
Abstract
Background:
Use of specialists and recommended drugs has beneficial effects for older adults living with Alzheimer’s disease and related dementia (ADRD). Gaps in care may exist for minorities, e.g., Blacks, and especially in the United States (U.S.) Deep South (DS), a poor U.S. region with rising ADRD cases and minority overrepresentation. Currently, we have little understanding of ADRD care utilization in diverse populations in this region and elsewhere in the U.S. (non-DS), and the factors that adversely impact it.
Objective:
To examine utilization of specialists and ADRD drugs (outcomes) in racial/ethnic groups of older adults with ADRD and the personal or context-level factors affecting these outcomes in DS and non-DS.
Methods:
We obtained outcomes and personal-level covariates from claims for 127,512 Medicare beneficiaries with ADRD in 2013–2015, and combined county-level data in exploratory factor analysis to define context-level covariates. Adjusted analyses tested significant association of outcomes with Black/White race and other factors in DS and non-DS.
Results:
Across racial/ethnic groups, 33%–43% in DS and 43%–50% in non-DS used specialists; 47%–55% in DS and 41%–48% in non-DS used ADRD drugs. In adjusted analyses, differences between Blacks and Whites were not significant. Vascular dementia, comorbidities, poverty, and context-level factor “Availability of Medical Resources” were associated with specialist use; Alzheimer’s disease and senile dementia, comorbidities, and specialist use were associated with drug use. In non-DS only, other individual, context-level covariates were associated with the outcomes.
Conclusion:
We did not observe significant gaps in ADRD care in DS and non-DS; however, research should further examine determinants of low specialist and drug use in these regions.
Keywords
INTRODUCTION
Alzheimer’s disease and related dementia (ADRD) affects more than 5 million Americans, mainly those older than 65 for whom it is a leading cause of death [1]. ADRD prevalence is expected to more than double by 2040 especially in some areas of the country such as the Southeast [2]. For the older population with ADRD, the literature reports gaps in medical care, including less than 25% of Medicare beneficiaries being diagnosed by, or receiving care from, a specialist such as neurologist, psychiatrist, or geriatrician [3–5], and at most 60% having ADRD drug treatment [6–10]. These care elements are associated with more timely diagnosis, lower costs of care and fewer institutionalizations [3, 11–17]. Moreover, in line with consistent evidence up to 2009 [18], a recent analysis showed racial/ethnic disparities in ADRD drug use [19]. This is worrisome because groups like Blacks have the highest ADRD prevalence [1, 20] and are highly represented in the Southeast where, together with rising ADRD cases, challenges to access to care exist [1]. Currently, we know little about the status or the driving determinants of ADRD care for racial/ethnic groups of older adults in the Southeast compared to the rest of the country, with one study reporting higher ADRD drug use in this region [7].
One region deserving closer scrutiny is the Deep South, a southeastern sub-region characterized by lower socioeconomic status and poor health care access and outcomes. It is important to examine how this context impacts the ability of older adults to access needed ADRD care. As suggested by conceptual frameworks developed to understand health care access [21], the socioeconomic, health and health care contexts together with patients’ personal and clinical characteristics, are important determinants of health care utilization and ultimately health outcomes. For example, area-level disadvantage is an additional risk factor beyond personal disadvantage for poor outcomes, including a higher utilization of inpatient care [22–26]. Therefore, a better understanding of personal and context-level determinants of ADRD care utilization for diverse groups of older adults with ADRD, in the Deep South and elsewhere in the country, will shed light on observed disparities and how to best provide current and future treatments.
The objective of this paper was to provide a snapshot of the care received over a one-year period by older adults with ADRD in the Deep South and non-Deep South. In each region, we examined 1) the utilization of specialists and ADRD drugs in Whites, Blacks, and other racial/ethnic groups; and 2) the degree to which personal and socioeconomic, health and health care contexts may impact access to these care elements. Our results provide a picture of the gaps that exist in the care for diverse older Americans with ADRD across geographic regions and elucidate factors to target in each region to ensure optimal care and prevent the exacerbation of existing health disparities as the prevalence of ADRD increases in the future.
MATERIALS AND METHODS
We conducted secondary analyses of 2012–2016 administrative claims data for Medicare beneficiaries with fee-for-service Part A (hospital), B (outpatient), and D (prescription drug coverage) from a 5% random sample of Medicare beneficiaries (standard research sample available from the Center for Medicare and Medicaid Services). Data included Medicare Part A and B claims for physician and other outpatient visits, inpatient and skilled nursing facility admissions, and records for filled prescriptions from the Medicare Part D Drug Event file. The University of Alabama at Birmingham’s Institutional Review Board considered this study exempt research.
