
Abstract
Background:
Dementia is one of the costliest diseases for health care systems with growing importance for policy makers.
Objective:
The aim of this study is to systematically review the current literature of excess cost studies for dementia and to analyze excess costs in a meta-analysis.
Methods:
A systematic literature search was conducted in PubMed, EconLit, NHS-EED, and Cochrane Library. 22 studies were included and assigned to one of three subgroups according to the time period that they analyzed during disease progression: the time of diagnosis, the time between diagnosis and death, and the time prior to death. Excess costs were analyzed using the ratio of means (ROM) and meta-analysis was performed by pooling ROMs in a random effects model.
Results:
Total costs were significantly higher for demented persons compared to non-demented persons at the time of diagnosis (ROM: 2.08 [1.71, 2.54], p < 0.00001, I2 = 98%) and in the time period between diagnosis and death (ROM: 2.19 [1.97, 2.44], p < 0.00001, I2 = 100%). The ROM was highest for professional home care (ROM: 4.96 [2.62, 9.40], p < 0.0001, I2 = 88%) and for nursing facilities (ROM: 4.02 [2.53, 6.40], p < 0.00001, I2 = 100%) for the time period between diagnosis and death.
Conclusion:
This meta-analysis is the first to assess excess costs of dementia by the ROM method on a global scale. We conclude that our findings demonstrate that costs of dementia constitute a substantial economic burden.
INTRODUCTION
Dementia is a syndrome in which a person’s cognitive abilities decline irreversibly and impair a person’s ability to perform activities of daily living independently [1]. The causes of dementia are manifold, the most frequent being Alzheimer’s disease, vascular dementia, dementia with Lewy-bodies, and Parkinson’s disease dementia [2]. More rare causes of dementia include prion diseases, frontotemporal dementia, Huntington’s disease, and many other conditions [3]. Dementia can be diagnosed if one of six of the following cognitive faculties defined in the Diagnostic and Statistical Manual of Mental Disorders is significantly impaired: complex attention, executive functioning, learning and memory, language, perceptual-motor functioning, and social cognition [1]. The severity of symptoms and need for assistance with activities of daily living increase in the time leading up to death.
Dementia is one of the costliest diseases for health care systems with an estimated total global cost of 818 billion US dollars with 46.8 million people being affected in 2015 [4]. It is estimated that the prevalence will double approximately every 20 years and will reach 74.7 million by 2030 [5]. This data indicates that the estimation of the costs of dementia is and will in future be of utmost importance for policy makers and health care officials.
Cost-of-illness (COI) studies have become an important tool to estimate the burden of disease in the health care sector. According to Byford et al., cost-of-illness studies aim to measure the entire costs for a disorder [6]. COI studies provide information on the total socioeconomic burden of a disease and can moreover provide detailed information which cost categories produce the highest expenditures. This can determine the allocation of research funds and highlight inefficiencies in health care systems [6].
In COI studies, costs can be classified as either direct, indirect, or intangible costs. Direct costs include expenditures for the treatment, cure, and rehabilitation of a diseased person, while indirect costs can be defined as forlorn revenue through lost productivity by the diseased person or their caregivers. Intangible costs can be described as a loss of quality of life (QoL) of the person with dementia or his caregivers [7]. They can be quantified with multidimensional QoL-instruments or willingness to pay analyses and are challenging to translate into monetary terms [8,9, 8,9]. Although measuring the entire costs of dementia, including direct, indirect, and intangible costs, would be ideal only few studies encompass indirect costs and literature on intangible costs of dementia is even scarcer.
Excess costs are an economic concept for assessing the burden of a disease in a population with other comorbid diseases, impairments, and age-related handicaps that also induce health care costs. The outcome measure for excess cost studies is the difference in mean costs for the group of people with the disease of interest and mean costs for a reference group without the disease that ideally is a matched cohort. Especially for diseases with a high rate of comorbidity (e.g., depression or other psychiatric conditions) or diseases of the elderly population (e.g., dementia or Parkinson’s disease) excess costs have been proven to be an accurate concept for cost-of-illness studies [10–12]. Furthermore, the ratio of means (ROM) has been proposed as an effect-measure for meta-analysis of COI studies reporting excess costs [12]. ROM is a meta-analytical effect measure for continuous outcome variables. It is calculated as the log of the ratio of means between the group with the disease and the reference group and can be aggregated over studies. ROM can be interpreted as the percentage difference in outcome (i.e., costs) between the group with the disease and the reference group used for comparison. The major advantage of ROM against other meta-analytical approaches for the aggregation of health care cost data is to rely on the relative difference between two samples instead of absolute differences. This method allows to pool studies with different outcome units, which is of particular interest when pooling cost data. The frequent observation that absolute cost values reported in different disease-specific COI show cross-study variation of up to several orders of magnitude can be ascribed to heterogeneity in the outcome units (i.e., cost categories) reported. Using ROM allows to aggregate cost data from different COI by circumventing this heterogeneity. For our purpose we therefore chose to assess the economic burden of dementia by applying the concept of ROM on eligible excess COI studies. To our knowledge, this meta-analysis is the first to assess excess costs of dementia by the ROM method.
COI studies can be conducted from numerous different perspectives. In broader terms, COI studies can be conducted from a societal, a patient’s, or a payer’s perspective [13]. From a payer’s perspective, data on costs are often acquired from insurance companies or health care providers. Therefore, indirect costs are often not reported in these studies. Studies conducted from a societal perspective include cost data from patients and payers and also encompass indirect costs incurred by informal care and lost productivity. For our meta-analysis, we included studies from a societal perspective as well as from a health care payer’s perspective.
Since dementia is a progressive illness that accompanies affected persons until their death, we analyzed the costs of disease for different time periods during disease progression: the time of diagnosis, the time between diagnosis and death and the time period prior to death.
In summary, the purpose of this study was to conduct a meta-analysis of existing excess COI studies from a societal or payer’s perspective as to establish a reliable source for the ROM of costs of people with dementia (PWD) compared to people without dementia (PWOD) at different time periods of disease progression.
METHODS
This meta-analysis was based on the PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses [14]. A systematic literature search was conducted in April 2020 in PubMed, EconLit, NHS-EED, and Cochrane Library. The search string ((dement* or “cognitive impairment” or Alzheimer*) and (cost* or economic* or expenditure* or financial* or spending* or “burden of illness” or “burden of disease”)) was applied for Boolean search in all before mentioned databases. 4,773 results were found in the initial search; additionally, 17 articles were identified through hand-searching cross-references. A detailed description of the search strategies for each database is provided in the Supplementary Material and displayed in Table 1.
