
Abstract
Background:
Hispanic older adults are a high-risk population for Alzheimer’s disease and related dementias (ADRD) but are less likely than non-Hispanic White older adults to have ADRD documented as a cause of death on a death certificate.
Objective:
To investigate characteristics associated with ADRD as a cause of death among Mexican-American decedents diagnosed with ADRD.
Methods:
Data came from the Hispanic Established Populations for the Epidemiologic Study of the Elderly, Medicare claims, and National Death Index.
Results:
The final sample included 853 decedents diagnosed with ADRD of which 242 had ADRD documented as a cause of death. More health comorbidities (OR = 0.40, 95% CI = 0.28–0.58), older age at death (OR = 1.18, 95% CI = 1.03–1.36), and longer ADRD duration (OR = 1.08, 95% CI = 1.03–1.14) were associated with ADRD as a cause of death. In the last year of life, any ER admission without a hospitalization (OR = 0.45, 95% CI = 0.22–0.92), more physician visits (OR = 0.96, 95% CI = 0.93–0.98), and seeing a medical specialist (OR = 0.46, 95% CI = 0.29–0.75) were associated with lower odds for ADRD as a cause of death. In the last 30 days of life, any hospitalization with an ICU stay (OR = 0.55, 95% CI = 0.36–0.82) and ER admission with a hospitalization (OR = 0.67, 95% CI = 0.48–0.94) were associated with lower odds for ADRD as a cause of death. Receiving hospice care in the last 30 days of life was associated with 1.98 (95% CI = 1.37–2.87) higher odds for ADRD as a cause of death.
Conclusion:
Under-documentation of ADRD as a cause of death may reflect an underestimation of resource needs for Mexican-Americans with ADRD.
INTRODUCTION
Alzheimer’s disease is the sixth leading cause of the death in the U.S. [1]. This is likely an underestimate as national death statistics reflect the number of older adults who die from but not with Alzheimer’s disease [2]. The likely under reporting of Alzheimer’s disease and related dementias (ADRD) as a cause of death is due in part to ADRD not being widely recognized as a terminal illness [3]. Yet, older adults with advanced ADRD have clinical presentations and mortality rates that are consistent with a terminal illness [4, 5]. A study of 323 nursing home residents with advanced Alzheimer’s disease revealed that 37% of the 177 individuals who died over an 18-month period developed pneumonia and 90% had problems eating in the last 3 months of life [6]. Less than 5% of the decedents experienced a major event, such as a stroke, seizure, or myocardial infarction in the last 3 months of life [6].
The cause of death section of a death certificate is typically completed by the physician who oversaw the decedent’s medical care [7]. Emphasis is often given to health events that occurred immediately prior to death and ADRD may not be considered even if it contributed to the sequence of events that led to death [8]. This makes it meaningful for ADRD to be documented on a death certificate because it suggests the physician recognized that ADRD can be a cause of death.
Awareness of ADRD as a cause of death may have implications for a person’s medical care. A study of over eleven thousand Belgian decedents with ADRD indicated that those who did not have ADRD documented as a cause of death were more likely to be hospitalized, to have an intensive care unit stay, and to receive cardiopulmonary resuscitation and mechanical ventilation in the last 180, 90, and 30 days of life compared to decedents who had ADRD documented as a cause of death [9]. Most Hispanic older adults report that they want end-of-life care that prioritizes comfort [10, 11], but these preferences are often not shared with family members or their physician [10]. Thus, it may be especially important for a physician overseeing the medical care of a Hispanic older adult with ADRD to recognize that ADRD can be a cause of death.
Current understanding of ADRD as a cause of death is largely based on evidence from studies of non-Hispanic White decedents. The U.S. older adult population is becoming increasingly diverse. The percentage of adults aged 65 and older who are Hispanic is projected to increase from 6.9% in 2010 to 18.4% in 2050 [12]. The prevalence of ADRD is higher among Hispanic older adults compared to non-Hispanic White older adults [13]. Hispanic older adults also have more severe symptoms when ADRD is diagnosed and live longer after ADRD is diagnosed than non-Hispanic White older adults [14–16]. Greater symptom severity and longer survival are both associated with Alzheimer’s disease being documented as a cause of death [17–19]. However, Hispanic decedents are less likely than non-Hispanic White decedents to have Alzheimer’s disease recorded as a cause of death [20, 21].