Study design
Among beneficiaries 66 years old or older in 2013, we identified ADRD cases in a three-year period (2013–2015) [27, 28] using a highly sensitive and specific (≥0.85) algorithm [29]. The algorithm specified International Classification Of Disease (ICD) diagnosis codes for Alzheimer’s disease (331.0, G30.0, G30.1, G30.8, G30.9), frontotemporal dementia (331.11, 331.19, G31.01, G31.09), vascular dementia (290.40–290.43, F01.50, F01.51), senile dementia (290.0, 290.20–290.21, 290.3, 290.10–290.13, F03.90, F03.91, F05), and other forms of dementia (331.2, 331.7, 294.0, 294.10, 294.11, 294.20, 294.21, 294.80, 797, G31.1, G94, G13.2, G13.8, G31.2, G91.4, F02.80, F02.81, F03, F04, F06.8, F06.1, R41.81, R54).
An “index event” was the first claim that contributed to case identification (Fig. 1). Follow-up was the period after the index event and until institutionalization in skilled nursing facility or hospice for 30 days or more, or death, or one year, whichever came first, with a minimum of 7 days. To have complete data for our outcomes, the analytic sample was limited to beneficiaries continuously enrolled in fee for service Medicare Part A, B, and D in the follow-up (N = 135,490). We also limited to those continuously enrolled in fee-for-service Part A and B in a look-back period of 365 days before the index event to examine existing comorbid conditions. The final sample included 127,512 beneficiaries.

Study design. ADRD, Alzheimer’s disease and related dementia.
Outcomes
Outcomes in follow-up were: 1) having at least one specialist visit (specialty code in physicians’ claims equal to 13 for neurology, 26 and 27 for psychiatry and general psychiatry, 86 for neuropsychiatry, and 86 for geriatric medicine [5]); and 2) having at least one filled prescription (minimum 7 days [19]) for ADRD drugs, specifically donepezil, galantamine, rivastigmine, and memantine.
Independent variable
The main independent variable was race/ethnicity [30]. Categories include Black (or African American), Non-Hispanic White, Hispanic, Asian/Pacific Islander, and Other (i.e., American Indian/Alaska Native, Other, and Unknown). The Deep South was defined as the states of Alabama, Georgia, Louisiana, Mississippi, and South Carolina, and non-Deep South as the rest of the U.S. states.
Conceptual framework and covariates
The choice of covariates was guided by the Behavioral Model of Access to Care that describes factors at personal and context level that would predispose or enable ADRD cases to seek medical care, and need factors for which they would access care [21]. These factors may differ for diverse groups of Deep South and non-Deep South populations. Personal-level predisposing factors included age and gender. Personal enabling factors at the time of the index event included Medicare/Medicaid dual eligibility (poverty indicator), and, as a proxy for personal socioeconomic status, the Area Deprivation Index (ADI) aggregated to 9-digit residential ZIP codes. The ADI is a composite measure of 17 variables in the domains of income, education, employment, and housing quality, with a national 1–100 scale and higher values indicating higher socioeconomic deprivation [31–33]. Personal need factors included clinical characteristics, i.e., dementia subtypes, the number of comorbid conditions and, for the ADRD drug utilization analysis, pre-existing cardiovascular conditions that may interfere with ADRD treatment (myocardial infarction [MI] and congestive heart failure). Comorbidities were identified in the look back period using the Charlson Comorbidity Index (CCI) algorithm (Fig. 1) [34].
For the context level, we used county-level Area Health Resources File (AHRF) data for the available time period closest to the 2013–2015 case identification period. We selected 23 variables to represent: Context-level predisposing factors: population age and race (proportion of 2015 population 65 and older and Black/African American), education (2012–2016 mean proportion of population 25 and older with less than high school diploma); and residence in large or small metro, micropolitan or rural county (based on Urban Influence Code) [35], other social conditions (2010 proportion of owner-occupied housing units, population density); context-level enabling factors: income/poverty (2012–2016 mean proportion of older population in deep poverty, 2015 unemployment rate and proportion of Medicare beneficiaries eligible for Medicaid), availability of medical resources (number per 1000 of neurologists, psychiatrists, internal medicine and primary care physicians, hospital beds, and skilled nursing facility beds), Medicare penetration (number per 1000 of 2015 Medicare Fee for Service beneficiaries, proportion of 2015 eligible beneficiaries enrolled in Medicare Advantage and Medicare Prescription Drug Plan), and quality of care (2015 number of Emergency Department (ED) Visits per 1000 Medicare beneficiaries); and context-level need factors: disability (2012-16 mean proportion of older population on disability) and comorbidities (2013–2015 mean number of deaths per 1000 due to cerebrovascular, ischemic heart disease, and other cardiovascular disease).
