
Abstract
Background:
Primary progressive aphasia (PPA) is associated with amyloid-β (Aβ) pathology. However, clinical feature of PPA based on Aβ positivity remains unclear.
Objective:
We aimed to assess the prevalence of Aβ positivity in patients with PPA and compare the clinical characteristics of patients with Aβ-positive (A+) and Aβ-negative (A–) PPA. Further, we applied Aβ and tau classification system (AT system) in patients with PPA for whom additional information of in vivo tau biomarker was available.
Methods:
We recruited 110 patients with PPA (41 semantic [svPPA], 27 non-fluent [nfvPPA], 32 logopenic [lvPPA], and 10 unclassified [ucPPA]) who underwent Aβ-PET imaging at multi centers. The extent of language impairment and cortical atrophy were compared between the A+ and A–PPA subgroups using general linear models.
Results:
The prevalence of Aβ positivity was highest in patients with lvPPA (81.3%), followed by ucPPA (60.0%), nfvPPA (18.5%), and svPPA (9.8%). The A+ PPA subgroup manifested cortical atrophy mainly in the left superior temporal/inferior parietal regions and had lower repetition scores compared to the A–PPA subgroup. Further, we observed that more than 90% (13/14) of the patients with A+ PPA had tau deposition.
Conclusion:
Our findings will help clinicians understand the patterns of language impairment and cortical atrophy in patients with PPA based on Aβ deposition. Considering that most of the A+ PPA patents are tau positive, understanding the influence of Alzheimer’s disease biomarkers on PPA might provide an opportunity for these patients to participate in clinical trials aimed for treating atypical Alzheimer’s disease.
INTRODUCTION
Primary progressive aphasia (PPA) is a heterogeneous clinical syndrome characterized by progressive language impairment due to focal degenerative change of the dominant hemisphere related to lan-guage function. Based on clinical features of lan-guage dysfunction and neuroimaging findings, PPA is classified as non-fluent/agrammatic variant PPA (nfvPPA), semantic variant PPA (svPPA), and logo-penic variant PPA (lvPPA) [1]. In addition, patients with PPA having clinical features of two or more subtypes are regarded as unclassified PPA (ucPPA) [1].
Studies showed that approximately 40% of PPA cases are associated with Alzheimer’s disease (AD) pathology [2, 3]. Specifically, 64–100% of lvPPA cases [2, 3] and approximately 60% of ucPPA cases are reported to have AD pathology [2]. However, very few studies have investigated the language profiles in patients with PPA having AD pathology. In 2018, the National Institute on Aging–Alzheimer’s Association task force proposed a new research framework using a biomarker-based definition of AD [4, 5], which included amyloid-β (Aβ, A), pathologic tau (T), and neurodegenerative/neuronal injury (N), termed as the AT(N) system. However, very few studies applied the AT system in patients with PPA [6]. Furthermore, the AT classification system has not been extensively applied in Korean PPA patients who have quite different language and culture from European PPA patients.
Herein, we assessed the prevalence of Aβ positivity in a relatively large sized cohort of Korean patients with nfvPPA, svPPA, lvPPA, and ucPPA sub-types. We also explored the language profiles and neuroimaging features related to Aβ in these patients. Finally, we applied the AT system in these patients with the additional information of in vivo tau bio-marker. We hypothesized that AT biomarker positivity differed across the PPA subtypes and might be associated with distinct language profiles in patients with PPA.
MATERIALS AND METHODS
Study participants
We recruited 110 patients with PPA who underwent either 18F-florbetaben PET (N = 62) or 18F-flutemetamol PET (N = 48) between October 2014 and December 2019. The patients were chosen from a multiple center-based cohort in Korea (81 from Samsung medical center (SMC), 15 from Busan National University Hospital, 7 from Gangnam Severance Hospital, and 7 from Gachon University Gil Medical Center). All patients met the core criteria for PPA, which are as follows: 1) language impairment is the first and the most prominent clinical feature; 2) language impairment is the main cause of impairment of activities of daily living, at least during the first 2 years after disease onset [1]. Based on the PPA consensus criteria [1] by looking for major and minor features of the PPA subtypes, patients were further classified as having nfvPPA, svPPA, lvPPA, and ucPPA. Patients were diagnosed as ucPPA when they fulfilled the criteria for multiple PPA subtypes (mixed type) [2, 7].
All patients underwent comprehensive dementia evaluation, including a clinical interview, neurologi-cal examination, clinical test for language function, standardized neuropsychological tests, blood tests, and conventional magnetic resonance imaging (MRI). Apolipoprotein E (APOE) genotyping was performed in 98 (89.1%) patients. For the evaluation of AD-associated paired-helical filament tau, 33 (30.0%) and 4 (3.6%) participants underwent 18F-flortaucipir PET and lumbar puncture, respectively.