Hispanic older adults with ADRD often receive potentially burdensome care at the end of life [22, 23]. This makes it important to identify characteristics associated with the end-of-life care of Hispanic decedents with ADRD. The documentation of ADRD as a cause of death may be especially impactful as it provides context to the events that led up to and were surrounding a person’s death. No studies to our knowledge have investigated if there are differences in the end-of-life care of Hispanic decedents diagnosed with ADRD according to if ADRD was documented as a cause of death. Existing evidence may not be generalizable to Hispanic populations because of biases in the diagnosis [24] and treatment [25] of ADRD and cultural differences in preferences for end-of-life care [26]. The main objectives of this study were to describe the healthcare utilization in the last year and last 30 days of life for Mexican-American decedents with ADRD and determine if there are differences according to if ADRD was documented as a cause of death.
METHODS
Data
This analysis used data from the Hispanic Established Populations for the Epidemiologic Study of the Elderly (H-EPESE) linked with the National Death Index and Medicare claims files [27, 28]. The H-EPESE began in 1993/94 with a cohort of 3,050 participants that was representative of Mexican-American adults aged 65 and older living in Texas, New Mexico, Arizona, Colorado, and California. Participants have been interviewed every two to four years and the most recent interview was completed in 2016. In 2004/05 (Wave 5) a new, representative cohort of 902 participants aged 75 and older was added to the sample. All participants recruited into the H-EPESE self-identified as Mexican-American. The survey files were used for information on decedents’ demographic characteristics.
We used data from the National Death Index for information on mortality status, age of death, and causes of death [29]. Additionally, a total of 2,580 H-EPESE participants have been linked with the following Medicare claims files for 1999 through 2016: Master Beneficiary Summary Files, Medicare Provider Analysis and Review files, Outpatient Standard Analytic files, and Carrier files. These files were used to identify decedents diagnosed with ADRD, number of health comorbidities diagnosed in the last year of life, and healthcare utilization during the last year and last 30 days of life.
Sample population
Figure 1 presents the selection of the analytic sample. We first identified participants in the Medicare-Linkage (n = 2,580) sample who became deceased before 2016. We used the Chronic Conditions Segments of the Master Beneficiary Summary File to identify decedents diagnosed with ADRD before death [30, 31]. In order to determine healthcare utilization during the last year and last 30 days of life, we included participants who had continuous enrollment in fee-for-service Medicare for one year before death. The final sample included 855 decedents.

Cohort Selection.
Measures
ADRD as a cause of death
The National Death Index includes ICD-10 codes for the underlying cause of death and up to twenty multiple causes of death [29]. The underlying cause of death is the disease or condition that started the sequence of conditions that led to the death [29]. We used the ICD-10-CM codes in the algorithm for ADRD or senile dementia to identify decedents with ADRD as an underlying or multiple cause of death.
Health status and healthcare utilization in the last year of life
We used the Medicare Provider Analysis and Review files, Outpatient Standard Analytic files, and Carrier files to determine the health comorbidities diagnosed in the last year of life according to the Charlson Comorbidity Index [32]. Decedents were categorized as having a comorbidity score of 0–2 points, 3-4 points, and ≥5 points. A higher score indicates a higher number of comorbidities.
We used the Medicare Provider Analysis and Review files, Outpatient Standard Analytic files, and Carrier claims files to create variables for any (i.e., one or more) acute hospitalizations, emergency room (ER) admissions, and physician visits in the last year of life. Any hospitalizations were categorized as none, hospitalization with no intensive care unit (ICU) stay, and hospitalization with a stay in the ICU. Also, the hospital diagnosis related group for the primary discharge diagnosis was grouped into one of twenty-five Major Diagnostic Categories [28]. Any ER admissions were categorized as none, ER admission with no hospitalization, and ER admission that included a hospitalization.
The variable for any physician visits was dichotomized as yes or no. A second variable was created in which physician visits were categorized as primary care, specialists, and other types of providers. Primary care providers included general practice, family practice, internal medicine, geriatric medicine, and nurse practitioners. Specialists included neurology, psychiatry, geriatric psychiatry, neuropsychiatry, cardiology, ophthalmology, orthopedic surgery, nephrology, hematology/oncology, and rheumatology. We selected these specialists based on the medical conditions that are highly prevalent in the H-EPESE. We defined a provider’s specialty according to the Centers for Medicare and Medicaid provider specialty code that was used on the majority of claims for that year. The last category included all other types of providers.
