
Abstract
Background:
Repetitive head impacts (RHI) from contact sports have been associated with cognitive and neuropsychiatric disorders. However, not all individuals exposed to RHI develop such disorders. This may be explained by the reserve hypothesis. It remains unclear if the reserve hypothesis accounts for the heterogenous symptom presentation in RHI-exposed individuals. Moreover, optimal measurement of reserve in this population is unclear and likely unique from non-athlete populations.
Objective:
We examined the association between metrics of reserve and cognitive and neuropsychiatric functioning in 89 symptomatic former National Football League players.
Methods:
Individual-level proxies (e.g., education) defined reserve. We additionally quantified reserve as remaining residual variance in 1) episodic memory and 2) executive functioning performance, after accounting for demographics and brain pathology. Associations between reserve metrics and cognitive and neuropsychiatric functioning were examined.
Results:
Higher reading ability was associated with better attention/information processing (β=0.25; 95% CI, 0.05–0.46), episodic memory (β=0.27; 95% CI, 0.06–0.48), semantic and phonemic fluency (β=0.24; 95% CI, 0.02–0.46; β=0.38; 95% CI, 0.17–0.59), and behavioral regulation (β=–0.26; 95% CI, –0.48, –0.03) performance. There were no effects for other individual-level proxies. Residual episodic memory variance was associated with better attention/information processing (β=0.45; 95% CI, 0.25, 0.65), executive functioning (β=0.36; 95% CI, 0.15, 0.57), and semantic fluency (β=0.38; 95% CI, 0.17, 0.59) performance. Residual executive functioning variance was associated with better attention/information processing (β=0.44; 95% CI, 0.24, 0.64) and episodic memory (β=0.37; 95% CI, 0.16, 0.58) performance.
Conclusion:
Traditional reserve proxies (e.g., years of education, occupational attainment) have limitations and may be unsuitable for use in elite athlete samples. Alternative approaches of reserve quantification may prove more suitable for this population.
Keywords
INTRODUCTION
Exposure to repetitive head impacts (RHI), particularly from contact sports, has been associated with later-life cognitive and neuropsychiatric disturbances, as well as the development of neurodegenerative diseases (e.g., chronic traumatic encephalopathy [CTE]) and other pathologies (e.g., white matter degeneration) [1–15]. However, not all individuals exposed to RHI develop cognitive or neuropsychiatric disorders [2, 16–19]. Among those who do, there is heterogeneity in the presence and severity of the presentation and underlying neuropathology [2, 20]. Identification of risk and resilience factors of the late effects of RHI is critical to facilitate disease detection, diagnosis, and treatment and prevention strategies.
The heterogeneous expression of cognitive and neuropsychiatric deficits following RHI exposure may be explained by the reserve hypothesis. Reserve is a heuristic to describe individual variations in cognition and/or function and can be conceptualized as two main components: brain reserve (BR) and cognitive reserve (CR) [21–23]. BR refers to an individual’s neurobiological capital, i.e., resistance to pathology [24–26]. It is often measured by dimensions like gray matter (GM) volume, white matter (WM) volume, or estimated intracranial volume (eTIV) [24–27]. Recent literature has identified eTIV as an appropriate operationalization of BR as it encompasses GM, WM, and cerebrospinal fluid (CSF) measures [27, 28]. CR represents the varying susceptibility of an individual’s cognitive abilities to neuropathology, i.e., resilience to the clinical manifestation of pathology. CR is typically estimated by measures referred to as proxies (i.e., representative measures of reserve). Common CR proxies include estimated premorbid intelligence/reading ability [29, 30], years or level of education [22, 31], and occupational attainment [32, 33]. Higher scores on proxy measures are typically associated with better cognitive performance [34]. The definitions and quantifying methods of reserve are continuously evolving and while recent attempts to clarify these concepts have been made [22, 24], there is currently no consensus. Moreover, evidence suggests that BR and CR independently and interactively contribute to the heterogeneity in one’s resistance and resilience to brain insult [35–37]. As a result, the current investigation refers to CR and BR collectively as reserve, i.e., an entity that accounts for the discrepancy between the degree of brain pathology and the clinical manifestation of pathology [35–37].
