
Abstract
Background:
Serum levels of inflammatory factors, such as C3, C4, C-reactive protein (CRP), immunoglobulin (Ig) G, IgA, and IgM, in patients with Alzheimer’s disease (AD) and their correlation with cognitive function remain unexplored.
Objective:
To investigate the expression of serum inflammatory factors in patients with AD and its correlation with cognitive function.
Methods:
Serum levels of C3, C4, CRP, IgG, IgA, and IgM in 200 patients with AD (mild, moderate, and severe) and those in 174 normal controls were assessed. Spearman’s rank correlation analysis was used to explore the relationships among biomarker levels, cognitive function, and activities of daily living (ADL).
Results:
Among these inflammatory factors, C3 and CRP levels were significantly lower, and IgG and IgA levels were significantly higher in the AD group than in the control group (p < 0.05). There were no significant differences in C4 and IgM levels between the two groups (p > 0.05). In all participants, CRP level was positively correlated with the Mini-Mental State Examination and Montreal Cognitive Assessment scores (p < 0.05). In the AD group, IgA level was negatively associated with ADL scores (p < 0.05). No significant correlation was detected between the other factors and different cognitive scores (p > 0.05).
Conclusion:
Inflammatory factors C3, CRP, IgG, and IgA have the potential to serve as biomarkers for AD. Furthermore, serum IgA was not only correlated with AD but also with ADL. These results support the hypothesis that inflammation is involved in the occurrence and development of AD.
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative disease with a complex pathogenesis. Current evidence suggests that inflammation plays an important role in the pathogenesis of AD [1]. Imbalances in the complement system also lead to pathological progression of AD [2]. In 1999, Yasojima et al. found that the levels of complement proteins along with their corresponding mRNAs belonging to classical activation pathways in the brains of patients with AD were significantly increased. These included C1q, C1R, C1s, C2, C3, C4, C5, C6, C7, C8, and C9 [3]. At the same time, it was shown that there was also a complement replacement activation pathway in the brain of AD [4]. Rogers et al. proposed in 1992 that amyloid-β (Aβ) aggregation could activate the complement system [5]. In addition to amyloid plaques, aggregated tau proteins have also been shown to activate the complement system [6]. Furthermore, microglia that are present in the central nervous system cooperate with the complement system in synergistic fashion. The continuous activation of complement system can cause microglia to secrete harmful substances, induce inflammation, and aggravate tissue damage. Microglia acquire different phenotypes in response to the activated complement system. In AD, damaged complement signals lead to a decreased ability of microglia to remove harmful substances and increased secretion of inflammatory factors, resulting in a series of changes [7]. Some studies have shown that the increased expression of complement C3 and C4 could be detected around amyloid plaques, and the plaque density was positively correlated with the expression of C3 and C4 [8]. It is suggested that complement plays an important role in the early stage of AD. In an AD mouse model, C-reactive protein (CRP) levels were found to increase the production of Aβ42, thus promoting the occurrence and development of AD [9]. AD leads to changes in immune function in the central and peripheral nervous systems [10]. Several trials have explored new neuroinflammatory biomarkers; these have led to a significant progress in the diagnosis, treatment, and prognosis of AD. A previous study has found that the levels of various inflammatory biomarkers were changed significantly in patients with AD [11]; however, the results were contradictory, and the relationships of the biomarker levels with cognitive function and ability to perform activities of daily living (ADL) remain unclear. Furthermore, the sample size in related studies on Chinese population is small. Moreover, the scales used for cognitive evaluation in the majority of studies until now are relatively simple. In most studies, the cognitive function scales only include Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) scale, which cannot accurately reflect the level of each cognitive domain. Therefore, it is still unknown whether inflammatory markers can reflect the function of specific cognitive domains. In this study, we further expanded the sample size and used multiple scales to assess different cognitive functions. This could help us better understand how the levels of inflammatory markers change at different stages of the disease and how they relate to specific areas of cognitive function.
In this study, we aimed to measure serum C3, C4, CRP, immunoglobulin (Ig) G, IgA, and IgM levels and evaluate their correlation with different cognitive function to provide help for the discovery of new biomarkers.
MATERIALS AND METHODS
Participants
We planned a study of continuous response variable. Based on previous study, we used power analysis to calculate the sample size. When the power is 0.8, we need to study 180 experimental subjects to be able to reject the null hypothesis that the population means of the experimental and control groups and equal with probability (power).