Healthcare utilization in the last 30 days of life
Measures for healthcare utilization in the last 30 days of life included having any acute hospitalizations, any ER admissions, being admitted to the ICU, having used a ventilator (yes/no), and having received hospice care. For decedents with any hospitalizations in the last 30 days of life, the hospital diagnostic related group was categorized into one of twenty-five Major Diagnostic Categories [28]. The Medicare claims files necessary to determine having received hospice care was only available for decedents who died between 2005 and 2016 (n = 551).
Statistical analysis
Independent sample t-tests and chi-square tests were used to describe the 853 decedents according to having ADRD documented as a cause of death. Logistic regression was used to model the association between decedent characteristics and the odds for having ADRD as a cause of death. Each healthcare utilization measure was analyzed separately. All models controlled for sex, being born in the U.S., Charlson Comorbidity Index Score in the last year of life, age of death, ADRD duration, and year of death (1999–2004, 2005–2010, 2011–2016).
Chi-square tests were used to compare the percentage of hospital discharges by Major Diagnostic Category in the last year and last 30 days of life according to ADRD as a cause of death. Statistical significance was set to p < 0.01 to account for multiple comparisons.
RESULTS
Demographic and health characteristics according to ADRD as a cause of death
Table 1 presents the descriptive characteristics of the 853 decedents diagnosed with ADRD according to having ADRD documented as a cause of death. The majority of decedents were female (61.9%) and born in the United States (57.6%). The average age of ADRD diagnosis was 84.2 years, the average age of death was 87.7 years, and the average ADRD duration was 3.0 years. Nearly half (48.2%) of all decedents had a comorbidity score of 5 or more points in the last year of life.
Demographic and health characteristics of Mexican-American decedents with ADRD according to having ADRD documented as a cause of death
*p < 0.05. Adjusted odds ratios controlled for cohort, gender, place of birth, age of death, ADRD duration, year of death, and comorbidity score in the last year of life. ADRD, Alzheimer’s disease and related dementias; OR, odds ratio; CI, confidence interval; SD, standard deviation.
Two hundred and forty-two (28.4%) decedents had ADRD documented as a cause of death. These decedents were more likely to be female, were older at time of diagnosis and death, had longer disease duration, were more likely to die between 2011–2016, and had a lower comorbidity score in the last year of life than decedents who did not have ADRD as a cause of death.
In the adjusted models, older age at death (adjusted odds ratio [aOR] = 1.18, 95% CI = 1.03–1.36) and longer ADRD duration (aOR = 1.08, 95% CI = 1.03–1.14) were both associated with significantly higher odds for ADRD as a cause of death. Conversely, a comorbidity score of 5 or more points in the last year of life was associated with significantly lower odds for ADRD as a cause of death (aOR = 0.40 95% CI = 0.28–0.58).
Hospitalizations and ER admissions according to ADRD as a cause of death
The healthcare utilization in the last year and last 30 days of life is shown in Table 2. Nearly half of decedents in the last year of life had a hospitalization that included an ICU stay (49.9%) and 81.8% had an ER admission with a hospital stay. Approximately 84% of decedents saw a physician in the last year of life and the average number of physician visits was 8.4. In the last 30 days of life, 31.8% of decedents had a hospitalization that included an ICU stay, 49.5% had an ER admission that led to a hospitalization, and 13.7% were on a ventilator during a hospital stay. Among the 650 decedents who died between 2005 and 2016, 44.5% received hospice care in the last 30 days of life.
Healthcare utilization in the last year of life and last 30 days of life for Mexican-American decedents with ADRD according to having ADRD documented as a cause of death
*p < 0.05. §Physician with specialty as general practice, family practice, internal medicine, and geriatric medicine, and Nurse practitioner. £Physician with specialty as neurology, psychiatry, geriatric psychiatry, neuropsychiatry, cardiology, ophthalmology, orthopedic surgery, nephrology, hematology/oncology, and rheumatology. ¥Hospice use included decedents who died between 2005 and 2016. †Controlled for cohort, gender, place of birth, age of death, ADRD duration, year of death, comorbidity score, and number of physician visits. ‡Controlled for cohort, gender, place of birth, age of death, ADRD duration, year of death, comorbidity score, and hospitalization with ICU. ±Controlled for cohort, gender, place of birth, age of death, ADRD duration, year of death, and comorbidity score. ADRD, Alzheimer’s disease and related dementias; OR, odds ratio; CI, confidence interval; SD, standard deviation; ER, emergency room.