Analysis
All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). We first used descriptive statistics to examine characteristics by race/ethnicity overall and across Deep versus non-Deep South. Chi Square and t-tests were used to identify statistically significant differences. To define potential underlying social contexts, we conducted an exploratory factor analysis (EFA) using the 23 selected context-level variables and the SAS PROC FACTOR. We eliminated one variable (number of internal medicine doctors per 1000) because it was highly correlated (> 0.8) with the number of neurologists and psychiatrists. Using Box’s test, a multivariate statistical test to check the equality of multiple variance-covariance matrices [36], we determined that the variance-covariance structure between the Deep and non-Deep South group was significantly different (p < 0.0001). Therefore, we ran the EFA separately for beneficiaries in the Deep and non-Deep South. Considering that underlying factors could be potentially correlated, an oblique rotation was applied. Four factors were retained based on a percentage of variance explained (≥5%) and interpretability. A factor loading≥0.5 was used to determine variables’ membership to a factor. After the first iteration, we eliminated rural status and population density because factor loadings were < 0.5 in both samples. Lastly, we estimated factor scores to be used in regression analyses by creating linear combinations of the final retained context-level variables.
Next, we examined the frequency of use of specialists and ADRD drugs across racial/ethnic groups in the Deep South and non-Deep South and tested unadjusted differences using Chi-square tests. Given the small size of racial/ethnic groups in the Deep South, we conducted adjusted analyses only for the Black and White populations in each region using a modified Poisson regression (proc genmod) to obtain relative risks (RR) and 95% confidence intervals (CI). To remain conservative given the large sample sizes, all results were considered statistically significant when the accompanying statistical test yielded a two-tailed probability of 0.0001.
RESULTS
Sample characteristics
Medicare beneficiaries with ADRD were 81.1% White, 9.8% Black, 5.8% Hispanic, 2.3% Asians, and 1.0% of other race/ethnicity, 71.9% females, 46.7% 85 or older, and 51.4% with 3 or more comorbidities (Table 1). More than 30% were Medicare/Medicaid dually eligible, the mean ADI was 48.8 (median 48), and 46.6% were from large and 31.5% from small metro areas. Compared to White beneficiaries, Blacks and Hispanics were younger, had more comorbidities, and higher mean ADI scores. In general, minority groups were about 60% or more Medicare/Medicaid dually eligible and more likely to live in large metropolitan areas. Follow up was on average 316 days, ranging from 314.8 for Whites to 329.8 for Asians.
Characteristics of Medicare beneficiaries* with Alzheimer’s disease and associated dementia in 2013–2015 (N = 127,512), by race/ethnicity and region
*Medicare beneficiaries with Part A, B, D and no HMO in follow-up period, i.e., one year post index event or until death or institutionalization, whichever comes first, and A,B, no HMO in one year before index event. CCI, Charlson Comorbidity Index; MM, Medicare/Medicaid; ADI, Area Deprivation Index.
Overall, 12,017 (9.4%) of beneficiaries lived in the Deep South (Table 1). Within racial/ethnic groups, 21.3% of Blacks, 8.9% of Whites, 1.4% of Hispanics, 1.4% of Asians and 3.7% of Others lived in this region. Compared to non-Deep South beneficiaries, significant differences (p < 0.0001) included Deep South beneficiaries being less likely to be 85 and older (39.8% versus 47.4%) and to live in large metro areas (20.7% versus 49.3%), being more likely to be Medicare/Medicaid dual eligible (43.3% versus 33.8%) and having a higher ADI (62.5 versus 47.4). The comorbidity profiles were similar, except for peripheral vascular disease being less frequent among Deep South beneficiaries (29.8% versus 38.5%). Significant differences at the context level (Table 2) included Deep South beneficiaries living in counties with a higher proportion of Black population (30.8% versus 11.8%) and low education (16.2% versus 12.9%), with lower availability of physicians and higher availability of hospital beds and utilization of ED visits, and higher disability and number of deaths for cerebrovascular (3.5 versus 2.8 per 1,000) and cardiovascular disease (9.5 versus 6.5 per 1,000).
