
Abstract
Background:
Behavioral features may reflect proteinopathies predicting pathophysiology in neurodegenerative diseases.
Objective:
We aimed to investigate associations of cerebrospinal fluid biomarkers of amyloidogenesis and neurodegeneration with neuropsychiatric features in dementia with Lewy bodies (DLB) compared with late-onset Alzheimer’s disease (AD) and cognitively healthy people.
Methods:
Consecutive outpatients with DLB were paired with outpatients with AD according to sex, dementia stage, and cognitive scores, and with cognitively healthy controls according to sex and age to investigate associations of cerebrospinal fluid amyloid-β (Aβ)42, Aβ40, Aβ38, total tau, phospho-tau Thr181, α-synuclein, ubiquitin, and neurofilament light with neuropsychiatric features according to APOE ɛ4 carrier status.
Results:
Overall, 27 patients with DLB (78.48±9.0 years old, eleven APOE ɛ4 carriers) were paired with 27 patients with AD (81.00±5.8 years old, twelve APOE ɛ4 carriers) and 27 controls (78.48±8.7 years old, four APOE ɛ4 carriers); two thirds were women. Behavioral burden was more intense in DLB. Biomarker ratios reflecting amyloidogenesis and neurodegeneration in DLB were more similar to those in AD when patients carried APOE ɛ4 alleles. After corrections for false discovery rates, the following associations remained significant: in DLB, dysphoria was associated with tauopathy and indirect measures of amyloidogenesis, while in AD, agitation, and night-time behavior disturbances were associated with tauopathy, and delusions were associated with tauopathy and indirect measures of amyloidogenesis.
Conclusion:
Biomarker ratios were superior to Aβ and tau biomarkers predicting neuropsychiatric symptoms when associations with isolated biomarkers were not significant. At the end, APOE ɛ4 carrier status influenced amyloidogenesis and tau pathology in DLB and in AD, and axonal degeneration only in DLB.
Keywords
INTRODUCTION
Neuropsychiatric features may reflect underlying amyloidogenesis and neurodegeneration predicting pathophysiologic progression in synucleinopathies [1] and in dementia syndromes [2], potentially measurable by biomarkers. Differences in type and severity of underlying proteinopathies may boost knowledge of disease pathogenesis and determine the most effective therapeutic choices [3].
While amyloid plaques are mainly composed of amyloid-β (Aβ)42, cerebrospinal fluid concentrations of Aβ40 reflect the total generation of Aβ in the brain [4]. Tauopathy follows the detectable imbalance between amyloidogenesis and clearance of Aβ in Alzheimer’s disease (AD) [5], but isolated measures of amyloidogenesis are seldom useful to discriminate between this dementia syndrome and dementia with Lewy bodies (DLB) [6]. Cerebrospinal fluid total tau and phospho-tau Thr181 are increased in AD reflecting axonal degeneration and the formation of ubiquitinated neurofibrillary tangles, respectively, while reduced α-synuclein may reflect the cortical synaptic dysfunction of DLB [7]. Cross-seeding of α-synuclein with tau may lead to their co-existence in intracellular inclusions [3].
Apolipoprotein E influences both the clearance and the extracellular aggregation of soluble Aβ [8], whereas APOE has an influence on tau-mediated disruption of dopaminergic and serotonergic networks by an Aβ-independent mechanism [9]. Nevertheless, APOE mainly influences Aβ deposition rather than gray matter volume or metabolism [10].
Olfaction dysfunction is a common feature to most synucleinopathies, but it is unknown how it correlates with neurodegeneration. In addition, the pathogenesis of neuropsychiatric symptoms in dementia most likely reflects neurochemical consequences of environmental and genetically-mediated pathological mechanisms [4]. Earlier studies showed that cerebrospinal fluid biomarkers may predict future behavioral impairment [11]. We aimed to evaluate associations of cerebrospinal fluid biomarkers of amyloidogenesis and neurodegeneration with neuropsychiatric features in DLB compared with AD and cognitively healthy people.
METHODS
Participants and clinical assessment
In this cross-sectional study, consecutive outpatients with probable DLB according to the fourth consensus report of the DLB Consortium [12] were recruited from the Behavioral Neurology Section of Hospital São Paulo, Federal University of São Paulo (UNIFESP); for these patients, dementia had to start at least one year before the onset of parkinsonism (otherwise, they would have Parkinson’s disease dementia) [2]. After all the patients with DLB were included in the study, they were matched with outpatients with late-onset dementia due to AD from the same center based on National Institute on Aging–Alzheimer’s Association criteria [13]; late-onset AD was considered when dementia started after patients were 65 years old. All patients with dementia had a magnetic resonance exam to exclude vascular lesions and to evaluate either medial parietal or medial, basal, or lateral temporal atrophy, and were matched according to sex and exact scores on the Clinical Dementia Rating [14] and the Mini-Mental State Examination [15]. Furthermore, patients with DLB were matched with cognitively healthy controls by sex and age (±2 years); controls necessarily had to score zero on the Clinical Dementia Rating [14]. All participants were recruited from September 2015 to October 2017.