In general, healthcare utilization was less for decedents with ADRD documented as a cause of death. An ER admission that did not include a hospitalization in the last year of life was associated with significantly lower odds for ADRD as a cause of death (aOR = 0.45, 95% CI = 0.22–0.92). A greater number of physician visits (aOR = 0.96, 95% CI = 0.93–0.98) and seeing a specialist compared to not seeing a physician (aOR = 0.46, 95% CI = 0.29–0.75) were also associated with significantly lower odds for ADRD as a cause of death. Decedents who had a hospitalization with an ICU stay in the last 30 days of life had 0.55 (95% CI = 0.36–0.82) lower odds for ADRD as a cause of death. Similarly, an ER admission with and without a subsequent hospitalization were associated with 0.67 (95% CI = 0.48–0.94) and 0.56 (95% CI = 0.31–1.02) lower odds for ADRD as a cause of death, respectively.
Over half (58.8%) of decedents with ADRD as a cause of death received hospice care in the last 30 days of life compared to 38.4% of decedents who did not have ADRD as a cause of death (aOR = 1.98, 95% CI = 1.37–2.87). Analysis of data from the 650 participants who died between 2005 and 2016 revealed that the associations between hospitalizations and ER admissions in the last 30 days of life and ADRD as a cause of death were partially reduced after controlling for hospice care (Supplementary Table 1).
Differences in hospital discharges by major diagnostic category according to ADRD as a cause of death
Figure 2 shows the percentage of hospital discharges in the last year and in the last 30 days of life by Major Diagnostic Category for decedents with and without ADRD as a cause of death. There were 1,570 hospital discharges in the last year of life and 519 discharges in the last 30 days of life for decedents without ADRD as a cause of death. The number of hospital discharges for decedents with ADRD as a cause of death was 453 in the last year of life and 148 in the last 30 days of life. The percentage of discharges for conditions of the circulatory system in the last year of life (ADRD = 11.7% versus no ADRD = 21.8%) and last 30 days of life (ADRD = 6.8% versus no ADRD = 19.5%) were significantly lower for decedents with ADRD as a cause of death (p < 0.001). Conversely, the percentage of discharges for conditions of the endocrine, nutritional, and metabolic system were significantly higher in the last year (ADRD = 9.1% versus no ADRD = 5.5%) and last 30 days of life for decedents with ADRD as a cause of death (ADRD = 12.2% versus no ADRD = 4.2%, p < 0.01).
