
Abstract
Background:
While most intervention studies conducted with dementia family caregivers have focused on depressive symptoms as the main outcome, no study has analyzed the effects of an intervention on comorbid clinical presentations of depressive and anxious symptomatology.
Objective:
The aim of this study was to examine the association between clinical depressive and anxious symptomatology at baseline and treatment responses of dementia family caregivers using samples from two randomized intervention trials with the same pre-post design.
Methods:
Specifically, the effects on depressive and anxious comorbidity of three intervention conditions (Cognitive Behavioral Therapy (CBT), Acceptance and Commitment Therapy (ACT), and a control group (CG)) were analyzed. Participants were 130 dementia family caregivers. In addition to sociodemographic variables, depressive and anxious symptomatology were measured.
Results:
Caregivers with clinical depressive and anxiety comorbid symptoms at baseline recovered less well from depressive symptoms after CBT (45.45%) and ACT (47.72%) interventions than caregivers with non-comorbidity (100% recovery in both treatments). No significant association between comorbidity and treatment responses on depression was found for the control group. Regarding anxiety, among participants with comorbidity at baseline, 36.36% of caregivers in CBT and 30.9 % in the ACT group recovered from anxiety symptoms after treatment, compared to 6.45% in the control group. Similar results were obtained regarding those caregivers who recovered both from clinical depressive and anxiety symptoms and showed comorbidity at baseline.
Conclusion:
Caregivers that show comorbid depressive and anxiety symptoms at baseline may benefit less from interventions than caregivers who do not show comorbidity.
Keywords
INTRODUCTION
Caregivers of relatives with dementia are considered to be in a vulnerable situation for suffering psychological problems due to the fact that they have to face many demanding tasks and are exposed to many difficult situations over years and for several daily hours [1], a challenging situation for their available coping resources [2, 3]. Consequently, providing care for a relative with dementia is considered to be a chronic stressful situation associated with negative consequences for caregivers’ psychological and physical health [4, 5].
Much of the caregiving literature has focused on analyzing depression or depressive symptoms as the main psychological outcome, with high reported prevalence rates for depressive disorders [6, 7]. Although less attention has been paid to anxiety in the caregiving literature, high prevalence estimates have also been reported for this emotional problem [7–9], which seems to be even more frequent than depression [10]. However, the number of studies analyzing emotional comorbidity (i.e., the simultaneous presentation of depressive and anxious symptomatology) in caregivers of relatives with dementia is limited. In a two-year longitudinal study, Joling et al. [10] found an incidence of comorbid depressive and anxious disorders of 32%. More recently, Barrera-Caballero et al. [11] have reported 54.79% of comorbid presentations of clinically significant depressive and anxious symptoms. In spite of the above, studies linking the simultaneous or comorbid presence of depressive and anxiety symptomatology among dementia family caregivers and treatment effects are lacking. A randomized controlled study conducted by Márquez-González et al. [12], in which 94.55% of the family dementia caregivers presented mixed depressive and anxiety comorbidity symptoms at baseline, found positive effects of an individualized modular intervention (Functional Analysis-guided Modular Intervention, FAMI), as compared with two manualized interventions, concerning comorbidity of depressive and anxious symptomatology, especially for maintaining the therapeutic benefits in the long term [12].
Several psychological interventions for dementia caregivers are empirically validated and recognized for decreasing depressive symptoms, the most commonly studied outcome variable in this field. Specifically, Cognitive Behavioral Therapy (CBT) has been shown to be effective for decreasing caregivers’ distress, showing large effect sizes for individual interventions [13–15]. On the other hand, although Acceptance and Commitment Therapy (ACT) intervention studies in dementia caregiving are sparse, there is empirical support showing that this therapy approach has a large effect on depressive symptoms and anxiety outcomes compared to control conditions [6, 14]. However, there are no current studies that analyze the impact of CBT or ACT on comorbid symptoms in dementia family caregivers.
Considering that intervention studies conducted with non-caregiving populations show that the comorbid presentation of depressive and anxiety symptoms has a negative impact on treatment outcomes [16], studies analyzing the effects of comorbidity on treatment response are needed. Specifically, in a non-caregiving population, Brown et al. [16] found that patients with comorbid anxious and depressive disorder tended to terminate treatment prematurely, needed longer to recover and showed a poorer response to treatment (psychotherapy or pharmacotherapy) than patients with major depression alone. The interventions analyzed in these studies may be more focused on therapeutic strategies to reduce either depressive or (to a lesser extent) anxious symptoms, and thus may fail to address the core mechanisms underlying the comorbidity. Treatments addressing these core processes that are common to anxiety and depressive symptoms, such as the above-mentioned FAMI, have been found to be more effective for reducing comorbidity in family caregivers of people with dementia in the long term [12]. There is a need for studies analyzing the role of co-occurring comorbidity symptomatology in treatment responses in order to guide research toward design of better-targeted treatments that are more likely to generate positive efficacy results in this vulnerable population [17], in which there are no studies.