Patients with dementia could not have other structural brain diseases (such as brain tumors or stroke) and had to be willing to participate on the research (along with their caregivers). Since small vessel disease is very common in the brains of older people, we employed the Modified Ischemic Score (modified version of the Hachinski ischemic score) [16] to exclude vascular dementia or mixed dementia, in which patients with DLB or AD could not score more than 2.
Controls were recruited mostly from the Orthopedics inpatient clinic, and usually had hip or hand fractures, so collection of cerebrospinal fluid took place right before surgery, during anesthetic induction. Controls could not have history of any brain diseases, should be willing to participate and undertake the same neuropsychiatric and motor tests as the patients with dementia.
All participants were assessed for sex, education, use of a cholinesterase inhibitor, memantine, levodopa, anti-psychotic therapy or anti-depressant therapy, hyposmia (reduced subjective sense of smell scored as yes or no), and scores on the Mini-Mental State Examination [15]. Information concerning age at dementia onset was determined following a review of medical records for cognitive and functional decline, and confirmed after an interview with the caregiver, who should have frequent visits with the patient (preferably a family member), so that patients with mild cognitive impairment would not be included. Caregivers also scored the Clinical Dementia Rating [14] and the Neuropsychiatric Inventory [17]. All assessments were conducted on weekdays at morning time, by the same examiner (FFO).
None of the participants could have an active infection, or be using antibiotics or antiviral drugs, so as not to affect the results of Aβ assessment in the cerebrospinal fluid. Participants would also be excluded if collection of cerebrospinal fluid by way of a spinal tap was impossible.
Cerebrospinal fluid analyses
Cerebrospinal fluid collection and biobanking were based on a traditional consensus [18], while reporting was mostly based on traditional guidelines [19]. Basically, withdrawal of approximately 12.0 ml of cerebrospinal fluid from each participant took place after an overnight fast via puncture with a 22-gauge needle in the L3-L4 or L4-L5 interspaces. No serious adverse effects were reported. The first 2.0 ml of cerebrospinal fluid were used for routine analyses of cellularity and biochemistry. Usable samples had to have less than 500 erythrocytes per μl. Samples were collected in separate polypropylene tubes and directly stored in ice, then centrifuged at 2000 g for 10 min, at 4°C, to remove cellular debris and other insoluble materials. Following centrifugation, supernatants of no more than 1.5 ml each were aliquoted to avoid freeze-thaw cycles, and immediately frozen in 2.0 ml polypropylene tubes at –80°C until analyses were performed. Sample storage in the same freezer always took place within two hours of collection of cerebrospinal fluid.
All cerebrospinal fluid analyses were performed randomized and in triplicates (Aβ42, Aβ40, Aβ38, and total tau) or duplicates (phospho-tau Thr181, α-synuclein, ubiquitin, and neurofilament light (NfL)) on the same week for each analyte by two of the authors (FFO and EFCN) who were blinded to the clinical information. For each analyte, one polypropylene tube from each sample was thawed for the first time, and then discarded after the reaction.
Cerebrospinal fluid concentrations of biomarkers were assessed by enzyme-linked immunosorbent assays, as follows: amyloid-beta (Aβ42, Aβ40, Aβ38), (EUROIMMUN, Lübeck, Germany); total tau and phospho-tau Thr181, (INNOTEST ELISA, Fujirebio, Ghent, Belgium); α-synuclein, (BioLegend, San Diego, USA); ubiquitin and NfL (Cloud-Clone, Houston, USA).
The lower limits of detection of all analytes were: Aβ42 (0.1 pg/ml), Aβ40 (0.1 pg/ml), Aβ38 (0.1 pg/ml), total tau (43.3 pg/ml), phospho-tau Thr181 (15.6 pg/ml), α-synuclein (6.1 pg/ml), ubiquitin (0.1 ng/ml), and NfL (6.5 pg/ml). Intra-assay variation (within assay precision for samples that were replicated on the same plate) for each of the analytes was: 6% for Aβ42, 6% for Aβ40, 6% for Aβ38, 10% for total tau, 10% for phospho-tau Thr181, 9% for α-synuclein, 11% for ubiquitin, and 12% for NfL.
Genotyping procedures
After blood was collected from all patients in tubes with ethylenediaminetetraacetic acid 0.1%, genomic DNA was extracted using a standard salting-out procedure for determination of APOE haplotypes after genotyping of rs7412 and rs429358 by way of Real-Time Polymerase Chain Reactions using TaqMan® SNP Genotyping Assays on the Applied Biosystems 7500 Fast Real-Time PCR System (Applied Biosystems, Foster City, CA, USA), following the standard protocols of the manufacturer. All genotyping procedures were carried out only after clinical data were collected from all patients.