Results of exploratory factor analysis to define county-level contexts in Deep South and Non-Deep South
All variables have positive factor loading values except when indicated by *; 1Deep South, Alabama, Georgia, Louisiana, Mississippi, and South Carolina; 2Non-Deep South, U.S. states not in the Deep South; 3Office-based non-federal physicians who provide patient care (2015); 4PCP, Primary Care Physicians; 5Number of Hospital Beds per 1000 population in 2015; 6Percent of Owner-Occupied Housing Units in 2010; 7Percent of county population 65 + in 2015; 8Percent of county population 25 + w/<HS Diploma in 2012-16; 9Percent of Medicare Beneficiaries in the county eligible for Medicaid in 2015; 10Percent of Civil Noninstitutionalized 65 + county population on Disability in 2012-16; 11ED Visits per 1000 Medicare Fee for Service beneficiaries in the county in 2015; 12Number of Skilled Nursing Facility Beds per 1000 population in 2015; 13Three year mean number of deaths per 1000 population in 2013-15; 14Number of Medicare Beneficiaries in Fee for Service plans per 1000 population in 2015; 15Percent of Medicare beneficiaries in Advantage care plans in 2015; 16Percent of eligible Medicare beneficiaries with Part D Prescription Drug Plans in 2015; 17Percent of county population Black/African American in 2015; 18Unemployment rate for the county population 16 + in 2015; 19Percent of Persons 65 + in Deep Poverty in 2012-16.
Exploratory factor analysis
The EFA revealed four slightly different underlying context factors for each region (Table 2). For the Deep South, these were: 1) Availability of medical resources (variance explained = 37.3%); 2) Socioeconomic and health context (variance explained = 43.5%); 3) Health insurance market context (variance explained = 33.4%); 4) Other context (variance explained = 26.7%). For the non-Deep South, these were: 1) Availability of medical resources (variance explained = 32.2%); 2) Socioeconomic context (variance explained = 28.5%); 3) Population health (variance explained = 25.5%); and 4) Health insurance market context (variance explained = 25.1%).
Use of specialists
