
Abstract
Background:
Photobiomodulation (PBM) affects local blood flow regulation through nitric oxide generation, and various studies have reported on its effect on improving cognitive function in neurodegenerative diseases. However, the effect of PBM in the areas of the vertebral arteries (VA) and internal carotid arteries (ICA), which are the major blood-supplying arteries to the brain, has not been previously investigated.
Objective:
We aimed to determine whether irradiating PBM in the areas of the VA and ICA, which are the major blood-supplying arteries to the brain, improved regional cerebral blood flow (rCBF) and cognitive function.
Methods:
Fourteen patients with mild cognitive impairments were treated with PBM. Cognitive assessment and single-photon emission computed tomography were implemented at the baseline and at the end of PBM.
Results:
Regarding rCBF, statistically significant trends were found in the medial prefrontal cortex, lateral prefrontal cortex, anterior cingulate cortex, and occipital lateral cortex. Based on the cognitive assessments, statistically significant trends were found in overall cognitive function, memory, and frontal/executive function.
Conclusion:
We confirmed the possibility that PBM treatment in the VA and ICA areas could positively affect cognitive function by increasing rCBF. A study with a larger sample size is needed to validate the potential of PBM.
Keywords
INTRODUCTION
Photobiomodulation (PBM) is a therapeutic treatment that irradiates the skin with red/near-infrared light (600–940 nm) [1]. According to research results, red/near-infrared light can activate energy metabolism and regulate local blood flow by promoting the secretion of intracellular nitric oxide (NO) and increasing activity of the mitochondrial respiratory chain [2, 3]. Additionally, it can induce stem cell differentiation and cell proliferation and regeneration by increasing the level of calcium ions (Ca2 +), reactive oxygen species, and ATP production [4]. Based on this, PBM is mainly used in treatments to relieve pain, edema, oxidative stress, and inflammation in various traumatic, acute, and chronic diseases [5–9]. In recent years, research on the efficacy of PBM has gradually expanded due to its neuroprotective benefits and application in treatment of various diseases, including neurodegenerative diseases [8–12].
Particularly, various studies have reported on the effect of PBM for enhancing cognitive function in neurodegenerative diseases based on its ability to influence regulation of regional cerebral blood flow (rCBF) [13–20]. In animal models, brain activity and cognitive function in rats improved significantly after PBM irradiation [21–24], and studies in humans have demonstrated the effectiveness and safety of PBM in terms of cognitive function in patients [18–20, 25–31].
Dementia is one of the most common neurodegenerative diseases associated with decreased cognitive function and brain activity [32]. Therefore, previous PBM studies related to neurodegenerative disease were mainly conducted on healthy individuals or patients with dementia [13, 25–29]. However, as dementia treatment mainly focuses on preventing or delaying progression, it is also necessary to observe the effect of PBM in pre-dementia stages, such as in the mild cognitive impairment (MCI) group, which shows a higher conversion rate to dementia than the normal group [33]. MCI is accompanied by cognitive decline and decreased cerebral blood flow, along with Alzheimer’s disease and other forms of dementia [34, 35]. Therefore, PBM may also have a positive effect on rCBF or cognition in MCI.
Since it has been suggested that PBM regulates local blood flow through NO production [17], most cognition-related PBM studies performed to date have used methods to increase rCBF using irradiating PBM, such as transcranial PBM [13, 25–29]. However, PBM has low light intensity, thus the light entering the brain can be affected by hair, making the clinical use of PBM difficult in areas with a lot of hair.
The main arteries that supply blood to the brain are the vertebral arteries (VA) and internal carotid arteries (ICA) [36]. Once these arteries enter the cranium, they branch exuberantly, eventually supplying blood to the deep and superficial regions of the brain [37]. The sternocleidomastoid muscle area through which the ICA passes and the trapezius muscle area through which the VA passes have less hair, making it easier to transmit light.