Outcome measures
The main outcome measure was the distinctive score in each behavioral domain of the Neuropsychiatric Inventory [17] or the presence or absence of subjective complaint of hyposmia according to variations in cerebrospinal fluid biomarkers or their ratios for each dementia syndrome. Secondarily, we assessed variations in cerebrospinal fluid biomarkers and their ratios according to APOE ɛ4 carrier status.
Statistical analyses
Values of cerebrospinal fluid biomarkers were expressed as absolute and treated as continuous measures; in addition, we analyzed some ratios that might track well with cognitive decline and cumulative brain pathology: Aβ42/Aβ40, Aβ42/Aβ38, total tau/phospho-tau Thr181, total tau/Aβ42, phospho-tau Thr181/Aβ42, α-synuclein/Aβ42, and total tau/α-synuclein. Discrete variables were compared by way of the Chi-square test, while the Mann-Whitney test (for two groups) and the Kruskal-Wallis test (for three groups) were used for comparisons of clinical features and cerebrospinal fluid biomarkers and ratios. Scores of each behavioral domain and subjective complaint of hyposmia were then logarithmically transformed to meet the normality assumptions for a general linear model that was employed for associations of hyposmia or scores in each domain of the Neuropsychiatric Inventory [17] with every biomarker or ratio for each group (DLB, AD, and controls), and adjusted for the following covariates: sex, years of education, age, estimated length of the dementia syndrome, number of APOE ɛ4 alleles and use of psychotropic drugs. Levels of significance from the general linear model were corrected for false discovery rates to minimize the occurrence of type I errors but, due to the preliminary nature of this study, final results were presented with and without the correction. The threshold of significance was set at p < 0.05.
Ethical aspects
This study is part of the research project 0370/2015 (CAAE 43868615.5.0000.5505) approved by the Ethics Committee of Hospital São Paulo, Federal University of São Paulo (UNIFESP), in June 2015, and followed The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. All invited patients and their legal representatives agreed to participate on the research and signed the Informed Consent Form before the evaluation.
RESULTS
Overall, 27 consecutive outpatients with DLB were included, and were paired with 27 outpatients with AD and 27 controls.
Table 1 shows clinical and demographic results from all participants. The mean age was similar for all groups. As expected, patients with dementia had higher Clinical Dementia Rating scores and lower Mini-Mental State Examination scores. Patients with AD used cholinesterase inhibitors and memantine more often, while use of Quetiapine and anti-depressants was more prevalent among patients with DLB. Only patients with DLB used levodopa, but the proportion was low.
Demographic and genetic results
aSD, standard deviation; b Chi-square test; c Kruskal-Wallis test; d Mann-Whitney test.
Table 2 shows the distribution of neuropsychiatric features among all participants. Patients with DLB had significantly higher scores in most domains of the Neuropsychiatric Inventory [17], but particularly in hallucinations and apathy.
Neuropsychiatric features
aSD, standard deviation; bKruskal-Wallis test for differences among neuropsychiatric symptom scores or prevalence of subjective complaint of hyposmia.
Table 3 shows the distribution of cerebrospinal fluid biomarkers and ratios for each group of participants according to APOE ɛ4 carrier status. Levels of Aβ42, Aβ38, total tau, α-synuclein, and ubiquitin were similar for all groups, regardless of APOE ɛ4 carrier status. Only for APOE ɛ4 non-carriers, Aβ42/Aβ38 was significantly higher in DLB; however, Aβ42/Aβ38 was also marginally significantly higher for APOE ɛ4 carriers with DLB than for APOE ɛ4 non-carriers with DLB. Measures of tau pathology in DLB were similar to those in AD when patients carried APOE ɛ4 alleles. The total tau/Aβ42 ratio was marginally significantly higher for all patients with dementia only when they were APOE ɛ4 carriers. The α-synuclein/Aβ42 ratio was lower for patients with DLB and higher for patients with AD only when they did not carry APOE ɛ4 alleles. Levels of ubiquitin and NfL were lower for APOE ɛ4 carriers with DLB than for APOE ɛ4 non-carriers with DLB.
Cerebrospinal fluid biomarkers
aSD, standard deviation; bKruskal-Wallis test for differences among the three groups according to APOE ɛ4 carrier status; c Mann-Whitney test was employed for comparisons between APOE ɛ4 carriers and APOE ɛ4 non-carriers from each group, while the following differences were found for dementia with Lewy bodies: Aβ42/Aβ38 (marginally significant at p = 0.054), total tau/phospho-tau Thr181 (p = 0.030), ubiquitin (p = 0.038), and NfL (p = 0.034); all other differences regarding biomarkers or their ratios were non-significant for dementia with Lewy bodies (p > 0.126), whereas no differences were significant for Alzheimer’s disease (p > 0.107) or controls (p > 0.206).