In our study, the participants were divided into two groups: the AD group and the normal control group. A total of 200 patients (75 males, 125 females, aged 45 to 78 years) with AD being treated in the department of neurology of Xuanwu Hospital in China were recruited from September 2019 to November 2020. Written informed consent was obtained from all respondents. The diagnosis of AD was based on the National Institute of Aging and the Alzheimer’s Association (NIA-AA) [12]. There were 65 male and 109 female patients in the control group, aged 43 to 79 years. The patients with AD group were divided into mild, moderate, and severe AD according to the clinical dementia rating (CDR) scale (mild: CDR = 1, moderate: CDR = 2, and severe: CDR = 3). The exclusion criteria for all subjects included who had severe heart, liver, kidney, and other medical diseases, mental illness, thyroid disease; recent history of infection and tissue damage; chronic inflammatory diseases (asthma and rheumatoid arthritis); recent (within 3 months) administration of statins, non-steroidal anti-inflammatory drugs, or anti-infective drugs.
Neuropsychological testing
Neuropsychological testing of the participants was conducted by clinical professionals. The rating scale for cognitive function included MMSE, MoCA scale, and the CDR scale. The auditory verbal learning test (AVLT), Boston naming Test (BNT), and clock drawing test (CDT) were used to detect the different cognitive domains among AD patients. ADL scale was used to measure the participants’ abilities to conduct the tasks involved in daily living; the higher was the ADL scores, the worse was the ability to conduct said tasks.
Assays
Non-fasting blood samples were collected with 5 mL serum-separating vacutainer tubes and centrifuged at 1300×g for 10 min. Serum inflammatory factors were measured using immune turbidimetry. The IMMAGE800 automatic specific protein meter (Beckman Coulter, Inc., Brea, CA, USA) was used for measuring the factors.
Statistical analysis
Data are reported as mean±SD. An independent sample t-test (between the two groups) or one-way ANOVA (among more than two groups) was used to analyze the normal distribution data. For skewness distribution data, Mann-Whitney U (to compare between the two groups) or Kruskal-Wallis tests (to compare among more than two groups) were used. Because the scale scores were non-normal distribution, the associations between continuous variables were tested using Spearman’s rank correlation analysis. Two-tailed p values < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS 25.0 statistical software system (IBM, Armonk, NY, USA).
RESULTS
Baseline characteristics of participants
The demographic characteristics of the participants enrolled in the study are shown in Table 1. There was no significant difference in age, sex, education level, and medical history between the AD group and the control group (p > 0.05). The MMSE and MoCA scores in the AD group were significantly lower than those in the control group (p < 0.001).
Baseline characteristics of participants
Data are shown as mean±SD. *p < 0.05, **p < 0.01, ***p < 0.001.
Serum C3, C4, CRP, IgG, IgA, and IgM levels in the AD group and control group
The serum C3, C4, CRP, IgG, IgA, and IgM levels in the AD group and control group are shown in Table 2. C3 and CRP levels in AD patients were significantly lower, and IgG and IgA levels in AD patients were significantly higher than those in the control group (p < 0.05). There were no significant differences in the C4 and IgM levels between the two groups (p > 0.05). Figure 1 shows the serum C3, CRP, IgG, and IgA levels in the AD and control group.
The serum inflammatory factors in AD group and control group
*p < 0.05, **p < 0.01, ***p < 0.001.