About 45% had at least one specialist visit (CI:45.2–45.8) (Fig. 2A), ranging from 43.0% of Asians (CI:41.3–44.8) to 49.5% of Hispanics (CI:48.3–50.6) (about 28% had visits with neurologists, 19.5% with psychiatrists, and about 7% with geriatricians). Deep South beneficiaries (41%, CI:40.1–41.8) were less likely to have specialist visits than non-Deep South beneficiaries (46.0%, CI:45.7–46.3) (p < 0.0001). In the Deep South, only 36.9% of Blacks (CI:35.0–38.7) versus 42.2% of Whites (CI:41.2–43.2) had at least one specialist visit, in contrast to 49.8% of Blacks (CI:48.8–50.7) and 45.5% of Whites (CI:45.1–45.8) in the non-Deep South. In analyses adjusted for personal- and context-level factors (Fig. 3, Supplementary Table 2), differences for Black and White beneficiaries were not statistically significant: relative risks for Blacks versus Whites were 0.89 (CI:0.84–0.95, p = 0.0017) in the Deep South and 1.03 (CI:1.01–1.06, p = 0.0033) in the non-Deep South.
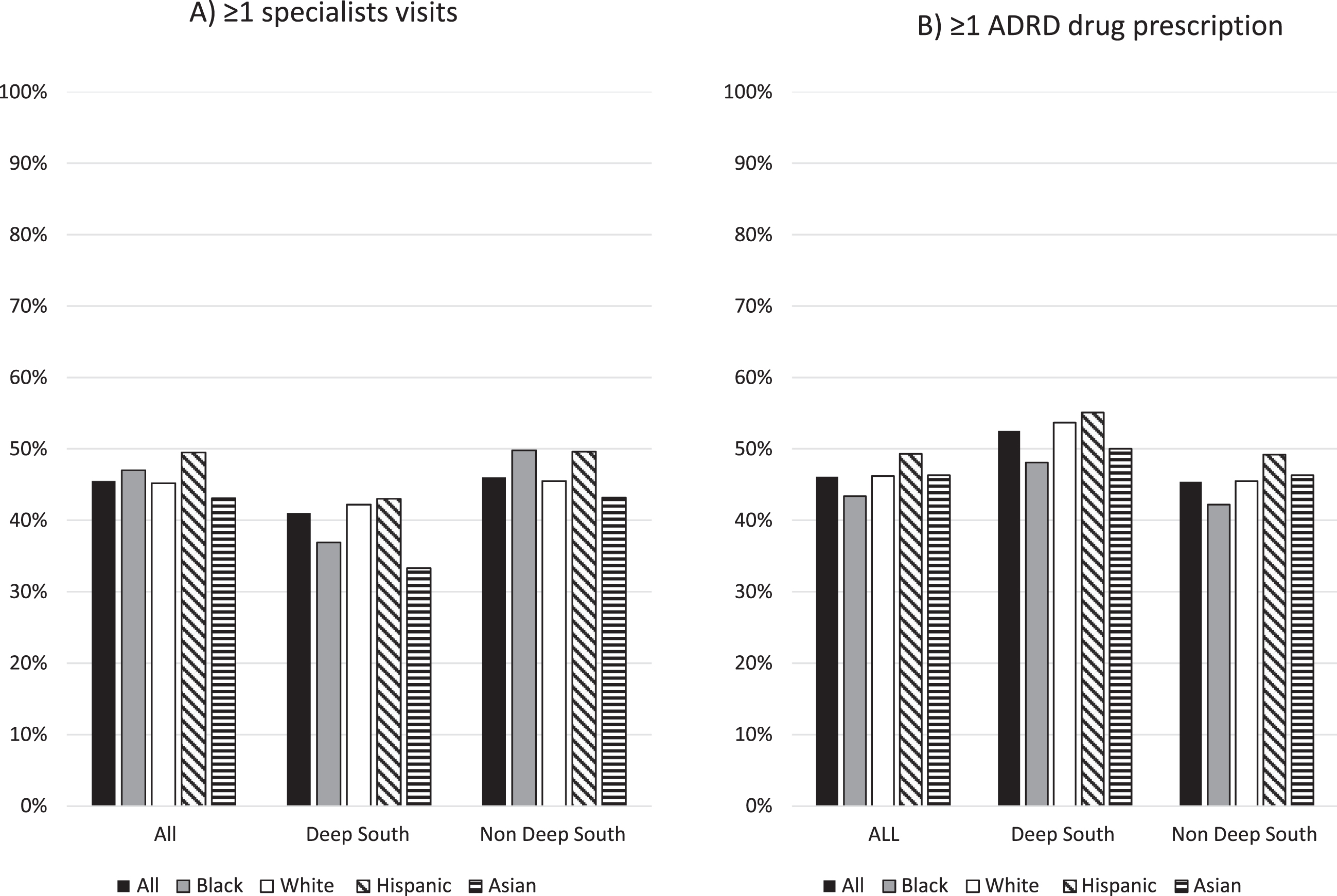
Proportion of Medicare beneficiaries with at least one visit with a specialist (neurologists, psychiatrist, or geriatrician) (1A) and with at least one prescription for ADRD drugs (donepezil, galantamine, rivastigmine, or memantine) (1B), by racial/ethnic demographic group and by geographic region. Deep South includes Alabama, Georgia, Louisiana, Mississippi, and South Carolina, non-Deep South includes all other U.S. states. Medicare administrative claims and prescription drug data, 2013–2015.
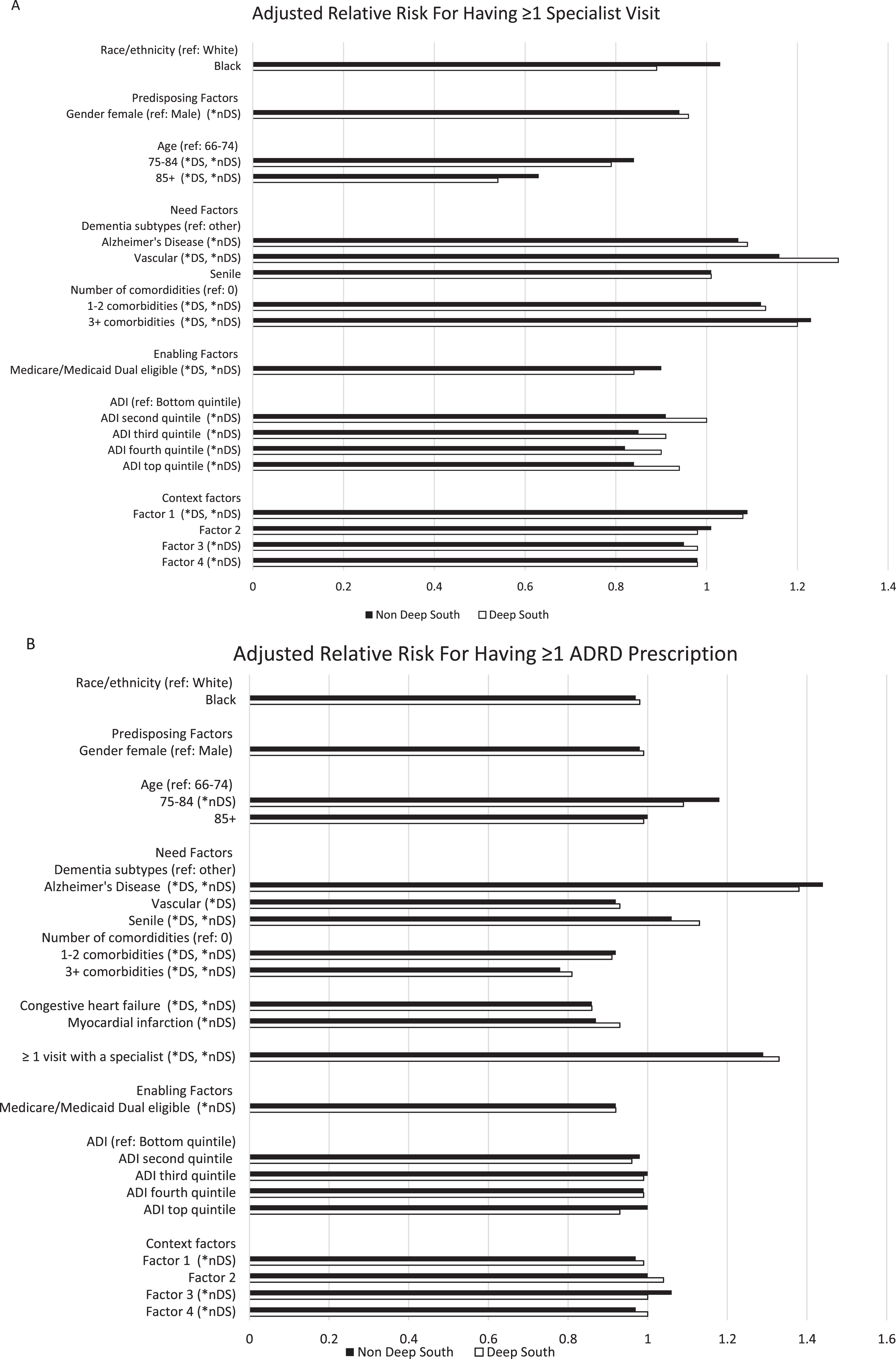
Adjusted relative risk estimates for utilization of specialists (at least one visit with a specialist) (3A) and ADRD prescription drug (at least one prescription) (3B) from modified Poisson regression analyses for Deep South (DS) and non-Deep South (nDS) beneficiaries. Deep South includes Alabama, Georgia, Louisiana, Mississippi, and South Carolina. *nDS, *DS, significant associations in analyses for non-Deep South or Deep South (p < 0.0001). Context factors: DS and nDS Factor 1 = Availability of medical resources; DS Factor 2 = Socioeconomic and health context; nDS Factor 2 = Socioeconomic context; DS Factor 3 = Health insurance market context; nDS Factor 3 = Population health; DS Factor 4 = Other context; nDS Factor 4 = Health insurance market context.