Reserve has been extensively studied in Alzheimer’s disease (AD) and AD-related dementias. Higher educational and occupational attainment have been shown to mitigate the clinical and neuropathological expression of AD [38–40], even in APOE ɛ4 carriers [33]. Moreover, higher estimated premorbid intelligence/reading ability has also been associated with improved cognitive recovery following traumatic brain injury (TBI) [29, 30]. Extant studies have also alluded to the possible role of reserve in the heterogeneous presentation of RHI-related deficits [4, 41]; however, formal investigations in this area are limited. Alosco et al. [42] examined the association between occupational attainment and years of education and age of symptom onset among 25 deceased American football players with severe CTE. Here, higher occupational attainment was found to be associated with a later age of symptom onset, but no effect was found for years of education. In addition to highlighting the need for further RHI-focused reserve research, this investigation raised the question of the suitability of traditional proxies for reserve quantification, particularly in elite former contact sport athletes.
Despite the convenience of single proxies for reserve estimation, reserve is a dynamic concept not sufficiently summarized by one component [22, 43]. Representing reserve in this way fails to distinguish between reserve itself and its contributing factors, likely resulting in significant measurement error [43, 44]. Individual proxy use for reserve quantification may also be problematic when considering RHI exposure. Firstly, years of education may not reflect quality of education in former elite athletes [42]. Most former elite athletes obtain 16 years of education with restricted variability due to the close relationship between sporting expertise and the American educational system. As a result, for athletic samples, education may not appropriately reflect complete reserve capacity. It is further considered that occupational attainment may be a poor measure of reserve in samples with RHI exposure. While Alosco et al. [42] found an effect for occupational attainment in their sample, they argue that low occupational attainment may be a consequence of RHI-related pathology (i.e., the pathology leads to functional impairment) rather than reflecting an individual’s complete reserve capacity. Therefore, a more refined measure of reserve is required to further our knowledge of its potential role in RHI-exposed samples and to gain an understanding of how it may contribute to clinical heterogeneity.
One alternative method of reserve quantification is the residual memory variance calculation [45]. Here, variance refers to the variability of a value(s) from the average. To calculate reserve using this method, the residual variance of cognitive performance (e.g., on an episodic memory task) is derived, after accounting for demographic factors (e.g., age, sex) and structural brain characteristics (e.g., total brain volume). This residual component encompasses all individual differences in cognition that cannot be explained by brain structure and demographic variables, thus representing a measure of reserve. This residual method of reserve quantification defines reserve as the discrepancy between one’s predicted and one’s observed level of cognitive performance [45, 46]. Higher positive residuals represent better than expected performance. The residual measure was shown to be correlated with traditional proxy measures of CR, highlighting the plausibility of this method. These findings have since been replicated and extended to different cognitive domains (e.g., executive functioning, language) across multiple samples [46–50]. Moreover, a recent review and meta-analysis of residual methods of reserve quantification strongly supports this technique as a measure of resilience and resistance in aging samples [51]. An important limitation of this approach, however, is that while a proportion of the residual likely represents reserve, there is also likely to be a significant but unknown proportion that is random error [49]. Nonetheless, applying such methodology to an RHI-exposed cohort would be a novel approach towards exploring the evident heterogeneity in symptom expression, or lack of thereof, following RHI exposure.
The objective of this study was to examine the association between reserve and cognitive and neuropsychiatric function in symptomatic former National Football League (NFL) players. The primary objective was to identify optimal measurement of reserve in this population. To do so, we used traditional individual proxy measures of reserve, in addition to the residual variance method of reserve quantification. Episodic memory and executive dysfunction are prominent symptoms following RHI exposure [2, 52–54]. Therefore, we targeted both the episodic memory and executive functioning domains to create residual episodic memory and executive functioning variance variables. The quantification of reserve by means of single proxies is problematic and the residual variance method may prove a suitable alternative to overcome these aforementioned issues in athletic samples.
MATERIALS AND METHODS
Participants and study design
The current sample included former NFL players from the National Institute of Neurological Disorders and Stroke–funded study entitled ‘Diagnosing and Evaluating Traumatic Encephalopathy Using Clinical Tests’ (DETECT; R01NS078337). Recruitment and data collection occurred between November 2011 and October 2015. Inclusion criteria included: male, aged 40–69 years, self-reported complaints of cognitive, behavior and/or mood symptoms at telephone screening, and a minimum of 12 years of organized American football, with at least two seasons in the NFL. Former NFL players were recruited to ensure the selected sample represented a population with high risk for CTE. Exclusion criteria included MRI and/or lumbar puncture contraindications, concussion history within 1 year of study entry, visual or hearing impairment that would compromise neuropsychological testing, lack of adequate decisional capacity to provide consent to participate, and/or a primary language other than English.
Upon enrollment to the DETECT study, participants completed a 2-to-3-day visit to undergo neuropsychological testing, neuroimaging, and demographic, medical, neurological, psychiatric, and physical evaluations. Only data relevant to the current investigation was examined. All participants provided written informed consent prior to participation. All study protocols were approved by the Boston University Medical Center and Brigham and Women’s Hospital Institutional Review Boards.