Table1
Titles and abstracts were screened for relevance. Studies that clearly did not concern COI for dementia were excluded in the first screening. Full-text examination followed using the following selection criteria which were adapted from a previously published meta-analysis on the excess costs of depression [12]. A detailed elaboration of the exclusion and inclusion criteria is provided in Supplementary Table 1.
Studies were considered eligible if they met the following inclusion criteria: The article had been peer-reviewed and an abstract written in English or German was available. No limitations were imposed regarding the region, sample size of the studies, or the diagnostic criteria they used. The article was published between April 1, 2010 and March 31, 2020. The study population included people of all ages that had been diagnosed with dementia (Alzheimer’s disease, dementia with Lewy-bodies, Parkinson’s disease dementia, vascular dementia or other). The study was conducted from a payer’s or a societal perspective. To analyze the excess costs of dementia studies had to compare a demented group (D) to a non-demented group (ND). Controls had to be selected from an “average” population except for the case of Parkinson’s disease dementia where controls had to have Parkinson’s disease. Total cost studies as well as studies focusing on a specific cost category were included. The study’s primary objective was to determine costs caused by dementia which had to be reported in mean costs per person for a specified time.
Studies were not considered eligible if they met the following exclusion criteria: Cost effectiveness studies, studies comparing different treatments, other interventional studies, cost-minimization studies, short reports, protocols, reviews, commentaries or editorials were not included. Studies that included persons diagnosed with mild cognitive impairment were excluded. Studies that only reported log mean, median, mean difference or modelled costs were not included.
Included studies were assigned to one of three subgroups according to the time period that they analyzed during disease progression: the time immediately following diagnosis, the time between diagnosis and death and the time prior to death. Studies were analyzed in the subgroup analysis for the time around diagnosis if they included subjects one year prior until one year after diagnosis. Studies were analyzed in the subgroup analysis for the time around death if they included subjects one year before death. All studies that did not define a specific time frame between diagnosis and death were analyzed in the subgroup analysis for the time between diagnosis and death.
We defined cost categories for the different types of costs that were reported in the articles: total costs, inpatient costs, outpatient costs, medication costs, costs for emergency room visits, costs for nursing facilities (NF), costs for professional home care (PHC), and costs for informal care. Year of pricing, currency and time interval of costs were extracted. If year of pricing was missing it was assumed to be the last year of the recruitment period. Costs were annualized, inflated to the year 2019 utilizing consumer price indices and converted to US dollars utilizing purchasing power parities (PPP). Mean annual costs in 2019 US dollar PPP are provided in the supplementary material (Supplementary Table 2).
We used ROM as an effect measure for meta-analytic aggregation which is calculated by dividing the mean costs for demented persons by the mean costs for non-demented persons. Using a ratio instead of absolute numbers shall allow a more accurate comparison of costs between studies originating from different countries with different GDP and currencies.
We used Excel Version 16.37 and Review Manager 5.3 for all calculations and plots. ROM and standard error were calculated and log-transformed in Excel. Unadjusted means were used if adjusted means and unadjusted means were both reported. Data then was pooled using generic inverse variance weighting in a random-effects model [15]. To calculate the 95% confidence interval for each ROM, a standard deviation of the costs for each group is needed. Missing standard deviations were imputed using the highest standard deviation of the studies that were included in the respective subgroup analysis [16]. For the calculation of total costs in the time period before death, we imputed the standard error from the sub-analysis of the time between diagnosis and death, since no study that had been conducted at the time around death reported standard deviations. We proceeded likewise with the analysis of inpatient and outpatient costs from studies that had been conducted at the time around diagnosis.
For visualization, pooled results of ROM and 95% confidence intervals were back transformed to non-logarithmic values and presented in forest plots as described by Friedrich et al. [17]. Study heterogeneity was evaluated using I2 statistics [18]. We performed meta-analyses for total costs, inpatient costs, outpatient costs, medication costs, professional home care costs, nursing facility costs, emergency room visit costs, and informal care costs separately.
A quality assessment of all included studies was conducted following the checklist published by Stuhldreher et al. [19] and can be found in Supplementary Table 3.
RESULTS
Search strategy
4,773 records were identified in a systematic screening of databases. 17 additional records were found in cross-references of studies. 91 duplicates and 2 non-English, non-German records were excluded before screening. 4,697 records were screened by title and abstract. 382 full-text articles were assessed under the inclusion criteria (see Fig. 1 and Table 1). Three studies were not included since participants were examined short term in a hospital setting and costs were only measured for the duration of the hospital stay and no data on average annual costs for the demented and non-demented group was compared (Ahern et al. [20], Annear et al. [21], and Husaini et al. [22]). This was not compatible with our inclusion criterion “Controls had to be selected from an “average” population except for the case of Parkinson’s Disease Dementia where controls had to have Parkinson’s disease”. 22 studies were included in a qualitative and quantitative synthesis for meta-analysis [23–44].