Studies in the field of dementia caregiving research would be useful as the presence of comorbid symptomatology could make caregivers especially vulnerable to suffering from other negative consequences of caring (i.e., higher presence of suicidal thoughts in caregivers) [18].
The aim of this study is to analyze whether clinically significant levels of comorbid depressive and anxious symptoms at pre-intervention is a relevant issue for predicting caregivers’ response to psychological treatment. To this end, data was drawn from previous randomized controlled studies that shared the same pre-post intervention design, comparing two different types of psychological interventions (CBT and ACT) with a control group [12, 14]. The main hypothesis of the study is that depressive and anxiety comorbid symptomatology will be associated with worse treatment responses in outcomes (depressive and anxious symptomatology) of both CBT and ACT programs.
METHODS
Participants and procedure
The participants in this study were recruited in the context of two previous randomized controlled trials aimed at developing and analyzing different psychological interventions (CBT, ACT, and FAMI) [12, 14] that shared the same pre-post intervention design. Specifically, data from 130 family caregivers of people with dementia were recruited through different social and health centers in the Community of Madrid. Inclusion criteria to participate in this study were: 1) identifying themselves as the main family caregiver of the cared relative; 2) devoting at least one daily hour in caregiving tasks during at least three consecutive months; 3) being at least 18 years old; 4) having participated voluntarily in one of the two previously mentioned intervention studies [12, 14]. In addition, an inclusion criterion for the two randomized controlled trials in which this study was framed was the presentation of baseline clinical depressive symptomatology (scores equal or higher to 16 in the CESD scale), but no specific criterion regarding baseline clinical anxiety symptomatology was included. Informed consents were obtained from all participants. Both clinical trials were approved by the Spanish Ministry of Economy and Competitiveness and the Ethics Committee of the Universidad Rey Juan Carlos.
The two studies shared the same methodological conditions regarding the intervention conditions (ACT, CBT, and control group). The first study consisted of a randomized controlled intervention study analyzing effects of two individual ACT and CBT interventions as compared to a control group (for a more detailed description of the study design, see Losada et al. [14]). The second intervention study compared the same individual ACT and CBT interventions and control group as in the first study, which were compared with a tailored modular intervention (FAMI) (for more information, see Márquez-González et al. [12]). The data from the FAMI intervention condition are not included in the present study. The design of the studies and the characteristics of each intervention in both research projects were the same. Both consisted of eight weekly individual two-hour sessions. The CBT intervention was developed based on previous interventions [19] and drawing upon the theoretical framework of the cognitive-behavioral model of caregiver distress [20]. Specifically, the CBT intervention consisted of four components or modules aimed at: 1) increasing the frequency of pleasant activities using behavioral activation techniques; 2) using cognitive restructuring for changing maladaptive thoughts about caregiving (e.g., “It is selfish for a caregiver to dedicate time to himself/herself when a relative is frail/sick and needs care”) into new ones that promote a more adaptive ways of thinking in order to increase functional coping strategies in the stress process (e.g. “Dedicate time to oneself when a relative is frail is a need and an excellent way of self-care in order to keep caring for a relative properly”); 3) promoting assertiveness skills (e.g., asking for help for sharing some caregiving tasks); and 4) providing relaxation techniques for reducing physiological activation.
The ACT intervention was specifically developed for dementia family caregivers (see Márquez-González et al. [21]) based on the therapeutic framework described by Hayes et al. [22] and the previous study with dementia caregivers conducted by McCurry [23]. The ACT based intervention was tested in Losada et al. [14] and Márquez-González et al. [12]. The ACT intervention consisted of three main modules: 1) acceptance of aversive internal events (emotions, sensations, and thoughts); 2) choosing meaningful courses of action consistent with one’s personal values; and 3) action oriented toward those values. Caregivers were trained to identify personal sources of experiential avoidance through experiential and cognitive defusion exercises and metaphors. In addition, the trap of control and the cost of the avoidant behaviors were analyzed, and acceptance strategies were taught. Simultaneously, caregivers were trained to identify personal values and barriers to engaging consistently with them and to increase actions consistent with these values.
In addition, the control groups of both projects shared the same format: a minimal support control group. Specifically, caregivers in the control group received a two- to three-hour workshop in a group format which consisted of psychoeducation about basic information of dementia (e.g., definition and description of dementia and behavioral and psychological symptoms of dementia and recommendations for managing dependency). This group did not receive a therapeutic intervention. Therefore, given that ACT, CBT, and the control group in these clinical intervention projects shared the same methodological conditions, data from these three conditions of the two different projects were selected and merged to conduct the analyses of this study. Specifically, pre- and post-intervention data were available for 41 participants in CBT, 49 in ACT, and 40 in the control group. Given that one of the inclusion criteria to participate in the different intervention clinical trials was that caregivers should report clinically relevant depressive symptoms (scores equal or high than 16 in the CES-D), all participants in this study presented clinical depressive symptoms.
