
Abstract
Background:
Alterations in levels of peripheral insulin-like growth factor-1 (IGF-1) in Alzheimer’s disease (AD) have been reported in several studies, and results are inconsistent.
Objective:
We conducted a meta-analysis to investigate the relationship between peripheral and cerebrospinal fluid IGF-1 levels and AD or mild cognitive impairment (MCI).
Methods:
A systematic search in PubMed, Medline, Web of Science, Embase, and Cochrane Library was conducted and 18 studies were included.
Results:
Results of random-effects meta-analysis showed that there was no significant difference between AD patients and healthy control (17 studies; standard mean difference [SMD], –0.01; 95%CI, –0.35 to 0.32) and between MCI patients and healthy control (6 studies; SMD, –0.20; 95%CI, –0.52 to 0.13) in peripheral IGF-1 levels. Meta-regression analyses identified age difference might explain the heterogeneity (p = 0.017). However, peripheral IGF-1 levels were significantly decreased in AD subjects (9 studies; SMD, –0.44; 95%CI, –0.81 to –0.07) and MCI subjects exhibited a decreasing trend (4 studies; SMD, –0.31; 95%CI, –0.72 to 0.11) in studies with sample size≥80. Cerebrospinal fluid IGF-1 levels also significantly decreased in AD subjects (3 studies; SMD, –2.40; 95%CI, –4.36 to –0.43).
Conclusion:
These findings suggest that decreased peripheral and cerebrospinal fluid IGF-1 levels might be a potential marker for the cognitive decline and progression of AD.
INTRODUCTION
Alzheimer’s disease (AD), the most common neurodegenerative disease, is clinically characterized by memory loss and progressive cognitive impairment. The World Health Organization estimated that people living with AD or other types of dementia is approximately 36 million, and this population will reach 80 million by 2050 worldwide [1]. Increased age is the leading risk factor for AD; therefore, its prevalence is increasing with the global rise in average life expectancy. During the past two decades, numerous drug candidates targeting amyloid-β (Aβ) or tau, neuropathological hallmarks of AD, have not been successful in clinical trials [2], and there might be two explanations for these unsatisfying results. Firstly, most patients are already in the stage of dementia and have not been accurately and timely diagnosed at the early stage; Secondly, the pathological mechanisms of AD are complicated, not just Aβ and tau. Therefore, other factors and early diagnosis should be carefully considered [3].
Insulin-like growth factor 1 (IGF-1) is a peptide growth hormone (GH), which plays an essential role in the growth of the body and development of the brain [4]. IGF-1 levels are positively associated with working memory, executive function, and verbal performance [5]. Aging is the major risk factor for AD and multiple biological processes that change with aging [6], and studies have found that decline in IGF-1 levels is correlated with aging [7], which might contribute to decline of brain functions. IGF-1 confers important neuroprotective effects in AD by promoting neuronal survival, reducing tau phosphorylation, and enhancing Aβ clearance, indicating that IGF-1 might be a potential diagnosis and treatment target for AD [8]. IGF-1 levels have been reported to be altered in AD patients. Numerous studies have found that AD patients have lower peripheral or cerebrospinal fluid (CSF) IGF-1 levels than cognitively normal individuals [9–12]. However, other studies have reported contradictory findings [13–16].
Therefore, this meta-analysis aims to investigate whether AD or mild cognitive impairment (MCI) is associated with alterations of IGF-1 in the blood and CSF, so as to understand the potential role of IGF-1 in the progression and outcome of AD.
MATERIALS AND METHODS
The present systematic review has been conducted and authored according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline [17].
Search strategy
Two investigators independently performed a systematic review of English language literature from “PubMed”, “Medline”, “Web of Science” “Embase”and “Cochrane Library”databases. Search terms insulin-like growth factor-1 OR IGF-1 AND Alzheimer’s disease OR cognitive impairment OR dementia were used for each database. Databases were searched until July 29, 2020.
Inclusion and exclusion criteria
The inclusion criteria of this study were original studies that reported data on blood or CSF IGF-1 concentrations in at least two groups of subjects [AD, MCI and healthy control (HC)]. The exclusion criteria included the following: 1) No relevant data on IGF-1 concentrations; 2) only one group of subjects was reported; 3) the same cohort of subjects was reported repeatedly; 4) the study types were non-human studies, case reports, commentaries, reviews, meta-analyses, conference abstracts, or unrelated topics.