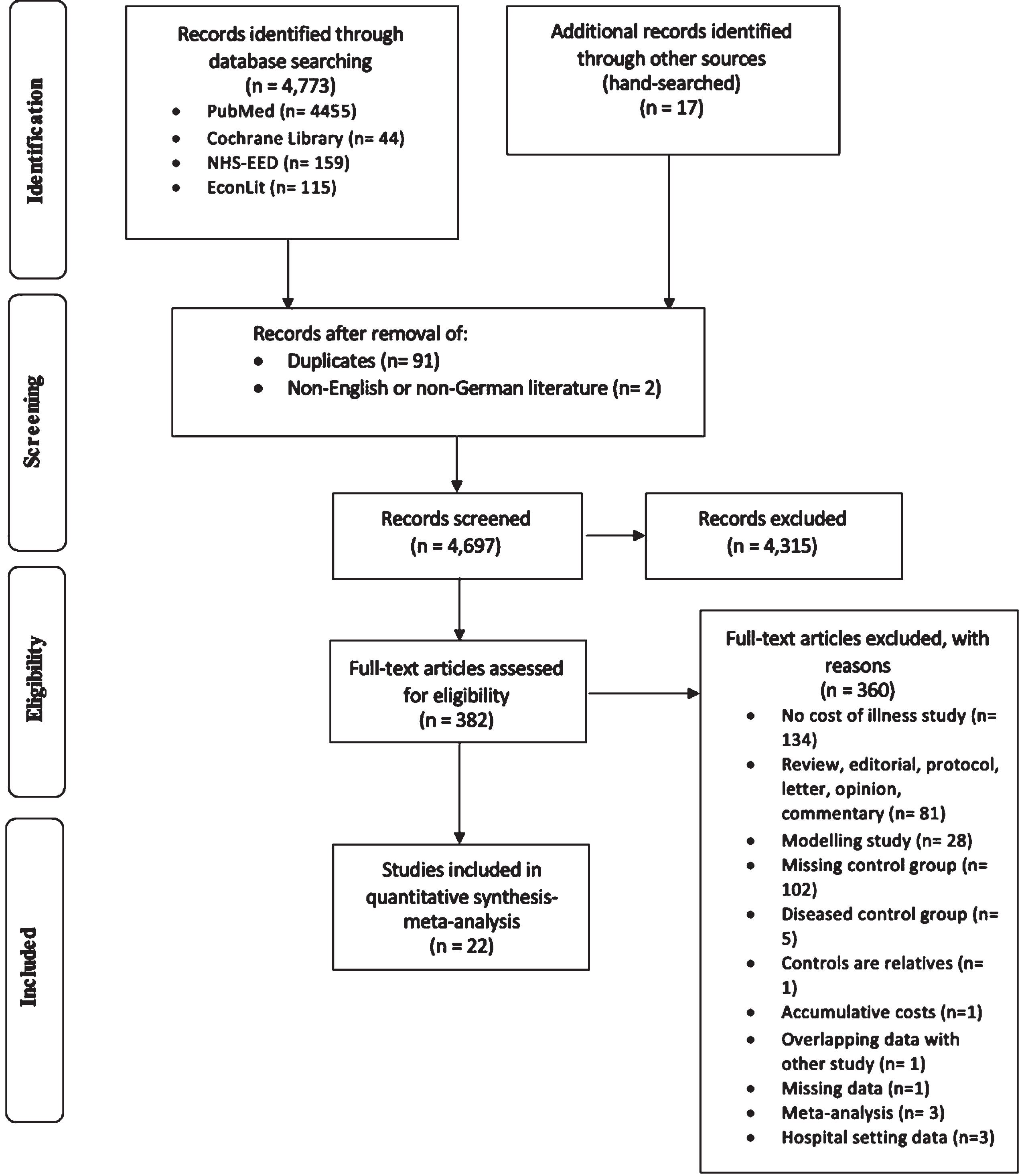
PRISMA Flow diagram.
General characteristics
Information retrieved from each study included 1) study characteristics (author, year, country, source of data and study perspective) and 2) sample characteristics (study population, age range, mean age, type of dementia, diagnostic instrument, diagnostic criteria, care setting, characteristics of controls, and sample sizes) and is depicted in Table 2.
General study characteristics
D, dementia; ND, no dementia; n/d, no data; RAI RUG, Resident Assessment Instrument Ressource Utilisation Groups; LBD, dementia with Lewy bodies; FTD, frontotemporal dementia; VaD, vascular dementia; AD, Alzheimer’s disease; NOS, not otherwise specified; NHI, National Health Insurance; FFS, Fee-for-service; ADRD, Alzheimer’s disease and related dementias; EMR, Electronical medical record; MEPS, Medical Expenditure Panel Survey; ADAMS, Aging, Demographics, and Memory Study; HSM, Handicap Santé Ménages; WHICAP, Washington Heights-Inwood Columbia Aging Project; MAPD, Medicare Advantage Prescription Drug; MEDALZ, Medication use among persons with Alzheimer’s disease; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer’s Disease and Related Disorders Association; ICD-10-GM, International Classification of Diseases 10 German Modification; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders IV. *We only used data for dementia (all types) in this meta-analysis. † Daras et al. did not report a sample size however they reported number of observations in their survey of five waves of data. ‡ We only used data for AD in this meta-analysis. §Daras et al. did not report a sample size however they reported number of observations in their survey of five waves of data. II We only used data for general dementia in this meta-analysis.
Description of general study characteristics
Time period
Five studies were conducted following the time of diagnosis [23–27]. 15 studies were conducted between diagnosis and death [30–44]. Three studies of which two were subdivided into two subgroups analyzed costs of dementia prior to the death of participants [28–30]. Daras et al.’s longitudinal study provided data on the time period between diagnosis and death and the time period before death [30]. In the time around diagnosis, data included from the longitudinal studies of Suehs et al. [23] and Taipale et al. [24] was retrieved for the first half year of diagnosis, data from Lin et al. [25] and Sopina et al. [26] was retrieved for the first year following diagnosis, and data from Brüggenjürgen et al. [27] was retrieved for the first quarter post-diagnosis. In the time around death, data included from the longitudinal study of Crouch et al. [28] data was retrieved for the last six months before death, and data from Pyenson et al. [29] and Daras et al. [30] was retrieved for the year of death.
Year of data/country
Year of data collection ranged from 1997 [37, 43] to 2018 [38]. 10 studies were conducted in North America ([23, 44], nine in Europe [24, 43], one in Australia [38], one in Argentina [41], and one in Taiwan [35].
Data source/age
Most studies were based on claims data (n = 10; [23, 42]), primary data (n = 5; [31, 43]), or a combination of those (n = 5; [30, 44]). Most studies included study participants without limitations to age (n = 8; [24, 43]) or limited their sample to participants aged over 65 years (n = 7; [25, 44]). 9 studies did not report mean age [24, 39]. Mean age was lowest in Rojas’s study (AD: 69.7 (SD: 5.1) years; ND: 68 (SD: 7.8) years) [41] and highest for the diseased group in Pyenson’s study (AD: 86) [29] and for the control group in Leicht’s study (84.74 (SD: 3.21) years) [40].
Study perspective
In this meta-analysis, we chose to include studies from a payer’s perspective and a societal perspective.
The different terms used for study perspectives are manifold [38]. Some studies chose a narrower perspective than others. Gnanamanickam et al. reported from a “broad health and social care provision perspective” [38], Leicht et al. reported from a “societal perspective” [40], Paraponaris et al. reported from a “society perspective” [31], Schwarzkopf et al. reported from a “payer perspective” [42], Vossius et al. reported from a “societal point of view” [43], Brüggenjürgen et al. reported from a “perspective of a SHI (Statutory Health Insurance)” [27], and Sopina et al. reported from a health system perspective [26]. We assigned all studies to a payer’s or a societal perspective (see Table 2). Studies that did not specifically state which perspective was applied but that were clearly reported from a societal or a payer’s perspective and not a patient’s perspective only were also included.