Measures
Traditional reserve proxies
A number of reserve proxies were derived. Participants’ level of education was defined by the number of formal years attained [22, 31]. An individual’s level of occupational attainment following their NFL career was obtained by categorizing participants’ occupation as high or low according to the U.S. Department of Labors’ Dictionary of Occupational Titles (DOT) [32, 55]. High attainment was classified as any professional, technical, or managerial profession (DOT codes 0–1). Low attainment was defined as work such as clerical or sales positions, processing occupations, and structural occupations (DOT codes 2–8). Miscellaneous occupations were classified with a DOT code of 9. For participants with multiple occupations, the highest level of attainment was used. One participant fell into the category of miscellaneous occupations (DOT code 9); however, due to similarities to occupations covered under DOT codes 2–8, this participant was classified as having low occupational attainment. The Wide Range Achievement Test-4 (WRAT-4) [56] reading subtest was used as a representative of an individual’s reading ability [29, 30]. As with most other reading ability estimates, the WRAT-4 measures the accumulation of learning at the age prior to insult, in addition to the altered trajectory of learning and development following the insult. Lastly, eTIV served as an additional proxy of reserve [27].
Neuropsychological and neuropsychiatric measurements
A comprehensive neuropsychological battery was administered to all participants to assess cognitive functioning. To limit the number of analyses, a subset of tests were selected a priori based on their ability to assess cognitive domains impaired following RHI exposure [8, 53] and included: the Trail Making Test (TMT) Parts A and B [57], Neuropsychological Assessment Battery (NAB) List Learning Long Delay Recall [58], Controlled Oral Word Association Test (COWAT) [59], and Animal Fluency Test [59]. In order to describe the clinical sample, neuropsychological test raw scores were converted into standardized scores accounting for age, sex, and/or educational attainment. However, as educational attainment is a well-recognized traditional proxy for reserve [22, 31], all statistical analyses used neuropsychological test raw scores. TMT Parts A and B were reverse coded to correct directionality (i.e., lower scores represent worse performance).
Symptoms of depression and neurobehavioral dysregulation were assessed using the Beck Depression Inventory-II (BDI-II) [60] and the Behavior Rating Inventory of Executive Functioning –Adult Version (BRIEF-A) Behavioral Regulation Index (BRI) [61], respectively. Raw BRIEF-A BRI scores were converted into standardized age-adjusted T-scores.
Cumulative Head Impact Index (CHII)
The CHII is a retrospective estimate of total cumulative exposure to RHI from participation in American football [4]. This value is derived using two sources of information; 1) self-reported athletic exposure (i.e., level of play, number of seasons played, position[s] played), and 2) objective estimates of head impact frequency based on position played, as determined by published helmet accelerometer studies. The development of the CHII has been previously described and validated [4]. The CHII was developed in former youth, high school, and college American football players (for which helmet accelerometer studies are available) to estimate the frequency of head impacts. However, published helmet accelerometer data are non-existent for professional level American football. Therefore, college-level estimates of head impact frequencies were applied to the DETECT sample to estimate their professional-level exposure. Higher CHII values indicate greater exposure to RHI.
MRI acquisition and processing
All participants underwent structural MRI on a 3-Tesla Siemens Verio MRI scanner with a 32-channel head coil and the Syngo MR-B17 software suite. Three-dimensional T1-weighted scans (MPRAGE [1 X 1 X 1 mm3; TR = 1800 ms; TE = 3.36 ms; acquisition matrix = 256 x 256; flip angle = 7°]) were acquired. We examined total brain volume, and hippocampal and white matter hypointensity (WM-hypo) volumes. Hippocampal and WM-hypo volumes served as specific regions of interest (ROIs) because of their known effects on cognitive and neuropsychiatric function, as well as their association with RHI exposure [62–65]. WM-hypo also captures cerebrovascular contributions to cognitive impairment and dementia. All imaging variables were only used to derive metrics of reserve. FreeSurfer 5.3 was used for automated segmentation of brain tissue and has been described in detail elsewhere [66, 67]. This program subdivides brain tissue into areas of GM, WM, and CSF. Total eTIV is also calculated. Visual quality assessment was conducted to ensure correct detection and automated segmentation occurred. Manual adjustments of the hippocampus were performed using Slicer 4.1 [68], as previously described [62, 69]. A trained neuroanatomist was involved in defining the criteria for these manual adjustments and intra- and inter-reader reliability was tested. Coronal slices were used to correct ROIs, from anterior to posterior, referring to sagittal slices for verification and volumes were subsequently extracted from the label maps of the left and right hippocampi. All images were processed by the Psychiatry Neuroimaging Laboratory at Brigham and Women’s Hospital.