Data extraction
Sample size, average age of each group, gender distribution of each group, dementia severity (Mini-Mental State Examination, MMSE), sampling type (serum, plasma, CSF), patient medication and detection technology (ELISA, enzyme-linked immunosorbent assay; RIA, radioimmunoassay; IRM, immunochemical assays), region, IGF-1 concentrations, standard deviation (SD) and p value were extracted from the included studies. And the data extraction was performed by two investigators independently in case of incorrection or data missing.
Statistical analysis
The primary meta-analysis, subgroup and sensitivity analyses were performed using Review Manager Ver. 5.3 (Cochrane Collaboration, Oxford, UK). All continuous primary and secondary outcomes were compared between AD/MCI and HC using standardized mean difference (SMD). SMD and two-sided 95%confidence intervals (CIs) were used as the summary statistic for the meta-analysis. SMD is the mean difference in the outcome between cases and controls divided by the pooled SD, which gives the result of a unit free effect size. Random-effects models were chosen for the meta-analysis. The heterogeneity among original studies and subgroups was evaluated using the chi-squared test and the I2 statistic.
Meta-regression was also conducted using Stata 12.0 to explore the influence of covariates, including sample size, age difference, male ratio, region, and detection technology [18]. To assess the relative influence on the heterogeneity of each study, sensitivity analyses were conducted per subgroup following the exclusion criteria. Subgroup analyses based on sample size (the total number of individuals in a study; < 80 or≥80), age difference (≤1 year or > 1 year), sampling type (serum or plasma), detection technology (Elisa or RIA/IRM) and region (Europe, Japan, etc.) were performed respectively.
Publication bias was evaluated using a funnel plot and Begg-Kendall test with Review Manager Ver. 5.3 (Cochrane Collaboration, Oxford, UK) and Stata respectively. The significance level for all statistical tests was set at a two-sided p-value of less than 0.05.
Data availability
For purposes of replicating procedures and results, the data generated and analyzed in the current study can be made available on request.
RESULTS
Study selection and characteristics
The initial search generated 536 records from PubMed, 467 from Medline, 1,374 from Web of Science, 604 from Embase, and 78 from the Cochrane Library. After screening the titles and abstracts, 134 appropriate articles related to the present subject were selected for full-text assessment. Finally, we identified 24 studies using our inclusion and exclusion criteria, of which six studies that investigated IGF-1 and AD were not included (Supplementary Table 1). A flow diagram of the study selection is displayed in Fig. 1.

Flowchart of meta-analysis for AD. AD, Alzheimer’s disease; IGF-1, insulin-like growth factor-1.
Data from the 18 studies included in this meta-analysis were obtained either from the publication or were sent to us by the authors when necessary. Study characteristics for AD are described in Table 1. The total sample sizes ranged from 15 to 437. The average ages of each study ranged from 60.8 to 81.9 years for AD patients and 55.8 to 78.8 years for HC. Thirteen studies documented the gender information. Male ratio ranged from 30–76%for AD patients and 23.47–70%for HC. Fourteen studies (77.8%) reported serum IGF-1 levels and only four studies reported plasma IGF-1 levels. Nine studies (50%) used ELISA detection technology of blood samples and the other 50%used RIA or IRM. Three studies reported the CSF IGF-1 levels. Study characteristics for MCI are described in Supplementary Table 2.
General characters of including studies and participants
AD, Alzheimer’s disease; HC, healthy control; ELISA, enzyme-linked immunosorbent assay; RIA, radioimmunoassay; IRM, immunochemical assays; Tec., technique.
