
Abstract
Background:
Many issues persist in the today’s Alzheimer’s disease (AD) screening and the breakthrough method is desired.
Objective:
We aim to validate the association between venous reflux and AD, and to develop a new method for AD screening.
Methods:
We examined spontaneous echo contrast, area, diameter, retrograde velocity, and anterograde velocity of the bilateral cervical internal jugular vein (IJV) using carotid ultrasonography.
Results:
A total of 112 patients participated in this study, with 26 diagnosed as AD. The proportion of both or either IJV spontaneous echo contrast (+) occupied 25 of total 26 AD patients, which showed 96.2%of sensitivity and 98.5%negative predictive value. The IJV velocities also showed significant correlation with AD diagnosis, although the IJV area or diameter did not.
Conclusion:
Our results indicate that the validation of the spontaneous echo contrast or velocities of the IJV are convenient AD diagnosis screening methods and that the venous reflux disturbance correlates with AD development.
INTRODUCTION
Dementia is a very significant issue in world health [1, 2], and Alzheimer’s disease (AD) occupies more than 50%of all dementia diagnoses in aged developed countries [3]. Thus, screening methods for the early detection of AD is important because appropriate treatment improves AD prognosis [4–6] and early intervention to lifestyle is important to address AD progression [7, 8]. However, usually, the diagnosis of AD is based on clinical criteria. Several biomarkers or imaging tools have been proposed for an early and objective diagnosis of AD [9]. However, many issues persist in the use of biomarkers for an objective AD diagnosis.
Confounding the identification of biomarkers for early AD diagnosis is the fact that the pathology of AD is not yet completely clarified. Many previous reports showed amyloid-c (Aβ) metabolism correlated with AD pathology [10], and the synthetic generation, cleavage, and clearance of Aβ is considered an important mechanism [11, 12].
The association between cerebrovascular and AD pathology in the perivascular fluid compartment is considered important in AD pathology [13–15]. Transcranial color-coded sonography (TCCS) permits non-invasive validation of intracranial arterial velocities [16], and several studies using TCCS have demonstrated that hemodynamic deterioration occurs in AD patients and in aged adults [17]. According to the Aβ clearance, vasomotion of the cerebrovascular smooth muscle cells is considered as the main driver of the intramural parietal drainage [18, 19]. For the brain drainage maintenance, arterial driver and venous drainer are closely related to each other [11]. Adding to the vasomotion of the cerebrovascular smooth muscle cells, multiple factors may concern with the brain intramural periarterial drainage [20]. Some previous studies showed the close relationship between arterial driver and venous drainer systems. Chronic ischemia of the brain white matter can result in demyelination and axonal loss, manifesting as white matter hyperintensities (WMHs) or leukoaraiosis [21, 22]. Increased WMH volume is associated with elevated AD risk [23, 24], and perivascular venous collagenosis has been linked to WMHs [25]. An expansion of the intracranial vein diameter is also associated with WMH volume [26]. These reports suggest that venous system change is associated with AD development involving with arterial driver system. However, the association between venous reflux and AD lacked data because direct intracranial venous reflux validation is challenging.
We hypothesize that venous reflux may be important in AD development due to the importance of venous function, especially in brain clearance. Although detecting intracranial venous flow directly is difficult, we found that the validation of internal jugular vein (IJV) velocities using carotid ultrasonography is simple, fast, and can be performed non-invasively at the bedside. Previous reports have correlated IJV hemodynamics to middle cerebral vein velocity [27, 28], which suggests that IJV hemodynamics may indicate, indirectly, intracranial venous hemodynamics. The aim of this study was to develop a new clinical method for early diagnosis of AD.
METHODS
Subjects and study design
This study was conducted as a single center study from June 1, 2017 to July 31, 2019. One hundred-twelve patients with any neurological disorder who were admitted to our department were prospectively enrolled. These patients may have various other diseases, as well as dementia. Progressed dementia or relentless neurological disease patients also participated, but severe acute stroke patients were excluded in this study. Severe acute stroke was defined as admission within 7 days after stroke onset and a National Institutes of Health Stroke Scale at admission of ≥20.