Statistical analyses
Statistical analyses were performed in R version 3.6.0 [70]. To normalize their distribution, WM-hypo volumes were log-transformed. Before analysis, all MRI variables were coded to ensure that higher scores indicated greater pathology (i.e., left hippocampal, right hippocampal, total GM, total WM, and eTIV were reverse coded). Listwise deletion was applied, omitting any observations with missing data on variables of interest. Statistical significance was defined by p < 0.05, with false discovery rate (FDR)-adjusted corrections for multiple comparisons. The above-described neuropsychological and neuropsychiatric test scores acted as primary outcome measures.
Traditional reserve proxies
Five separate linear regression analyses were conducted to assess the association between traditional reserve proxies (i.e., level of education, occupational attainment, reading ability, and eTIV) and participants’ neuropsychological test performance and reported neuropsychiatric symptoms. To examine each proxy’s representation of reserve and to avoid multicollinearity, separate regression analyses were performed. The following covariates were included due to their suggested contribution to reserve and their previous association with cognitive and behavioral/mood symptom expression: age [71–73], racial identity [74–76], CHII [4, 20], and APOE genotype [33, 78–80]. CHII was chosen as a representative measure of RHI exposure as it encompasses several estimates of RHI into a single metric. Racial identity was coded as 0 and 1 for White and Black or African American race, respectively. APOE genotype was coded as 0 and 1 for non-carriers (absence of an ɛ4 allele) and carriers (presence of at least one ɛ4 allele), respectively.
Residual episodic memory and executive functioning variance
Residual episodic memory variance was computed by regressing the residuals of NAB List Learning Long Delay Recall raw scores on age, racial identity, APOE ɛ4 status, CHII, logWM-hypo, total brain matter volume, and total hippocampal volume. Episodic memory was chosen as it is one of the most prominent symptoms associated with RHI exposure [2, 9]. All variance of the NAB List Learning Long Delay Recall variable that could be explained by demographics or brain pathology was removed. That is, the residuals represented the discrepancy between a participant’s observed NAB List Learning Long Delay Recall performance and the performance predicted by the aforementioned predictors. Executive dysfunction has also been identified as a prominent RHI-related symptom [8, 53]. Residual executive functioning variance was computed using this same method, substituting NAB List Learning Long Delay Recall raw scores for TMT Part B raw scores. The resulting unstandardized residual terms were then used individually as representative metrics of reserve for this sample. All variables were coded to ensure higher residual scores indicated higher reserve, i.e., better performance than predicted. All subject-specific residuals were calculated using the leave-one-out cross validation technique, i.e., with the subject deleted when estimating the predicted value of that subject. Next, the linear regressions were repeated separately for each of the residual variables, the newly created reserve term acting as the predictor and the neuropsychological and neuropsychiatric test raw scores (not including NAB List Learning Long Delay Recall or TMT Part B, where applicable) as the outcomes. To determine how well these predictive models performed, leave-one-out cross validation was completed. Bivariate Pearson correlations were conducted to investigate the relationship between the individual newly created residual variables and the four traditional reserve proxies.
RESULTS
Sample derivation
The final sample size for all analyses was 89. This was derived following exclusion of one participant due to poor effort, as reflected by failure on numerous symptom validity tests, multiple neuropsychological scores at floor (i.e., lower limit), and the presence of external evidence supporting this conclusion. Two more participants were removed due to missing occupational attainment data. Neuroimaging data was available for 81 participants, following the exclusion of those who did not complete MRI and those with inadequate data quality due to motion artifact. Table 1 summarizes the sample characteristics. Tables 2 3 display the neuropsychological, neuropsychiatric, and MRI characteristics for the current sample.
Demographic, athletic, medical, and APOE carrier status characteristics in former NFL players
SD, standard deviation; y, years; AFE, age of first exposure; CHII, cumulative head impact index; APOE, Apolipoprotein E.
Neuropsychiatric and neuropsychological raw scores and standardized scores in the former NFL player sample (N = 89)
TMT, Trail Making Test; NAB, Neuropsychological Assessment Battery; COWAT, Controlled Oral Word Association Test; BRIEF-A BRI, Behavior Rating Inventory of Executive Functioning –Adult Version Behavioral Regulation Index; BDI-II, Beck Depression Inventory-II. 1To limit the number of analyses, a subset of tests were selected a priori based on their ability to assess cognitive domains impaired following RHI exposure [8, 53]; 2All statistical analyses used neuropsychological test raw scores; 3In order to describe the clinical sample, neuropsychological test raw scores were converted into standardized scores accounting for age, sex, and/or educational attainment. Raw BRIEF-A BRI scores were converted into standardized age-adjusted T-scores; 4Before analysis, Trails A and B were reverse coded to correct directionality (i.e., lower scores represented worse performance).