Disease and diagnostic criteria
Four studies were limited to Alzheimer’s disease [23, 27], and one study examined costs in Parkinson’s disease dementia [43]. In the study by Vossius et al., costs for a group of people with Parkinson’s disease were compared to costs for a group of patients with Parkinson’s disease and Parkinson’s disease dementia [43].
Rojas et al. compared costs for people with Alzheimer’s disease, frontotemporal dementia, and vascular dementia with healthy subjects [41]. Since there was only one group of healthy subjects to compare data with, we only included data for the group of people with Alzheimer’s disease in this study. Chen et al. reported costs for dementia (all types), Alzheimer’s disease, Lewy body disease, frontotemporal dementia, vascular dementia, other/classified elsewhere/NOS/mixed and one non-demented control group [34]. Here, we compared demented (all types) to non-demented participants. Pyenson et al. reported costs for Alzheimer’s disease, general dementia, and a non-demented control group [29]. Here, we chose to compare general dementia to the non-demented control group.
Diagnosis reported in medical records from insurance companies or health care providers were most frequently used as a diagnostic instrument (n = 16; [23–30, 42]), followed by in-person physician diagnosis (n = 6; [33, 44]) and self- or proxy-reports (n = 2; [30, 31]). ICD-Code was the preferred diagnostic criterium in most studies.
Study setting
Two studies only included people living in residential care [33, 38], five studies only included community-dwelling people [26, 44], and Daras et al.’s study compared a cohort of persons from both settings [30]. Crouch et al. compared costs of a group of people living in a rural area with costs of a group of people living in an urban area [28]. When two different cohorts were given, we included both cohorts as separate studies in this meta-analysis.
Controls/Total number of participants
In total, 6,172,081 subjects participated in the included studies of which 785,394 were demented and 5,386,687 were controls, not including the number of participants from Daras et al.’s study since they were not reported [30].
Quality assessment
We conducted a quality assessment for each of the included studies in which we used criteria adapted from König et al. and Stuhldreher et al. [12, 19]. Of all criteria from the quality assessment studies fulfilled 84% on average. The least frequently fulfilled criteria were reporting of missing data (27%, see Supplementary Table 3) and study perspective (32%).
Cost categories
We analyzed eight different cost categories in our meta-analysis: total costs, inpatient costs, outpatient costs, medication costs and costs for nursing facilities, professional home care, emergency room visits, and informal care. Table 3 illustrates which cost categories were included by each study. All studies that were included in this meta-analysis are listed herein with their year of pricing, currency, and time period for costs. Other cost categories that were not included in this meta-analysis were for example hospice costs [25, 34]. Hospice costs were not comparable to another since all three studies were conducted at different times after diagnosis.