For all enrolled patients, we recorded age, gender, disease causing admission, AD diagnosis, cognitive function tests [Mini-Mental State Examination (MMSE), Hasegawa Dementia Rating Scale-Revised (HDS-R), and Frontal Assessment Battery (FAB)], atrial fibrillation (AF), Fazekas scale, and IJV parameters. The diagnosis of AD was according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) or the International Classification of Diseases, Eleventh Revision (ICD-11) by two neurologists with > 10 years of experience and who were blinded to the jugular vein information. We also diagnosed the vascular dementia (VaD) based on the National Institute of Neurological Disorders and Stroke-Association Internationale pour la Recherché et I’Enseignement en Neurosciences diagnostic criteria [29], the dementia with Lewy bodies (DLB) based on the fourth consensus report of the DLB Consortium revised diagnosis criteria “probable” [30], and the idiopathic normal pressure hydrocephalus (iNPH) based on the Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition) diagnosis criteria “probable” [31].
The Fazekas scale assessed perivascular hyperintensity grading and deep and subcortical white matter hyperintensity grading using magnetic resonance image (MRI) fluid attenuated inversion recovery (FLAIR) sequence [32] and was conducted by two neurologists with > 5 years of experience, who were blinded to the jugular vein information. The proportion of the antiplatelet or anticoagulant drugs using was calculated.
We divided AD diagnosed patients into two subgroups depending the MMSE score: MMSE < 10 group (low MMSE group) and the baseline MMSE≥10 group (high MMSE group) for the analysis based on the AD severity.
The ethics committee of our university approved this study, and the committee obtained exemption from approval from the institutional review board based on our guidelines (approval #Rin-Dai 20-054). All participants provided informed consent to participate in this study.
Internal jugular vein validation
We validated the IJV using carotid duplex ultrasonography (Fig. 1). We evaluated several parameters of bilateral cervical IJV, including spontaneous echo contrast (+ or –, with - indicating no contrast in bilateral IJVs), cross-sectional area (cm2, in the largest viewing location), diameter (mm, in the longest viewing location), retrograde velocity (cm/s, to brain), and anterograde velocity (cm/s, to heart) while the participant lay supine on a bed. From the above parameters, we calculated the average values of bilateral cross-sectional area (cm2), diameter (mm), retrograde velocity (cm/s), and anterograde velocity (cm/s) of the jugular vein. All participants were examined by using the ProSound Alpha 7 unit (Hitachi, Ltd., Tokyo, Japan) with a linear probe. One author, certified by the Japanese Association of Neurosonology, examined all IJV parameters.
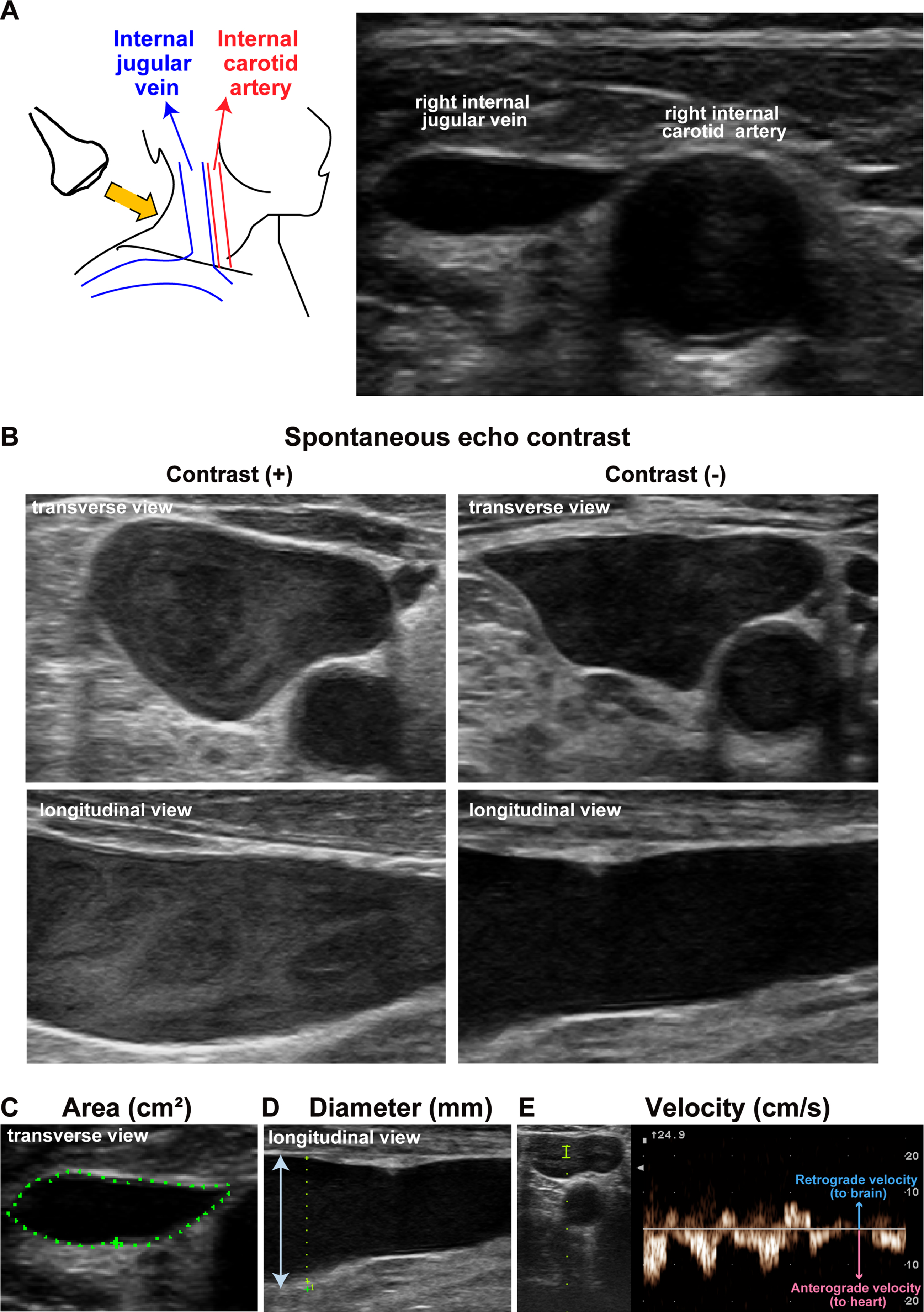
Internal jugular vein validation with carotid duplex ultrasonography. A) Schema of examination (left panel). Actual image (right panel). B) Spontaneous echo contrast images showing (+) are left side panels and (–) are right side panels. C-E) Each internal jugular vein parameter.
Outcome definition