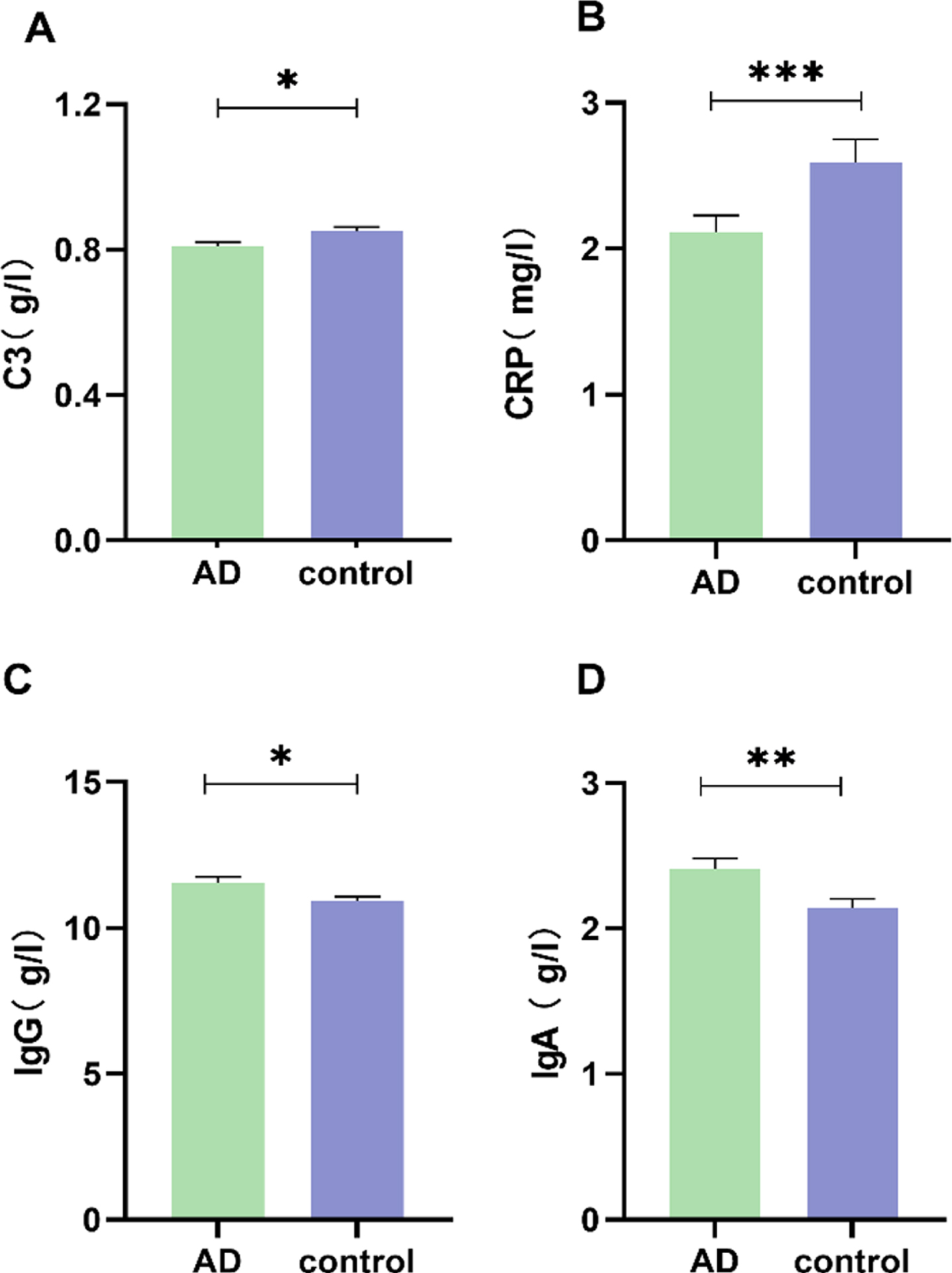
Analysis of AD serum inflammatory factors: C3, CRP, IgG, and IgA levels in healthy controls and AD patients (mean±SEM). *p < 0.05, **p < 0.01, ***p < 0.001.
Serum C3, C4, CRP, IgG, IgA, and IgM levels depending on the severity of AD (Table 3)
There was a significant difference in serum CRP and IgA levels among the AD groups of different severities (p < 0.05). After pairwise comparison, the CRP levels in patients with mild and moderate AD were significantly lower than those in controls (p < 0.05). Although the CRP level in patients with severe AD was lower than that in the control group, this difference was not statistically significant (p > 0.05). The IgA levels in patients with mild and severe AD were significantly higher than those in the controls (p < 0.05). No significant differences were found between patients with moderate AD and the control group regarding the serum IgA level (p > 0.05). Figure 2 shows the changes in serum CRP and IgA levels in different groups. No significant differences were found in C3, C4, IgG, IgM levels among the different severities of AD groups (p > 0.05).
The serum inflammatory factors in different severity of AD
Data are shown as mean±SD. *p < 0.05, **p < 0.01. #compared with control, p < 0.05.