Need factors associated with having specialist visits (Fig. 3A, Supplementary Table 2) included having vascular dementia (RR > 1.16, p < 0.0001 in both regions), higher number of comorbidities, specifically 3 or more in the Deep South (RR = 1.20, 1.12–1.29, p < 0.0001) and 1 or more in the non-Deep South (RR≥1.12, p < 0.0001). Among enabling factors, being Medicare/Medicaid dually eligible in both regions, and a higher ADI in the non-Deep South, were associated with a lower likelihood of having specialist visits. Factor 1, Availability of medical resources, was significantly associated with utilization of specialists for both Deep and non-Deep South beneficiaries (Deep South RR = 1.08, 1.05–1.11, non-Deep South RR = 1.08, 1.08–1.09, p < 0.0001). No other context factors were significantly associated with specialist utilization for Deep South beneficiaries. Other two factors, Population health (Factor 3, RR = 0.95, 0.95–0.96, p < 0.0001) and Health insurance market context (Factor 4, RR = 0.98, 0.97–0.99, p < 0.0001), were significantly associated with specialist use for non-Deep South beneficiaries indicating lower specialist utilization in contexts with poorer health (higher number of deaths and utilization of ED and SNF), and in those with higher penetration of fee-for-service Medicare.
Use of ADRD drugs
Just over 46% (CI:45.8–46.3) had at least one ADRD drug prescription (Fig. 2B), from 43.4% of Blacks (CI:42.6–44.3) to 49.3% of Hispanics (CI:48.1–50.4). Deep South beneficiaries (52.5%, CI:51.6–53.4) were more likely to have at least one ADRD prescription than non-Deep South beneficiaries (45.4%, CI:45.1–45.7) (p < 0.0001). In the Deep South, Blacks (48.1%, CI:46.2–50.0) were the least likely and Hispanics the most likely (55.1%, CI: 45.7–64.6) to have at least one prescription. Similarly, in the non-Deep South, 42.2% of Blacks (CI:41.2–43.2) and 49.2% of Hispanics (CI:48.0–50.3) had at least one prescription (Fig. 2B).