Measures
In addition to sociodemographic variables (age of caregivers, sex, kinship, economic conditions, years studied, perceived health, daily hours caring, time since care began), the following variables were evaluated:
Frequency and reaction to disruptive behaviors. The frequency and reaction subscales of the disruptive behavior factor of the Revised Memory and Behavior Problems Checklist [24] in its Spanish version [25] were used. The frequency subscale consists of 8 items assessing how often the care-recipient present observable disruptive behaviors (e.g., destroy property) with answers ranging from 0 (never occurred) to 4 (occurs daily or more often). The reaction subscale consists of 8 items measuring caregivers’ distress or reaction associated to such disruptive behaviors (e.g., “how much this behavior upset you”), with responses ranging from 0 (not at all) to 4 (extremely). Cronbach alphas in this study for the frequency and reaction subscale were 0.55 and 0.75, respectively.
Depressive symptoms. The Spanish version [26] of the Center for Epidemiological Studies-Depression Scale (CES-D) [27] was used. It consists of 20 items assessing caregivers’ depressive symptoms levels during the last week with scores ranging from 0 (rarely or none of the time) to 3 (most or all of the time). Scores equal to or higher than 16 constitute the cut-off suggesting clinical depression [28]. In this study, Cronbach’s alpha was 0.87.
Anxiety symptoms. This was assessed using the Tension-Anxiety subscale from the Profile of Mood States (POMS) [29] in its Spanish version [30]. It consists of 9 items assessing caregivers’ anxiety levels during the last week with scores ranging from 0 (not at all) to 4 (extremely). Scores equal to or higher than 13 are indicative of clinical levels of anxiety symptoms [14]. Cronbach’s alpha found in this study was 0.89.
Measure of treatment response. We consider depressive symptoms recovered when caregivers presented scores less than 16 on the CES-D scale [27] after treatment. In addition, recovery from anxiety symptoms was considered when caregivers scored less than 13 on the POMS scale [29] at post treatment.
Data analysis
First, following Tabachnick and Fidell [31] criteria, normality and univariate and multivariate outliers were analyzed. Differences in the sociodemographic, stressors, treatment conditions, and outcome-assessed variables between caregivers with baseline depressive and anxious comorbid symptoms and non-comorbid symptoms (only depressive symptoms) were assessed using mean differences test (t-test) and independent test (χ2). The comorbid presentation of depressive and anxious symptomatology was considered when participants showed equal or higher scores than 16 in the CES-D [27] and 13 in the POMS [29]. In addition, the associations between comorbid depressive and anxiety symptoms at baseline and depression recovery after treatment (presenting depressive symptoms scores below 16 on the CES-D scale after intervention) were analyzed for each condition group (CBT, ACT, and control group) using the chi-squared test. As mentioned above, due to the design of the study, all caregivers presented depressive symptoms at baseline to participate in the study but presenting anxiety symptomatology at baseline was not an inclusion criterion. For this reason, the association between treatment response on anxiety (caregivers who recovered presented scores below 13 on the POMS scale after treatment) by condition groups (CBT, ACT, and control group) was analyzed only in caregivers with baseline comorbid symptoms using the chi-squared test. In addition, the association between treatment response on mixed depressive and anxiety comorbidity by condition groups was also tested in caregivers with baseline comorbid symptoms using chi-squared test. Specifically, the proportions of participants recovered from depression and anxiety were tested, considering as recovery scores under 16, the clinical cut-off point in the CES-D for depression, and under 13 in the POMS for anxiety. The treatment response for combined depressive and anxiety comorbidity was calculated scoring simultaneously < 16 on the CES-D and < 13 on the POMS in participants showing comorbid symptomatology at baseline assessment.
RESULTS
Differences between caregivers with comorbid and non-comorbid symptoms in the assessed variables at baseline
Table 1 shows differences between caregivers with depressive and anxious comorbid symptoms and caregivers with non-comorbid symptoms in the baseline study variables. The rates of caregivers with depressive and anxiety comorbid and non-comorbid (depressive but not anxiety symptoms) were 81.54% and 18.46%, respectively. Results show that caregivers in the comorbid group were younger (t = 2.18; p < 0.05) and presented higher frequency of (t = –2.64; p < 0.01) and distress associated with (t = –3.39; p < 0.01) disruptive behavioral problems than the non-comorbid group. No significant differences between comorbid and non-comorbid groups were found in time since caring (t = –0.64; p = 0.52), hours caring (t = 0.41; p = 0.68), years studied (t = 0.56; p = 0.57), economic conditions (t = –0.17; p = 0.87) and perceived health (t = 1.04; p = 0.30). In addition, no sex (χ2 = 0.90; p = 0.34) nor kinship (χ2 = 3.16; p = 0.21) differences were found between comorbid and non-comorbid groups. The comorbid caregivers group presented higher depressive (t = –4.61; p < 0.01) and anxiety symptoms (t = –11.32; p < 0.01) than the non-comorbid group. Finally, no significant differences between comorbid and non-comorbid presentations were found for intervention conditions (χ2 = 1.03; p = 0.60).