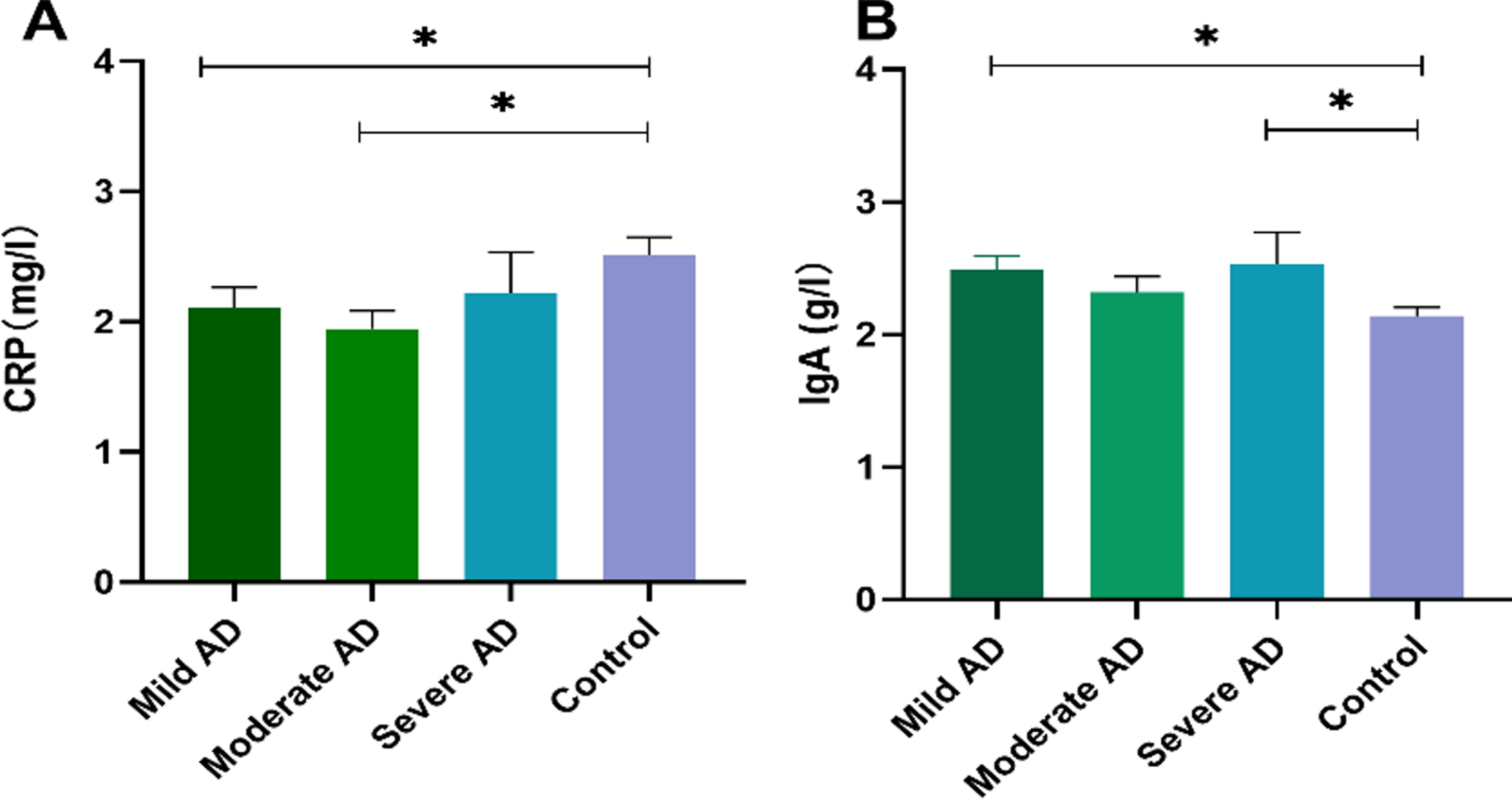
Differences in serum CRP and IgA levels in different dementia groups. A) Differences in serum CRP levels in different dementia groups. B) Differences in serum IgA levels among the different dementia groups (mean±SEM). *p < 0.05.