The primary outcome in this study is the correlation between spontaneous echo contrast of the IJV and AD diagnosis. Secondary outcomes are the correlation between spontaneous echo contrast and cognitive function, Fazekas scale, or AF, and the correlation between cross-sectional area (cm2), diameter (mm), or velocity (cm/s) of the IJV and AD diagnosis, cognitive function, Fazekas scale, or AF.
Analysis of data
All statistical analyses were performed using JMP 15 statistical software (SAS Institute Inc., Cary, NC). The data are expressed as median±inter quartile range (IQR) and were analyzed using the chi-square test, nonparametric Wilcoxon’s rank sum test, or the Spearman’s rank correlation coefficient. Data with p < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
Patient characteristics are shown in Table 1. A total of 112 patients were included in this study. Seventy patients (67.0%) admitted to the hospital due to the cerebrovascular disease and the remaining 42 patients (37.5%) due to the non-cerebrovascular disease. Cranial MRI performance rate reached 97.3%(three patients could not undergo MRI because of contraindications; two due to permanent pacemakers and one due to claustrophobia). The proportion of the antiplatelet drugs using was 43.8%and that of the anticoagulant drugs using was 30.4%. Twenty-six patients (23.2%) were diagnosed as AD and a total of 22 patients (19.6%) had AF. We divided the 26 AD patients into 2 subgroups based on the MMSE score to low MMSE group (n = 14) and high MMSE group (n = 12).
Patient characteristics
MRI, magnetic resonance image.
Correlation between spontaneous echo contrast and AD diagnosis
The results of the correlation between spontaneous echo contrast of the IJV and AD diagnosis is shown in Table 2. The proportion of both or either IJV spontaneous echo contrast (+) was 25 (96.2%) of the 26 AD patients. Negative predictive value of the IJV spontaneous echo contrast to AD was 98.5%, while positive predictive value was 53.2%.
Correlation between spontaneous echo contrast and AD diagnosis
AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination. anonparametric Wilcoxon’s rank sum test was performed. bchi-square test was performed. **p < 0.01, ***p < 0.001.
According to the AD severity subgroups, there was no significant difference to the spontaneous echo contrast proportion between high MMSE group and low MMSE group.
Correlation between spontaneous echo contrast and cognitive function, Fazekas scale, AF, and antiplatelet/anticoagulant drugs
The results of the correlation between spontaneous echo contrast of the IJV and the cognitive function, Fazekas scale, and AF is shown in Table 3. All of the cognitive function scales, MMSE, HDS-R, and FAB, are significantly lower in the IJV spontaneous echo contrast (+) group than the (–) group (***p < 0.001, ***p < 0.001, **p < 0.01, respectively). The Fazekas scales, both periventricular hyperintensity (PVH) and deep and subcortical white matter hyperintensity (DSWMH), are significantly higher in the spontaneous echo contrast (+) group than the (–) group (***p < 0.001, ***p < 0.001, respectively). The proportion of AF was also significantly higher in the spontaneous echo contrast (+) group than the (–) group (*p < 0.05). All continuous AF patients (n = 7) demonstrated spontaneous echo contrast in the IJV. Although there was no significant difference between antiplatelet drugs using (+) and (–) groups, the proportion of spontaneous echo contrast (+) was significantly higher in the anticoagulant drugs using (+) group (*p < 0.05).