Sociodemographic differences for comorbidity and no comorbidity in caregiver groups at pretreatment. N = 130
Differences between caregivers with comorbid and non-comorbid symptoms in depression recovery
Table 2 shows the associations between baseline caregivers’ comorbid symptoms and caregivers’ recovery in depressive symptoms after treatment by condition groups. Significant differences were found between caregivers’ comorbidity and depressive symptoms recovery for both CBT (χ2= 5.73; p < 0.05) and ACT (χ2 = 5.63; p < 0.05) groups. Specifically, caregivers with comorbidity symptoms recovered less well from depressive symptoms after intervention in both CBT (45.45%) and ACT (47.72%) conditions, as compared to caregivers with no comorbidity, who recovered 100% in both conditions. No significant differences were found for the control group (χ2 = 1.15; p = 0.28), in which 25.81% of caregivers with comorbidity symptoms recovered from depressive symptoms, as compared to the 44.44% of caregivers with no comorbidity that recovered. Figure 1 shows the percentage of comorbid and non-comorbid caregivers who recover from depressive symptoms by conditions groups.
Differences in depression recovery by comorbidity and treatment groups
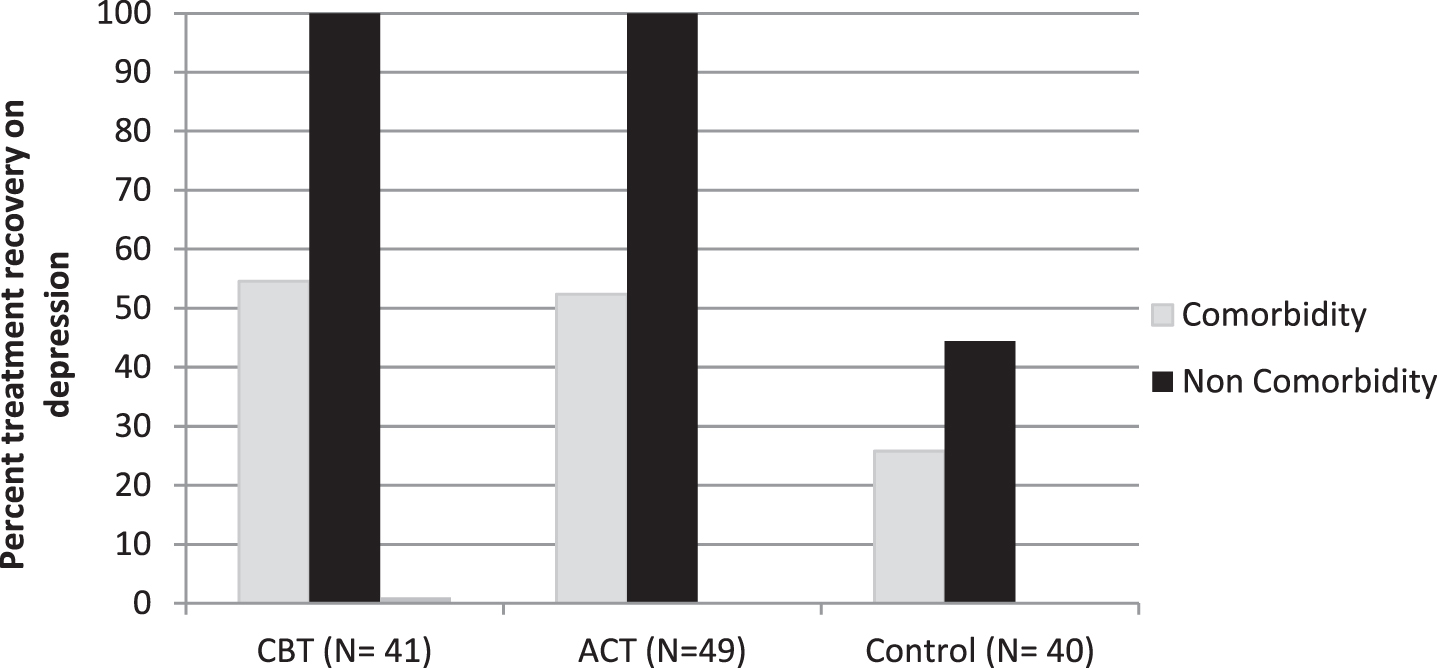
Percentage of participants responding in depression at post treatment by comorbidity at pre-intervention and intervention groups.