IGF-1 levels in AD and MCI patients
Serum IGF-1 values reported by Salehi et al. were much greater than those in other studies for AD subjects and were reported as outliers in a previous meta-analysis [19], and therefore, these data were excluded from the current meta-analysis. The remaining 17 studies with 2,264 subjects (1,119 AD patients and 1,145 HC) were further analyzed. The pooled SMD using a random-effects model was –0.01 ng/mL (95%CI: –0.35 to 0.32; I2 = 92%; p = 0.94), indicating that there was no significant difference between AD patients and HC in blood IGF-1 levels (Fig. 2A). Six studies with 965 subjects (437 HC and 528 MCI patients) were pooled for analysis of IGF-1 in MCI. Similarly, there was no difference between MCI patients and HC (SMD = –0.20, 95%CI: –0.52 to 0.13; I2 = 80%; p = 0.23) (Fig. 2B).

Forest plot of peripheral IGF-1 in AD and MCI in included studies. AD, Alzheimer’s disease; HC, healthy control; MCI, mild cognitive impairment; IGF-1, insulin-like growth factor-1.
Interestingly, we found that the total sample size was more than or less than 80, and the findings of these literature were inconsistent. Therefore, we conduct subgroup analysis based on sample size. When studies with a total sample size < 80 were excluded, the results showed significantly decreased peripheral IGF-1 levels in AD subjects (9 studies, SMD = –0.44, 95%CI: –0.81 to –0.07, I2 = 93%; p = 0.02) (Fig. 3A) and MCI subjects exhibited a decreasing trend compared with HC subjects (SMD = –0.31, 95%CI: –0.72 to 0.11; I2 = 87%; p = 0.15) (Fig. 3B). However, this was not found in studies with a total sample size of < 80 (Supplementary Figure 1).
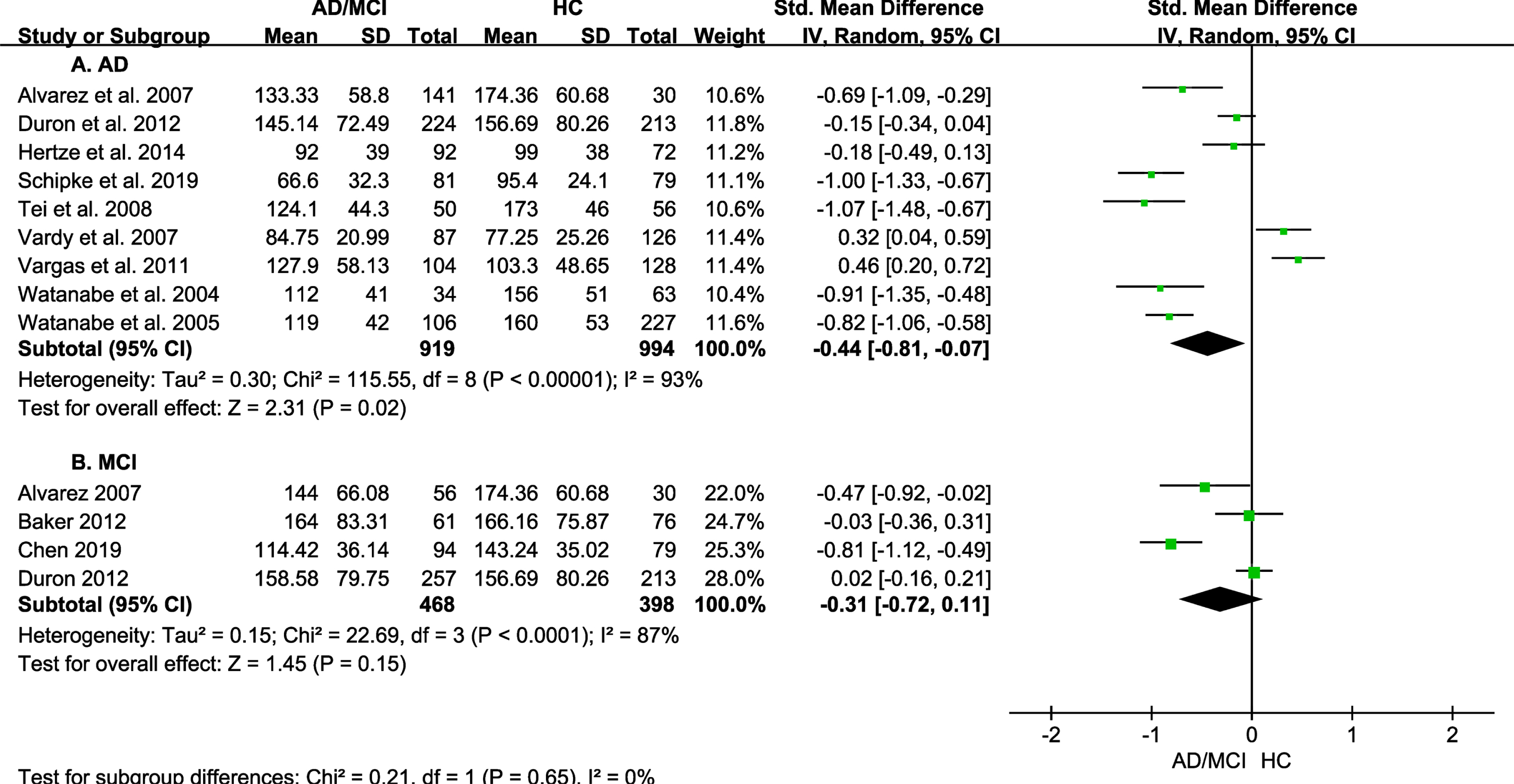
Forest plot of peripheral IGF-1 in AD and MCI with sample size of studies less than 80 were excluded. AD, Alzheimer’s disease; HC, healthy control; MCI, mild cognitive impairment; IGF-1, insulin-like growth factor-1.
Although there are only 3 studies on CSF IGF-1 levels in AD, we found CSF IGF-1 levels were significantly decreased in AD patients (SMD = –2.40, 95%CI: –4.36 to –0.43; I2 = 97%; p = 0.02) (Fig. 4).

Forest plot of CSF IGF-1 in AD. AD, Alzheimer’s disease; HC, healthy control; CSF, cerebrospinal fluid; IGF-1, insulin-like growth factor-1.
Sensitivity analysis