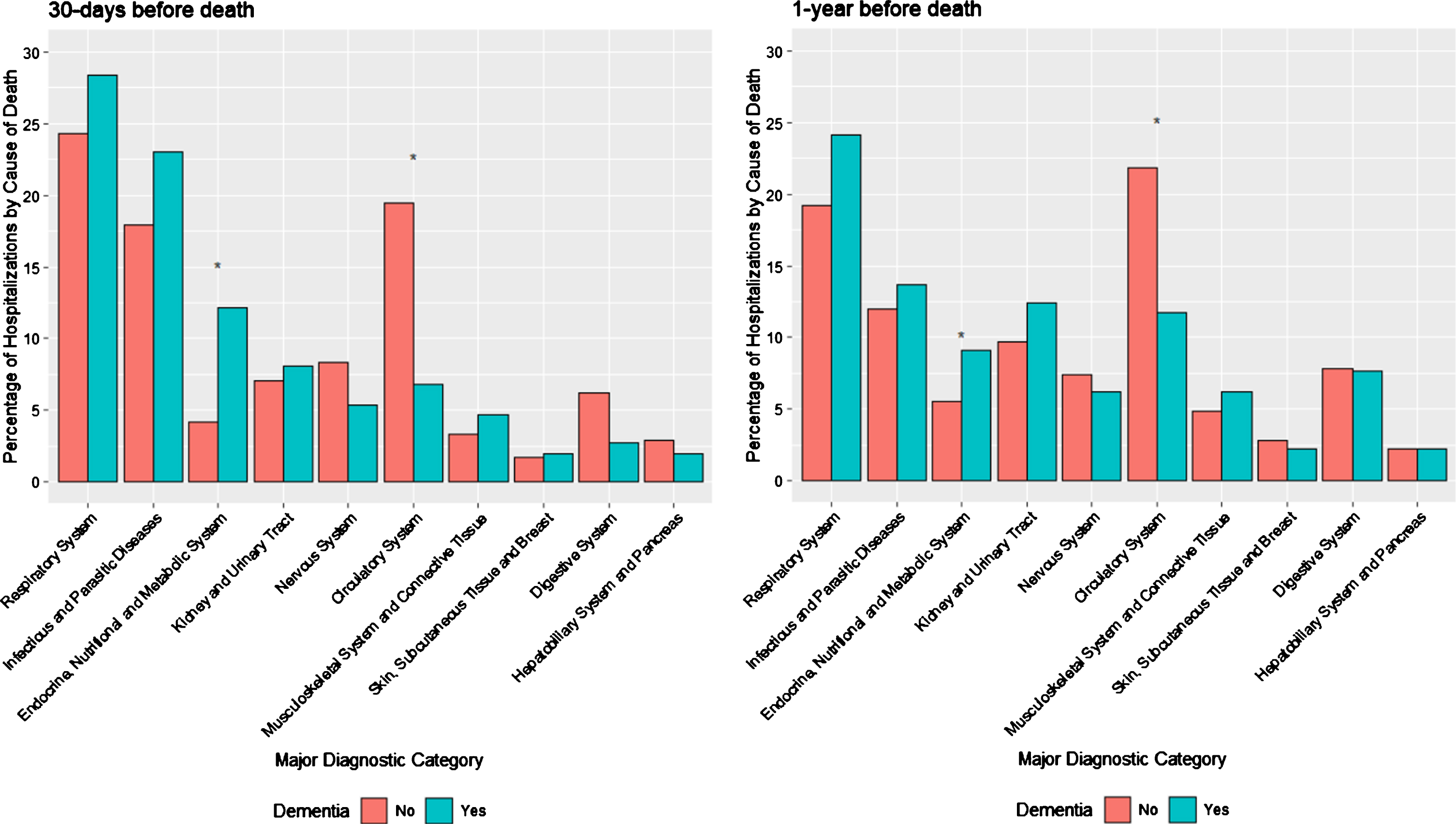
Percentage of hospital discharges by major diagnostic category in the last year and 30 days of life according to Alzheimer’s disease and related dementias as a cause of death. *p < 0.001. There were 519 discharges during 30 days before death and 1,570 discharges during 1 year before death for subjects without ADRD as cause of death; the numbers of discharge for subjects with ADRD were 148 and 453 during 30 days and 1 year before death.
DISCUSSON
We sought to describe the healthcare utilization during the last year and last 30 days of life for Mexican-American decedents diagnosed with ADRD and determine if there are differences in healthcare utilization according to if ADRD is documented as a cause of death. Decedents who had any ER admissions, hospitalizations, and ICU stays in the last year and last 30 days of life had significantly lower odds for ADRD to be documented as a cause of death. Having seen a specialist in the last year of life was also associated with significantly lower odds for ADRD to be documented as a cause of death. This is evidence that Mexican-American decedents with ADRD and who had ADRD documented as a cause of death received less intensive end of life care than those diagnosed with ADRD but did not have ADRD documented as a cause of death. Our findings support the importance of considering ADRD as a terminal illness that can be a cause of death.
We observed that a greater percentage of hospital discharges in the last 30 days of life for decedents with ADRD as a cause of death were for conditions of the endocrine, nutritional, and metabolic system. This includes chronic conditions such as diabetes and nutritional disorders such as vitamin deficiencies. In these instances, greater attention may be given to ADRD as a cause of death because it can make managing a chronic condition more difficult or worsen the severity of a condition [33]. Conversely, a greater percentage of hospital discharges in the last 30 days of life for decedents in which ADRD was not documented as a cause of death were for conditions of the circulatory system, which includes acute (e.g., heart attack, cardiac arrest) and chronic (e.g., hypertension) conditions. Less consideration may be given to ADRD as a cause of death when a person is hospitalized for an acute event and thus be less likely to be included on a death certificate.
