
Abstract
Background:
The Memory Alteration Test (M@T) is a verbal episodic and semantic memory screening test able to detect subjective cognitive decline (SCD) and Mild Cognitive Impairment (MCI).
Objective:
To adapt M@T, creating a Greek version of the Memory Alteration Test (M@T-GR), and to validate M@T-GR compared to the Mini-Mental State Examination (MMSE), and Subjective Cognitive Decline- Questionnaire (SCD-Q) MyCog and TheirCog.
Methods:
232 people over 55 years old participated in the study and they were classified as healthy controls (HC, n = 65), SCD (n = 78), or MCI (n = 89).
Results:
The ANCOVA showed that the M@T-GR’s total score was significantly different in HC and SCD (I-J = 2.26, p = 0.032), HC and MCI (I-J = 6.16, p < 0.0001), and SCD compared to MCI (I-J = 3.90, p < 0.0001). In particular, a cut-off score of 46.50 points had an 81%sensitivity and 61%specificity for discriminating HC from SCD (AUC = 0.76, p < 0.0001), while a cut-off score of 45.50 had a sensitivity of 92%and a specificity of 73%for discriminating MCI (AUC = 0.88, p < 0.0001), and a cut-off score of 45.50 points had a sensitivity of 63%and a specificity of 73%for discriminating SCD from those with MCI (AUC = 0.69, p < 0.0021). Exploratory factor analysis indicated that there was one factor explaining 38.46%of the total variance. Internal consistency was adequate (α= 0.75), while convergent validity was found between M@T-GR and MMSE (r = 0.37, p < 0.0001) and SCD-Q TheirCog (r = –0.32, p < 0.0001).
Conclusion:
The M@T-GR is a good to fair screening tool with adequate discriminant validity for administration in people with SCD and MCI in Greece.
Keywords
INTRODUCTION
In light of the projected rapid worldwide increase of people with Alzheimer’s disease (AD), there is a strong interest in detecting the early risk stages that may allow early intervention or the prevention of this public health problem which has high social and economic impact. On the other hand, mild cognitive impairment (MCI) is a clinical condition which can be recognized as a precursor of dementia and risk factor for AD [1–3], with a conversion rate to dementia of 4–25%per year [4–7], representing a transitional stage between normal cognition and mild AD [1, 7–10]. In Greece, the MCI incidence rate is approximately 54.07 new cases in 1,000 participants, while MCI is found to occur at a rate of 26.3%among older adults in Northern Greece [11].
The MCI patients present a high probability to evolve into AD in the immediate future [12], while another preclinical stage, the so-called subjective cognitive decline (SCD), is considered as a concept harbinger of future objective impairment [13–19]. A global effort to standardize the definition of SCD has already been launched [20, 21], but the development of a psychometric questionnaire or scale to identify, measure, and operationalize the construct of SCD has been proven to be elusive so far, as it is impeded by problems with internal consistency, test-retest reliability, and content validity [21]. Recent evidence suggest that the prevalence of SCD as investigated in 15 countries worldwide including 40,000 older adults was around 25%[22], while in Greece, it seems that among 1,500 older adults, the percentage that reported at least one complaint related to SCD was 76.6%[23]. In particular, the Subjective Cognitive Decline Initiative Working Group (SCD-I WG) suggests that in the SCD population, incidence of dementia was 17.7/1,000, while higher age, lower Mini-Mental State Examination (MMSE), and genetic predisposition increased the risk of developing dementia in SCD [24]. However, diagnosing preclinical stages of AD is a complex process while the performance on screening tests can be included on the disease-oriented diagnosis [25–27]. Currently, there are several diagnostic tools for assessing dementia [28, 29], but the sensitivity for the early detection of its preclinical stages such as SCD is very low [10, 31]. Nevertheless, lately some studies have investigated the potentiality of developing discriminating tests and have found high sensitivity and specificity for discriminating SCD from MCI [32], However, SCD is often unrecognized in primary care centers [24, 33–35], due in part to the lack of easy and useful cognitive screening tests for this stage of the disease, and the absence of consensus of using a standardized tool for discriminating SCD. A recent review of the SCD and broader cognitive aging has proposed heterogeneity in several aspects of cognitive self-report measures including number of questions [36–38], mode of administration [39, 40] and type of response [41, 42]. Therefore, the field currently lacks a single accepted neuropsychological instrument for the assessment of SCD, including the fundamental nature of the questions, cognitive domains of greatest interest, and optimal items for each domain [21]. With regards to the use of instruments, some studies use complete published questionnaires [43, 44], while others use groups of items from existing measures [45] or develop new items for a specific study [46–48]. Finally, while selecting appropriate measures stands among the most critical decisions made in clinical research contexts, the SCD literature, in many cases, does not thoroughly discuss selection decisions.