Based on this theory, we hypothesized that PBM near the major arteries that supply blood to the brain could be associated with improved cognitive function and cerebral blood flow in patients. To confirm this hypothesis, we assessed whether rCBF increased through long-term use of PBM in the VA and ICA regions in patients with MCI. Further, we examined whether the PBM-induced changes in rCBF correlated with an improvement in cognitive function.
MATERIALS AND METHODS
This study was conducted from December 2019 to June 2020. This pilot study was approved by the Pusan National University Yangsan Hospital ethics committee (approval no. 03-2018-003) and registered on Clinictrials.gov (NCT04721093). We enrolled 14 elderly adults. The sample size is based on previous studies [13, 25–29]. The inclusion criteria for this study were patients aged over 55 years diagnosed with MCI. MCI was diagnosed by a neurological specialist according to the criteria for neurocognitive examination [38]. The exclusion criteria were those with neurological disorders, those with mental disorders, such as major schizophrenia, and those with a Mini-Mental State Examination (MMSE) score of 18 or less and considered to have dementia [39]. Informed consent was obtained from the patients.
Several previous studies chose near-infrared light wavelengths between 810 and 1064 nm to penetrate the bone [13, 27–29]. However, in this study, we chose a lower wavelength because the light passes through the skin and not the bone. The wavelength of 600 nm (±20 nm) has been reported as a wavelength that promotes the production of NO in vivo [40]. The PBM device (Color-DNA-WSF U, Color Seven; 610±10 nm wavelength; 3.0 mW/cm2±20%) was attached to the sternoclavicular mastoid muscle, in the ICA area, and the trapezius muscle, in the VA area of the patients (Fig. 1). Detailed parameters of PBM can be found in Table 1.
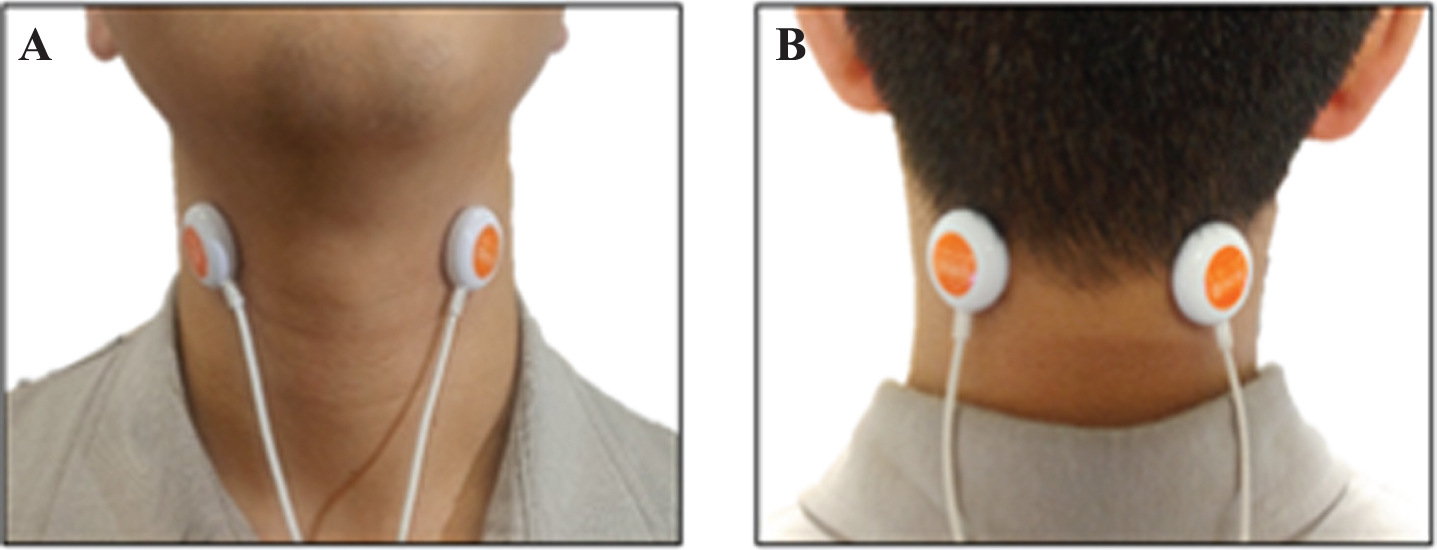
The PBM device was applied and irradiated simultaneously at the sternoclavicular mastoid muscle in the ICA area (A) and the trapezius muscle in the VA area (B) of the patients.