Tables 4 and 5 show associations between logarithmically transformed scores of neuropsychiatric features and cerebrospinal fluid biomarkers and their respective ratios in patients with dementia. Apathy and appetite and eating abnormalities were the only behavioral symptoms unassociated with any biomarkers or their ratios, whereas ubiquitin was the only biomarker unassociated with any neuropsychiatric features. Figure 1 shows the most representative associations for patients with DLB, while Fig. 2 shows the most representative associations for patients with AD.
Associations between logarithmically transformed scores of neuropsychiatric features and cerebrospinal fluid biomarkers and their respective ratios for patients with dementia with Lewy bodies
General linear model adjusted for sex, years of education, age, estimated length of the dementia syndrome, number of APOE ɛ4 alleles and use of psychotropic drugs: *significant p < 0.05 (uncorrected); **significant p < 0.05 (corrected for false discovery rates).
Associations between logarithmically transformed scores of neuropsychiatric features and cerebrospinal fluid biomarkers and their respective ratios for patients with late-onset Alzheimer’s disease
General linear model adjusted for sex, years of education, age, estimated length of the dementia syndrome, number of APOE ɛ4 alleles and use of psychotropic drugs: *significant p < 0.05 (uncorrected); **significant p < 0.05 (corrected for false discovery rates).
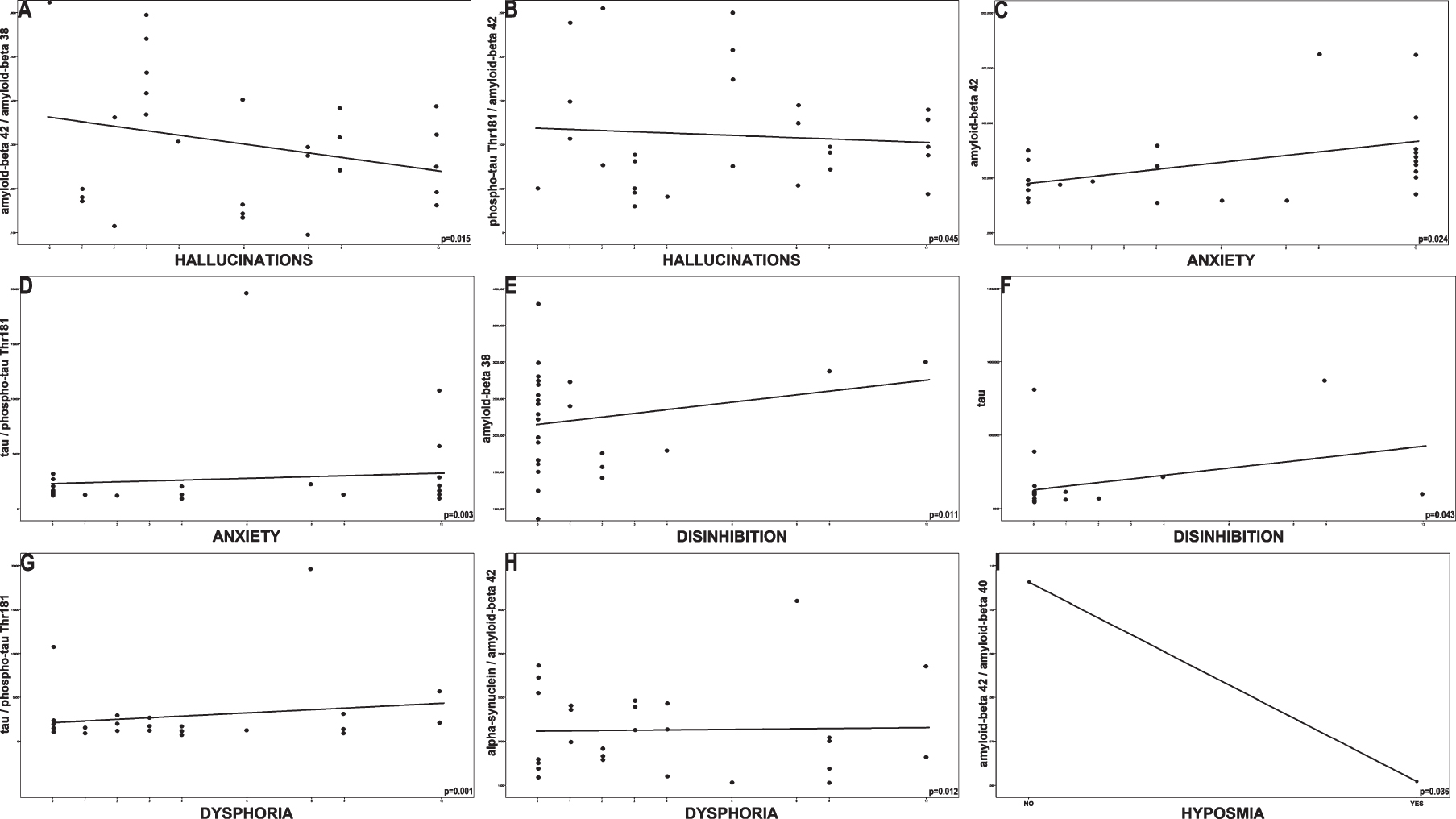
Associations between neuropsychiatric features and cerebrospinal fluid biomarkers and their respective ratios for the group of patients with dementia with Lewy bodies (with raw data and uncorrected p-values). A) Hallucinations were inversely associated with Aβ42/Aβ38. B) Hallucinations were inversely associated with phospho-tau Thr181/Aβ42. C) Anxiety was associated with Aβ42. D) Anxiety was associated with total tau/phospho-tau Thr181 (with a similar scatterplot for total tau/Aβ42). E) Disinhibition was associated with Aβ38. F) Disinhibition was associated with total tau. G) Dysphoria was associated with total tau/phospho-tau Thr181 (with a similar scatterplot for total tau/Aβ42). H) Dysphoria was associated with α-synuclein/Aβ42 (with a similar scatterplot for total tau/α-synuclein). I) Subjective complaint of hyposmia was inversely associated with Aβ42/Aβ40.