Thus, it seems crucial to develop a memory screening test capable of distinguishing MCI and SCD from HC, oriented to the healthcare professionals that allows them to differentiate the preclinical groups of AD and that is easily applicable in daily practice in primary care centers. The Memory Alternation Test (M@T) is an accurate screening test with high discriminative properties for amnestic MCI (aMCI) and mild AD dementia among the general primary care population [49]. Moreover, its constructors have used it also for categorizing older adults as SCD, MCI, and healthy participants [50–52] with high discriminative properties showing high diagnostic performance [49–51, 53–55]. M@T constitutes a brief and comprehensive screening test assessing several memory subtypes, and it arises as a promising alternative for the detection of early cognitive impairment [50]. It is based on the consolidation memory theory stating that episodic memory requires the medial temporal lobe (MTL) for consolidation, being afterwards stored in neo-cortical circuits as part of the semantic memory system [56], which is known to be affected at earliest stages of AD [57]. The neurodegenerative progression of aMCI and AD includes metabolic abnormalities in cortical brain regions. Comparatively with other screening tests (e.g., MMSE), the M@T is the only one that showed good discriminative properties for differentiating mild AD and SCD populations, while it has differentiated SCD from MCI with a sensitivity of 96%and a specificity of 70%in Portuguese older adult population [50]. Nevertheless, some recent studies have found sufficient discriminative ability of SCD and MCI using the Montreal Cognitive Assessment [58], but even it has not been decided up to now as a screening tool for SCD population. It has been found that the M@T scores of the aMCI cases who converted to AD were significantly lower than those who did not [50]. Therefore, lower M@T scores could indicate a more severe MCI status, and could imply closer follow-up of the aMCI group in order to detect AD conversion [54]. According to previous studies, the M@T is an accurate screening test that can measure early AD progression [49, 55] and its association with brain metabolism suggesting that performance in M@T was associated with in vivo changes over cortical brain regions in MCI population. However, while internal consistency is reported to be high [50, 51], the clinical utility needs more research. Another limitation of M@T is that it has been developed to screen MCI and typical AD; therefore, its discriminative properties have not been studied in atypical AD presentations or other dementias in which language or frontal dysfunctions can be the earliest manifestation.
Furthermore, the Subjective Cognitive Decline Questionnaire (SCD-Q) is a new questionnaire for quantifying SCD that has been proved useful for discriminating among all the groups with different degrees of cognitive impairment, from healthy controls to dementia [59]. The SCD-Q consists of a part I-MyCog, named MyCog, using the respective yes or no self-administered questions; and a part II-TheirCog, TheirCog, which includes the same questions, but the answers are provided by the informant or caregiver. MyCog has been found to be useful for quantifying self-cognitive decline in SCD with robust internal validity [59]. The SCD-Q has been found to be correlated to participants’ objective cognitive performance and has the ability to discriminate SCD and HC with sensitivity 85%and specificity 80%[59]. Longitudinal studies have found that informants’ reports were associated with worse performance on memory tests and hence an increased risk of cognitive impairment and progression to dementia, thus facilitating identification of very early neurodegenerative decline [20, 60–65]. In summary, the most important advantage provided by the SCD-Q is the possibility to quantify decline as reported by the participant and the informant at different degrees of cognitive impairment. Part I (MyCog) is useful to identify SCD groups and is also able to discriminate between individuals with SCD who had sought help at memory units and those who had not. Part II (TheirCog), the informant’s report, was associated more with the participant’s objective cognitive performance and provided good cognitive impairment discrimination.
The aim of the present work was to assist further understanding on the psychometric properties and clinical usefulness of the M@T in Greek middle-aged, older, and older-old adult population (M@T-GR) across different groups of SCD, MCI, and HC. In our consideration, the use of different cognitive indicators assessed by screening tests and the inclusion of multiple measures can lead some light in understanding the cognitive state and reaction in adults of advanced age that have SCD or MCI. For this reason, we also attempted to study the association of the MMSE and SCD- Q and M@T-GR scores. More specifically our study’s hypotheses were: 1) M@T-GR would show increased structural validity and internal consistency, 2) M@T-GR would show high convergent validity in comparison with other neuropsychological tests such as MMSE and SCD-Q, and 3) M@T-GR would have increased discriminant validity between the three groups (HC, SCD, and MCI).
MATERIALS AND METHODS
Participants and settings
A cross-sectional research design with a convenience sampling approach was used in the study involving volunteers living in different residential areas of Thessaloniki in Greece. From September 2018 to December 2019, participants were recruited from the Memory & Dementia Outpatient Clinic of the 1st Neurological Department of Aristotle University of Thessaloniki, Greece, U.H. AHEPA (http://www.med.auth.gr/), and from the Day Centers of the Greek Association of Alzheimer’s Disease and Related Disorders (GAADRD; http://www.alzheimer-hellas.gr/index.php/el/) after visiting each department for a regular assessment for a first time.
The participants were invited to participate if they were native Greek speakers and schooled in Greece, aged 55 years and older, being capable of hearing and communicate verbally and in absence of motor control deficits. All participants were diagnosed by a neuropsychiatrist according to medical history, neurological examination, neuropsychological tests at first place and then with structural magnetic resonance imaging (MRI) and other necessary laboratory examinations. Overall, 250 participants took part in the study and only 232 were finally included in the analysis. We did not include participants younger than 55 years or if their examinations showed that cognitive impairment may be due to other reasons. The SCD group consisted of 78 participants, the MCI included 89 participants, while the HC group consisted of 65 participants. We used the Petersen criteria for MCI [12], and the IWG-2 Guidelines [34] as well as the latest SCD-I Working Group suggestions [20] for SCD. More specifically, HC and SCD were mentally and physically healthy who shared a similar age and educational background. All participants were right-handed, had normal or corrected-to-normal vision and audition (effective communication between patient and clinician), and had no other neurological, psychological, or serious medical disorders, which might affect cognitive performance. Given that there are some existing studies, which have shown that in discrimination tasks, the left-handed participants show differences with regards to brain activation compared to right-handers, in order to avoid any confounding factor, we excluded people who were left-handed so as to minimize any confounding factor that might influence our results [66, 67]. We strived to exclude participants where other etiologies could explain self-perceived memory deficits including vascular (examination of ischemic lesions of MRI, blood testing), psychiatric (interview, depression scale, psychoactive drugs, etc.), or other systematic etiologies by carefully evaluating their medical examinations.
