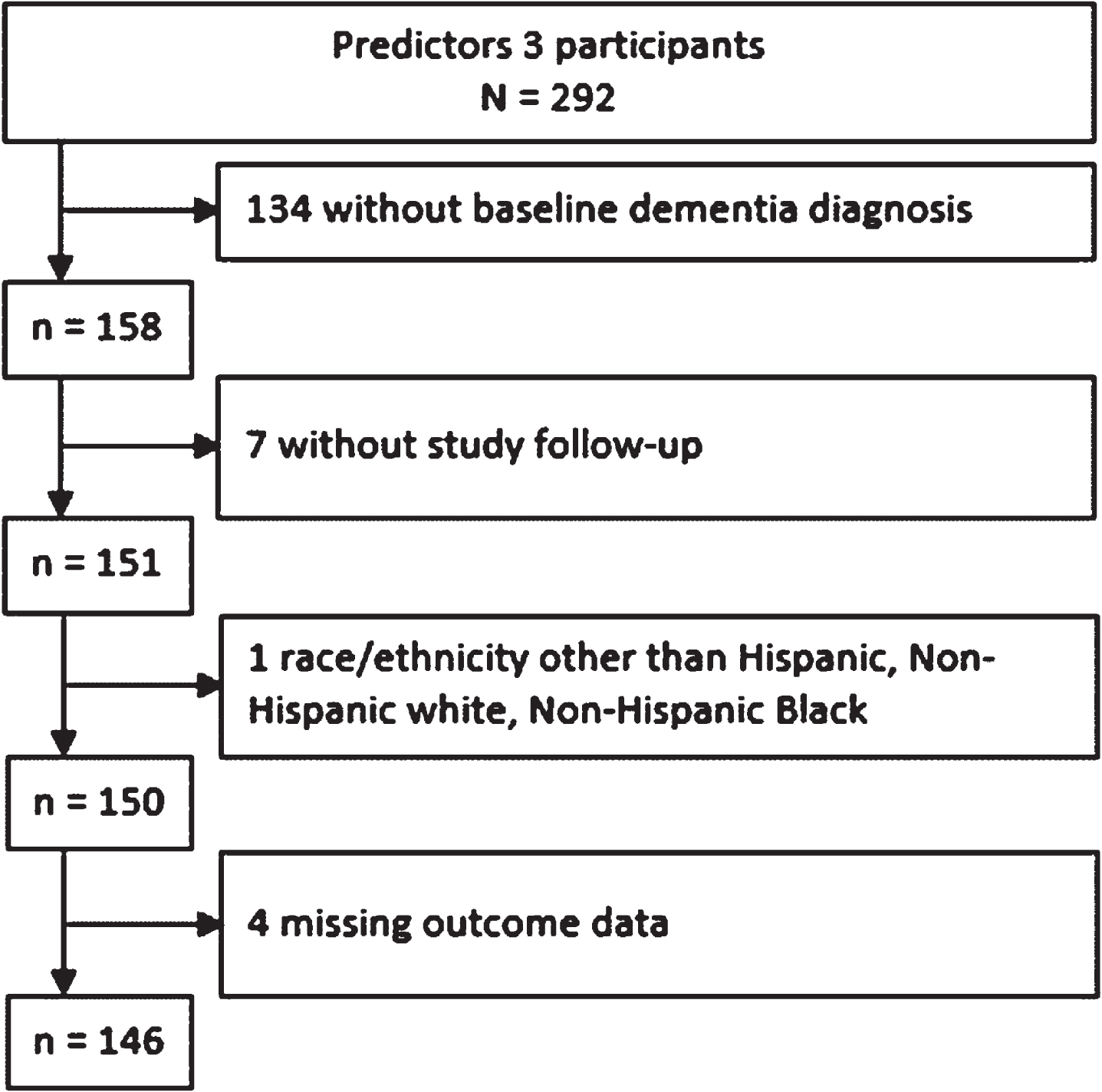
Population flow chart depicting study analytical sample selection.
P3 participants are evaluated annually by trained, bilingual research staff with a comprehensive set of measures and questionnaires including: a neuropsychological test battery, functional, psychiatric, medical, and demographic assessments. During the baseline visit, participants are asked their impression of which language (English or Spanish) would lead to their best performance [10]. The language chosen is then used to administer the baseline visit, as well as each follow up visit. All measures used in the study have been translated into Spanish by a committee of Spanish speakers from the Dominican Republic, Puerto Rico, Cuba and Spain, and then back-translated to ensure validity. Scoring criteria were modified when necessary. Participants were given credit for responses that reflected regional dialects [10]. In addition to evaluating the participant, research staff conduct interviews on the required informant of the participant. The informant may be a family member, close friend, or home health attendant of the participant [10]. Details in respect to P3 assessment methods have been previously published [10]. All P3 participants and informants have signed informed consent for study participation, and the P3 study protocol has been approved by the Institutional Review Board of the New York State Psychiatric Institute.
Participants completed a neuropsychological test battery spanning the following four areas: Semantic Processing (15-item Boston Naming Test (BNT) and Category Fluency: Animals, Food, Clothing); Executive Functioning (Letter Fluency (CFL) and Wechsler Adult Intelligence Scales-Revised (WAIS-R) Similarities subtest); Memory (Selective Reminding Test (SRT), a serial list learning task consisting of recall and recognition components); and Visuospatial (5-item Rosen Drawing Test) [13]. Additionally, participants were assigned an EIC rating as part of the Dependence Scale at each annual visit [10]. EIC endpoint was defined as reaching a score of 3 on the EIC (patient needing health-related facility) [10]. Participants were assessed for level of everyday function using the Clinical Dementia Rating (CDR) scale and for presence of EPS.