Summary statistics of MRI indices measured in former NFL players (N = 81)1
1Neuroimaging data was available for 81 participants, following the exclusion of those who did not complete MRI and those with inadequate data quality due to motion artifact; 2Before analysis, all variables were coded to ensure that higher scores indicated greater pathology (i.e., left hippocampal volume, right hippocampal volume, total gray matter volume, total white matter volume, and estimated intracranial volume were reverse coded); 3To normalize their distribution, white matter hypointensity volumes were log-transformed.
Traditional reserve proxies
Linear regression analyses
Regression analyses revealed a statistically significant association between age and racial identity, and several of the neuropsychological and neuropsychiatric outcomes (Supplementary Table 1). Older age correlated with worse performance on TMT Part B (p < 0.01) and NAB List Learning Long Delay Recall (p = 0.01). Black or African American race was associated with worse performance on TMT Parts A (p = 0.01) and B (p = 0.01), NAB List Learning Long Delay Recall (p = 0.03), Animal Fluency (p = 0.03), and the COWAT (p = 0.05). No significant effects were found for the CHII or APOE ɛ4 status on any of the neuropsychological or neuropsychiatric test scores (Supplementary Table 1).
The WRAT-4 had a significant effect on TMT Part A (p = 0.04), NAB List Learning Long Delay Recall (p = 0.04), Animal Fluency (p = 0.04), and the COWAT (p < 0.01). Higher WRAT-4 scores were associated with better test performance. Higher WRAT-4 scores were also associated with lower BRI (p = 0.04) scores, indicating less impairment. The largest effect was evident for the COWAT (β=0.38), followed by NAB List Learning Long Delay Recall (β=0.27), BRI (β=–0.26), TMT Part A (β=0.25), and Animal Fluency (β=0.24) (Fig. 1A; Supplementary Table 2). No significant effects were found for years of education, occupational attainment, or eTIV on any of the neuropsychological or neuropsychiatric test scores (Supplementary Table 2).
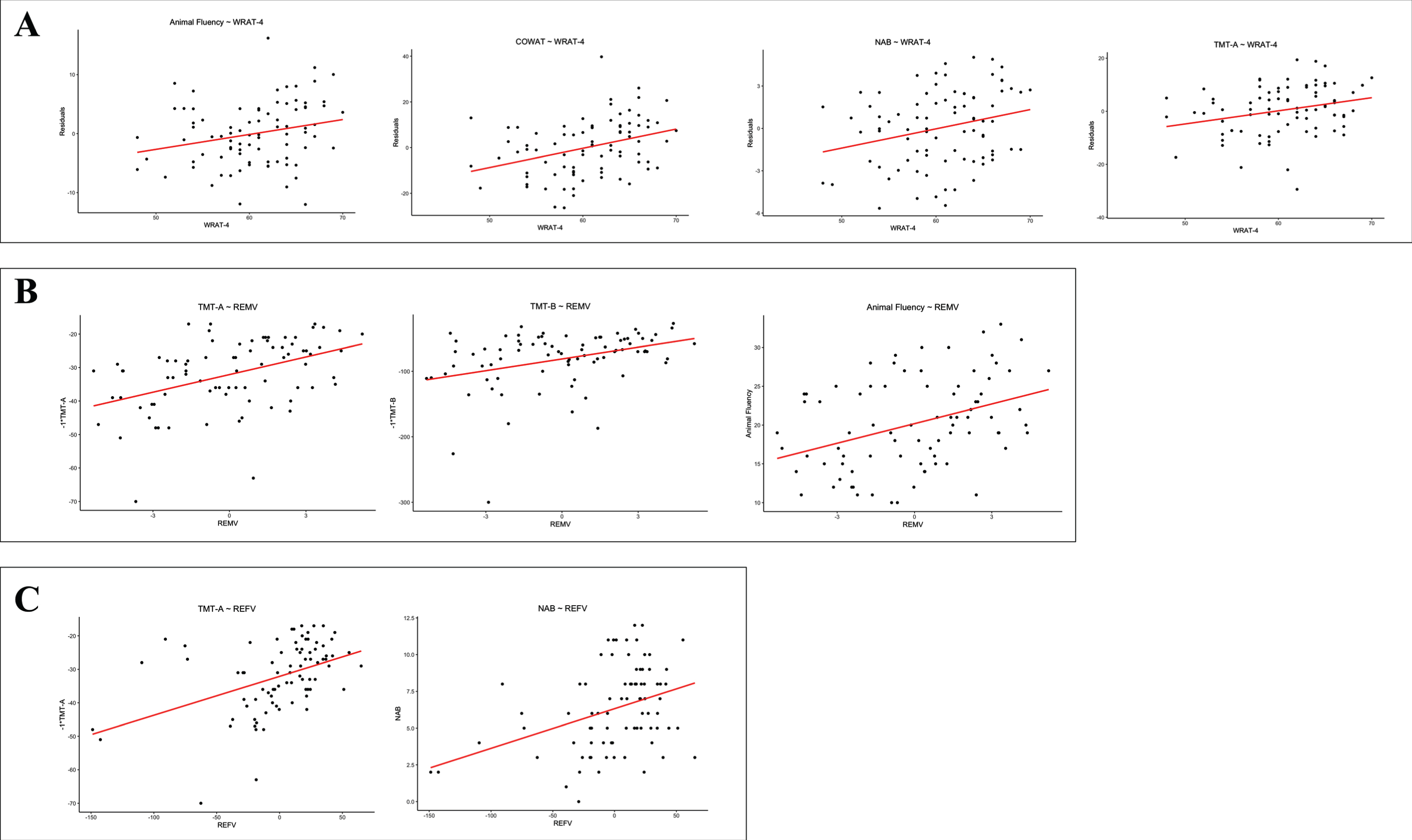