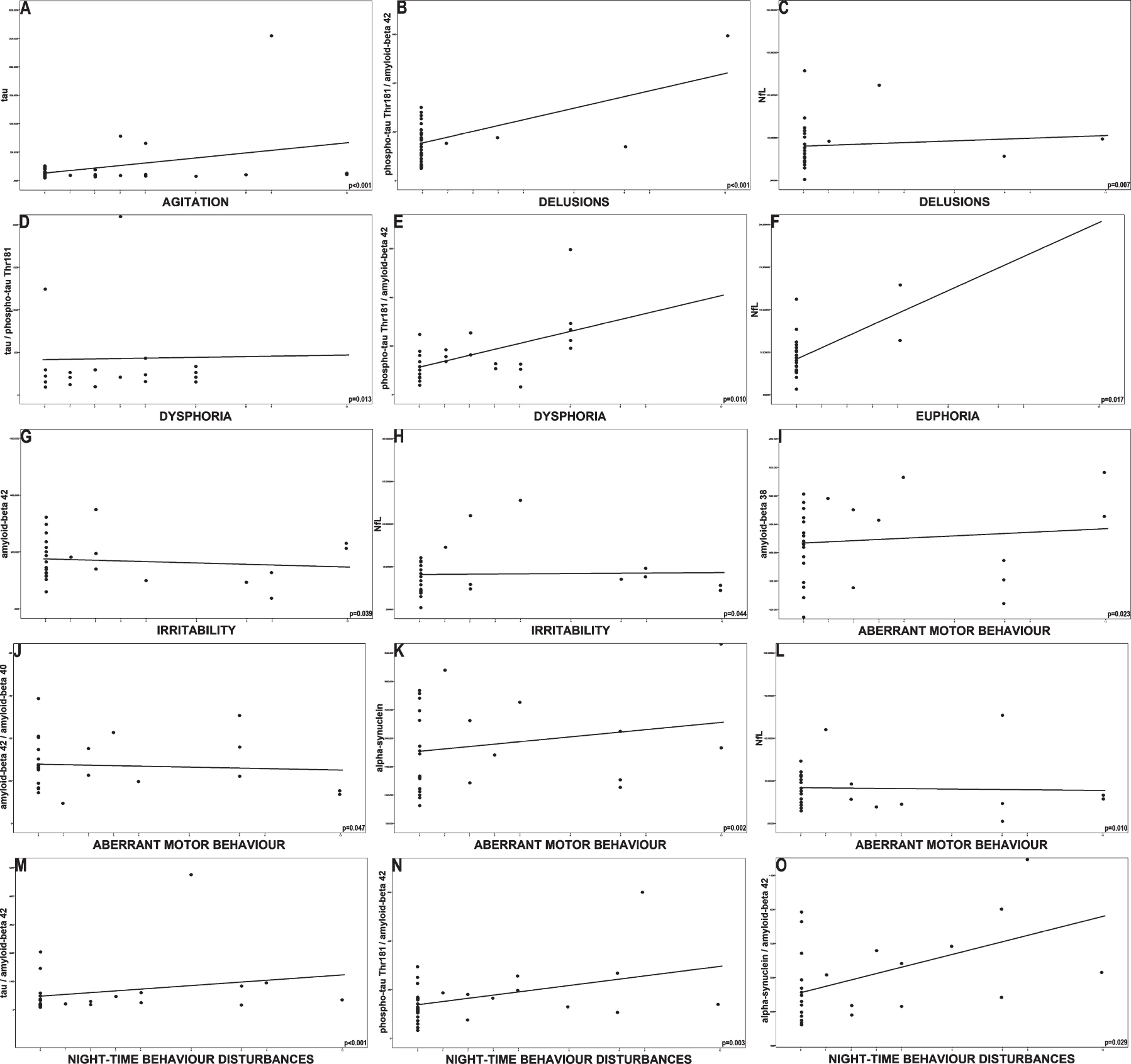
Associations between neuropsychiatric features and cerebrospinal fluid biomarkers and their respective ratios for the group of patients with Alzheimer’s disease (with raw data and uncorrected p-values). A) Agitation was associated with total tau (with similar scatterplots for total tau/phospho-tau Thr181, total tau/Aβ42, and total tau/α-synuclein). B) Delusions were associated with phospho-tau Thr181/Aβ42 (with a similar scatterplot for α-synuclein/Aβ42). C) Delusions were associated with NfL. D) Dysphoria was associated with total tau/phospho-tau Thr181 (with similar scatterplots for Aβ42, total tau, total tau/Aβ42, and total tau/α-synuclein). E) Dysphoria was associated with phospho-tau Thr181/Aβ42. F) Euphoria was associated with NfL. G) Irritability was inversely associated with Aβ42. H) Irritability was associated with NfL. I) Aberrant motor behavior was associated with Aβ38. J) Aberrant motor behavior was inversely associated with Aβ42/Aβ40. K) Aberrant motor behavior was associated with α-synuclein. L) Aberrant motor behavior was inversely associated with NfL. M) Night-time behavior disturbances were associated with total tau/Aβ42 (with similar scatterplots for total tau, total tau/phospho-tau Thr181, and total tau/α-synuclein). N) Night-time behavior disturbances were associated with phospho-tau Thr181/Aβ42. O) Night-time behavior disturbances were associated with α-synuclein/Aβ42.
The following significant trends were observed in patients with DLB: hallucinations were inversely associated with Aβ42/Aβ38 and phospho-tau Thr181/Aβ42; anxiety was associated with Aβ42, total tau/phospho-tau Thr181, and total tau/Aβ42; disinhibition was associated with Aβ38 and total tau; dysphoria was associated with total tau/phospho-tau Thr181, total tau/Aβ42, α-synuclein/Aβ42, and total tau/α-synuclein; and subjective complaint of hyposmia was inversely associated with Aβ42/Aβ40.