Moreover, a mild clinical depression (as per pathophysiology often a comorbid condition) was considered an exclusion criterion for all participants. Depressive symptoms were assessed with the Geriatric Depression Scale-15 (GDS-15) rating scale using a cut-off score of < 5 at the time of the study visit. Despite that GDS-15 is generally used for people over 65, several research studies have found good sensitivity and specificity also for younger older adults [68–70]. Furthermore, following a meta-analysis of 17 studies, a study recommended using the GDS-15 for routine depression screening in primary medical care settings [71]. Therefore, we used it regularly for depression assessment in older adults in our study as well. Equivalently, we have used the Perceived Stress Scale and Neuropsychiatric Inventory [72] for the assessment of mood and emotional state, since it is a critical component for the evaluation of the SCD and MCI participants, since emotional distress can cause or exacerbate cognitive problems. To ensure adherence to the inclusion criteria and accurate categorization of our three groups, all available data of each individual including laboratory results, neuroimaging data, the patients’ medical history, and additional questionnaires were carefully reviewed. Thus, by taking all aforementioned measures, we have minimized the risk of recruiting participants with SCD due to reasons other than AD.
Ethical issues
Participants at the assessment were orally and written informed for the purpose of their participation and they had the opportunity to ask questions. They were also informed that all the data would be collected through an electronic database and the research team would make every effort to preserve their confidentiality. The participants gave written informed consent at the time of their visit, agreeing that their participation to the evaluation was voluntary and that they could withdraw the evaluation at any time, without giving a reason and without cost. The research team ensured that all participants have been adequately informed about the study aim and we ensured that the GDPR was applied for handling personalized data and storage anonymized coded information regarding the participants. They also informed and agreed that according to the European Union rules, their personal data could be deleted from the web-database after a written request. The evaluation was approved by the Scientific and Ethics Committee of GAADRD (41/06-06-2018).
Summary of M@T subtests and their scores
Neuropsychological assessment
The neuropsychological assessment was conducted privately in a quite environment between the clinician and the participant in order to minimize any possible distraction and enable the patient to concentrate. The MMSE [73] is probably the most widely used screening test for dementia. Despite that MMSE and other related cognitive tests have shown low sensitivity and specificity in differentiation between SCD and HC, we have followed a similar protocol to previous validation studies using M@T [50–52, 55]. Therefore, we administered MMSE as a neuropsychological tool to test the M@T validity. The maximum MMSE score is 30. It includes 10 points for orientation, 6 for immediate memory, 5 for calculation, 2 for naming, 3 for verbal comprehension, 1 for drawing, 1 for reading, 1 for repetition, and 1 for writing. To detect cognitive deficits, we used the Greek version of the MMSE [74]. Moreover, we also administered the Subjective Cognitive Decline- Questionnairre (SCD-Q) [59]. To assess depressive and anxious symptoms in older adults, we used the GDS-15 [75] and Perceived Stress Scale [76], respectively, and finally, the M@T-GR was used. Each participant was assessed in one session conducted by a trained psychologist with expertise in psychogeriatric and neuropsychological assessment. In order to confirm the inclusion criteria, during the semi-structured interview, the psychologist applied a socio demographic questionnaire and an inventory of current clinical health status, past habits, and medical history (with self-report by the participants). When was possible this information has been confirmed by a third part (family member, a clinical doctor, or medical records).
M@T administration and scoring procedure
The M@T [50] is a screening test with high discriminative properties for aMCI and early AD among the general primary care population. The maximum M@T score is 50. M@T has minimum 40, and maximum 50 questions (depending on the participant’s free recall success). One point is given for each correct answer, while there are 3 questions which have maximum score more than 1 point. All the questions are oral and have only one possible answer. It includes 5 points for coding, 5 points for retrieval and 5 points for orientation, 10 for free and 10 for cued recall, and 15 points for semantic memory. M@T was developed and validated in Spain but has been translated into English, although not validated in this form [77]. For the present validation study, we used the English version.
Translation process
The standards of International Test Commission [78] for the translation and adaptation of psychological tests were considered. Working independently, three researchers incited the translation of the original M@T from the English to the Greek version [53, 77]. That independent translation resulted in two versions of the scale and then one common version was established. This version was then submitted to back-translation by a bilingual speaker who was not familiar with the original scale. Finally, an English native speaker compared the back-translation version with the English M@T original. Then researchers determined that the translation was suitable. No significant changes were made to the original scale. The most significant change that was made relies on adapting the name of the boy “Luis” in encoding. Given that this name does not exist in Greek language and thus would be not familiar to Greek older adults, we used a similar disyllable Greek name “Tasos”. Additionally, we tested the comprehensibility of the final version of the scale through one-to-one interviews with 10 older adults and 3 psychologists chosen randomly. All the items were considered clear and comprehensible. Finally, the Greek version of M@T (M@T-GR) was declared to be final (see the Supplementary Material).