Scatterplots of significant relationships between reserve proxies and neuropsychological test scores. A) WRAT-4 and animal fluency (p = 0.04), the COWAT (p < 0.01), NAB (p = 0.04), and TMT A (p = 0.04). B) Residual episodic memory variance and TMT A (p < 0.01), TMT B (p < 0.01), and animal fluency (p < 0.01). C) Residual executive functioning variance and TMT A (p < 0.01) and NAB (p < 0.01). Statistical significance was defined by a false discovery rate adjusted p-value<0.05. Age, racial identity, CHII, and APOE genotype were included as covariates. Non-significant associations presented in Table 4 and Supplementary Table 1 not shown. CHII, cumulative head impact index; WRAT-4, Wide Range Achievement Test-4; COWAT, Controlled Oral Word Association Test; NAB, Neuropsychological Assessment Battery List Learning Long Delay Recall; TMT A, Trail Making Test Part A; TMT B, Trail Making Test Part B; REMV, residual episodic memory variance; REFV, residual executive functioning variance.
Residual Variance
Residual Episodic Memory Variance
Residual episodic memory variance scores were associated with better TMT Part A (p < 0.01), TMT Part B (p < 0.01), and Animal Fluency (p < 0.01) performance (Fig. 1B). The standardized regression coefficients for these analyses are reported in Table 4. Larger effects for residual episodic memory variance were seen for TMT Parts A and B and Animal fluency, as compared to the WRAT-4. The leave-one-out cross validation technique validated our results (Table 5, Supplementary Figure 1).
Standardized regression coefficients of residual episodic memory and executive functioning variance and neuropsychological and neuropsychiatric tests
TMT, Trail Making Test; NAB, Neuropsychological Assessment Battery; COWAT, Controlled Oral Word Association Test; BRIEF-A BRI, Behavior Rating Inventory of Executive Functioning –Adult Version Behavioral Regulation Index; BDI-II, Beck Depression Inventory-II. 1TMT Parts A and B were reverse coded to correct directionality (i.e., lower scores represented worse performance); 2Statistical significance was defined by a false discovery rate adjusted p-value<0.05. Age, racial identity, CHII, and APOE genotype were included as covariates.
Standardized regression coefficients with leave-one-out residuals as metric of reserve
TMT, Trail Making Test; NAB, Neuropsychological Assessment Battery; COWAT, Controlled Oral Word Association Test; BRIEF-A BRI, Behavior Rating Inventory of Executive Functioning –Adult Version Behavioral Regulation Index; BDI-II, Beck Depression Inventory-II. 1TMT Parts A and B were reverse coded to correct directionality (i.e., lower scores represented worse performance); 2Statistical significance was defined by a false discovery rate adjusted p-value <0.05. Age, racial identity, CHII, and APOE genotype were included as covariates.