The correlation between inflammatory factors and cognitive function
Spearman’s correlation showed that in all participants, serum CRP level was positively correlated with the MMSE and MoCA scores (p < 0.05) (Table 4). The patients in the AD group were analyzed further and no significant correlation was detected between the serum inflammatory factors levels and the MMSE or MoCA scores (p > 0.05) (data not shown). Correlation analysis also showed a significant negative correlation between serum IgA level and ADL scores in the AD group (p < 0.05) (Table 5). No significant correlation was detected between the other factors and different cognitive scores (p > 0.05) (Table 5).
Correlation between serum inflammatory factors and MMSE and MOCA scores in all subjects
*p < 0.05, **p < 0.01, ***p < 0.001.
Correlation between serum inflammatory factors and cognitive scale scores in the AD group
The r value is shown in the table; *p < 0.05.
DISCUSSION
Our study evaluated the levels of serum inflammatory factors, namely C3, C4, CRP, IgG, IgA, and IgM in patients with AD. The association of inflammatory factors with the cognitive functions and ADL ability was also evaluated.
CRP is a protein that rises sharply in the acute phase of inflammatory reactions. At present, it is widely used as a non-specific inflammatory index in clinical settings. Increased CRP level is deemed a risk factor for cardio-cerebrovascular and other disorders. Several studies have suggested that increased CRP levels may promote the development of AD [13, 14]. Gabin et al. proposed that elevated serum CRP concentrations increased the risk of AD in people aged 60–70.5 years, while the opposite association was found in older people aged over 70.6 years [14].
Thus, the results of serum CRP levels in patients with AD are contradictory. Our study observed that serum CRP level was significantly lower in patients with AD but not in mild cognitive impairment (MCI). The serum CRP level changes dynamically in different stages of the disease [15]. The results of our study may raise the hypothesis that there may be an increase in serum CRP levels before or during the development of AD, but as the disease progresses, serum CRP levels may decrease after AD becomes clinically evident [14, 16]. In the clinical stages of AD, there may be a decrease in the inflammatory response [16]. If these findings are verified, they may provide references for future treatment. After the diagnosis of AD has been confirmed, the use of anti-inflammatory drugs may not have a strong effect. Past epidemiological studies have shown that anti-inflammatory drugs may reduce the risk of AD; however, some clinical trials have not shown that non-steroidal anti-inflammatory drugs could slow down AD progression. Once the obvious clinical symptoms of AD appear, the relevant medication is of little significance. Dynamic monitoring of serum CRP level is of great significance in predicting the progression of AD. At the same time, some other studies have obtained different results [11, 18]. For example, two previous studies have found that the levels of serum CRP in the AD group were significantly increased [11, 17]. In contrast, another study also found that there was no significant difference in serum CRP levels between the AD group and the control group [18]. This may have been due to the heterogeneity of the subjects included in different studies or inaccuracy of the diagnosis. Strict diagnostic parameters used to differentiate between AD and MCI in our study may provide further support for the possibility of CRP decrease in the late stage of AD. A meta-analysis found that serum CRP levels were significantly lower in patients with mild to moderate AD than in the control groups, but no significant difference was found between severe AD and the control groups [19], which was in agreement with the results of our study.
Our study also found that serum CRP levels were associated with MMSE and MoCA scores in all subjects, but there was no significant correlation for this trend in the AD group. In contrast, Nilsson et al. pointed out that serum CRP levels in patients with AD were significantly negatively correlated with MMSE scores and survival period [20]. Some studies have found that serum CRP levels were related to executive function [21, 22]. However, a longitudinal study in 2005 showed no significant correlation between serum CRP levels and different cognitive scores [23]. These results indicated that CRP had been involved in the function of brain structure related the cognition. The correlation between CRP level and cognitive function needs to be further verified.