We excluded patients with secondary causes of cognitive deficits examined by blood tests including vitamin B12 test, syphilis serology, and thyroid/kidney/liver function tests. Patients with structural lesions on conventional brain MRI, including brain tumor, cerebral infarction, cerebral hemorrhage, or severe white matter hyperintensities, assessed using the modified Fazekas ischemic scale, were also excluded. Patients clinically diagnosed with other types of neurodegenerative diseases such as AD, behavioral variant frontotemporal dementia, cortico-basal syndrome, progressive supranuclear palsy, dementia with Lewy bodies, or Parkinson’s disease dementia at baseline evaluation were also excluded.
The institutional review boards at the SMC, Busan National University Hospital, Gangnam Severance Hospital, and Gachon University Gil Medical Center approved this study. Written informed consent was obtained from the patients or caregivers of patients with advanced dementia.
Diagnostic process for determining PPA subtype
All the patients with language problems went through a three-step diagnostic process. In the first step, experienced clinicians with the help of neurology residents or fellows obtained a history with respect to language impairments as well as cognitive, behavioral, and functional impairments. The presence of the features of PPA was clinically judged based on the interview of patients and caregivers and the patients underwent a clinical screening test for language functions including tasks for spontaneous speech, single-word comprehension (asking the patient to point to an item), repetition, confrontation naming, single word reading and writing was performed on their first visit to the outpatient clinic. In the second step, the speech language pathologist team independently performed clinical interview for language disturbances and screening task for particle/postposition use, speech screening test for apraxia of speech (AOS) and dysarthria. The speech language pathologist team also performed the K-WAB including fluency of spontaneous speech, auditory word recognition, command comprehension, repetition, confrontational naming, reading, writing and generative naming. On the basis of these results, the speech language pathologist team made their own judgment as to which subtype of PPA the patient had. Finally (third step), the patient returned to the clinic with all the results (speech language reports, neuropsychological reports, blood tests, and MRIs) which led to a consensus for the diagnosis of PPA subtype.
For 35 (31.8%) patients who did not complete K-WAB, presence of the features of PPA were clinically judged based on the interview of patients and caregivers and the patients underwent a clinical screening test for language functions including tasks for spontaneous speech, single-word comprehension (asking the patient to point to an item), repetition, confrontation naming, single word reading and writing was performed on their first visit to the outpatient clinic.
We did not determine agrammatism using cut point. However, we clinically and carefully judge agrammatism by analyzing the length of utterances, grammatical complexity of the utterances, manifestations of grammatical errors such as errors in particles/postposition, conjunction, and verb conjugation.
Acquisition of Aβ-PET and determination of Aβ positivity
All participants underwent Aβ-PET as follows: 52 18F-florbetaben PET and 29 18F-flutemetamol PET scans at SMC employing the Discovery STe PET/CT scanner (GE Medical Systems, Milwaukee, WI, USA); 3 18F-florbetaben PET and 12 18F-flu-temetamol PET scans at Busan National University Medical Center employing the Discovery STe PET/CT scanner (GE Medical Systems, Milwaukee, WI, USA); 7 18F-florbetaben PET scans at Gangnam Severance Hospital employing the Biograph mCT PET/CT scanner (Siemens Medical Solutions; Malvern, PA, USA); and 7 18F-flutemetamol PET scans at Gachon University Gil Medical Center employing the Siemens Biograph 6 True-point PET/CT scanner (Siemens, Knoxville, TN, USA). For 18F-florbetaben PET and 18F-flutemetamol PET, a 20-min emission PET scan with dynamic mode (con-sisting of 4×5 min frames) was performed 90 min after injecting 311.5 MBq 18F-florbetaben or 197.7 MBq 18F-flutemetamol. We reconstructed PET images in a 128×128×48 matrix with 2×2×3.27 mm voxel size using the ordered-subsets expectation maximization (OSEM) algorithm (18F-florbetaben, iteration = 4 and subset = 20; 18F-flute-metamol, iteration = 4 and subset = 20).
Two clinicians (one nuclear medicine physician and one neurologist) visually evaluated the Aβ-PET images, blinded to the clinical information, and categorized the images as either Aβ-positive (A+) or Aβ-negative (A–) using visual reads. In case of discrepancy, consensus was reached through discussion. 18F-florbetaben PET was regarded as positive if the amyloid plaque load on the scans was 2 or 3 based on the plaque load scoring system. 18F-flutemetamol PET was classified as positive when one of the five brain regions (frontal, parietal, posterior cingulate and precuneus, striatum, and lateral temporal lobes) was positive in either hemisphere [8].