Sensitivity analysis results were shown in Supplementary Table 3. The fixed-effect model was used to estimate the stability of the results in AD patients and HC and showed that IGF–1 levels were significantly lower in AD patients than in the controls (SMD = –0.18, 95%CI: –0.27 to –0.09; p < 0.0001).
IGF-1 levels were lower in AD patients than in controls in studies with a mean age difference > 1 year (SMD = –0.66, 95%CI: –0.97 to –0.35; p < 0.0001). However, the results were contrary in studies with a mean age difference≤1 year (SMD = 0.54, 95%CI: 0.12 to 0.95; p = 0.01). When studies involving serum or plasma samples were included, the IGF-1 level was not statistically different between AD patients and HC (p = 0.72 and 0.41, respectively). Moreover, when studies related to the detection technology of RIA and IRM or ELISA were included, IGF-1 levels were not statistically significant in AD patients compared with HC (p = 0.26 and 0.29, respectively). No heterogeneity was found within Japanese studies, when comparing IGF-1 levels in AD patients and controls (I2 = 0, p = 0.58), and the IGF-1 levels in AD patients were lower than those in HC (SMD = –0.89; 95 %CI: –1.08 to –0.70; p < 0.00001). What is more, we did correlation analysis between the mean IGF-1 level and male ratio in AD and HC group respectively. Results showed that there were no gender specific differences in IGF-1 levels both in AD and HC groups (r = –0.159, p = 0.642 for AD group; r = –0.377, p = 0.253 for HC group).
Meta-regression analyses
A univariate meta-regression analysis was performed to explore the influence of sample size, age difference, region, and detection technology on the study effect size. The result revealed that only the age difference contributed to the heterogeneity (β coefficient = –0.102, p = 0.017). It was found that the higher the age difference in studies, the lower the SMDs of IGF-1 effects (Supplementary Figure 2). Furthermore, we did meta-regression analysis considering male ratio as covariate and coefficient of male ratio was not statistically significance (β coefficient = –0.051, p = 0.953), and there were no gender specific differences in IGF levels.
Publication bias
The Egger’s and Begg’s tests did not indicate evidence of publication bias (p = 0.35, p = 0.30, respectively). The funnel plot for the overall results also did not show any significant bias (Supplementary Figure 3).