Cost Assessment
¶Costs for emergency room visits and outpatient costs were combined. ** Costs for hospitalizations, medical assistant visits and paid caregivers were zero for the control group. †† Year of pricing is assumed to be the last year of the recruitment period
Forest plots of costs around time of diagnosis (ROM, 95% CI).
Forest plot of costs around time of death (ROM, 95% CI).
Paraponaris et al. and Leicht et al. were the only investigators to assess costs of informal care in a cohort study [31, 40]. They used both replacement method and opportunity cost method to value informal care. We analyzed their data on informal costs that had been calculated using the replacement method.
Forest plots
Time period between diagnosis and death
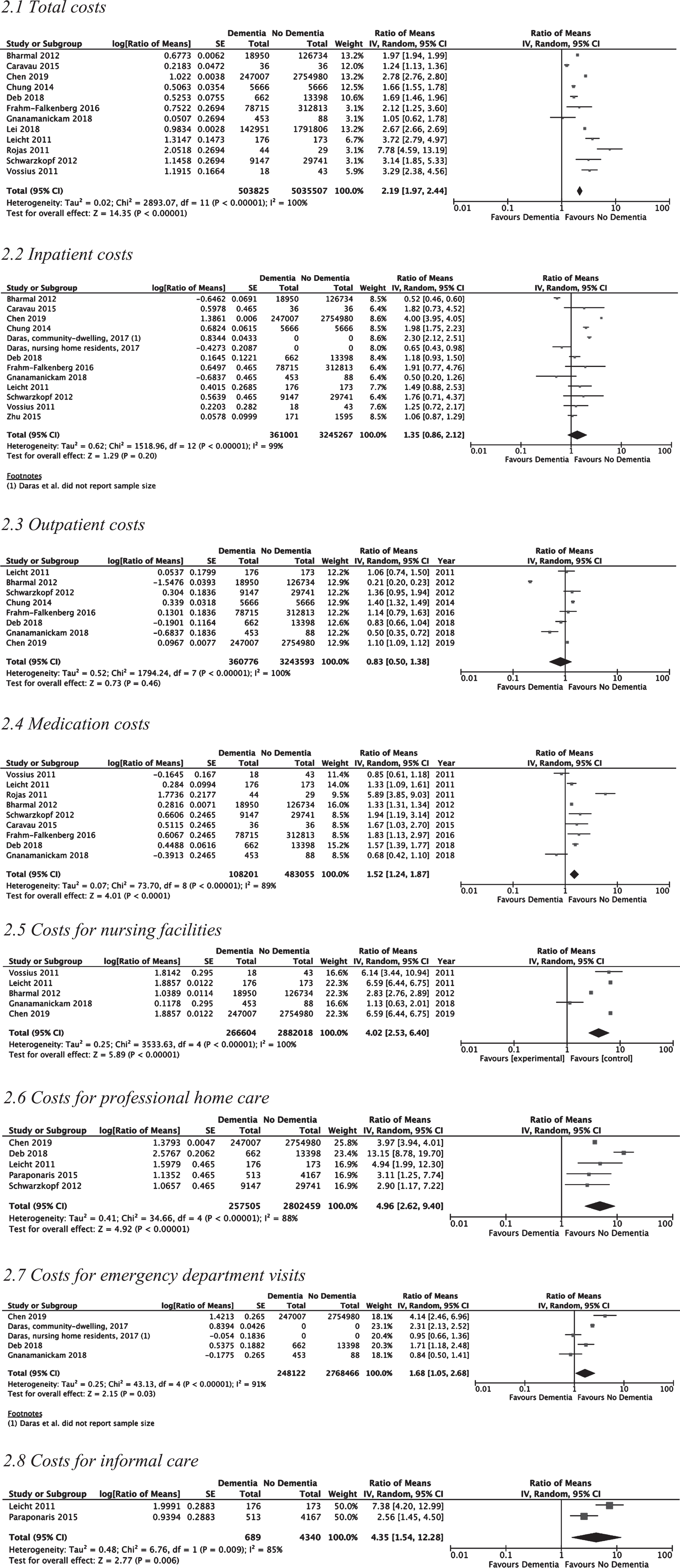
Analysis of total costs during the time period between diagnosis and death was performed for 12 studies [32–43]. Total costs ranged from $1,839 in Rojas et al.’s study [41] to $64,606 in Gnanamanickam et al.’s study [38] for demented subjects and from $236 in Rojas et al.’s study [36] to $61,412 for non-demented subjects in Gnanamanickam et al.’s study [38] (see Supplementary Table 2). Total costs were significantly higher for demented persons (ROM: 2.19 [1.97, 2.44], p < 0.00001, I2 = 100%). Medication costs were also higher for demented persons (ROM: 1.52 [1.24, 1.87], p < 0.0001, I2 = 89%; see Fig. 2) ranging from $286 in Rojas et al.’s study [41] to $5,074 in Bharmal et al.’s study [32] versus $49 in Rojas et al.’s study [41] to $3,829 in Bharmal et al.’s study [32] for non-demented persons. However, the analyses of inpatient costs (ROM: 1.35 [0.86, 2.12], p = 0.20, I2 = 99%) and outpatient costs were not significantly higher for demented persons (ROM: 0.83 [0.50, 1.38], p = 0.46, I2 = 100%). Costs for nursing facilities from five studies (ROM: 4.02 [2.53, 6.40], p < 0.00001, I2 = 100%) [32, 43] were significantly higher for PWD with costs ranging from $626 in Chen et al.’s study [34] to $60,332 in Gnanamanickam et al.’s study [38] than for PWOD with costs ranging from $95 in Chen et al.’s study [34] to $53,626 in Gnanamanickam et al.’s study. Costs for professional home care from five studies (ROM: 4.96 [2.62, 9.40], p < 0.00001, I2 = 88%) [32, 42] were significantly higher for PWD with costs ranging from $204 in Rojas et al.’s study [41] to $22,857 in Paraponaris et al.’s study [31] than for PWOD with costs ranging from zero in Rojas et al.’s study to $7,345 in Paraponaris et al.’s study [31]. Costs for emergency room visits from four studies (ROM: 1.68 [1.05, 2.68], p = 0.03, I2 = 91%) [30, 38] were significantly higher for demented than for non-demented people as well with costs ranging from $102 in Gnanamanickam et al.’s study [38] to $4,139 in Chen et al.’s study [34] for PWD compared to $122 in Gnanamanickam et al.’s study [38] to $999 in Chen et al.’s study [34] for PWOD. Costs for informal care were examined by Paraponaris et al. [31] and Leicht et al. [40]. In the analysis of informal costs using the replacement cost method (otherwise known as proxy good method) people with dementia had significantly higher costs for informal care (ROM: 4.35 [1.54, 12.28], p = 0.006, I2 = 85%) compared to non-demented people. Informal care costs for PWD were $8,726 in Paraponaris et al.’s study [31] and $18,625 in Leicht et al.’s study [40]. Informal care costs for PWOD were $1,765 in Paraponaris et al.’s study [31] and $2,523 in Leicht et al.’s study [40].