Acquisition of tau PET and determination of tau PET positivity
Thirty-three participants underwent 18F-AV-1451 PET at Gangnam Severance Hospital using the Biograph mCT PET/CT scanner (Siemens Medical Solutions, Malvern, PA, USA). For 18F-AV-1451 PET, a 20-min emission PET scan was performed 80 min after injecting 280 MBq 18F-AV-1451. We reconstructed PET images in a 256×256×223 matrix with 1.591×1.591×1 mm voxel size using the OSEM algorithm (iteration = 6 and subset = 16), and co-registered to individual MRIs, which were normalized to a T1-weighted MRI template. Normalized parameters were applied to transform the co-registered PET images into the MRI template. We obtained the standardized uptake value ratios (SUVRs) using the cerebellar gray matter as the reference region. We used the SPM version 8 (SPM8) software with MATLAB 2014b (MathWorks, Natick, MA, USA) for data processing. To analyze regional PET uptake, we used the Freesurfer software (version 5.1; https://surfer.nmr.mgh.harvard.edu/) to describe the region of interest (ROI) masks. We measured the regional SUVRs for 25 cortical regions, as previously described [9].
Tau PET images were categorized as either tau-positive (T+) or tau-negative (T–) based on in vivo Braak staging. We defined 18F-AV-1451 PET scans as positive if the in vivo Braak stage was ≥III/IV (using the conditional inference tree approach) and negative if the in vivo Braak stage was < III/IV. This approach includes decision tree-based regression models to determine in vivo Braak staging based on AV-1451 uptake [10]. As previously described in detail [9], this regression model assigns subjects with a mean Braak V/VI ROI AV-1451 SUVR >1.578 to the in vivo Braak stage V/VI. The remaining subjects underwent the same procedure as Braak III/IV (>1.331) followed by Braak I/II (>1.286) ROIs, leaving the remaining participants in the in vivo Braak stage 0.
Assessment of phosphorylated tau in the CSF
Four participants underwent lumbar puncture at Busan National University Hospital for the evaluation of CSF biomarkers including Aβ1 - 42, t-tau, and p-tau181. CSF samples were analyzed as previously described [11]. CSF tau was classified as positive if the p-tau181 level in the CSF was more than 56.4 pg/mL. This cut-off was chosen based on a previous study that showed that 56.4 pg/mL is the optimal cut-off value for CSF biomarkers that could differentiate the AD-associated dementia group from the normal cognition group [11]. As described in previous studies [12, 13], CSF p-tau181 assessment and 18F-AV-1451 PET are equally good for diagnosing AD, and the correlation between SUVR values in 18F-AV-1451 PET and p-tau181 levels in the CSF was robust.
Acquisition of three-dimensional MR images
Three-dimensional T1 turbo field echo MRI was performed on 71 participants with PPA at SMC using a 3.0 T MRI scanner (Philips 3.0T Achieva) with the following imaging parameters: sagittal slice thickness of 1.0 mm with 50% overlap; no gap; repetition time of 9.9 ms; echo time of 4.6 ms; flip angle of 8°; and matrix size of 240×240 pixels reconstructed to 480×480 over a field view of 240 mm.
MRI data processing for cortical thickness measurements
We used the CIVET anatomical pipeline (version 2.1.0) to process the MRI data [14]. The detailed procedure of MRI data processing has been described in a previous study [15]. Seventeen cortical thickness values could not be calculated because of technical errors including CIVET pipeline error (n = 4), error due to atrophy (n = 10), skull mask error (n = 1), par error (n = 1), and Laplace error (n = 1). As a result, 54 cortical thickness values were obtained.
Cortical thickness pattern analysis
To analyze the cortical atrophy pattern of each patient with ucPPA, we used the Inbrain® program, which is a Korea Food and Drug Administration (KFDA)-cleared software for individualized cortical atrophy pattern analysis and a registered trademark of MIDAS Information Technology Co., Ltd. The program can perform fully automatic MRI image analysis of brain structures using the pre-calculated cortical thickness data. The proposed method was composed of two steps as described in our previous study [16].
Language assessment
We administered the Korean version of the Western Aphasia Battery (K-WAB), which is a standardized language function test [17], to 75 participants with PPA at SMC. These patients were evaluated by a certified speech-language specialist. The scoring systems of the K-WAB mostly remained the same as those of the original Western Aphasia Battery. However, some aspects of the rating scale were changed, as previously described [18]. Few patients could not complete all the tests. We acquired additional results using the Korean version of the Boston naming test (K-BNT) and assessed semantic word fluency and phonemic word fluency using the Seoul Neuropsychological Screening Battery, 2nd edition [19], from participants with PPA at Busan National University Hospital.
Statistical analyses
We performed the independent t-test for continuous variables and chi-square test for categorical variables to compare the clinical characteristics of patients with A–and A+ PPA. To compare the frequency of Aβ positivity between PPA subtypes, we used the chi-square test and Fisher’s exact test with Bonferroni correction. To compare the language features between patients with A–and A+ PPA, we performed the analysis of covariance (ANCOVA) adjusted for age, sex, and years of education. SPSS version 25.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the statistical data. Statistical significance was set at p < 0.05.