DISCUSSION
In this meta-analysis, 21 studies were pooled for further analysis and found no significant difference between AD and HC and MCI and HC in peripheral IGF-1 levels. However, CSF IGF-1 levels were lower in AD subjects, even when only 3 studies were pooled. We found that the sample size of the included studies was more than 80 or less than 80, and the results were inconsistent, and a subgroup analysis was further conducted for a total sample size < 80 or≥80. The results showed that peripheral IGF-1 levels in AD and MCI were contrary in two subgroups. Peripheral IGF-1 levels were significantly lower in AD subjects and showed a decreasing trend in MCI subjects in studies with a total sample size≥80, but an increasing trend of peripheral IGF-1 levels in AD subjects in studies with a total sample size < 80. Meta-regression showed that age difference could account for the heterogeneity in the included studies. Age was related to the decline in the IGF-1 level have been reported previously. The meta-regression analysis also found that there was a negative correlation between age difference and the SMDs of IGF-1 effects. Considering peripheral IGF-1 levels significantly decreased in AD subjects, the SMD (IGF-1 in AD minus IGF-1 in HC) was frequently negative and smaller, and the age different would be significantly larger. In the study we analyzed, average age in HC group was smaller than AD group. In other words, in those studies with lower IGF-1 levels, the average age of AD patients was statistically higher than that of HC. This indicated that older patients with AD had lower IGF levels.
IGF-1 is an important part of the GH/IGF-1 axis, which plays a vital role in the development and function of the brain [20]. Aging is associated with a decline in IGF-1, which might contribute to cognitive decline [21]. The reduction of IGF-1 during aging might be a result of different epigenetic modifications [22]. Higher serum IGF-I levels were associated with slower cognitive decline in elderly patients [23]. In aging-related cognitive decline, these deficits can be reversed when IGF-1 is supplied [24]. Studies have found that serum IGF-1 levels in MCI or AD were downregulated, and lower peripheral IGF-1 levels were associated with higher risk of incidence of AD [12, 25–28]. In a familial AD study, plasma IGF-I level was significantly reduced in the members carrying the Swedish amyloid-β protein precursor (AβPP) 670/671 mutation with AD compared to age-matched controls, which suggest the importance of IGF-1 in the development of AD [26]. Trueba-Saiz et al. found that the CSF IGF-1 levels were significantly lower in AD patients than in healthy controls [16], which is consistent with the findings from our meta-analysis. And the brain expression of IGF-I and IGF-I signaling was decreased in advanced human AD were reported in postmortem studies [29]. After anti-AD drug treatment or intervention, the abnormalities of IGF-1 were also relieved with the improvement of symptoms and cognitive impairment [30]. Decreased levels of serum IGF-I combined with MMSE scores also have been demonstrated as an indicator to predict non-responders to donepezil among AD patients [31], supporting the potential of IGF-I as a disease biomarker in AD patients.
Several studies have given some mechanism explanations for the changes of IGF-1 in the occurrence and development of AD. Lower levels of IGF-1 relate to brain atrophy and globally less integrated brain functional network [32]. The entrance of peripheral IGF-I into the brain could promote the clearance of amyloid peptides known to accumulate in the AD brain and the decreased peripheral IGF-I might acerbate the progression of AD [16]. And early disruption of the entrance of peripheral IGF-1 into the brain could elicit AD-like pathology, cognitive impairment, and amyloidosis in healthy rodents [33]. IGF-1 could alleviate the expression of Aβ40 and key enzymes related to Aβ production (α-, β- and γ-secretases) in AD transgenic mice brain, and decrease the phosphorylation of AβPP and reduce the production of Aβ [34]. Moreover, overexpression of IGF-1 could protect hippocampal neurons from the toxicity of Aβ oligomers and prevents memory loss in AD mice [35], suggesting a therapeutic potential of IGF-1 in AD. Besides, IGF-1 could modulate phosphorylation of the tau protein, an early component in the development of AD. Exogenous administration of IGF-1 or upregulation expression of astrocytic IGF-1 could improve cognitive injuries and tau phosphorylation in animals [36]. IGF-1 also could maintain astrocytic function and coordinate hippocampal-dependent spatial learning through regulating astrocytic mitochondrial function and the redox status [37]. IGF-1, produced by microglia, have been reported to promote neuronal survival and axonal growth [38].