Regarding differences by treatment condition on depression recovery, significant differences among caregivers with comorbidity at baseline were found in depression recovery between caregivers in the control group versus ACT (χ2 = 5.20, p < 0.05) and CBT (χ2 = 5.47, p < 0.05), with lower rates for both cases found in the control group. No significant differences were found among caregivers with baseline comorbidity between caregivers in the ACT versus CBT groups (χ2 = 0.04, p = 0.85) in rates of depression recovery. Along the same lines, recovery rates in the case of non-comorbid caregivers were the same for CBT and ACT conditions (100% for both), and a lower recovery rate was found in the control condition (44.44%). Specifically, among caregivers with non-comorbidity at baseline, significant differences in rates of depression recovery between caregivers in the control group versus ACT (χ2 = 5.66, p < 0.05) and CBT (χ2 = 6.30, p < 0.05) were found, with lower rates in both cases for the control group.
Differences in anxiety treatment response in caregivers with depressive and anxiety comorbid symptoms at baseline by treatment condition
Results show significant associations between recovery from anxiety after treatment and condition groups (CBT, ACT, and control) in caregivers with depressive and anxiety comorbidity in baseline scores (see Table 3). Specifically, results show that 36.36% and 35.71% of caregivers with previous comorbidity recovered from anxiety symptoms after treatment in CBT and ACT conditions, respectively. Only 6.45% of caregivers recovered in the control group. Figure 2 graphically represents rates of recovery from anxiety by groups. Results show that among caregivers with comorbidity at baseline, significant differences in rates of anxiety recovery between caregivers in the control group versus ACT (χ2 = 8.55, p < 0.01) and CBT (χ2 = 8.37, p < 0.01) were found, with lower rates found for both cases in the control group. No significant differences in rates of anxiety recovery between caregivers in the CBT versus ACT groups (χ2 = 0.003, p = 0.95) were found.
Differences in anxiety recovery in participants with comorbidity by treatment groups
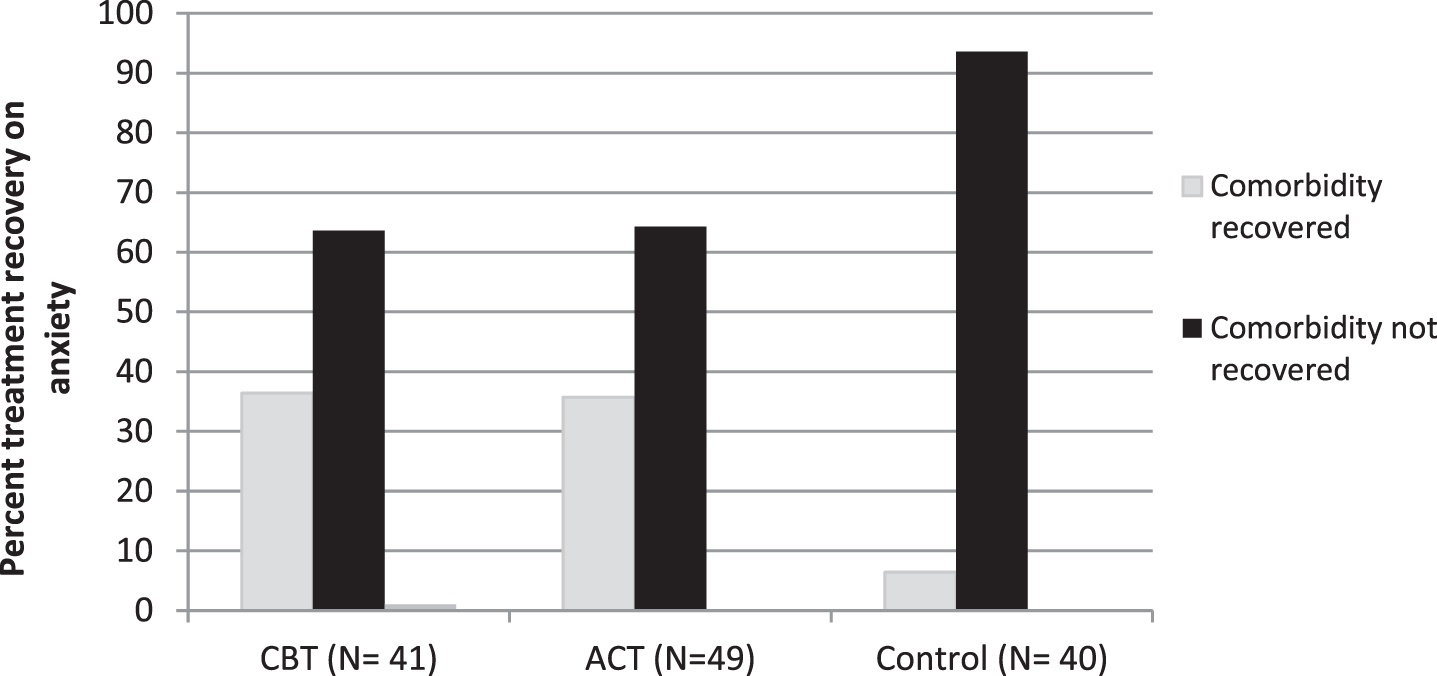
Percentage of participants with comorbidity recovered and not recovered in anxiety by intervention groups.