Forest plots of costs between diagnosis and death (ROM, 95% CI).
Time period around diagnosis
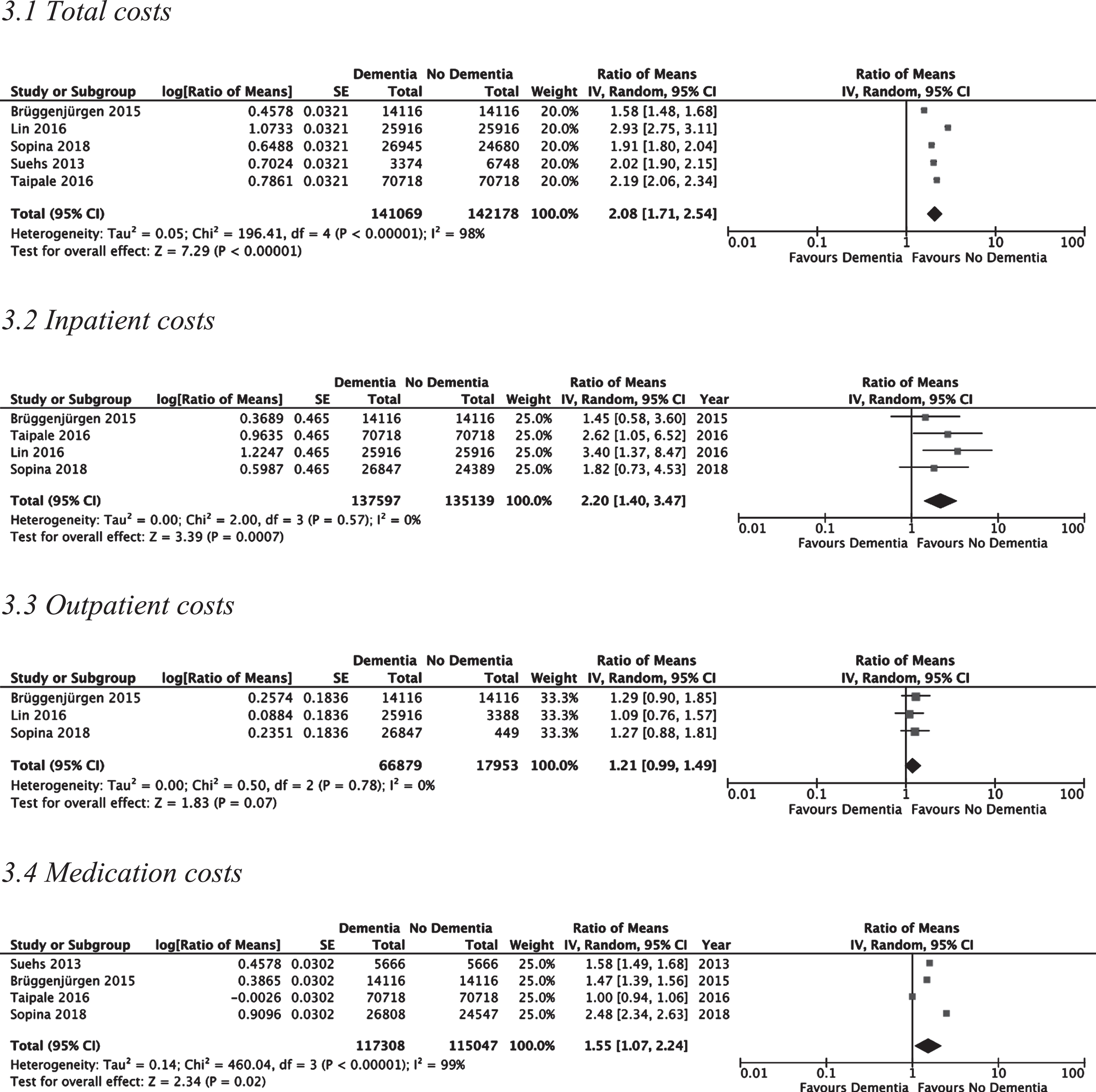
Analysis of total costs at the time of diagnosis was performed for five studies [23–27]. Total costs were significantly higher for demented persons (ROM: 2.08 [1.71, 2.54], p < 0.00001, I2 = 98%) with costs ranging from $10,782 in Sopina et al.’s study [26] to $29,298 in Lin et al.’s study [25] for PWD compared to $5,636 in Sopina et al.’s study [26] to $10,084 in Brüggenjürgen et al.’s study [27] for PWOD. Meta-analysis for medication costs revealed significantly higher costs for PWD (ROM: 1.55 [1.07, 2.24], p < 0.02, I2 = 99%) with costs ranging from $1,954 in Taipale et al.’s study [24] to $2,974 in Suehs et al.’s study [23] for demented people compared to $1,138 in Sopina et al.’s study [26] to $1,959 in Taipale et al.’s study [24] for non-demented people. Inpatient costs were significantly higher as well (ROM: 2.20 [1.40, 3.47], p < 0.0007, I2 = 0%) with costs ranging from $7,347 in Sopina et al.’s study [26] to $14,414 in Taipale et al.’s study [24] for PWD compared to $3,663 in Lin et al.’s study [25] to $5,499 in Taipale et al.’s study [24] for PWOD. Outpatient costs were not significantly higher for demented persons (ROM: 1.21 [0.99, 1.49], p < 0.07, I2 = 0%).
Time period around death
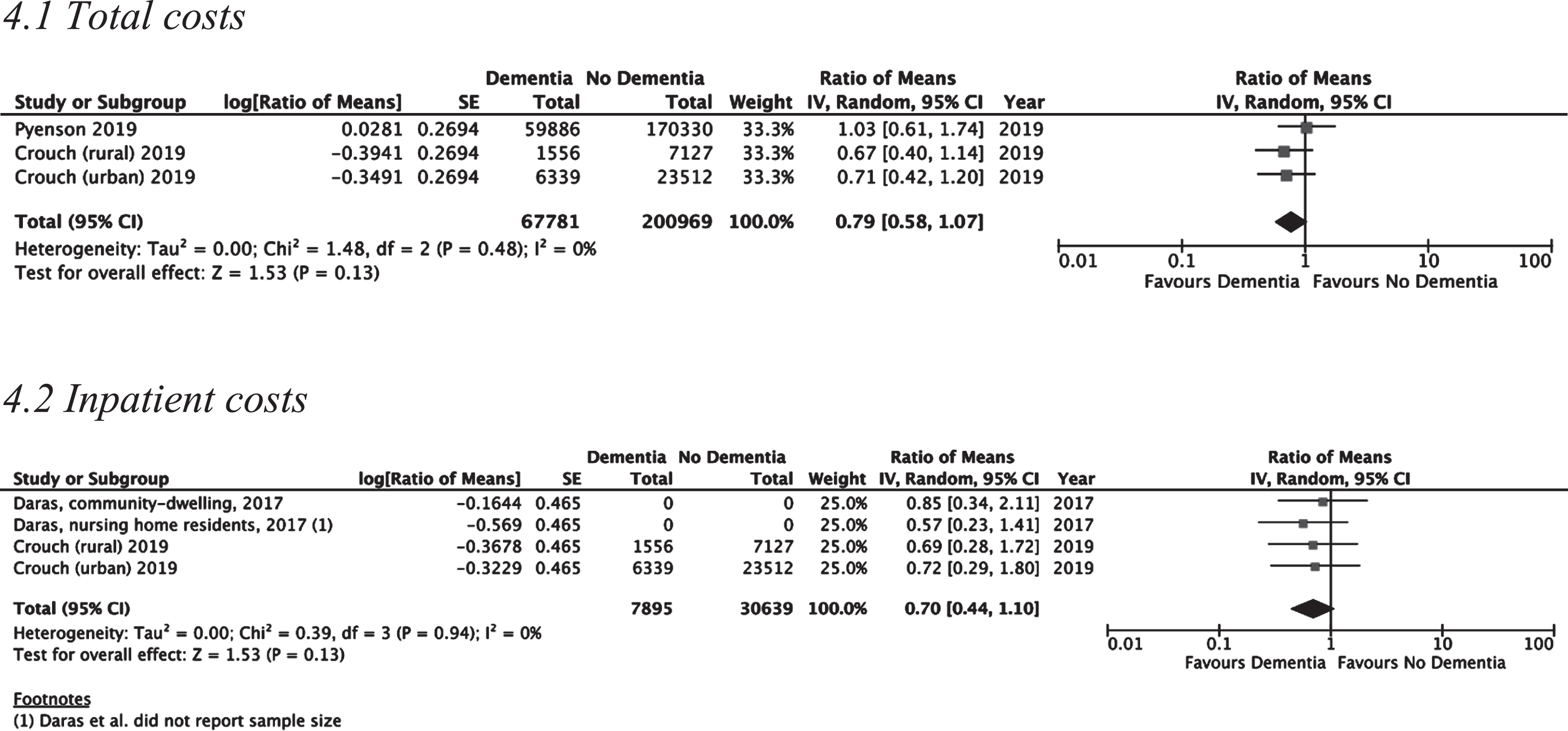
For the time period around death there was only sufficient data to compare total costs and inpatient costs between demented and non-demented people. Analysis of total costs was performed for two studies [28, 29] and three study populations, respectively. Total costs were not significantly higher for demented persons at the time of death (ROM: 0.79 [0.58, 1.07], p = 0.13, I2 = 0%) with costs ranging from $36,704 in Pyenson et al.’s study [29] to $51,408 in Crouch et al.’s study (for the subgroup of the urban population) [28] for PWD compared to $35,689 in Pyenson et al.’s study [29] to $72,887 in Crouch et al.’s study (for the subgroup of the urban population) [28] for PWOD. Analysis of inpatient costs was performed for two studies [28, 30] and four study populations. Inpatient costs were also not significantly higher for demented persons at the time of death (ROM: 0.70 [0.44, 1.10], p = 0.13, I2 = 0%) with costs ranging from $16,083 in Daras et al.’s study (for the subgroup of the people living in residential care) [30] to $35,884 in Crouch et al.’s study (for the subgroup of the rural population) [28] for PWD compared to $28,409 in Daras et al.’s study (for the subgroup of the people living in residential care) to $50,474 in Crouch et al.’s study (for the subgroup of the urban population) [28] for PWOD.