Correlation between spontaneous echo contrast and cognitive function, Fazekas scale, AF, and antiplatelet/anticoagulant drugs
AF, atrial fibrillation; CAF, continuous atrial fibrillation; DSWMH, deep and subcortical white matter hyper-intensity; FAB, Frontal Assessment Battery; HDS-R, Hasegawa Dementia Rating Scale-Revised; IQR, inter quartile range; MMSE, Mini-Mental State Examination; PAF, paroxysmal atrial fibrillation; PVH, periventricular hyper-intensity. anonparametric Wilcoxon’s rank sum test was performed. bchi-square test was performed. *p < 0.05, **p < 0.01, ***p < 0.001.
Correlation between internal jugular vein parameters and AD diagnosis, cognitive function, Fazekas scale, AF, and antiplatelet/ anticoagulant drugs
The results of the correlation between the average values of cross-sectional area (cm2), diameter (mm), and retrograde or anterograde velocity (cm/s) of the IJV and cognitive function or the Fazekas scale are shown in Supplementary Figures 1 and 2. The results of the correlation between each IJV parameter and AD or AF are shown in Table 4. Although MMSE, HDS-R, FAB, PVH, or DSWMH scores were not significantly correlated with the average values of cross-sectional area or diameter, they showed significant correlation with average retrograde or anterograde velocity. The average retrograde or anterograde velocity of the IJV showed positive correlations to cognitive function scores (Supplementary Figure 1). In contrast, the average retrograde or anterograde velocity of IJV showed negative correlations to Fazekas scales (Supplementary Figure 2). The average retrograde or anterograde velocity of the IJV was significantly lower in patients with AD diagnosis than without AD diagnosis (***p < 0.001 and ***p < 0.001, respectively), although there was no difference in the average cross-sectional area or diameter (Table 4).
Correlation between internal jugular vein parameters and AD diagnosis, Fazekas scale, AF, and antiplatelet/anticoagulant drugs
AF, atrial fibrillation; CAF, continuous atrial fibrillation; IQR, inter quartile range; MMSE, Mini-Mental State Examination; PAF, paroxysmal atrial fibrillation. All Area, Diameter, retrograde, and anterograde velocity parameters were calculated by average. Wilcoxon’s rank sum test was performed for all analyses. *p < 0.05, ***p < 0.001.
According to the AD severity subgroups, there was no significant difference to the average retrograde or anterograde velocity of the IJV between high MMSE group and low MMSE group. There was no significant difference to the IVJ parameters between antiplatelet drugs using (+) and (–) groups or between anticoagulant drugs using (+) and (–) groups.
DISCUSSION
Our results indicate that 1) spontaneous echo contrast and the velocity of the IJV significantly correlate with AD, although the cross-sectional area or diameter does not; 2) spontaneous echo contrast and the velocity significantly correlate with cognitive function and the Fazekas scale; and 3) spontaneous echo contrast significantly correlates with AF. These finding suggest that spontaneous echo contrast or low flow velocity of the IJV may be useful in screening AD diagnosis and that venous flow congestion from intracranial may be associated with AD pathology.
In regard to AD screening, several approaches have developed [7]. Cognitive screening instruments using pencil and paper include the MMSE and Montreal Cognitive Assessment (MoCA) and both popular screening tools and are considered gold standard methods for AD diagnosis screening. The MMSE had a sensitivity of 78%for AD, while the MoCA detects nearly 90–100%of AD [33, 34]. However, these two methods require significant time. Although the MoCA shows sufficiently high sensitivity, it requires > 15 min for a single examination [34]. In addition, 1 examiner performing many MoCA examinations in one day is a stressful and tough task. Since these instruments using pencil and paper are limited for large population screening, touch panel type methods using computers have developed for supplemental screening for AD diagnosis [35, 36]. These touch panel-type methods reduce the requirement for many examiners, but introduce other issues, such as using designated instruments (often expensive) for the examination. Our findings in this study alleviate all of the above issues because spontaneous echo contrast validation of the bilateral IJV is simple (less stressful for examiner), requires only a few minutes (fast), and requires only the common carotid ultrasonography. Because of high sensitivity (96.2%in our study), we suggest that spontaneous echo contrast validation of the bilateral IJV and following cognitive function tests such as MMSE or MoCA are the powerful method for AD screening of a large population. In addition, detecting pre-AD patients who will progress the AD in future, which cannot be achieved using cognitive functional scales, is a very important goal in the dementia treatment strategy [37, 38]. Our developed screening method may help detect the pre-AD patients, but this requires more study.