In analyses adjusted for personal and context-level factors (Fig. 3B, Supplementary Table 2), differences for Blacks and Whites were not statistically significant. Relative risks for Blacks versus Whites were 0.98 (0.93–1.03, p = 0.409) in the Deep South and 0.97 (0.95–1.00, p = 0.051) in the non-Deep South.
For Deep South beneficiaries, having Alzheimer’s disease (RR = 1.38, 1.33–1.44) or senile dementia (RR = 1.13, 1.08–1.19), specialist visits (RR = 1.33, 1.28–1.38), and comorbidities (including congestive heart failure, RR = 0.86, 0.82–0.91), were significantly associated with using ADRD drugs (p < 0.0001) (Fig. 3B, Supplementary Table 2). These same factors, plus evidence of MI (RR = 0.87, 0.85–0.90) and being Medicare/Medicaid dually eligible (RR = 0.92, 0.91–0.94), were significantly associated with ADRD drug use in non-Deep South beneficiaries. In addition, in this region, Availability of medical resources (Factor 1, RR = 0.97, 0.96–0.98) and Health insurance market (Factor 4, RR = 0.97, 0.96–0.97) were negatively, and Population health (Factor 3, RR = 1.06, 1.05–1.07) was positively, associated with ADRD drug use (p < 0.0001) indicating higher drug use in contexts with fewer medical resources, lower Medicare fee-for-service penetration, and sicker populations.
DISCUSSION
Among older Medicare beneficiaries who received medical care for ADRD in 2013–2015, 40% to about 50% had visits with specialists or filled one or more prescriptions for ADRD drugs in the Deep South and non-Deep South regions of the U.S. Overall, we did not observe racial/ethnic disparities in this care. In addition, different personal and context-level factors may be important to improve access to these elements of ADRD care in these two regions.
Our results may indicate an improvement in use of specialists among older adults with ADRD. A previous study reported that about 15% of 2008–2009 Medicare beneficiaries with ADRD were diagnosed by psychiatrists or neurologists, and only about 22% had specialist visits in the year post diagnosis [5]. Another reported that less than 25% beneficiaries up to 2012 were diagnosed by specialists or had such specialists as predominant clinicians [3, 4]. Our results on ADRD drug use are in line with previous reports that found drug use in at most 60% Medicare beneficiaries in the years 2000s [6–10], and more recently in about 40% of beneficiaries with Alzheimer’s disease and 33% of those with claims for ADRD or ADRD symptoms [10, 19]. While these trends are problematic, an improvement in the utilization of specialists may lead ultimately to higher ADRD drug use, with potential beneficial impact on patient outcomes and lower health care utilization and costs of care [3, 17]. It would be important to examine the association of our ADRD care elements with utilization of ED visits, hospital care, and long-term institutionalization to provide a comprehensive account of care to manage disease and to address physical and cognitive decline for older adults with ADRD across U.S. regions. This would be particularly relevant for beneficiaries in the Deep South who live in contexts with higher overall use of ED and a higher number of hospital and SNF beds. Across regions, we found that use of specialist was lower while ADRD drug use was in general higher in the Deep South than in the non-Deep South. This latter finding on drug use is in line with a previous report for the South region [7]. Because we conducted separate analyses for Deep South and non-Deep-South due to the different contexts identified for the two regions, we did not explain these differences. However, it is worth noticing that the availability of specialists, especially psychiatrists, was lower for beneficiaries in the Deep South, and such availability, reflected in our factor named Availability of medical resources, had a significant association with specialist use. Moreover, due to the lower use of specialists and the prevalent dementia subtypes in the Deep South, especially the lower prevalence of what we termed “senile” dementia, we would have expected lower ADRD drug utilization in this region compared to the non-Deep South. Together, these results suggest that an examination of referral, diagnosing, and prescribing patterns is warranted to better understand differences in ADRD care in the two regions.
In line with others [5], in adjusted analyses we did not find significant differences in specialist use of Black and White beneficiaries within each region. Results on the ADRD drug utilization are somewhat different from previous reports of lower utilization in Blacks and other minorities in the years 2000s [7–9]. Similar to our study, others have found higher utilization in Hispanics; however, these studies also found lower adherence or higher discontinuation for this group [6, 19]. Thus, an analysis of adherence across minority groups in Deep and non-Deep South is warranted. Furthermore, further study of geographic variability in ADRD care utilization within racial/ethnic groups may be worthwhile, in particular to explain the factors that may contribute to the higher use of specialists in Black beneficiaries with ADRD in the non-Deep South.