Heterogeneity and sensitivity analysis
Heterogeneity of most analyses was considerably high. High heterogeneity of costs might be caused by differences in GDP, health care systems, and study settings. We assumed that demented patients in residential care might have lower expenditures for inpatient and outpatient services than community-dwelling people. We therefore performed a sensitivity analysis excluding studies that only encompassed people living in residential care [30, 38] for the time interval between diagnosis and death (see Supplementary Table 4). This did not lead to a significant ROM between demented and non-demented persons for inpatient costs (ROM: 1.46 [0.76, 2.83] p = 0.26, I2 = 99%) and outpatient costs (ROM: 0.88 [0.51, 1.53], p = 0.66, I2 = 100%) for the time period between diagnosis and death.
Matching cohorts is a method to minimize confounding in a study by equalizing the distribution of variables that are potential confounders [45]. In this meta-analysis twelve studies used matched control groups [23–27, 44], while 10 studies used unmatched controls [28–30, 43]. In order to assess the effect of matching on the ROM for each cost category we conducted a sensitivity analysis in which unmatched cohorts were excluded. This sensitivity analysis was only possible for the subgroup of studies conducted in the time period between diagnosis and death since all studies conducted at the time around diagnosis were matched cohort studies [23–27] and all studies conducted at the time around death were unmatched cohort studies [28–30]. Sensitivity analysis for total costs revealed a higher ROM between demented and non-demented persons (3.11 [1.77, 5.46] p < 0.0001, I2 = 94%) when including matched cohorts only compared to the analysis of total costs in which we did not exclude unmatched cohort analyses (ROM: 2.19 [1.97, 2.44], p < 0.00001, I2 = 100%). A higher difference in costs with costs being higher for PWD could also be shown for medication costs (analysis including only matched controls: ROM: 2.28 [1.16, 4.48] p = 0.02, I2 = 92%; analysis including matched and unmatched controls: ROM: 1.52 [1.24, 1.87], p < 0.0001, I2 = 89%). In the sensitivity analyses of inpatient costs, costs for demented persons compared to matched controls turned out significantly higher which they had not been in the analysis including matched and unmatched cohort studies (analysis including only matched controls: ROM: 1.55 [1.04, 2.30] p = 0.03, I2 = 86%; analysis including matched and unmatched controls: ROM: 1.35 [0.86, 2.12], p = 0.20, I2 = 100%). The sensitivity analysis of outpatient costs also delivered significant results (analysis including only matched controls: ROM: 1.34 [1.19, 1.50] p < 0.00001, I2 = 17%; analysis including matched and unmatched controls: ROM: 0.83 [0.50, 1.38], p = 0.46, I2 = 100%). However, in the analysis of professional home care costs the opposite could be shown with costs being less increased in the analysis including only matched control cohorts (ROM: 3.55 [2.10, 6.00] p < 0.0001, I2 = 0%) compared to the analysis including matched as well as unmatched control cohorts (ROM: 4.96 [2.62, 9.40], p < 0.00001, I2 = 88%).
DISCUSSION
The objective of this meta-analysis was to assess the excess costs of dementia and to provide an updated overview of the research on the cost-of-illness of dementia. Furthermore, we aimed to provide pooled estimates of excess costs in terms of a meta-analysis. Since absolute estimates in cost-of-illness studies can differ by several orders of magnitude, due to heterogeneity in the consideration of cost categories, we used the ROM approach to pool cost data over studies. This approach has several advantages, especially its independence from the magnitude of absolute costs due to differences in cost assessments. Furthermore, also between-study differences in prices or purchasing power are strongly reduced, if not eliminated by using this approach. However, it also comes with some disadvantages. First, ROM only works for studies providing mean costs for a group of affected persons together with mean costs for a non-affected comparator group. This precondition strongly reduces the number of eligible studies since most cost-of-illness studies report only costs for affected persons. Excluding all of these studies means to ignore a considerable amount of evidence but is inevitable if one wants to apply meta-analytic pooling to cost-of-illness studies. Secondly, ROM can neither compensate for the variation of absolute costs due to the skewed nature of cost data, which can also affect the relative difference between groups, nor for heterogeneity resulting from differences in health care systems between countries.
Studies included in our analysis were relatively heterogeneous, in particular regarding the countries in which the studies were conducted, the types of dementia included, the samples used as controls, the cost categories considered, and the timing of the inclusion of patients regarding disease progress. All of these differences can affect the cost estimates. For example, type of dementia might affect health care utilization in different cost sectors, since treatment can differ by dementia subtype. The composition of the comparator group might affect the morbidity structure and hence health care costs. Twelve studies tried to control for this problem by generating a matched control group [23–27, 44], while 10 studies used unmatched controls [28–30, 43]. In four out of five sensitivity analyses that only included matched controls the ROM for PWD increased compared to the analyses including both matched and unmatched controls. This is an important finding, especially for the design of studies in future research.
The consideration of cost categories also differed considerably between studies which strongly affects absolute costs. We used ROM instead of absolute costs to overcome this problem; however, this approach uses the implicit assumption that the relative increase in costs induced by dementia is comparable over different cost categories which might not be the case. Also, the timing of cost measurement within the disease progress of dementia can affect costs. Here we identified three types of studies: studies analyzing cost immediately following the dementia diagnosis, studies analyzing costs before death, and studies analyzing costs at any time between diagnosis and death. To overcome this heterogeneity, we analyzed three subgroups according to the time between diagnosis and death to which the reported cost data are referring to. Since these groups have different samples, the cost categories which could be pooled differed strongly with total costs and inpatient costs being the only cost categories represented in all three subgroups.