Differences in combined depressive and anxiety treatment response in caregivers with depressive and anxiety comorbid symptoms at baseline by treatment condition
The treatment response for simultaneously or combined depressive and anxiety symptoms was calculated in caregivers with depressive and anxiety comorbid symptoms at baseline for each treatment condition.
Results show significant associations between combined depressive and anxiety recovery after treatment and condition groups in caregivers with depressive and anxiety comorbid in baseline scores (see Table 4). Results show that 36.36% and 30.95% of caregivers with previous comorbidity recovered from depressive and anxiety comorbidity after treatment in CBT and ACT conditions, respectively, while 6.45% of caregivers recovered in the control group. Figure 3 graphically shows rates of recovery on depressive and anxiety comorbidity by groups. Among caregivers with comorbidity at baseline, significant differences on rates of depressive and anxiety comorbidity recovery were found between caregivers in the control group versus ACT (χ2 = 6.56, p < 0.05) and versus CBT (χ2 = 8.37, p < 0.01), with lower rates found for both cases in the control group. There were no significant differences in rates of anxiety recovery between caregivers in the CBT versus ACT groups (χ2 = 0.24, p = 0.62).
Differences in mixed depressive and anxiety comorbidity recovery in participants with comorbidity by treatment groups
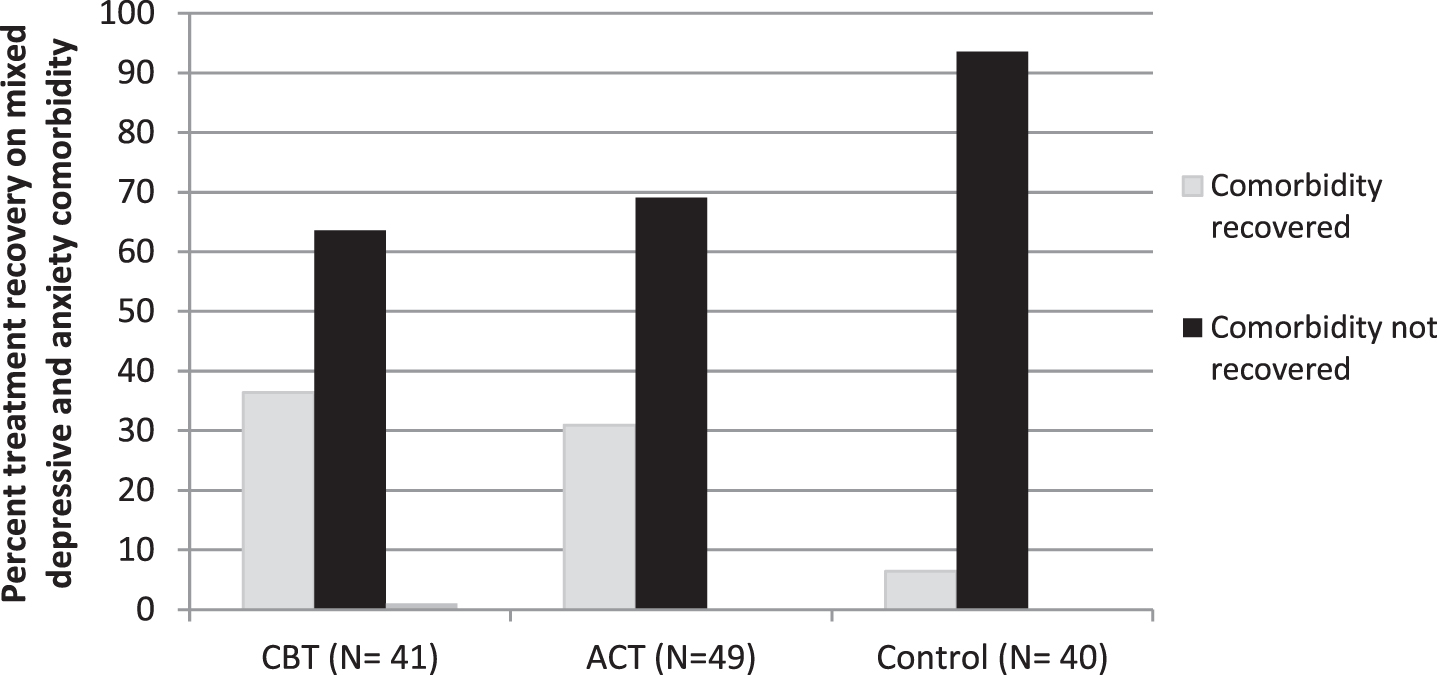
Percentage of participants with comorbidity recovered and not recovered in mixed depressive and anxiety comorbidity by intervention groups
DISCUSSION
The aim of this study was to analyze the role of baseline depressive and anxiety comorbid symptoms on treatment responses in family caregivers of people with dementia. Consistent with our hypotheses, the results of this study suggest that caregivers with comorbid baseline depressive and anxious symptomatology present a worse response to individual psychological interventions, as compared to caregivers with no comorbid symptoms, for both types of interventions analyzed: CBT and ACT. Specifically, the results show that, while almost half of the caregivers with comorbid symptoms showed a significant recovery in depressive symptoms in CBT (54.54%) and ACT (52.38%) conditions, 100% of caregivers with non-comorbid symptoms recovered in both types of interventions. These rates contrast with those found in the control group, in which 25.8% and 44.44% of caregivers with comorbid symptoms and non-comorbid symptoms, respectively, recovered from depressive symptoms. It is noteworthy to find how comorbidity may contribute to decreasing the benefits of therapy, in terms of depressive symptoms recovery, to a point where CBT and ACT are almost as inefficient for comorbid caregivers as the control condition is for the non-comorbid ones (54.54% and 52.38% versus 44.44%).