For cortical thickness analysis from MRI data, we used a MATLAB-based toolbox (freely available online at the University of Chicago website: https://galton.uchicago.edu/faculty/InMemoriam/worsley/research/surfstat/). To identify the differences in cortical atrophy patterns between the A–and A+ PPA subgroups, we analyzed the localized differences in cortical thickness using a general linear model after adjusting for age, sex, years of education, and ICV. Because multiple comparisons were performed for 81,924 vertices, we considered an uncorrected p-value of 0.01 as significant.
RESULTS
Clinical characteristics of the participants
Table 1 shows the clinical characteristics of patients with PPA. The mean age of patients was 73.9±7.4 years, 55 (50.0%) patients were women, mean years of education was 11.1±4.6, and the mean Mini-Mental State Examination (MMSE) score was 18.6±8.9. All patients were right-handed. There were no differences in the mean age, sex ratio, years of education, mean MMSE score, Clinical Dementia Rating-sum of box (CDR-SOB) score, and the frequency of APOE4 carriers between the four PPA subtypes.
Demographics and clinical characteristics of study participants
Values are presented as mean±standard deviation. The p-value was obtained by independent t-test and chi-square test. aMMSE scores were collected from 102 (92.7%) of the 110 participants. bCDR scores were collected from 92 (86.0%) of the 107 participants. cAPOE genotyping was performed in 98 (89.1%) of the 110 participants. svPPA, semantic variant primary progressive aphasia; nfvPPA, non-fluent variant primary progressive aphasia; lvPPA, logopenic variant primary progressive aphasia; ucPPA, unclassified primary progressive aphasia; MMSE, Mini-Mental State Examination; CDR-SOB, Clinical Dementia Rating (sum of boxes).
Frequency of Aβ positivity according to PPA subtypes