C3 is the central component of the complement activation pathway. In our study, serum C3 level was significantly lower in the AD group than in the control group, but there was no significant correlation with different cognitive domain scores. The increase in serum C3 level is considered to be associated with a variety of diseases [24]. While the lack of C3 leads to the progression of AD, its presence seems to promote the clearance of Aβ plaque [25]. It is also speculated that there may be a decrease in C3 levels in patients with AD [24]. This hypothesis is consistent with the significant decrease of serum C3 in the AD group found in our study. Rasmussen et al. found that the lower was the level of C3 at the baseline, the higher was the risk of developing AD, and this effect was more pronounced in homozygous apolipoprotein E (APOE) ɛ4 carriers [26]. Uchida et al. concluded that the concentration of serum C3 was decreased significantly in patients with amnesia MCI (aMCI) and AD [27]. However, one study found that plasma C3 concentrations in AD patients were significantly lower than in those with MCI, but there was no significant difference compared with controls [28]. Thambisetty et al. found that the concentrations of plasma C3 were increased in patients with AD [29]. The use of different detection technology affects the results. Our results showed that the levels of serum CRP and C3 in the AD group were significantly lower than those in the control group. The combination of these results can help us to better understand the special manifestation of inflammatory response in AD. There may be an increase in inflammatory response before the occurrence of AD, but as the disease progresses and its presence is diagnosed, the inflammatory response may weaken. Inflammation status changes dynamically at different stages of the disease; therefore, it is of great significance to dynamically monitor the level of inflammation in the body.
Ig is a type of immunoreactive molecule with antibody activity or a chemical structure similar to that of the antibody. Our study found that serum IgG and IgA levels were significantly higher in the AD group, indicating considerable variations in immune function in AD patients, similar to the results of a previous study [30]. However, other studies have made different conclusions [31]. Studies addressing Ig levels are rare. Some studies have found that periodontal disease-related antibodies may be a risk factor for AD [32]. The receptor of advanced glycation products (RAGE) belongs to the Ig family. Wilson et al. found that the plasma concentrations of anti-RAGE and Aβ Ig in patients with AD were significantly higher, and that of IgG was gradually increased with the severity of dementia [33]. Our study found that serum IgA level in patients with mild and severe AD was significantly higher than that in the control group. No significant differences were found between patients with moderate AD and the control group with regard to the serum IgA level. The reason for that observation was not very clear. In the course of AD development, the body’s immune function changes dynamically. We found no significant difference in the pairwise comparison between AD subgroups of different dementia severity, but it cannot be excluded that the severity of dementia could affect Ig levels. In our study, a significant negative correlation was seen between serum IgA level and ADL scores. With the increase in serum IgA level, the ADL ability was improved. IgA seems to have a protective effect to some extent, and the application of some immunotherapies in AD has proved that Ig levels in vivo may play a beneficial role [34]. Dodel et al. found that the cognitive ability of AD patients was improved after the administration of anti-Aβ antibody [35]. These findings also have certain significance for guiding treatment. Improving the body’s immunity may help reduce the risk of AD. The decline of immune level can promote the occurrence and development of AD. Moreover, to our knowledge, the correlation between Ig levels and specific cognitive domains and ADL has not been uncovered. This new finding suggests that Ig may play a protective role, but more extensive research is needed.
A primary strength of our study is that it is a sizable representation of Chinese AD cases in comparison to those included in prior studies. Furthermore, we excluded the users of anti-inflammatory drugs, which makes the results more convincing, because the use of anti-inflammatory drugs can affect the level of peripheral inflammatory factors. In our study, 200 patients with AD and 174 controls were enrolled, and the variations in serum levels of inflammatory factors, as well as their correlation with different cognitive functions, were observed. The results can provide evidence to further explore new biomarkers. Despite these strengths, the potential limitation of our study is its cross-sectional design; moreover, cerebrospinal fluid biomarkers were not measured and imaging data were not available.
In summary, we observed that serum levels of C3 and CRP levels were significantly lower while serum levels of IgG and IgA were significantly higher in patients with AD than those in the controls. Inflammatory factors including C3, CRP, IgG, and IgA may be potential biomarkers of AD. In addition, serum IgA levels were not only correlated with AD but also with ADL. Obtained results support the hypothesis that inflammation is involved in the occurrence and development of AD. At the same time, our research results are also helpful to developing novel treatments for AD. Further studies with a larger sample size and longitudinal analysis of AD patients are warranted to explain the relationship between inflammatory biomarkers and cognitive functioning.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the Key Project of the National Natural Science Foundation of China (81530036); the National Key Scientific Instrument and Equipment Development Project (31627803); the Key Project of the National Natural Science Foundation of China (U20A20354); Beijing Scholars Program; Beijing Brain Initiative from Beijing Municipal Science & Technology Commission (Z201100005520016, Z201100005520017).