The following significant trends were observed in patients with AD: agitation was associated with total tau, total tau/phospho-tau Thr181, total tau/Aβ42, and total tau/α-synuclein; delusions were associated with NfL, phospho-tau Thr181/Aβ42 and α-synuclein/Aβ42; dysphoria was associated with Aβ42, total tau, total tau/phospho-tau Thr181, total tau/Aβ42, phospho-tau Thr181/Aβ42, and total tau/α-synuclein; irritability was inversely associated with Aβ42, whereas euphoria and irritability were associated with NfL; aberrant motor behavior was associated with Aβ38 and α-synuclein, and inversely associated with NfL and Aβ42/Aβ40; night-time behavior disturbances were associated with total tau, total tau/phospho-tau Thr181, total tau/Aβ42, phospho-tau Thr181/ Aβ42, α-synuclein/Aβ42, and total tau/α-synuclein, whereas the absence of hallucinations in patients with AD precluded statistical assessments.
After corrections for false discovery rates, the following results remained significant: in DLB, associations of dysphoria with total tau/phospho-tau Thr181 and total tau/Aβ42; and in AD, associations of agitation with total tau, total tau/phospho-tau Thr181, total tau/Aβ42, and total tau/α-synuclein, associations of delusions with phospho-tau Thr181/Aβ42 and α-synuclein/Aβ42, and associations of night-time behavior disturbances with total tau, total tau/phospho-tau Thr181, total tau/Aβ42, and total tau/α-synuclein.
DISCUSSION
Behavioral features
In this study, we found that patients with DLB had significantly higher scores in most behavioral domains, but particularly in hallucinations and apathy, as expected [20], leading to more frequent use of anti-psychotics and anti-depressants. One study had shown that underlying synuclein pathology was associated with hallucinations and poor executive function in patients with AD [7] but, since we had no patients with AD with hallucinations, our sample was probably more proper for comparisons with DLB. Furthermore, appetite and eating abnormalities and apathy were the only neuropsychiatric symptoms unassociated with any biomarkers or their ratios, consistent with some [21] but not all [22] studies. One of the reasons for this discrepancy might be that most of our patients were in the mild and moderate dementia stages while, apparently, apathy is more strongly associated with amyloidogenesis in severe dementia [23].