Residual Executive Functioning Variance
Residual executive functioning variance scores were associated with better TMT Part A (p < 0.01) and NAB List Learning Long Delay Recall (p < 0.01) performance (Fig. 1C). The standardized regression coefficients for these analyses are reported in Table 4. Larger effects for residual executive functioning variance were seen for TMT Part A and NAB List Learning Long Delay Recall, as compared to the WRAT-4. The leave-one-out cross validation technique validated our results (Table 5, Supplementary Figure 1).
Post-Hoc analyses
Post-hoc analyses were performed to investigate the potential moderating effect of 1) the WRAT-4 (as the only significant traditional reserve proxy), 2) residual executive functioning variance, and 3) residual episodic memory variance on the relationship between the CHII and neuropsychological test performance and neuropsychiatric symptoms. Separate linear regression analyses were performed as above, with the addition of a 1) CHII x WRAT-4, 2) CHII x residual executive functioning variance, and 3) CHII x residual episodic memory variance interaction term. None of the interaction terms had a statistically significant effect on any of the neuropsychological or neuropsychiatric tests.
Bivariate Pearson correlations
The WRAT-4 was found to be statistically significantly correlated with residual episodic memory variance (r = 0.24, p = 0.03). No significant correlations were identified between residual episodic memory variance and the remaining three traditional reserve proxies, years of education, occupational attainment, and eTIV (Table 6). Additionally, no significant correlations were identified between residual executive functioning variance and the four traditional reserve proxies (Table 6).
Bivariate Pearson correlations between residual variance variables and four traditional reserve proxies
WRAT-4, The Wide Range Achievement Test-4.
DISCUSSION
This study investigated the role of reserve in 89 male, symptomatic, former NFL players and examined multiple methods for the measurement of reserve. Similar to other populations, higher reserve may contribute to the symptom heterogeneity observed within and across samples of former elite American football players. Residual episodic memory variance scores were shown to be associated with better performance on tests of attention and information processing, executive functioning, and semantic fluency, while residual executive functioning variance scores were associated with better performance on tests of attention and information processing and episodic memory. We additionally found that a measure traditionally believed to estimate reading ability was associated with better neuropsychological test performance and decreased neurobehavioral dysregulation, after accounting for covariates. Years of education, occupational attainment, and eTIV were not associated with cognitive test performance or neuropsychiatric symptoms.
Higher reading ability has been shown to mitigate cognitive dysfunction in neurological disorders such as AD and TBI [30, 81–83]. The current investigation indeed observed significant effects for the WRAT-4. Although word-reading tests such as the WRAT-4 have been a commonly used proxy of reserve, they may underestimate premorbid intelligence in individuals who have been exposed to head impacts at an early age [30, 77]. Moreover, the WRAT-4 provides an estimation of one’s reading ability rather than being a direct measure of intelligence itself. While this estimation may capture a proportion of reserve, it likely also encompasses a significant proportion of measurement error. A more comprehensive estimate of premorbid intelligence is needed for future studies in this population. We additionally hypothesized that reserve metrics (e.g., WRAT-4) may moderate the relationship between exposure to RHI and cognitive test performance. No such effects were found. RHI exposure in our sample of former professional athletes was retrospectively estimated using the CHII by applying accelerometer data of American football players at collegiate level. Helmet accelerometer studies are not available for the NFL and thus, as this study focused on professional athletes, the CHII may have underestimated RHI exposure in our sample. Nevertheless, the CHII remains one of the most refined metrics for quantifying RHI exposure. Accelerometer data of professional American football players is needed to overcome this limitation in future studies of this population.
No associations were identified between years of education and cognitive test performance or neuropsychiatric symptom expression. This was also the case for occupational attainment. In former professional American football players, years of education may not capture complete reserve capacity [42]. Most NFL players attain 16 years of education, which may explain the restricted variability in education duration in the current sample. In this all-male sample, variability is also lacking in eTIV [84, 85]. Lastly, in contrast to Alosco et al.’s [42] findings, the current investigation found no significant effect for occupational attainment. Again, >65% of participants in the current study reported high occupational attainment. There are also substantial differences between this sample and Alosco et al., the latter of which included a small sample of brain donors with autopsy-confirmed stage III/IV CTE. Alosco et al. also examined informant-reported age of symptom onset, whereas the present study used objective measures of cognitive and neuropsychiatric function.