Statistical analysis
For data analysis, the IBM SPSS Statistics for Windows (version 25.0; IBM Corp, Armonk, NY) was used [79]. For relevant demographic characteristics and for the measures of the frequencies, means and standard deviation were obtained, according to the nature of the variable. The variables representing demographic characteristics of the sample were age and years of education. Regarding age, the sample was categorized in three age-groups: middle-aged adult group: 55–64 years, older adult group: 65–74 years, and older-old adult group: 75–89 years. The analyses carried out included Covariate Analysis of Variance (ANCOVA), by using as independent variables the demographic characteristics (age in years) and group, and as dependent variables the total scores on the M@T subtasks. The Scheffe test was used for post hoc multiple comparisons. The Scheffe post hoc test was chosen since it tests all possible comparisons, it is robust in relation to non-normality, and it provides maximum protection against type I error [80]. To examine the psychometric properties of the M@T-GR, we specifically examined its structural validity using exploratory factor analysis, convergent validity, discriminant validity, and internal consistency. Receiver operating characteristic curve (ROC curve) analysis was also used for assessing the predictive value of the M@T total score and M@T subtasks to discriminate the HC group and SCD and MCI groups respectively, for each age-group. Specifically, we divided HC into two subgroups (n of middle-aged HC = 32, n of older adult HC = 29), SCD into three subgroups (n middle-aged SCD = 26, older adults SCD = 38, older-old SCD = 14), and MCI into three subgroups (n middle-aged SCD = 11, older adults SCD = 51, older-old SCD = 27). At this point it must be mentioned that there was no older old adult HC subgroup in the analysis, due to the fact that there were only 5 people in this subgroup. The cutoff points were determined by maximizing the Youden index [81]. The area under the curve (AUC) of the ROC curve was used in order to quantify the M@T total score and its subscales discriminant potential in fair, good, perfect, or excellent according to the relative literature (AUC values from 1.0 are perfect, 0.9–0.99 is excellent, 0.8–0.89 is good, 0.7–0.79 is fair, and 0.51–0.69 is a poor test [82]).
RESULTS
Demographic characteristics
The majority of the 232 participants were female (78.2%). The mean age was 67.23 (SD = 14.59, range = 55–89). Table 2 shows that there were no statistically significant differences between the HC, SCD, and MCI, with regards to the years of education. Regarding MMSE, we found statistically significant differences between HC and MCI.
The table presents mean (M) and standard deviation (SD) of demographic characteristics among participants (HC = 65, SCD = 78, MCI = 89)
Structural validity: exploratory factor analysis of the M@T-GR
Prior to performing exploratory factor analysis with principal component analysis (PCA), the suitability of data for factor analysis was assessed. The Kaiser–Meyer–Oklin value was 0.7, exceeding the recommended value of 0.6 and according to Field (2013), was a good value. The Bartlett’s test of sphericity reached statistical significance [χ2 (15) = 254.182, p < 0.0001], supporting the factorability of the correlation matrix (Bartlett, 1954). In an initial analysis performing Kaiser’s (1960) criterion, the PCA revealed the presence of six components - factors with eigenvalue > 1, explaining a total of 38.46%of the total variance. The scree plot revealed a clear break after the first component suggesting that the M@T items assess only one underlying dimension or factor. After the inspection of the scree plot, we reran the analysis defining the number of factors to 1. Thus, the uni-factorial solution kept the same 38,46%of the total variance as the previous analysis (Fig. 1). Table 4 displays the item loadings on the factor.