Regarding recovery from clinical anxiety symptoms among those caregivers with baseline comorbid symptoms, the results of this study show that 36.36% and 35.71% of caregivers in the CBT and ACT groups, respectively, recovered from anxiety symptoms after intervention. Similarly, considering combined recovery from depressive and anxiety symptoms, results show that 36.36% in the CBT group and 30.95% in the ACT group recovered from depressive and anxious comorbidity after intervention. These results suggest that the presence of baseline depressive and anxiety comorbidity may constitute an impediment to treatment response.
The results also show that most caregivers who participated in this study, which was framed in the context of different clinical intervention trial studies for dementia caregivers [12, 14], presented clinically comorbid anxiety and depressive symptoms (81.54%). Hence, only 18.46% of caregivers who participated in this study presented exclusively depressive symptoms without the presence of clinically relevant anxiety symptoms. These results support the high prevalence of comorbidity between depression and anxiety in family caregivers of relatives with dementia [10]. It is noteworthy that most intervention studies on dementia caregiving are focused on the outcome of depressive symptoms, while little consideration is given to the potential presence of anxious symptomatology (alone or in combination with depressive symptoms) [32]. This is particularly striking given that anxious symptomatology has been found to be a very a prevalent emotional problem in dementia family caregivers [10, 11]. As pointed out by Cooper et al. [32], there is a need for intervention studies that specifically target anxiety or comorbidity in dementia caregivers. According to Cooper and colleagues [32], intervention strategies aimed at reducing caregivers’ depression levels may not show the same effect for anxiety levels, and different specific strategies may be required for this purpose.
The results of this study also suggest that caregivers with anxiety and depressive comorbid symptoms are younger and report a higher frequency of and distress linked to disruptive behavioral problems, as compared to caregivers with just depressive symptoms. This is consistent with a previous study showing that among stressors, distress associated with disruptive behaviors is an important risk factor for developing comorbid symptoms in dementia caregivers after controlling for sociodemographic variables [11]. It would be interesting to design psychological interventions explicitly aimed at modifying behavioral problems of the care-recipient for caregivers with simultaneous anxiety and depressive comorbid symptoms. In both types of interventions analyzed in this study, CBT and ACT, there is no specific module focused on training caregivers to change directly the frequency of and distress linked to behavioral problems of the care-recipient.
It has been suggested that comorbidity is a completely different aspect than merely a unique manifestation of symptoms [33–37], and it may be possible that comorbid and non-comorbid caregivers present differential needs that are not fully covered by each of these therapeutic approaches, which are manualized (CBT or ACT). It would be useful to design psychological interventions aimed at addressing the specific needs of caregivers, considering the comorbid manifestation of symptoms, through specific modules from each of these two frameworks. In this sense, our research team has recently analyzed an individualized modular intervention guided by functional analysis (FAMI) [12], which has shown to have significant beneficial effects on both depressive and anxious symptoms. Although these effects were not significantly different from the ACT and CBT conditions at post-treatment, FAMI showed greater effectiveness in the long term with comorbidity between depressive and anxious symptomatology. These results suggest that individualized modular interventions may be more effective for caregivers with comorbidity because functional analysis may allow the selection of the specific treatment modules (e.g., avoidance, passivity/lack of significant activity, maladaptive cognition) which address, in each individual case, the core dysfunctional mechanisms involved in the maintenance of comorbid anxious and depressive symptomatology.