In response to the aforementioned limitations of the individual reserve proxies, this study examined more refined approaches of reserve quantification. Residual episodic memory and executive functioning variance variables were created and tested for their association with cognitive and neuropsychiatric function. Residual episodic memory variance showed a significant association with better performance on tests of attention and information processing speed, executive functioning, and semantic fluency. Residual executive functioning variance was similarly associated with better performance on tests of episodic memory and attention and information processing speed performance. Larger effect sizes were evident for the residual variance approach as compared to a test of reading ability in regard to associations with neuropsychological test performance. Unlike reading ability score, the residual cognitive variance scores were not associated with any of the neuropsychiatric measures. This may be because risk factors for neuropsychiatric symptoms in this population are distinct from those used to create the residual cognitive variance scores. Behavioral disturbances in former elite contact sport athletes may also have distinct causes and/or etiologies compared with cognitive impairments. Correlation analyses revealed that a significant correlation existed between a measure of reading ability and residual episodic memory variance. This remains consistent with our findings that, out of the four traditional proxies measured in this study, reading ability was superior. On the other hand, CR is a multidimensional construct and previous research has shown that traditional reserve proxies represent distinct components of reserve, thus each providing a unique contribution to individual performance on cognitive tests [86–88]. Our findings could alternatively suggest that the newly created residual variance variables capture different aspects of reserve than the traditional reserve proxies and reading ability most closely resembles that which is measured by these variables.
The cognitive and neuropsychiatric symptomatology associated with RHI is heterogenous. Even among those with comparable neuropathological load, there can be differences in symptom presence and severity [9, 65]. Not all those subject to RHI experience subsequent cognitive dysfunction or neurobehavioral dysregulation [18, 89]. High reserve in individuals exposed to RHI may be protective against cognitive decline and may explain some of the inconsistent findings in the literature [18, 91]. Individual differences in the susceptibility to age-related brain changes have been examined extensively with regard to reserve [23, 40]. Previous research has shown that high reserve, as measured by traditional reserve proxies, is protective of cognitive decline [92, 93] and the presence of neuropsychiatric symptoms [94, 95]. Furthermore, despite higher severity of AD-related pathology, those with high reserve can still appear clinically similar to those with low reserve and less AD pathology [39]. The exact neural mechanism underlying reserve is currently unknown [39]. Colangeli et al. [96] showed that reserve proxies (i.e., education, occupation, and leisure activities) were associated with activation in the anterior cingulate cortex. Also, Wilson et al. [97] demonstrated that reduced neuronal density (i.e., reserve at the neuronal level) in the locus coeruleus and brain stem neurofibrillary tangles and Lewy bodies were predictive of the rate of cognitive decline in AD. Research has also indicated that the relationship between amyloid plaques and cognitive functioning is moderated by formal years of education [98]. Reserve factors may similarly influence the expression of p-tau and other neuropathologies, as well as resulting clinical syndromes associated with RHI.
There are limitations to our findings. While a number of significant effects were found, the meaningfulness of these effects remains unclear (as shown in Fig. 1). Moreover, the sample included male former NFL players, and it is unclear if our findings generalize to the broader American football population, other contact sports, or female athletes. Future research should focus on exploring alternative methods of reserve/resilience quantification in these other samples. The current research was also cross-sectional. Prospective studies are needed to determine how reserve factors might mitigate cognitive and neuropsychiatric decline. Defining and quantifying reserve, particularly in groups with RHI exposure, is problematic and no consensus has yet been reached. The comparison of results between reserve-based research investigations remains difficult and there is a great need for a more exhaustive and standardized method of reserve estimation. The residual variance method shows promise towards finding a solution to these issues by encompassing multiple aspects of reserve into a single component. Although, the proportion of the residual scores that represent reserve versus random error is unknown, significant measurement error also exists when estimating reserve using traditional proxies. Future research should focus on investigating the applicability of the residual variance approach to reserve quantification in a sample with neuropathologically confirmed CTE to provide further insight into the role of reserve in the clinical expression of this pathology. Furthermore, more refined measures of reserve are required to further understand its predictors. This investigation made use of total brain, hippocampal, and WM-hypo volumes to derive residual variance scores in order to capture the effects of atrophy and cerebrovascular disease. Other brain regions and types of pathology might be more suitable in people exposed to RHI, such as microstructural injury from diffusion tensor imaging. Therefore, future research should focus on exploring alternative methods of capturing the effects of atrophy and cerebrovascular disease.
Conclusions
Reading ability, residual episodic memory variance, and residual executive functioning variance as proxies of reserve were associated with better cognitive test performance in former NFL players. Larger effects were evident for the residual cognitive variance approach. The quantification of reserve by means of single proxies (e.g., years of education, occupational attainment) remains problematic and may be unsuitable for use in this population. The residual variance method may be a suitable alternative to overcome these issues. Continued research is needed to better define optimal measurement of reserve and resilience in former elite American football players and other contact sport populations.