Forty-one patients with PPA (37.3%) were A+. The frequency of Aβ positivity differed across the PPA subgroups (p < 0.001) (Fig. 1). Specifically, patients with lvPPA had the highest frequency of Aβ positivity (81.3%), followed by ucPPA (60.0%), nfvPPA (18.5%), and svPPA (9.8%). The frequency of Aβ positivity in patients with lvPPA was significantly higher compared to that in patients with nfvPPA (p < 0.001) and svPPA (p < 0.001), while it was not significantly different from that in patients with ucPPA (p = 0.213). The frequency of Aβ positivity in patients with ucPPA was also significantly higher than that in patients with nfvPPA (p = 0.038) and svPPA (p = 0.002).
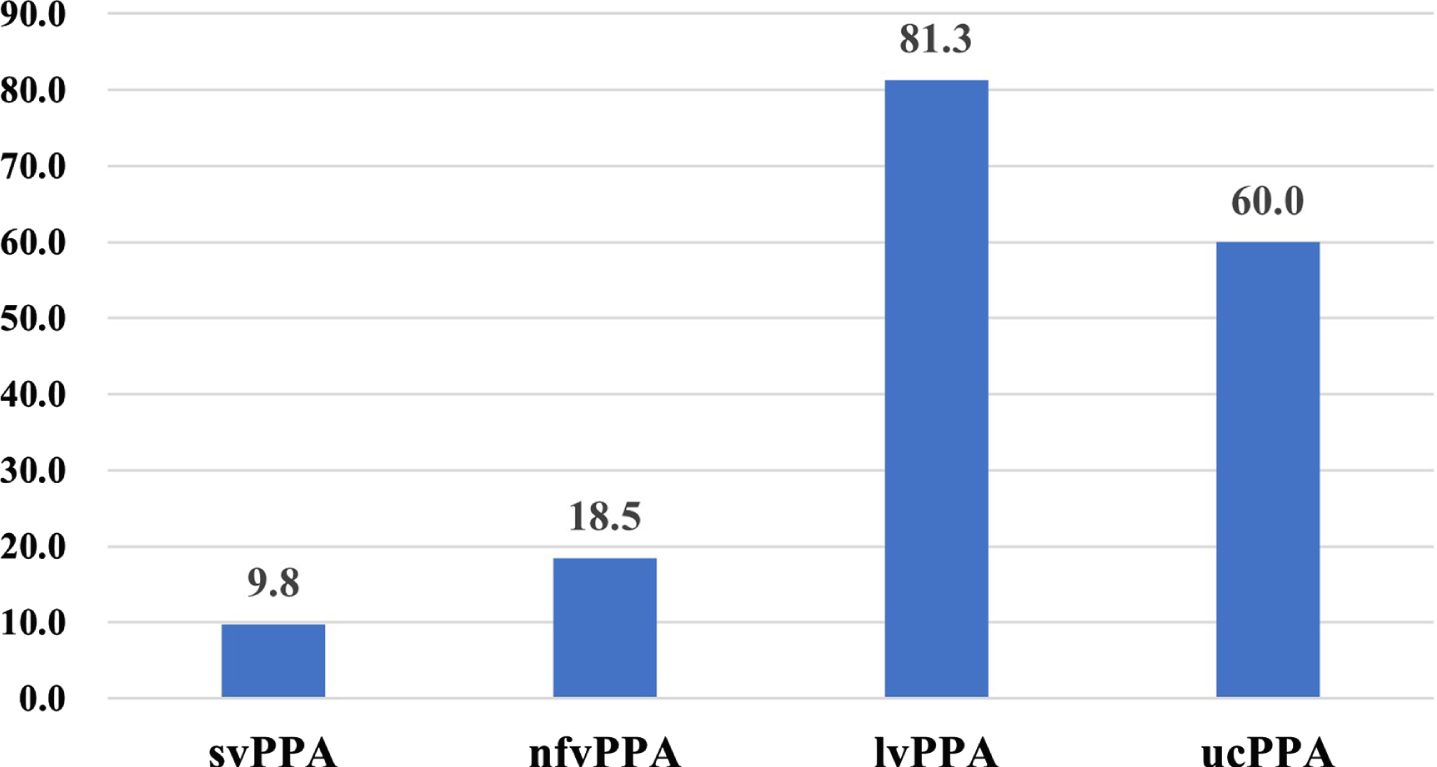
Frequency of Aβ positivity in different PPA subtypes. Values depicted in the bar plot represent Aβ positivity in different PPA subtypes. Aβ, amyloid; svPPA, semantic variant primary progressive aphasia; nfvPPA, non-fluent variant primary progressive aphasia; lvPPA, logopenic variant primary progressive aphasia; ucPPA, unclassified primary progressive aphasia.
Detailed clinical characteristics of 10 patients with ucPPA
Among 10 patients with ucPPA, all six of the patients with A+ ucPPA showed mixed features of lvPPA and svPPA, including one or two core features and supporting features of each PPA subgroup (Fig. 2). These patients had dominant left parietotemporal atrophy, except one patient who had the atrophy pattern of svPPA. However, patients with A–ucPPA were prone to have non-fluent features and frontal atrophy.
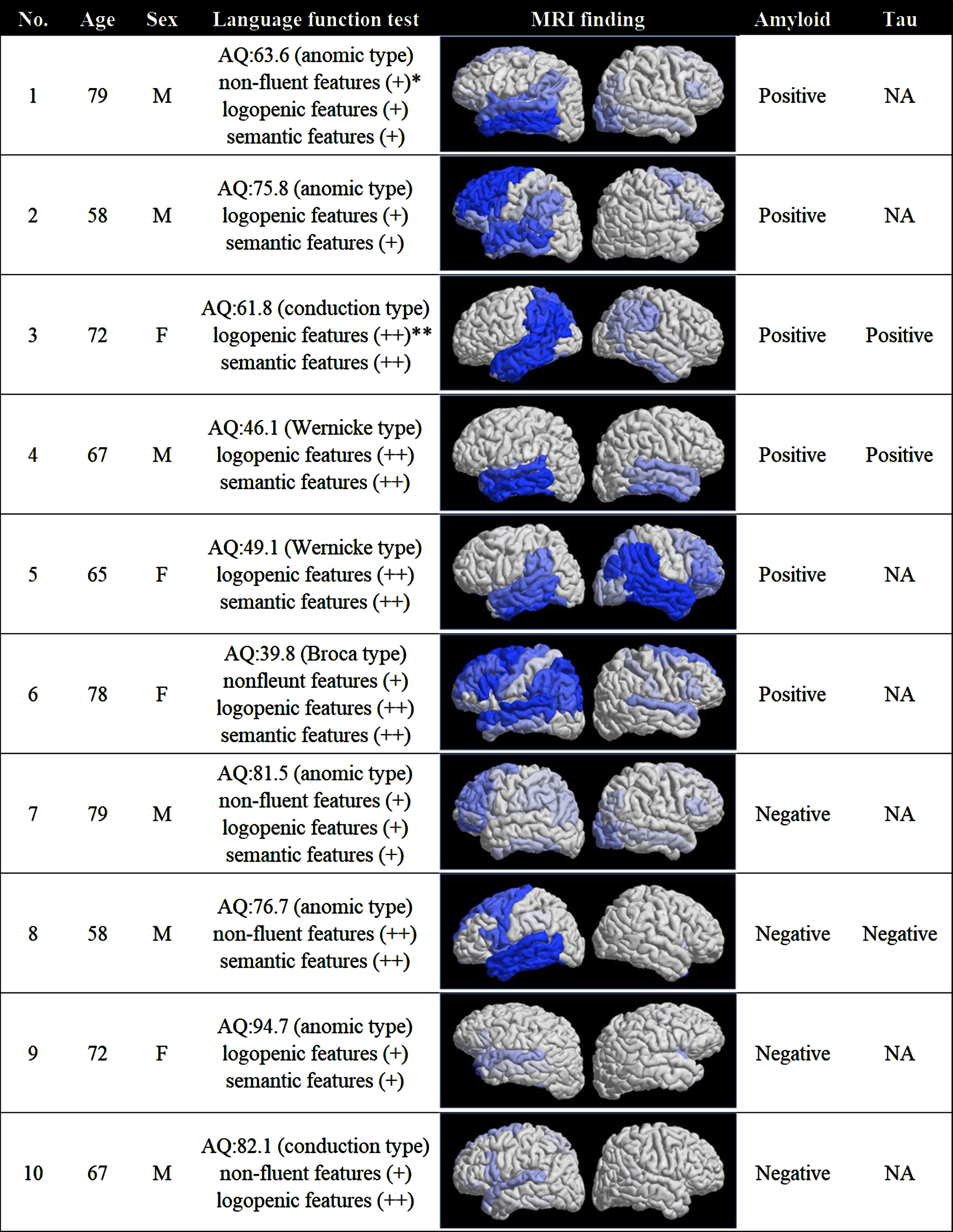
Detailed clinical, language, and brain MRI findings in ucPPA. Figure shows demographics and patterns of language impairment and cortical atrophy in 10 patients with ucPPA. *(+) met at least one core feature and sub-features in each PPA subtype. **(++) met at least two core features in each PPA subtype. ucPPA, unclassified primary progressive aphasia; AQ, aphasia quotient.