The results of this study present clinical implications. These findings provide support for the importance of considering clinical anxiety symptoms as a potential outcome in dementia caregiver interventions [32], as most intervention studies are designed considering just depressive symptoms as inclusion criteria for participating in studies. Furthermore, it would be useful to expand the scope of outcome measures, analyzing the joint presence of different emotional distress outcomes, such as depressive and anxiety comorbid symptoms, for the design of psychological interventions in caregivers as the limited outcome measures constitute a limitation of studies [38]. Moreover, it would be useful to consider other outcome measures understudied in the caregiver intervention field, such as ambivalence, guilt, positive affect, negative affect, positive emotions, which have been shown to have different patterns of association with caregivers’ coping and emotional distress variables [38, 39]. Future studies should consider not only depressive symptoms but also different dimensions or potential factors implicated in the dementia caregiver process, such as stressors, coping and diverse outcome variables including anxiety symptoms and comorbid symptoms in order to identify the core targets of interventions. In addition, it would be useful to design longitudinal studies for analyzing different potential trajectories, including that of developing anxiety and comorbidity symptomatology, and the factors that contribute to explain them in order to design psychological interventions in this population. Researchers should consider not only a “picture” of caregivers’ situations at a given point (considering just the most studied outcome: depression) but also the whole “film” of their trajectories in order to identify variables involved in the development of caregivers’ comorbid symptoms, which may help to guide and make clinical decisions regarding the best intervention for each caregiver profile.
Consistent with the suggestions of Cheng et al. [38–40], we think future dementia caregiving studies should consider other potential variables as intervention targets, including comorbidity outcomes and its predictors, such as core resource mediators, dementia severity and caregivers’ transitions. Along these lines, as suggested above, it seems it would be more appropriate to analyze which are the specific mechanisms that may play an important role in explaining caregivers’ comorbid symptoms for every single case, instead of applying structured or manualized interventions for all caregivers. Modular interventions developed on the basis of a functional analysis which allows the identification of the core dysfunctional processes explaining the specific pattern of emotional symptomatology in each case [12] may be more useful in effectively treating comorbidity between anxious and depressive symptoms.
Some limitations of the study should be noted. Firstly, the caregiver sample included volunteer caregivers with clinical depressive symptomatology who wanted to participate in an intervention program. It is possible that the percentage of comorbidity between depressive and anxiety symptoms at baseline may be overestimated. In this sense, it is difficult to compare rates of comorbidity found in previous dementia intervention studies as most of these studies are designed for caregivers with high levels of distress, mostly considering depressive symptoms, but not anxiety symptoms. Another limitation of the study is related to the criteria we used to define clinical comorbid symptoms, i.e., the sub-syndromal cutoffs of CES-D and POMS scales for depression and anxiety, respectively, which do not allow the findings of this study to be compared to previous studies. The harmonization of diagnostic criteria with respect to comorbidity is desirable for comparing the results of future investigations regarding predictors and treatment response. Finally, the design of the study —in which the caregiver sample did not include caregivers with clinical anxiety symptomatology at baseline—does not allow differences between caregivers with comorbidity to be compared to non-comorbidity at baseline in treatment response in anxiety symptomatology as, while all caregivers presented depressive symptoms at baseline, only some caregivers presented anxiety symptoms. Finally, the small sample size of the study does not allow us to control important variables such us sociodemographic characteristics (e.g., caregiver age) and stressors in the analysis. It may be necessary to conduct and analyze psychological intervention studies on larger samples in order to calculate predictions of which caregiver profile had a poor or better treatment response, controlling for variables based on the stress and coping theoretical model.
In summary, the results of this study suggest that caregivers with comorbid depressive and anxiety symptomatology before intervention may benefit less from psychological interventions than caregivers with only depressive symptoms. Caregivers with simultaneous clinical manifestation of anxiety and depressive symptoms may represent a more vulnerable caregiver profile, as this mixed symptomatology constitutes an impediment to psychological treatment response. The design of psychological interventions specifically suited for dementia caregivers suffering from depression and anxiety comorbidity is needed.
Footnotes
ACKNOWLEDGMENTS
The authors thank all the caregivers for their participation in the study and also the following centers for collaborating with us in the project: Fundación Cien, Fundación Maria Wolff, Centro de Salud General Ricardos, Centro de Salud García Noblejas, Centro de Salud Benita de Ávila, Centro de Salud Vicente Muzas, Centro Reina Sofía de Cruz Roja, Centro de Psicología Aplicada de la Universidad Autónoma de Madrid.
The preparation of this paper was supported by grants from the Spanish Ministry of Economy and Competitiveness under grants PSI2012-31239, PSI2015-65152-C2-1-R, and partially by the Spanish Ministry of Science and Innovation under grant [PID2019-106714RB-C21] and by an FPU grant [FPU17/02548 from the Spanish Ministry of Education, Culture and Sport].
This study was approved by the Spanish Ministry of Economy and Competitiveness and the Ethics Committee of the Universidad Rey Juan Carlos.