The contexts in which diverse groups of beneficiaries from the Deep and non-Deep South lived, and in which access to care decisions are made, were different. Others have found that context-level factors, e.g., living in counties designated as health profession shortage or with a higher number of Federally Qualified Health Centers, were associated, for example, with ADRD drug use [6]. Compared to those in the non-Deep South, Deep South beneficiaries were from counties with lower socioeconomic status where affordability of care and availability of medical resources were limited, and where a higher prevalence of disease and disability was accompanied by medical care that may not be accessible or accommodating (as reflected by higher use of ED and hospital care). This context may not be conducive to a continuity of care that is necessary for older adults with dementia, and lead instead to “revolving door” care as described by Pratt et al. [37]. However, only the county availability of specialists was significantly associated with use of specialists in the Deep South. Individual factors had a more prominent role including affordability as indicated by the significant Medicare/Medicaid dual eligibility indicator. This may explain observations of disparities at our institution, where Black patients were less likely to access the memory specialty clinic than white counterparts, thus having less neuroimaging or ADRD drugs ordered [38]. Moreover, none of the context factors were associated with ADRD drug use in the Deep South where some dementia subtypes, seeing a specialist, and existing comorbidities were significant determinants. In the non-Deep South, the contexts we labeled Population health, Availability of medical resources, and Health insurance market, may have an impact albeit low: these results indicated that contexts of poorer population health (i.e., higher number of deaths per capita for a number of common conditions and higher availability of ED and SNF) and of lower medical resources and fee-for-service Medicare penetration, including Part D, were those with higher use of ADRD drugs. These findings deserve further scrutiny to understand the existing underlying characteristics of health care access in each region, i.e., characteristics such as health care availability, accessibility, acceptability, affordability, and accommodation [39]. The factor Population health may reflect contexts in which care is less acceptable by the older population or treatment patterns overall more aggressive. The combination of the factors Availability of medical resources and Health insurance market factor may reflect how accommodating the fee-for-service health care system is and the restrictions that may exist on utilization of specialists and drugs for Medicare beneficiaries with ADRD. While previous studies on quality of care under managed care have reported mixed results [40], it is unknown whether managed care plans provide better access to specialists and ADRD drugs than fee-for-service plans, and whether this practice spills-over to fee-for-service beneficiaries, as suggested by our results for the factor “Health insurance market.” Further quantitative and qualitative analyses should further explore the context of access to care to develop policies and interventions at the system and clinical practice level that can improve the care older Americans with ADRD.
This study has some limitations. Results are not generalizable to beneficiaries on managed care or on fee-for-service Medicare without Part D coverage. In our study period, between a quarter and a third of Medicare beneficiaries were enrolled in managed care plans, and some racial ethnic groups, in particular Hispanics, were overrepresented among the enrollees [40]. Given our findings on the impact of the Health insurance context, the utilization of ADRD specialists and drugs in this population may be higher than what reported here. Moreover, the beneficiaries included in our analyses did not differ in race/ethnicity or residence in the Deep South from all beneficiaries with ADRD we identified in this random sample of Medicare beneficiaries. The exact diagnosis date cannot be established in these data: health care utilization and drug use may vary depending on how far individuals are from their diagnosis. We cannot assess whether beneficiaries had a referral to specialists or a prescription for ADRD drug. We only examined whether ADRD drug prescriptions were filled: we cannot assess if beneficiaries actually used the drugs and were adherent to treatment. In line with others [19], we have included several types of dementia even though ADRD drugs are indicated for Alzheimer’s disease. Moreover, dementia subtypes are defined based on billing codes. Therefore, conclusions about how appropriate the extent to which beneficiaries use ADRD drugs should be made with caution. The geographic level used was constrained by the data available: for example, ADI scores were obtained at ZIP code level, which may be too large to capture the true personal neighborhood disadvantage [41]. Even with this imprecision, we found some associations of the ADI with our outcomes. Some racial/ethnic groups were small (e.g., Asian/Pacific Islanders), especially in the Deep South), and we could not conduct adjusted analyses for these groups. To further understand health care utilization across racial/ethnic groups in the Deep South, a larger sample size is needed. Lastly, health care utilization may be impacted by several factors in combination, but we did not examine interactions among the various factors considered here. Future studies should examine, for example, the interaction of personal and context level factors.
In conclusion, use of specialists for Medicare beneficiaries in the Deep South was lower across all racial/ethnic groups than for beneficiaries not living in this region, while use of ADRD drugs was higher. Within each region, there were no significant differences in this care for Black and White beneficiaries when considering personal- and context-level factors. Larger samples are needed to examine differences in care across other racial/ethnic groups. Some socioeconomic, health, and health care contexts may be important determinants of access to this care and should be further examined for diverse older adults with ADRD in the Deep South and in the rest of the country. Future elucidation of what contributes to ADRD care that is available, accessible, acceptable, accommodating, and affordable, is a must to ensure that this population receives the best ADRD care possible now and in the future.