Clinical, language, and neuroimaging features according to Aβ positivity
There were no differences in the mean age, sex ratio, years of education, and CDR-SOB score between patients with A–PPA and A+ PPA. Patients with A+ PPA had a lower mean MMSE score (p =0.039) compared to patients with A–PPA (Table 2). Regarding APOE genotype, there were no differences in the frequency of APOE4 carrier between A+ and A–PPA across four subtypes. In terms of language impairment, patients with A+ PPA had a lower mean repetition score (57.5±29.1) than those with A–PPA (69.6±28.4, p = 0.038) after adjusting for age, sex, and education (Table 2). However, there were no differences in other language features between the two groups.
Clinical and language features of study participants according to amyloid positivity
Values are presented as mean±standard deviation or number (percentage). p-value was calculated by independent t-test and chi-square test. **p-value was calculated by analysis of covariance after adjusting for age, sex, and education. #p-value was calculated by Fishers Exact test. aMMSE was collected from 102 (92.7%) of the 110 participants. bCDR-SOB was collected from 92 (86.0%) of the 107 participants. cAPOE genotyping was performed in 98 (89.1%) of the 110 participants. A+, amyloid positive; A–, amyloid negative; PPA, primary progressive aphasia; MMSE, Mini-Mental State Examination; CDR-SOB, Clinical Dementia Rating (sum of boxes); svPPA, semantic variant primary progressive aphasia; nfvPPA, non-fluent variant primary progressive aphasia; lvPPA, logopenic variant primary progressive aphasia; ucPPA, unclassified primary progressive aphasia; K-BNT, Korean version of Boston naming test.
Figure 3 shows the topography of cortical atrophy in patients with A+ PPA. Compared to patients with A–PPA, those with A+ PPA exhibited cortical atrophy in the left inferior parietal, superior temporal, and posterior cingulate regions.

Cortical thickness in patients with A–and A+ PPA. The figure shows voxel wise contrasts between patients with A–and A+ PPA, and uncorrected p-value of 0.01 was considered as significant. A–, amyloid negative; A+, amyloid positive; PPA, primary progressive aphasia.
Neuroimaging features of patients with typical discordant PPA
Figure 4 shows cortical atrophy patterns in patients with discordant PPA. Patients with A–lvPPA had dominant frontal atrophy, and those with A+ nfvPPA and A+ svPPA had diffuse atrophy.

Brain MRI findings in discordant cases (A–lvPPA, A+ svPPA, and A+ nfvPPA). A–, amyloid negative; A+, amyloid positive; svPPA, semantic variant primary progressive aphasia; nfvPPA, non-fluent variant primary progressive aphasia; lvPPA, logopenic variant primary progressive aphasia.
Application of the AT system in patients with PPA
Thirty-seven patients with PPA were classified as follows: 19 (51.4%) A–T–PPA, 1 (2.7%) A+ T–PPA, 4 (10.8%) A–T+ PPA, and 13 (35.1%) A+ T+ PPA. The frequency of tau positivity was 92.9% (13/14) in A+ PPA subgroup and 12.5% (4/23) in A–PPA subgroup (Fig. 5). Among the four patients with A–T+ PPA, three patients were clinically diagnosed with svPPA. In addition, there were differences in the distribution pattern of AV-1451 uptake in svPPA and nfvPPA patients according to Aβ positivity (Fig. 6).

Application of the AT system in patients with PPA. Values depicted in the bar plot represent the number of PPA subtypes in each AT status. A–, amyloid negative; A+, amyloid positive; T–, tau negative; T+, tau positive; svPPA, semantic variant primary progressive aphasia; nfvPPA, non-fluent variant primary progressive aphasia; lvPPA, logopenic variant primary progressive aphasia; ucPPA, unclassified primary progressive aphasia.