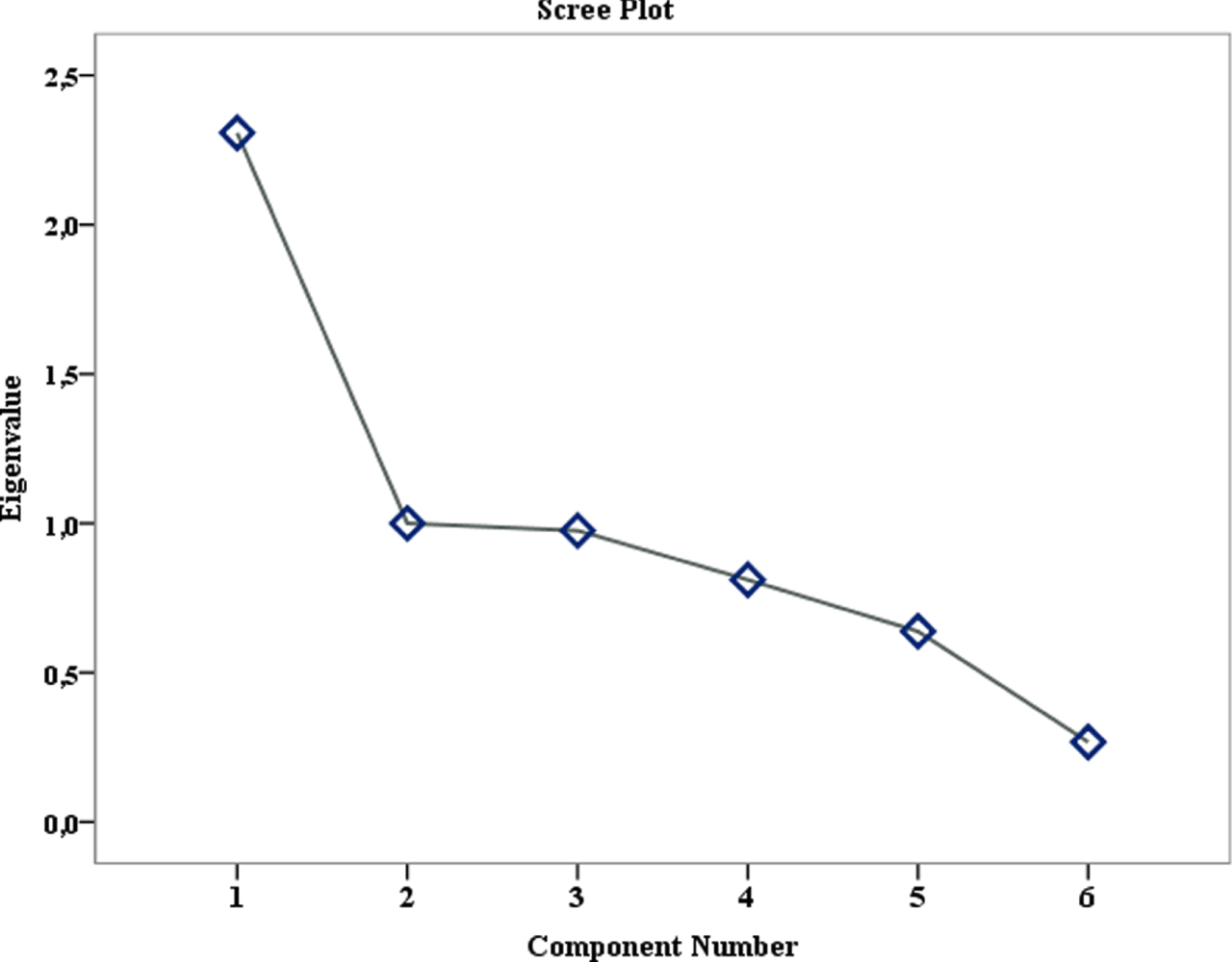
Scree plot illustrating after applying PCA for factor analysis of the M@T.
Convergent Validity of the M@T: Pearson correlations with SCD-Q and MMSE
*p < 0.05; **p < 0.001.
Factor structure of the M@T
*Factor loadings over 0.40 appear in bold.
Internal consistency of the underlying factor of the M@T-GR
More specifically M@T-GR, consisting of 6 items was found to be reliable with a Cronbach’s alpha coefficient (α= 0.75), which indicates adequate level of internal consistency. M@T-GR has demonstrated satisfactory internal consistency in HC, SCD, and MCI. A more detailed analysis reveals that there is no impact on the internal consistency reliability of M@T-GR with the exclusion of any item.
Convergent validity of the M@T-GR
In order to assess convergent validity, we computed Pearson correlations of the total score of SCD-Q MyCog with M@T total score and its subscales. Coding, Free Recall, and Cued Recall were found to correlate significantly with SCD-Q My Cog. Table 4 presents convergent validity using Pearson’s correlation coefficient for the M@T total score and its subscales with SCD-Q TheirCog. Total answer score to part II TheirCog also showed a significant Pearson’s correlation with M@T total score and four subscales: Coding, Orientation, Free Recall, and Cued Recall. MMSE total score showed a significant and positive correlation with: M@T total score, Coding, Retrieval, Orientation, Semantic Memory, Free Recall, and Cued recall.
Discriminant validity of the M@T-GR
One-way ANCOVA was conducted to examine whether there is a statistically significant difference between HC, SCD, and MCI diagnostic groups in M@T-GR total score and its subscales controlling for age variable. In particular, M@T total score was significantly different between HC and SCD (I-J = 2.26, p = 0.032), HC and MCI (I-J = 6.16, p < 0.0001), and SCD compared to MCI (I-J = 3.90, p < 0.0001).
In detail, statistically significant differences were found in M@T subscales between HC, SCD, and MCI with regards to: Coding: F(2, 221) = 4.51, I-J = 0.274, p < 0.01, Free recall: F(2, 221) = 20.93, p < 0.0001, Cued Recall: F(2, 221) = 16.36, p < 0.0001, Orientation: F(2, 221) = 19.169, p < 0.0001, and Semantic Memory: F(2, 221) = 10.61, p < 0.0001 after controlling age in years. On the other hand, post-hoc Scheffé’s comparisons showed statistically significant difference between HC and MCI with regards to M@T subscales: Coding: I-J = 0.52, p < 0.0012, Free Recall: I-J = 2.37, p < 0.0001, Cued Recall: I-J = 1.26, p < 0.0011, Semantic Memory: I-J = 1.19, p < 0.0012. There is a significant effect of the diagnosis on the M@T Free Recall subscale between HC and SCD: I-J = 0.998, p = 0.0112. Figure 2 shows the distribution of the scores for each group. On the other hand, SCD-Q MyCog and TheirCog showed no statistically significant different scores between HC and SCD or SCD and MCI. Whilst statistically significant difference was found between groups only in SCD-Q TheirCog total score: F(2,221) = 3.41, p = 0.0351 Post-hoc Scheffé’s showed statistical significant difference solely between HC and MCI: I-J = 3.01, p = 0.0284.