Although some included studies have found that IGF-1 levels were significantly increased in AD patients or peripheral IGF-1 was not an important determinant of AD risk [39]. Complicated mechanisms and several factors of AD may account for the inconsistent results. Firstly, we found that contrary or negative results were mainly from the studies with a small sample size (N < 80) [14, 40]; the low number of samples may influence the results and quality of studies and also amplify the effects of other influencing factors. Secondly, in AD patients, peripheral IGF 1 is negatively correlated with disease duration and decreases with age [41]. Some studies have postulated that the increase in IGF-1 levels may be a compensatory change in the early stages of AD, which can increase the clearance of Aβ or inhibit Aβ production through α-secretase and β-secretase [42]. IGF-I acts early in AD (reflected as increased IGF-1 level), followed by deficiency when the disease progresses (reflected as decreased IGF-1 level). What is more, apolipoprotein E (APOE) ɛ4 allele is the strongest genetic risk factor for AD. Although some studies have demonstrated that the APOE ɛ4 allele can increase IGF-1 levels [43], the available information of APOE alleles in these included studies are limited, making it difficult to analyze the impact of APOE on IGF-1 changes in AD. And the potential effect of APOE should been considered in future studies. What’s more, the effect of IGF-1 on glucose regulation should not been ignored. AD has even been considered to be “brain insulin resistance” or type III diabetes [44]. Insulin resistance is related to the abnormalities of energy metabolism in the brain of AD patients [45], which might cause a compensatory increase in IGF-1. Studies have demonstrated that peripheral IGF-1 levels are significantly increased in AD patients with type 2 diabetes (T2DM) compared with those without T2DM [46]. In addition to diabetes, other co-morbidities might also affect IGF-1 levels. Among the subjects enrolled in this study, there were 6 studies reported the existence of co-morbidities [10, 27], including hypertension, hyperlipidemia, etc. And these studies did not conduct further analysis. However, the co-morbidities of subjects are also a factor that needs to be carefully considered in future. Furthermore, IGF-1 was also affected by some drugs in AD patients. Donepezil, as a commonly used drug for AD, could reverse downregulation of IGF-1 in mice [47] and elderly males [48]. For some studies, IGF-1 in CSF have not been found to change in AD patients [11, 14], except for the factors mentioned above, and the remarkably lower level of IGF-1 in CSF than in peripheral may account for these negative results. And improved or novel detection methods will be essential to unravel the relationship between CSF IGF-1 and AD or cognitive decline.
Limitations
There are some limitations in this study. First, the number of included subjects and individual studies was relatively small compared with other meta-analyses. Second, marked heterogeneity was observed among the included studies, although the meta-regression showed that age difference could account for part of the heterogeneity. Third, APOE genotypes were not reported by most of the studies, hindering the exploration of the role of IGF-1 levels in different APOE genotypes.
CONCLUSIONS
This meta-analysis summarizes and analyzes the current research on changes in IGF-1 in peripheral and CSF in AD. Although we did not find a significant difference in peripheral IGF-1 between the AD and the control groups in the overall meta-analysis, peripheral IGF-1 was significantly reduced in AD patients and showed a decreasing trend in MCI patients in the analysis of studies with a sample size≥80. Furthermore, dysregulation of IGF-1 has been found in other types of dementia or diseases associated with cognitive impairment, such as vascular dementia [27], indicating that low IGF-1 levels are linked to impaired cognitive function. Therefore, IGF-1 could be a potential marker for the early diagnosis and outcome of AD and monitoring of drug efficacy in the future.
Footnotes
ACKNOWLEDGMENTS
This study was supported by National Natural Science Foundation of China (81801048); Beijing Hospitals Authority Youth Programme (QMS20200805); Beijing Municipal Natural Science Foundation (7184215); the Key Project of the National Natural Science Foundation of China (81530036); the National Key Scientific Instrument and Equipment Development Project (31627803); the Key Project of the National Natural Science Foundation of China (U20A20354); Beijing Scholars Program; Beijing Brain Initiative from Beijing Municipal Science & Technology Commission (Z201100005520016, Z201100005520017).