Parameters of the PBM device
In previous studies that looked at cognitive changes after applying PBM in humans, stimulation sessions were carried out daily or three times a week. In the protocols, cognitive function improved after 6–12 weeks of treatment [13, 25–29]. Accordingly, patients enrolled for the present study were treated with 30 min sessions, five times a week for a period of 8 weeks. Participants visited the hospital a total of 40 times for treatment. The patients were told not to take drugs that could affect cognitive function, such as Albix and Whanin Donepezil; depression treating agents, such as escitalopram; or blood pressure medication, throughout the duration of the study. Cognitive function assessments and technetium-99m hexamethyl propylenamine oxime single photon emission computed tomography (Tc-99m HMPAO SPECT) scans were performed at the beginning and at the end of the PBM treatment. Participants were tested only twice, before PBM and after an 8-week interval to minimize the learning effect.
In order to assess overall cognitive function, all patients were evaluated using the Montreal Cognitive Assessment (MoCA) [41]. The Verbal Learning Test (VLT) was used to assess the patients’ memory domain [42]. In order to evaluate the frontal/executive functions the Trail Making Test (TMT) was applied to all patients [43]. The Boston Naming Test (BNT) was employed to assess the patients’ visual confrontation naming [44]. The last test implemented in the present study was the Rey Complex Figure Test (RCFT), which allowed for the evaluation of the patients’ ability to recognize and recall complex geometric designs [45].
Changes in rCBF were measured through Tc-99m HMPAO SPECT imaging, which was then converted into a Z-score using Tc-99m HMPAO SPECT (General Electric NM 830 SPECT, USA). The Z-score is the standard deviation of region means from the normal group. The closer the Z-score is to 0, the closer it is to the average value of the normal group.
Statistical analyses were performed using SPSS Statistics 18 (SPSS Inc, Chicago, IL). Repeated-measure ANOVAs were used to control for baseline differences in the study group age values and covariates and compare the cognitive tests scores and the rCBF Z-score before and after the patients underwent treatment. A p-value < 0.05 was considered to be statistically significant.
RESULTS
All patients completed treatment without dropout. No side effects were observed during the treatment period. Patients were found to have had consumed drugs, such as antihistamines and acetaminophen; however, they did not take drugs that could affect rCBF or cognition related to the results of this study. There were a total of 14 patients, of which 5 were men and 9 were women. The mean age of the patients was 63.86±6.10 years. They had an average of 12.36±2.71 years of education, and a mean MoCA score of 20.14±2.10. Detailed results of demographic analysis can be found in Table 2.
Baseline demographics of the patients
MoCA, Montreal Cognitive Assessment.
Figure 2 shows 3D cortical surface images before and after PBM. There were statistically significant differences between the baseline and after treatment rCBF Z-score in the following areas of the cerebral cortex: medial prefrontal cortex (mPFC) (F = 7.977, p = 0.018), lateral prefrontal cortex (lPFC) (F = 6.901, p = 0.025), anterior cingulate cortex (ACC) (F = 51.619, p = 0.000), and occipital lateral cortex (OLC) (F = 7.958, p = 0.018) (Table 3).

Z-score 3D cortical surface images before and after PBM. The image indicates that the rCBF is closer to that of the normal group after (B) than before PBM (A). The Z-score is the standard deviation of region means from the normal group. The closer the Z-score is to 0 (black color), the closer it is to the average value of the normal group.