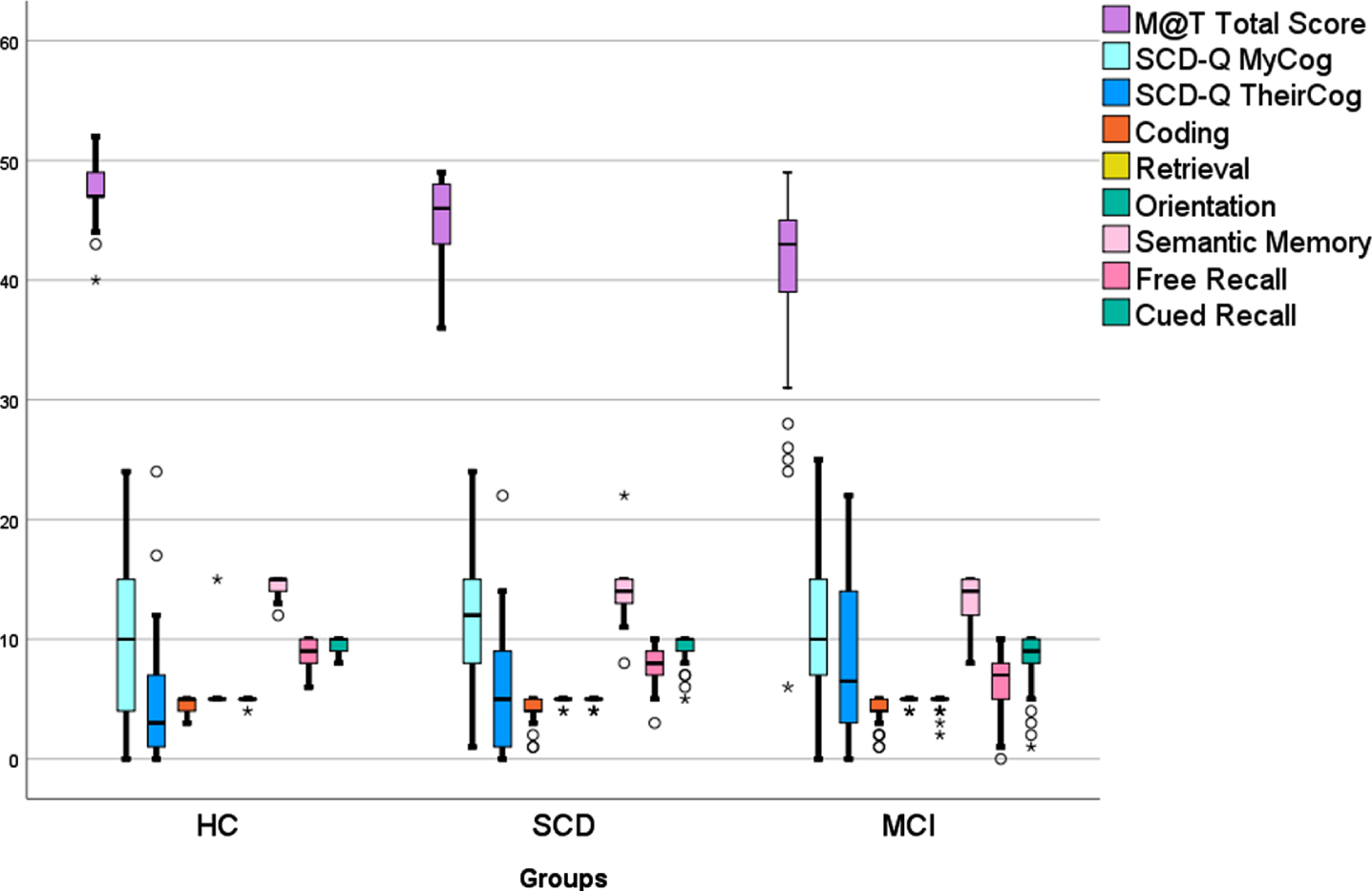
Distribution of M@T scores and SCD-Q (median, first and third quartile and outliers) for HC, SCD, and MCI.
ANCOVA test for discriminating between HC, SCD, and MCI using M@T and SCD-Q. Mean, SD, and p
Given that age-group significantly affected M@T performances, we examined the ROC curves in the three age-groups of the participants. The ROC curve analysis was applied in order to analyze the predictive values and to evaluate the diagnostic accuracy of M@T-GR, to discriminate HC from SCD, HC from MCI, and SCD from MCI. Figure 3 provides the graphic representations of the ROC’s curves, while Table 6 shows the ROC curves analyses’ results for the M@T as a screening test for SCD and MCI in middle-aged adults, older adults, and older-old adults. We did not compute the ROC for older-old sample of HC and SCD, given that we did not have adequate number of people allocated in older-old adult HC subgroup.