Approximately one-quarter of the 853 decedents had ADRD documented as a cause of death. This percentage is lower than what has been reported in studies of predominately non-Hispanic White decedents diagnosed with ADRD [18, 34–36]. Several factors likely contribute to the apparent under-reporting of ADRD as a cause of death for Mexican-American decedents diagnosed with ADRD prior to death. First, the prevalence of comorbid health conditions that are common causes of death for older adults with ADRD such as diabetes are higher among Hispanic older adults with ADRD than non-Hispanic White older adults [37]. ADRD may be less likely to be considered as a cause of death if the decedent had a high number of comorbid conditions that are common causes of death [8]. This is supported by our finding that decedents with a greater number of comorbidities in the last year of life had significantly lower odds to have ADRD documented as a cause of death. This is also consistent with the findings from an autopsy study of 423 decedents diagnosed with ADRD in which Hispanic decedents had a high burden of cerebrovascular disease pathology and mixed-dementia pathology whereas non-Hispanic White decedents had a high burden of Alzheimer’s disease pathology only (i.e., non-mixed Alzheimer’s disease) [38].
Longer ADRD duration was associated with significantly higher odds for ADRD being documented as a cause of death. This is an important finding because ADRD diagnosis can be influenced by systemic, structural, and cultural factors. Biases in cognitive testing [39], limited access to physicians who specialize in ADRD [40], and physicians not addressing concerns about changes in memory [41] are among several factors that can contribute to a delayed or missed diagnosis of ADRD for Hispanic older adults. A timely diagnosis of ADRD is important for the person and their family to discuss with a physician about future plans for medical care [42]. However, Hispanic patients and family members rarely report that they have discussed with a clinician about disease prognosis or end of life care [10].
Hospice is an increasingly common site of death for decedents with ADRD [43]. We observed that decedents who received hospice care during the last 30 days of life had nearly two times higher odds to have ADRD documented as a cause of death. To be eligible for hospice, Medicare requires the patient to have a prognosis of 6 months or less as determined by their attending physician and the hospice medical director [44]. The attending physician is typically the patient’s primary care physician or a specialist related to the terminal diagnosis [44]. Presumably, the attending physician is knowledgeable of the patient’s medical history and the influence that ADRD has had on the patient’s prognosis. This may contribute to ADRD being recognized as a cause of death by the attending physician and more often being documented on the death certificate. Hospice is associated with preventing burdensome and unnecessary medical care at the end of life [45]. However, language barriers [46] and lack of awareness about hospice services [47] contribute to Hispanic older adults being less likely to receive hospice care than non-Hispanic White older adults [48].
Limitations
We used data from the National Death Index to determine ADRD as a cause of death. The cause of death documented on a death certificate can be incorrect when compared to autopsy reports [49]. Second, we used ICD codes in Medicare claims files to identify decedents diagnosed with ADRD. Medicare claims have been shown to have low sensitivity for identifying older Hispanic adults with ADRD [50]. We also did not have data to determine ADRD severity at the time of death. Autopsy studies have associated greater ADRD severity with different causes of death [51], including greater likelihood for ADRD as a cause of death [35]. Finally, we could only include decedents who were enrolled in fee-for-service Medicare. Approximately half of all Hispanic Medicare beneficiaries are enrolled in a Medicare Advantage plan [52].
This study also has important strengths. First, Hispanic older adults are an under-studied population. Prior studies have been limited by a small number of Hispanic decedents with ADRD. Second, we used data from a population-based cohort of older Mexican-American adults living in the Southwestern US. Nearly 65% of Hispanic adults in the United States are Mexican American [53]. Third, our data source included survey data of decedents that have been linked with Medicare claims files. This allowed us to include information not available in claims files along with detailed information about healthcare utilization.
CONCLUSION
Greater healthcare utilization in the last year and last 30 days of life were associated with lower odds for ADRD being documented as a cause of death among Mexican-American decedents diagnosed with ADRD. Having received hospice care in the last 30 days of life was associated with higher odds for ADRD as a cause of death. This is new evidence that important differences exist in the healthcare utilization at the end of life for Mexican American decedents with ADRD according to ADRD being documented as a cause of death. The under documentation of ADRD as a cause of death may result in underestimation of healthcare resource need for dementia care in the Mexican-American population. Future research should investigate the role of sociocultural factors that influence the timeliness of an ADRD diagnosis and end of life care may have on the apparent under reporting of ADRD as a cause of death among Mexican American decedents with ADRD.