Individual Cox models were used to determine the predictive value of each neuropsychological test at baseline on relative risk of meeting severe dependency defined by the EIC rating. Years from initial visit until the last visit was used as the time variable for those who did not meet the EIC endpoint, or until the onset date of meeting EIC otherwise. Cox analyses were adjusted for baseline age, gender, ethnicity, education level, presence of EPS, and CDR score. Taking into consideration that the study sample is predominately Hispanic/Latino, we ran sensitivity analyses to assess a potential interaction by Hispanic/Latino ethnicity by fitting unadjusted cross-product models for each predictor by ethnicity.
RESULTS
Table 1 shows baseline characteristics and study endpoints by EIC status. The analytical study sample included 146 elders diagnosed with AD and enrolled in the Predictors 3 cohort with a mean age of 85 years, and an age range between 70–104 years of age at baseline. Participants were seen for annual study visits with a mean follow up time of 3.30 years. 74 participants did not reach the EIC endpoint status, and 72 participants reached the EIC endpoint. 125 out of 146 (86%) participants were Hispanic/Latino, 119 were female (82%), and 108 (74%) had an education of 0–8 years. Place of birth of the study sample was predominately the Dominican Republic (67%), followed by the United States (12%), Other (12%), and Puerto Rico (9.7%). Regarding testing language, 81%of participants were tested in Spanish. 65%of participants were monolingual Spanish speaking, speaking no English at all. Previous work provides empirical evidence to support the premise that the neuropsychological tests used in the study measure equivalent cognitive constructs in the English and Spanish language [13].
Baseline Characteristics by Equivalent Institutional Care Rating (EIC) endpoint status
AD, Alzheimer’s disease; Hisp., Hispanic; Mos., Monthly; CDR, Clinical Dementia Rating Scale; EPS, Extrapyramidal Sign; SRT, Selective Reminding Test; HS, High school; 1Statistics presented: Median (IQR); n (%); 2Statistical tests performed: Wilcoxon rank-sum test; chi-square test of independence; Fisher’s exact test.
Table 2 shows both the unadjusted and adjusted Cox proportional hazard models. Each row shows in turn the results for a one-point increase in each predictor of interest for unadjusted Cox and adjusted models for the risk of reaching the EIC outcome. We ran all Cox models with the individual neuropsychological predictors by ethnicity interaction term, and none were significant (p > 0.05). Better performance in neuropsychological assessments measuring memory and semantic processing predicted lower risk of meeting severe dependency in the adjusted Cox models (BNT (hazard ratio (HR1) = 0.90, 95%CI [0.81, 0.99], p = 0.036), Category Fluency (HR1 = 0.83, 95%CI [0.75, 0.91], p < 0.001), SRT Delayed Recall (HR1 = 0.81, 95%CI [0.66, 0.99], p = 0.044), and SRT Recognition (HR1 = 0.88, 95%CI [0.80, 0.97], p = 0.011). The assessments measuring Executive Functioning (Letter Fluency and WAIS-R Similarities) and Visuospatial (5-item Rosen Drawing Test) scores were not statistically significant predictors for the risk of reaching the EIC outcome.
Cox Proportional Hazard Model results
1HR, Hazard Ratio; CI, Confidence Interval; SRT, Selective Reminding Test. All adjusted models adjusted for age, gender, ethnicity, education, presence of extrapyramidal signs, and Clinical Dementia Rating Scale.
DISCUSSION
Neuropsychological assessments are essential for the differential diagnosis of AD dementia [1–5] and have predictive utility for disease progression and mortality [2, 5]. There is a deficit in the literature on robust neuropsychological predictors of severe functional dependency in diverse cohorts. The importance of assessing these relationships in multiethnic, community-based cohorts should be emphasized.
The current study found that relatively preserved semantic processing and memory abilities in dementia is associated with a reduction in risk of severe dependency in a community-based, multiethnic cohort of elders diagnosed with AD. These results are consistent with the literature demonstrating that both semantic processing and memory can help predict the progression of AD [2, 4], and extend knowledge regarding predictors of disease outcomes to a multiethnic community cohort. From a clinical standpoint, it is informative to compare the effect of these cognitive scores to that of age on the risk for severe dependency. In our study, a one-year increase in age has a HR of 1.04 (p = 0.05), such that for every year older at baseline, individuals have a 4%higher chance of developing severe dependency. In comparison, for each one-point increase in naming scores, there is a 10%reduction in risk of developing severe dependency, similar to the magnitude of risk reduction for being 2.5 years younger at baseline. Interestingly, these results diverge from work demonstrating that disproportionate executive dysfunction predicts mortality in a similar cohort [5], perhaps suggesting that the disease mechanisms which contribute to severe dependency and mortality are not one in the same. Future research should further examine the differences in neuropsychological predictors of dependency versus mortality in AD.
Certain limitations should be noted. The neuropsychological battery used in the study was relatively limited in scope. Perhaps a broader set of measures might have allowed us to see relationships between severe functional dependency and other cognitive domains. Additionally, we were not able to control for duration of illness in the analyses; however, disease stage was included as a covariate in the models (mild, moderate, or severe), allowing the examination of cognitive scores independent of severity. Third, we cannot rule out the possibility of type I error given that we ran 8 independent models. However, the fact that the four significant findings hang together within the domains of memory and semantic functioning suggest that the statistically significant results were not random. Finally, we did not have a large enough sample size, and a sufficient distribution of race and ethnicity to fully explore the extent to which neuropsychological predictors of dependence may vary as a function of these demographic characteristics. A sensitivity analyses suggested that findings were not significantly different in Hispanic versus Non-Hispanic participants; however, further work in a larger cohort is needed in this regard to more fully articulate potential differences in disease outcomes.