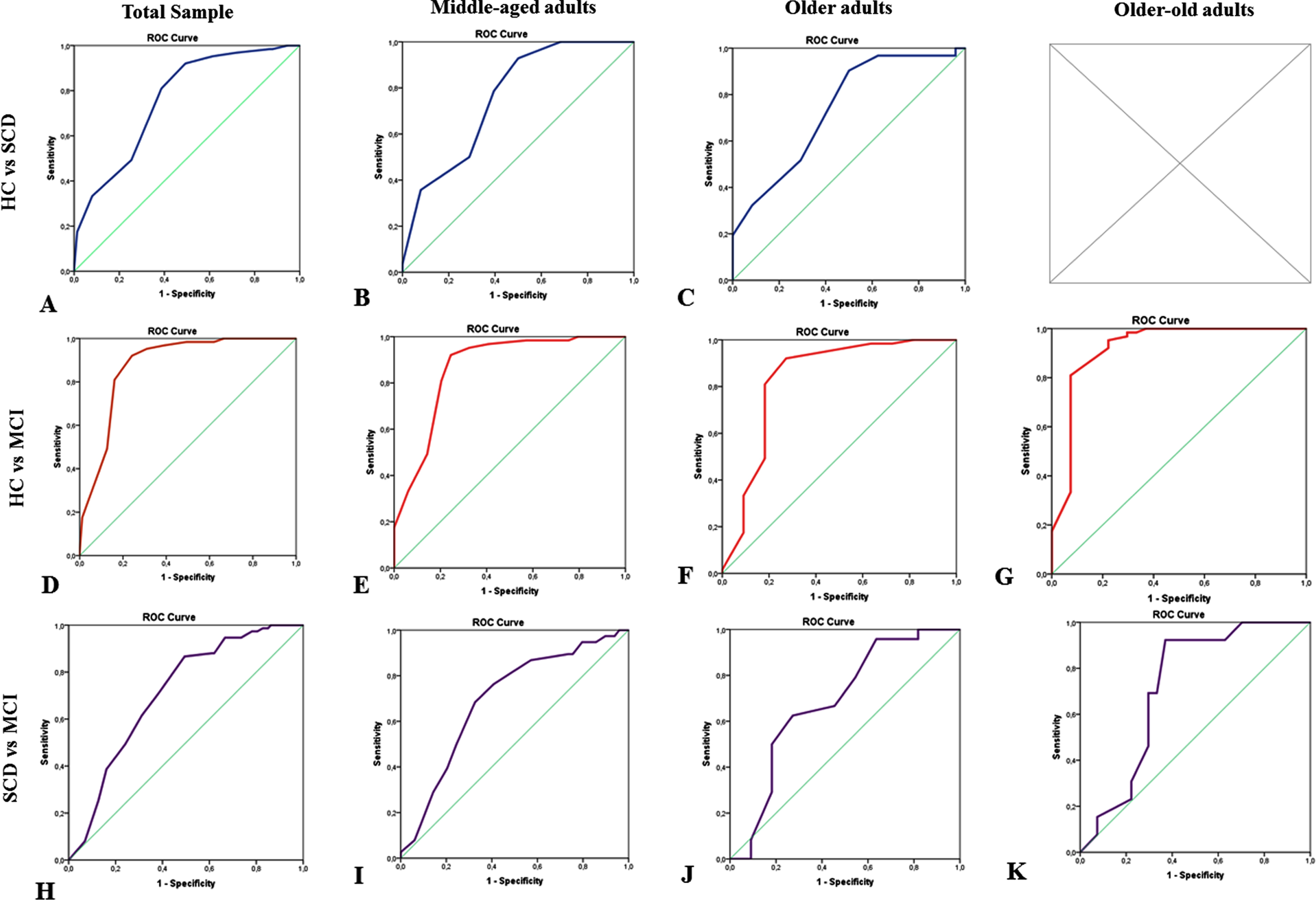
ROC curves for the discrimination between HC, SCD, and MCI people by means of the M@T-GR.
Cutoff points and diagnostic utility of the M@T to discriminate between HC, SCD, and MCI groups
DISCUSSION
The purpose of the study was to develop the first Greek adaptation of M@T and to explore the associations between demographic variables, and global cognition as measured by MMSE, SCD-Q, and M@T-GR. Our study showed that M@T constitutes a good to excellent discriminative test for detecting MCI from HC, good to fair for distinguishing SCD and MCI, and fair enough to discriminate HC from SCD. It is brief and easy to administer and score and can be considered as an effective screening test with adequate discriminative properties for the assessment of SCD population.
In agreement with previous reports [49–53, 77], our results suggest that the HC obtained higher M@T global score than SCD and MCI by mean value. In detail, at the level of M@T-GR subtests, the HC also demonstrated significantly higher performances than SCD and MCI. All participants who were not successful in subtest Coding had achieved high performance in the subtest Cued recall. This can be explained in adult population given that Free recall as a cognitive function measures the ability to perform complex executive functions and speed, which are widely impaired due to aging [83]. These results should be interpreted cautiously, but can reinforce that episodic memory deficits could indicate an early predictor of AD [57] and the M@T as a comprehensive test that reflects the consolidation memory theory stating [49, 77]. Despite that the MMSE is a widely used clinical instrument, it foresees an average exposure time of approximately 10 min and only discriminates MCI and AD from HC, its sensitivity and specificity is low for SCD and MCI [24, 33], and is not very sensitive for discriminating SCD from HC [52]. This is related to the fact that memory deficits are often the earliest feature of AD, and global cognitive scales present low sensitivity and specificity for detecting SCD [84]. Indeed, in our sample, the MMSE showed a low performance for discriminating early SCD and HC. In addition to MMSE, the SCD-Q showed also low discriminative validity between HC and SCD. On the other hand, this initial phase of Greek adaptation of M@T-GR supports the potential of M@T as a screening tool with fair validity and suggests the possibility of a similar functioning of the Greek, Portuguese, English, and Spanish versions of the instrument. Thus, given that episodic memory has been shown to be an important marker of cognitive decline associated with dementia, especially in early phases of the disease, we believe that semantic memory items presented in the M@T are the reason for the good to fair results of this screening test.