Cerebrospinal fluid biomarkers
In accordance with the literature, only patients with AD had mean total tau/Aβ42 > 0.52 [24], but marginally significantly higher than in DLB only for APOE ɛ4 carriers [25]. Aβ42 and Aβ42/Aβ40 are usually lower in AD [26], but we did not find significant differences among our groups regardless of APOE ɛ4 carrier status. Concomitant amyloid pathology in DLB improves prediction of linguistic and cognitive dysfunction [27] and limits the use of cerebrospinal fluid measures of amyloidogenesis for differential diagnosis [28]. As biomarkers lose specificity with increasing age [29], the fact that our patients and controls were relatively old might have produced even less significant differences.
APOE ɛ4 carrier status affected Aβ42/Aβ38 and determined similar tauopathy for DLB and AD particularly when they were APOE ɛ4 carriers. This is an original finding that reflects analogous pathophysiological mechanisms in DLB and AD, though effects of APOE ɛ4 over measures of neurodegeneration and mostly amyloidogenesis had been previously described for cognitively healthy older people [30]. Likewise, an original study had shown that Aβ38 could potentially distinguish between AD and DLB when combined with Aβ42, but not in isolation [31].
Aggregated α-synuclein is the major component of Lewy bodies [32], but it is not well known if Lewy body α-synuclein affects cerebrospinal fluid α-synuclein levels; conflicting results from different studies may be due to the examination of different isoforms of α-synuclein [33]. In our findings, APOE ɛ4 carrier status influenced α-synuclein/Aβ42 but not total tau/α-synuclein in DLB, probably reflecting the fact that tauopathy in DLB is more similar to AD and less affected by APOE ɛ4 carrier status than amyloidogenesis. In synucleinopathies, cerebrospinal fluid tau does not tend to rise from the earliest stages because tau is colocalized with α-synuclein [32]; furthermore, α-synuclein increases cellular secretion of Aβ, whereas Aβ may stimulate the aggregation of α-synuclein [3], both mechanisms possibly affected by APOE ɛ4 carrier status.
Levels of NfL correspond to non-specific large-caliber axonal damage associated with aging or neurological diseases, may be involved in the formation of Lewy bodies, and have proven discriminative value in Parkinson’s disease [34] and dementia syndromes [35]. In addition to biomarkers of amyloidogenesis and tauopathy, NfL may help discriminate AD from cognitively healthy people [36]. In our sample, levels of NfL in patients with DLB were affected by APOE ɛ4 carrier status. Furthermore, an original finding in patients with DLB was that subjective complaint of hyposmia was associated with measures of amyloidogenesis. One study [37] with patients with Parkinson’s disease found independent associations of early psychotic symptoms with hyposmia and amyloidogenesis, while another [3] did not find biomarker correlations with standardized smell identification assessments, but these associations might be more significant for patients with dementia.
Ubiquitin is present in Lewy bodies and neurofibrillary tangles [38], but its cerebrospinal fluid levels were not associated with any neuropsychiatric symptoms reflecting probable lack of usefulness to predict pathophysiology. Isolated biomarkers were not useful to distinguish dementia syndromes in this study, possibly due to underlying amyloid pathology in all participants resulting from their older age, but also potentially due to our modest sample size. Nevertheless, biomarker ratios had several significant associations with behavioral features, confirming the expected pathophysiological links.
Associations of behavioral features with cerebrospinal fluid biomarkers in DLB
Considering that we detected hallucinations only in patients with DLB, and inversely associated with Aβ42/Aβ38, we assume that amyloidogenesis may lead to more hallucinations in these patients, but these results did not survive multiple correlations.
Depression supports clinical diagnosis of DLB but might be a risk factor for both DLB and AD [2]. In our findings, dysphoria was associated with tauopathy in dementia syndromes, but only in DLB did this association survive multiple correlations. In contrast, one study showed APOE-adjusted evidence of amyloidogenesis but not tauopathy in patients with mild cognitive impairment who had chronic subsyndromal symptoms of depression [39], suggesting early associations of depression with amyloidogenesis, while our findings would correspond to late associations with tauopathy.
Only in DLB, anxiety was associated with tauopathy but also with evidence of amyloidogenesis, which is in line with an earlier study with patients who had mild cognitive impairment [21]. Exclusively in patients with DLB, disinhibition was associated with tauopathy. Nevertheless, these associations did not survive multiple correlations.
Associations of behavioral features with cerebrospinal fluid biomarkers in AD
Agitation was strongly associated with tauopathy in AD even after corrections for false discovery rates, supporting its importance as the most consistent behavioral symptom related with cerebrospinal fluid biomarkers in AD [22, 40].
Though we could not assess hallucinations in AD, one study showed that APOE ɛ4 alleles induce psychosis in women with AD through the formation of Lewy bodies [41]. Furthermore, delusions were associated with indirect measures of amyloidogenesis, tauopathy and axonal degeneration only in patients with AD.