The AV-1451 uptake patterns in patients with nfvPPA and svPPA according to amyloid positivity. A–, amyloid negative; A+, amyloid positive; svPPA, semantic variant primary progressive aphasia; nfvPPA, non-fluent variant primary progressive aphasia.
DISCUSSION
In this study, we evaluated the AD biomarkers in a relatively large cohort of Korean patients with carefully phenotypes PPA. Our major findings were as follows. First, Aβ positivity was highest in the lvPPA (81.3%) subtype, followed by ucPPA (60.0%), nfvPPA (18.5%), and svPPA (9.8%) subtypes. Second, compared to patients with A–PPA, patients with A+ PPA manifested cortical atrophy mainly in the left superior temporal and inferior parietal regions and had lower repetition scores. Further, more than 90% (13/14) of patients with A+ PPA showed tau positivity. Taken together, our findings will help clinicians to better understand the influence of AD biomarkers on clinical characteristics and neuroimaging findings in individuals with PPA. Moreover, it might prompt researchers to include patients with A+ PPA in clinical trials involving AD therapeutic agents.
Our first major finding was that Aβ positivity was the highest in lvPPA (81.3%), followed by ucPPA (60.0%), nfvPPA (18.5%), and svPPA (9.8%). Our findings were generally consistent with recent in vivo biomarker studies, which showed that the range of Aβ positivity in patients with lvPPA was 86–96%, with nfvPPA was 0–25%, and with svPPA was 11–21% [7, 21]. Notably, 60% of our patients with ucPPA showed Aβ positivity on PET. However, the frequency of Aβ positivity in ucPPA varied among studies (19%-75%) [2, 22]. These discrepancies might be due to the fact that different criteria of ucPPA were used. In fact, our findings were supported by two other previous studies that used the same criteria, where they showed that ucPPA patients (mixed type) were more likely to have Aβ positivity (60% and 75%) [2, 7]. However, in the previous study showing that the frequency of A+ in ucPPA was 19%, they diagnosed patients with ucPPA when they showed isolated single language impairments, such as anomia or dyslexia (incomplete type) or multiple PPA subtypes (mixed type) [1]. In that study, the frequency of ucPPA with incomplete type (n = 10, 62.5%) was higher than that of ucPPA with mixed type (n = 6, 37.5%). Further studies with larger samples will be needed to investigate the frequency of Aβ positivity within the ucPPA subtypes. To the best of our knowledge, a few previous studies have explored the differences in clinical and imaging characteristics between patients with A+ and A–ucPPA. In the present study, all patients with A+ ucPPA showed mixed clinical features of lvPPA and svPPA. These findings could be linked to the cortical atrophy pattern that patients with A+ ucPPA showed mainly left temporoparietal atrophy, different from typical atrophy patterns observed in svPPA and lvPPA. However, three out of four patients with A–ucPPA manifested mixed clinical features of nfvPPA and svPPA. These findings are also in line with the cortical atrophy pattern that patients with A–ucPPA showed mainly left frontotemporal or frontal atrophy. Therefore, our findings suggest that patients with ucPPA, especially those with logopenic features or parietal atrophy, are prone to present Aβ positivity on PET. This finding is supported by previous studies showing that the impaired speech repetition is associated with Aβ deposition in ucPPA [7] while the presence of agrammatism, which is one of the symptoms related to frontal dysfunction, makes Aβ pathology unlikely [2].
Our second major finding was that compared to A–PPA, the A+ PPA subgroup manifested lower repetition scores. Our findings might be related to a high proportion of A+ in lvPPA (81.3%) and ucPPA (60%) showing impaired repetition. Patients with A+ PPA showed cortical atrophy mainly in the left superior temporal and inferior parietal regions. These areas of the brain are involved in regulating speech repetition [23, 24]. Thus, our language assessment outcomes and imaging findings corroborate with each other. Specifically, these regions are the posterior components of the language network. The left inferior parietal and superior temporal cortices are implicated in phonological processing and repetition, respectively [25–27]. Further studies are needed to investigate the pathobiology of selective vulnerability in these regions in patients with A+ PPA.
In the present study, the presence of APOE4 carrier was not found to be associated with Aβ positivity in patients with PPA across four subtypes, although it is a well-known risk factor for Aβ deposition in the Alzheimer’s continuum [28, 29]. The correlation between APOE4 carrier and Aβ deposition in PPA remains controversial. Two previous studies showed that APOE4 carrier is a risk factor for Aβ positivity in svPPA [7, 30] and nfvPPA subtypes [7] whereas it is not related to Aβ positivity in lvPPA subtype [7, 30]. Our finding was comparable with the results of other studies showing that APOE4 carrier is not associated with Aβ positivity in any of the PPA subtypes [2, 31].