Time period between diagnosis and death
In the time period between diagnosis and death total costs were 119% higher for demented than for non-demented persons, the highest overall cost factors being costs for professional home care with 396% higher costs and nursing facilities with 302% higher costs. Nursing care has been previously shown to be the main cost factor in the treatment of people with dementia [46–48]. This finding is highly intuitive since by definition dementia leads to impaired ability to perform activities of daily living independently [1]. Costs for professional home care, informal care, and nursing facilities showed the strongest cost difference between demented and non-demented persons of all cost categories analyzed in our study. While costs for nursing facilities might only become relevant for the most severe health states at the end of life of persons with dementia, professional care at home is utilized over a long period of time over the disease course. Home care costs will also be substantially underestimated since a considerable amount of home care is provided as non-professional informal care by relatives [40]. Similar to the time directly following the diagnosis medication costs might be increased due to the utilization of anti-dementia drugs. It has been shown that dementia increases the risk for falls and related injuries [49], which might explain the increase in costs for emergency department visits.
Time period around diagnosis
At the time around diagnosis, total costs, inpatient costs, and medication costs were significantly higher for demented people in comparison to non-demented controls. Total costs were 108% higher for demented persons than non-demented persons. Excess costs of medication and inpatient treatment were even highest at the time around diagnosis. According to Taipale et al., the increase of inpatient costs around the time of diagnosis might be caused by the diagnostic process itself which leads to an early increase in hospital costs pre-diagnosis and an increase in medication costs immediately post-diagnosis in their study [24]. The increase of health care costs prior to diagnosis of dementia can be explained by the fact that it is a progressive neurodegenerative disease where cognitive changes are present prior to formal diagnosis [37, 50]. The increase in medication costs might be explained by the use of anti-dementia drugs, or by an optimization of other drugs induced during the diagnostic procedure resulting in the dementia diagnosis. For example, diagnosis of vascular dementia might lead to an optimization of drugs for hypertension. Also use of over-the-counter products for the brain might increase medication costs in persons with dementia.
Time period around death
At the time around death, total costs were not proportionally higher for demented than for non-demented persons. A possible explanation for lower medical costs might be that in the final stage of disease families and physicians abstain from complex treatment plans for comorbidities, such as cancer, with regard to the general state of health of the demented person [29]. It is well known that health care costs considerably increase before death. Hence, costs in the comparator group might be increasing as well—independent from the underlying diseases—resulting in a dispersion of cost differences between the groups. However, it has to be considered that only three study groups could be included in the subgroup analysis of total costs and Pyenson et al.’s [29] as well as Daras et al.’s [30] study did not report costs for major cost categories such as nursing facilities and professional home care.
Limitations
We acknowledge that this review and meta-analysis has its limitations. We imputed standard errors if they were missing. We also included studies that only reported one cost category or had small sample sizes. Moreover, literature research was limited to studies published in English or German between 01.04.2010 and 31.03.2020 which might have led to reporting bias. Our search only included a limited number of databases (PubMed, EconLit, NHS-EED, Cochrane Library) and potentially has missed other relevant literature.
Dementia is a highly underdiagnosed disease. According to the World Alzheimer Report of 2011, about 39% of dementia cases are being diagnosed [33]. Underdiagnosis leads to underestimation of macroeconomic costs. However, it can also lead to overestimation of total costs per person since more severe cases are more likely to be diagnosed and treated. In a policy paper of the Department of Health and Social Care from the UK three reasons for underdiagnosis were identified: 1) dementia is highly stigmatizing which prohibits diagnosis, 2) memory loss is falsely considered to be a normal finding in aging people, and 3) dementia is believed to be untreatable [51, 52]. These misconceptions can be addressed through initializing programs for early diagnosis especially for primary care physicians and through raising awareness in the general population.
Most studies included more than one cost category. However, the included cost categories in each study were highly variable. Total, inpatient, outpatient and medication costs were most frequently reported. One study reported medical costs as a sum of outpatient, inpatient, emergency department, home health service costs and costs for facility encounters [23]. On the other hand, Schwarzkopf et al. reported outpatient costs for general practitioner visits and medical specialist visits separately [42]. This inconsistency in study design leads to difficulties in pooling results in a meta-analysis. A guideline for cost-comparison studies of dementia should be implemented to facilitate future research.
Nonetheless, we could show that there are differences in health care expenditures for people with dementia over the course of the disease. Cost factors contribute differently to the overall expenditures and should be targeted differently with disease progression. More studies that report data from a societal perspective, ideally in a longitudinal setting, are needed to demonstrate the real cost differences for different cost categories. Direct costs for social care such as costs for nursing facilities, day care, home nursing services, food supply, transportation and social workers have been shown to be much higher cost factors than direct medical costs in high income countries. 45% of costs are estimated to be incurred by informal care, 40% of costs by direct costs of social care, and 15% of costs by direct medical costs [53]. Costs for professional care increase with disease progression [54]; however, this cost category was underrepresented in our analysis. Only eight of 22 studies in this meta-analysis reported costs for professional home care [25, 40–42]. Only six of 22 studies had collected data on costs for nursing facilities [28, 43]. The source of data for most studies in this meta-analysis was claims data, e.g., from insurance companies. Since costs for professional caregiving are often not fully covered by health insurance, it is very likely that the real difference of costs between demented and non-demented persons is higher than estimated by our study.
We found only two studies that assessed excess costs for informal care [31, 40]. As 83% of care is provided informally [55], the real excess costs of dementia from a societal perspective must be substantially higher than in our analysis. New research suggests that the current state of literature only represents the “tip of the iceberg” of the real-world costs of dementia [56]. More studies including a comparison group and data on hours and costs spent on informal care are needed.
CONCLUSION
Our findings demonstrate that costs of dementia constitute a substantial economic burden. A strength of this study was that studies from different countries and health care systems were included. To our knowledge, this is the first study to assess excess costs of dementia by means of the ROM method. More research on excess costs of dementia is needed as a guide for health economic decision making. Cost-of-illness studies should include a comparison group, encompass formal and informal costs and ideally also intangible costs and should follow subjects over a long term. Future research is needed to identify development of costs for this disease with globally increasing prevalence and significance.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0174r2).