Cognitive and rCBF Z-score outcome measures
Data are expressed as mean±SD (standard deviation). H df, Hypothesis df; E df, Error df; MoCA, Montreal Cognitive Assessment; VLT, Verbal Learning Test; TMT Trial Making Test; BNT, Boston Naming Test; RCFT, Rey Complex Figure Test; lPFC, Lateral Prefrontal Cortex;, mPFC, Medial Prefrontal Cortex; PIC, Parietal Inferior Cortex; PSC, Parietal Superior Cortex; OLC, Occipital Lateral Cortex; PVC, Primary Visual Cortex; PC, Precuneus Cortex; SC, Sensorimotor Cortex; TLC, Temporal Lateral Cortex; TMC, Temporal Mesial Cortex; ACC, Anterior Cingulate Cortex; PCC, Posterior Cingulate Cortex. p < 0.05*.
In cognitive assessments, statistically significant trends were found in MoCA (F = 63.247, p = 0.000), VLT (F = 14.967, p = 0.003), TMT (F = 5.175, p = 0.046), BNT (F = 18.749, p = 0.001), and RCFT (F = 9.244, p = 0.012) (Table 3) between the measurements taken before and after PBM treatment.
DISCUSSION
In this study, we examined changes in rCBF and cognitive functions derived from PBM irradiation in the VA and ICA regions in patients with MCI. Furthermore, this is the first study to directly investigate whether changes in cognitive function are associated with changes in rCBF in patients irradiated with PBM in the VA and ICA regions.
We found that rCBF in the mPFC, lPFC, ACC, and OLC increased in patients after PBM. This finding is similar to that of previous studies that showed an increase in rCBF after transcranial or intranasal PBM in healthy participants [19, 46], patients with dementia [13], MCI [27], and traumatic brain injury [20, 47]. Thus, this result confirmed our hypothesis that PBM increases cerebral blood flow by promoting the secretion of intracellular NO.
Additionally, scores on the MoCA, VLT, TMT, BNT, and RCFT cognitive tests were improved in patients irradiated with PBM. The improved cognitive evaluation domains were executive function, language, and visual memory. Working memory and executive function are considered the most important functions associated with the mPFC and ACC [26, 48]. The lPFC is primarily involved in working memory, executive functions, and combination of complex languages [49]. The OLC processes and communicates the visual form of objects [50]. Therefore, the increase in regional blood flow to these structures seems to be related to improvement in cognitive function.
According to the hypotheses presented in previous studies, PBM can promote the activity of mitochondria or activate energy metabolism in the brain [2, 3]. In this study, since the PBM was not directed to the brain, it is difficult to expect this effect. Nevertheless, significant improvements in cognitive function after intervention were seen. This presents the possibility that PBM in the VA and ICA areas may be a treatment option for cognitive improvement in MCI patients through improvement in rCBF. Moreover, compared to transcranial or intranasal PBM, PBM in the VA and ICA areas is easy to apply, and it can be clinically useful because of its therapeutic effect even with low wavelength light without obstacles, such as hair and the skull.
The present study did not assess a placebo control group; therefore, this study presents limitations regarding the difficulty to exclude the learning effect in patients due to repeat cognitive function evaluations before and after undergoing PBM therapy. Furthermore, it is difficult to generalize the results due to the small sample size. However, the present study is meaningful because it is the first PBM study to analyze rCBF and cognitive changes by examining PBM in the VA and ICA regions in MCI patients. PBM stimulation of the ICA and VA areas shows promise as a novel cognitive therapy for patients with MCI.
The results of this study confirmed the possible positive effect of PBM in the VA and ICA regions on cognitive functions and rCBF and showed that cognitive improvements after PBM are related to rCBF increase. These results are meaningful, in that, they serve as evidence to support the results of previous studies that improved cognitive function through PBM. A randomized control trial study with a larger sample size is required to obtain a generalization of the effects of PBM on patients with MCI.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Technology Innovation Program (‘10067221’) funded By the Ministry of Trade, Industry & Energy (MOTIE, Korea) and Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT (NRF-2017M3A9E9032772).