Additionally, in the present study, M@T-GR has shown significant discriminative properties for detecting MCI and SCD among HC population. The influence of age between the HC, SCD, and MCI turned out to have a significant effect. Thus, we allocated the participants in three age groups (middle-aged, older, and older-old adults). The ROC curve analysis of the M@T-GR, suggests a better diagnostic accuracy to discriminate older adult SCD from HC with 81%sensitivity and 61%specificity. These findings are consistent with other studies showing increased sensitivity of M@T in discriminating preclinical stages of SCD and MCI compared to HC [49–51, 77]. In our sample, an ideal cut-off point to differentiate the middle-aged adults SCD from MCI reached of 46.50 points, similarly to what was described in the original work [50]. In contrast to a previous finding [55], we verified a significant correlation coefficient between the M@T-GR and MMSE, suggesting fair convergent validity. Our study verified a lower and negative relationship between SCD-Q MyCog and SCD-Q TheirCog and M@T-GR. Based on the capacity of M@T-GR for discriminating HC from patient population, it can be considered as a valuable and useful tool that may help the clinicians and neuropsychologists to derive patients to outpatient clinics. From a psychometric point of view, the optimal M@T-GR cut-off score to distinguish SCD middle-aged adults from HC should be 42.50. In this sense, although we have given specific cut-off points, one may use a different cut-off with more sensitivity or more specificity depending on the characteristics of the aging population to be screened. We found fair performance values (AUC ≥0.76) with sensitivity (≥92%) and specificity (≥75%) when the M@T-GR was applied in our middle-aged group of MCI compared to HC. The cut-off score of the M@T-GR varies according to the diagnosis suspected. The M@T-GR was applied using a cutoff score of 45.50 points, for the diagnosis of MCI (AUC = 0.88). This performance is higher than observed in previous studies [52]. Furthermore, we found a sensitivity of 72%and a specificity of 61%to differentiate between older-old adults with SCD and MCI using a cutoff score of 43.50 points. In particular, we found much higher sensitivity 92%and specificity 78%of detecting older-old MCI compared to HC using M@T-GR compared to a recent approach (M@T-total score: sensitivity 85%and specificity 84%) [52]). In Peru, M@T has been shown to be a reliable test with high precision to discriminate between early AD, aMCI, and HC in low educational level individuals [51]. The Portuguese version of M@T has 97%sensitivity and 71%specificity to differentiate SCD and MCI, with a cut-off score of 32 points. Similarly, our study found a cut-off point (39.50) to differentiate SCD and MCI with 92%sensitivity and 63%specificity. Considering the M@T-GR assessment (total score and subtests) for discriminating between SCD and HC, the M@T-GR total score is statistically significant compared to M@T-GR subtests. This suggests that the total score to discriminate between these conditions is more accurate than using the subtests alone. On the other hand, the M@T-GR total score is practically equal to the M@T-GR free recall for discriminating SCD from HC, suggesting that this subtest is as accurate as using the full test. Additionally, the exploratory factor analysis of the M@T-GR showed that the Kaiser Bartlett of sphericity reached statistical significance, supporting the factorability of the correlation matrix, suggesting that the M@T-GR items assess only one underlying dimension or factor.
An important limitation of the M@T-GR, in agreement with other screening tests, is that it should not be used in isolation for diagnosis purposes of SCD. It could suggest the diagnosis, but other clinical and neuropsychological testing is needed to confirm the existence of SCD. Visual memory, language, executive, and other relevant neuropsychological functions related to the AD process are not assessed by the M@T. The M@T, as a screening tool, may suggest SCD or MCI diagnosis but does not establish it, since the diagnosis should be made considering the results of a full neuropsychological evaluation.
CONCLUSION
The M@T-GR adaptation provides quick and efficient screening with adequate discriminative properties for SCD and MCI Greek Population among the general primary care population. It seems to be a valuable screening test easily administered, that can provide an important objective, is cost effective, and is a useful tool to discriminate SCD and MCI from HC elders in Greece. The Greek adaptation and validation completed in this study can be considered a first step toward using screening tools for detecting SCD population in primary care. Still, further studies to assess psychometric properties of the translated scales are necessary to validate it. Overall, the results proved that this instrument can be considered as an adequate tool for discriminating early preclinical stages from healthy elders. Future research is recommended to examine the best component solution and if there are differences between the HC, SCD, and MCI.
Footnotes
ACKNOWLEDGMENTS
The authors would like to express their gratitude to the psychologists from Greek Association of Alzheimer’s Disease team for all precious help on developing the Greek translation of the scale and contributing to its validation. This research has been co-financed by the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call RESEARCH-CREATE-INNOVATE (project code: T1EDK-02668).