Our final major finding, which is noteworthy, was that more than 90% (13/14) of patients with A+ PPA had AD-specific tau positivity. Aβ positivity is observed in various types of dementia other than AD. It has been controversial whether in vivo A+ in other dementias reflects a primary diagnosis of AD or it is just an incidental finding. Previous studies showed that the frequency of tau positivity is 93% in A+ AD, 64% in A+ MCI, and 36% in A+ NC participants [32]. However, A+ other clinically diagnosed dementias showed low tau positivity: 26% in A+ dementia with Lewy bodies and 32% in A+ subcortical vascular dementia, suggesting that most of the A+ other clinically diagnosed dementias do not represent the primary diagnosis of AD [9, 33]. However, there is a paucity of information regarding tau positivity in patients with A+ PPA. Given that Braak stage III/IV might be important for the primary diagnosis of AD [32, 34], our findings suggest that A+ PPA might be an indicator of the primary diagnosis of AD. Furthermore, there were differences in the distribution pattern of AV-1451 uptake between A+ PPA and A–PPA patients. Specifically, most A+ PPA patients showed increased AV-1451 uptake in AD signature pattern but A–PPA patients showed increased AV-1451 uptake in regions where they showed cortical atrophy. We think that increased AV-1451 uptake in A–PPA patients might be related to increased neuroinflammation through MAO-A activity. The important role of AD biomarkers underlying language disturbances in PPA emphasizes the need for molecular imaging with the expectation that future treatment may target the disease-specific protein.
In the present study, the frequency of Aβ positivity in patients with svPPA and nfvPPA was similar to that in cognitively healthy persons, suggesting that in vivo Aβ positivity in patients with svPPA and nfvPPA might be an incidental finding. However, since most of them showed tau positivity also, Aβ positivity in svPPA and nfvPPA might be an indicator of atypical clinical features of AD rather than an incidental finding. Further pathological studies are needed to confirm our findings. Four out of 37 patients with PPA were A–T+, which included three patients with svPPA and one with nfvPPA. All patients with A–T+PPA underwent 18F-AV-1451 PET, and the characteristics of 18F-AV-1451 ligand might have contributed to this uncommon group of patients with A–T+. One possible explanation is the monoamine oxidase A (MAO-A) cross-reactivity of the 18F-AV-1451 ligand, which is known to bind to reactive astrocytes (mainly MAO-A) [35, 36]. Another mechanism might be that 18F-AV-1451 could weakly bind to the straight tau, which is commonly found in frontotemporal lobar degeneration tauopathies [37] as well as TDP-43 [38], although it has been widely used for the detection of AD-specific paired helical filament tau.
The biggest strength of this study patients with the standardized phenotyping of PPA is the large number of patients with the standardized phenotyping of PPA who underwent noninvasive Aβ imaging. However, our study had some limitations. First, although pathology data from post-mortem brain autopsy is considered as the gold standard for detecting Aβ in the brain, we used the Aβ-PET data interpreted by visual assessment. However, this limitation could be mitigated to some degree by a previous study showing that the results of Aβ-PET corroborate with autopsy findings [39]. In addition, visual assessment was highly concordant with Aβ positivity assessed using SUVR cut-off categorization [40, 41]. Second, other pathologies such as argyrophilic grain disease, Lewy body disease, hippocampal sclerosis, and incidental TDP-43 proteinopathy were not considered because we performed a pathologic study in only a small number of patients with PPA. Third, because of the cross-sectional study design, we could not investigate the different patterns of progression in language impairment and cortical atrophy between patients with A–and A+ PPA. Further longitudinal studies are necessary to identify the prognosis of A+ and A–PPA. Finally, the number of patients who underwent 18F-AV-1451 PET were only around a third. Further studies with larger samples will be needed to replicate our findings, that Aβ positivity in PPA might be an indicator of atypical clinical features of AD rather than just an incidental finding. Nevertheless, our study is noteworthy to report because it is relatively larger than previous studies and is based on Korean PPA patients who have a different language and culture from English-speaking PPA patients. Additionally, we found that the unclassified PPA patients with a mixed type showed a higher frequency of Aβ+. Furthermore, unlike previous studies, we applied an amyloid and tau classification system to categorize around a third of the PPA patients.
CONCLUSION
In this study, the frequency of AT biomarker positivity differs across the PPA subtypes, and AT biomarkers are associated with distinct language profiles in patients with PPA. Moreover, since most of the patients with Aβ+ PPA are also positive for tau, understanding the influence of AD biomarkers on PPA might provide an opportunity for these patients to participate in clinical trials aimed towards the treatment of atypical forms of AD.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Younghoon Seo (Samsung Medical Center) for English language editing.
This study was supported by the Fourth Stage of Brain Korea 21 Project in Division of Intelligent Precision Healthcare, a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare and Ministry of science and ICT, Republic of Korea (grant number : HU20C0111), and a fund(2021-ER1006-00) by Research of Korea Disease Control and Prevention Agency.