The AD patients in this study were clinically diagnosed because the aim of this study is to develop a new method for AD screening. For AD pathology analysis, the AD diagnosis should be based on the biomarkers Pittsburgh compound B positron emission tomography (PiB-PET) and cerebrospinal fluid (CSF) Aβ42 evaluation. Thus, we should recognize the limitation following discussion according to the association between venous reflux and AD, which is within the speculation. Regard to the development of AD pathology, the venous congestion and the low flow velocity significantly correlated with cognitive function, while the IJV cross-sectional area or diameter did not, which suggests that venous flow from the brain may be involved in AD pathophysiology. Several scientists have proposed the importance of clearance of drainage systems by cerebrovascular dynamics [11, 40]. Because the brain lacks a traditional lymphatic system for clearing products, it has been hypothesized that the cerebral vascular motion is involved with the perivascular fluid compartment [40]. This vascular motion has been revealed in some of the pathways, such as vessel caliber changes from both the cardiac cycle pulsations [41] and low frequency flow oscillations (LFOs) induced by the arterial wall smooth muscle [42]. Previous data suggests a decreased vascular elasticity may cause both diminished cardiac cycle induced vessel caliber changes and diminished LFOs, which results in a decrease in clearance [43–45]. Although cleavage and clearance of Aβ and related products under the healthy venous circumstance is considered to be important, especially in AD development [11, 12], the data of venous reflux in AD is absent. Although our results did not validate intracranial veins directly, IJV dynamics synchronize intracranial venous dynamics [28]. Our results reveal a relationship between venous reflux of congestive flow and AD, which suggests that venous flow disturbance may be associated with AD development.
Our results also show the importance of the relationship among venous reflux, WMHs, and AF. Our results indicate a significant relationship between the spontaneous echo contrast of the IJV and Fazekas scale and significant correlation between IJV velocities and Fazekas scale. These findings support the previous hypothesis of a relationship between venous reflux and white matter abnormalities related to AD development [46, 47]. In addition, the relationship between AF and cognitive function has been examined recently [48]. However, the mechanisms of AF-dependent decrease in cognitive function are not clear because previous meta-analysis showed that AF decreases the cognitive function independent of a history of the arterial stroke [49]. Actual brain intramural periarterial drainage system is considered as complex [44]. Vasomotion of the cerebrovascular smooth muscle failure triggers the intramural periarterial drainage system failure, which results in WMHs. Venous drainer system failure synchronously occurs and progresses with the arterial vasomotion failure, and these complex failures introduce the Aβ clearance decline [44]. Multiple factors such as AF influences this complex pathology. Our results finally showed that the proportion of spontaneous echo contrast (+) was significantly higher in the anticoagulant drugs using (+) group, although there was no significant difference between antiplatelet drugs using group. Anticoagulant therapy has potential to decrease the spontaneous echo contrast than anti-platelet therapy [50, 51]. We speculate the reason is due to the backgrounds of the anti-coagulant drugs users, which were AF and blood hypercoagulability status.
There are some limitations to our study. First, sample size was not large, as this was a pilot study. Second, there was no data from healthy persons and the control group consisted of the heterogeneous disease patients because all the participants in this study were hospitalized. Even the participants who were not AD had some diseases including VaD, DLB, and iNPH. Third, mild cognitive impairment status was not considered in this study although the correlation to the cognitive function was validated. We should recognize the proportion of participants having cerebrovascular disease was 62.5%in this study. An advanced study of a large sample size that includes healthy participants is needed for future research. Fourth, the AD patients in this study were diagnosed clinically but not pathologically. A total of 15%of patients with clinically diagnosed AD enrolled in the Alzheimer’s Disease Neuroimaging Initiative (ADNI) were reported amyloid negative by PiB-PET [52]. Pathological AD diagnosis participants were most desired for the validation of the AD diagnosis method accuracy. However, CSF Aβ42 evaluation by lumbar puncture or amyloid deposition evaluation by PiB-PET was difficult in this pilot study. The validation of the relationship between the IJV spontaneous echo contrast or velocity and pathological diagnosed AD participants is the next stage issue.
In conclusion, spontaneous echo contrast of the bilateral IJV may be a convenient AD diagnosis screening method.