Only in AD was irritability associated with measures of amyloidogenesis and axonal degeneration, but none of these associations survived multiple correlations. One study found an association of low baseline Aβ42 with prospective improvement in irritability in AD [4], while frontal-lobe-mediated behavioral dysfunction is not associated with hippocampal atrophy and might precede this pathological change [21], particularly in non-AD dementias.
It has been reported that increased brainstem α-synuclein may be associated with REM sleep behavior disorder in patients with Parkinson’s disease [3], but behavioral symptoms affect sleep satisfaction in both AD [42] and DLB [2]. The magnitude of night-time behavior disturbances is implicitly linked to metabolic dysfunctions within limbic networks vulnerable to AD pathophysiology [42], corresponding to our finding that night-time behavior disturbances were associated with measures of tauopathy and synucleinopathy only in AD.
Only in AD, aberrant motor behavior was associated with evidence of amyloidogenesis (but not after corrections for multiple correlations), though its associations with indirect measures reflecting less synucleinopathy or axonal degeneration could be explained by other mechanisms such as synaptic dysfunction or neuronal loss, or also by lower test scores. Nonetheless, it has been reported that up to 30% of patients with AD present fluctuating neuropsychiatric symptoms despite similarity in APOE ɛ4 carrier status, tauopathy, and amyloidogenesis [43].
Final considerations
Patients with AD had higher levels of education while patients with DLB had lower levels of education, possibly due to chance because this is not a consistent finding in the literature [20] and only patients with DLB were consecutively recruited. Furthermore, the effects of education over behavioral symptoms in dementia are controversial [9].
Patients with AD used cholinesterase inhibitors and memantine more often and, as expected [44], had less neuropsychiatric symptoms; however, since we corrected our analyses for the use of psychotropic drugs, our results were hardly compromised. Cholinesterase inhibitors do not seem to affect cerebrospinal fluid biomarkers, but the same cannot be said about Risperidone [4]; despite this issue, some of our patients used Quetiapine and Olanzapine, but not Risperidone.
The cross-sectional nature of this study is a limitation, though it has been demonstrated that baseline values of most biomarkers are usually correlated with their own estimated longitudinal changes [3]. We tried to minimize this setback by matching patients in the same dementia stage and adjusting our analyses by demographic and genetic confounds, thus preventing biased effects of APOE ɛ4 alleles over neuropsychiatric symptom scores in different dementia stages [9]. Other limitations include the fact that all participants came from the same center, and the relatively small sample size, though our study was powered to identify significant differences for many associations.
Overall, biomarker ratios were superior to Aβ and tau biomarkers predicting neuropsychiatric symptoms when associations with isolated biomarkers were not significant, but similar when these associations were significant. APOE ɛ4 carrier status influenced amyloidogenesis and tau pathology in DLB and in AD, but associations of measures of axonal degeneration with neuropsychiatric features were observed only in patients with AD. Future longitudinal studies should address whether the uneven associations of behavioral symptoms with these biomarkers may be modified by pharmacological therapy.
PRIOR PRESENTATION OF INFORMATION FROM THE PAPER
Preliminary aspects of this study were previously presented (and published in the form of abstracts) at the following meetings:
1. TAU>2020 Global Conference
(Alzheimer’s Association, Washington/USA, February 2020)
2. AAIC>19 – Alzheimer’s Association International Conference 2019
PODIUM PRESENTATION
(Alzheimer’s Association, Los Angeles/USA, July 2019)
https://doi.org/10.1016/j.jalz.2019.06.4462
2020 Lewy Body Dementias PIA Day (vimeo): https://player.vimeo.com/video/434857973
3. AAIC>18 – Alzheimer’s Association International Conference 2018
(with an Alzheimer’s Association Travel Fellowship to the first author)
(Alzheimer’s Association, Chicago/USA, July 2018)
https://doi.org/10.1016/j.jalz.2018.06.912
4. 70th Annual Meeting of the American Academy of Neurology
(American Academy of Neurology, Los Angeles/USA, April 2018):
https://n.neurology.org/content/90/15_Supplement/P4.190
5. 3rd Congress of the European Academy of Neurology
ORAL PRESENTATION
(European Academy of Neurology, Amsterdam/NETHERLANDS, June 2017)
https://doi.org/10.1111/ene.13367
Press Release (VJDEMENTIA):
Footnotes
ACKNOWLEDGMENTS
This work was sponsored by FAPESP–The State of São Paulo Research Foundation (grant #2015/10109-5 and grant #2015/18125-0).
This study is part of the research project 0370/2015 (CAAE 43868615.5.0000.5505) approved by the Ethics Committee of Hospital São Paulo, Federal University of São Paulo (UNIFESP), in June 2015. All invited patients and their legal representatives agreed to participate on the research and signed the Informed Consent Form before the evaluation.
The sponsor had no role in study design, in data collection, in analysis and interpretation of the data, in the writing of the report, or in the decision to submit the paper for publication.