
Abstract
Background:
Several modifiable risk factors for dementia have been identified, although the extent to which their modification leads to improved cognitive outcomes remains unclear.
Objective:
The primary aim is to test the hypothesis that a behavior modification intervention program targeting personalized risk factors prevents cognitive decline in community-dwelling, middle-aged adults with a family history of dementia.
Methods:
This is a prospective, risk factor management, blinded endpoint, randomized, controlled trial, where 1510 cognitively normal, community-dwelling adults aged 40–70 years old will be recruited. Participants will be screened for risk factors related to vascular health (including physical inactivity), mental health, sleep, and cognitive/social engagement. The intervention is an online person-centered risk factor management program: BetterBrains. Participants randomized to intervention will receive telehealth-based person-centered goal setting, motivational interviewing, and follow-up support, health care provider communication and community linkage for management of known modifiable risk factors of dementia. Psychoeducational health information will be provided to both control and intervention groups.
Results:
The primary outcome is favorable cognitive performance at 24-months post-baseline, defined as the absence of decline on one or more of the following cognitive tests: (a) Cogstate Detection, (b) Cogstate One Card Learning, (c) Cogstate One Back, and (d) Cognitive Function Instrument total score.
Conclusion:
We will test the hypothesis that the BetterBrains intervention program can prevent cognitive decline. By leveraging existing community services and using a risk factor management pathway that tailors the intervention to each participant, we maximize likelihood for engagement, long-term adherence, and for preserving cognitive function in at-risk individuals.
Keywords
INTRODUCTION
Dementia is the second largest cause of death in Australia, of which Alzheimer’s disease (AD) is the most common form. No disease modifying therapy is currently available. However, it is estimated that approximately 35%of all dementias can be attributed to risk factors that are potentially modifiable [1, 2]. Risk factors for late-life cognitive decline are well established and include hypertension, low physical activity, poor diet quality, anxiety and depressive symptoms, low cognitive engagement, and poor sleep [2–7]. Several major challenges in reducing disease burden with behavior modification exist, including the implementation of innovative solutions that are effective in changing behaviors and changing behaviors that favorably modify disease onset in a timeframe that allows for the prevention of cognitive decline.
Clinicopathological studies of AD suggest that pathophysiological changes can begin up to 30 years before the onset of clinical symptoms [8, 9], with the accumulation of AD proteinopathies (e.g., amyloid-β (Aβ), tau) likely beginning in midlife (e.g., 40–70 years) [10–12]. This has given rise to the prevention strategy of identifying cognitively normal at-risk individuals for early intervention to slow cognitive decline and the clinical onset of AD [13, 14]. Modifiable risk factors have been shown to have the strongest association with dementia risk in the decades before clinical diagnosis of dementia. As such, behavioral interventions targeting personalized risk factors for cognitive decline may have maximal efficacy when implemented in midlife [4, 15–17].
While mood, vascular risk (including nutrition and physical inactivity), cognitive engagement, and sleep are modifiable risk factors for dementia, some barriers limit their successful management. Participation rates in behavior modification trials are low. Only 13–47%of trial participants seek to improve diet or increase physical activity [18, 19]. Additionally, risk factors for dementia vary between individuals and therefore effective solutions need to be specific to an individual’s risk factor profile, providing a targeted, relevant, and person-centered approach. Person-centered approaches are advantageous as they may encourage individuals to adopt and enact risk mitigation strategies that will be effective in their daily lives and leverage existing community services around the individual to promote long-term adherence [20].
There are several multi-domain behavior modification trials to prevent cognitive decline (e.g., the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) and Maintain Your Brain (MYB)) [21, 22], yet few have utilized a person-centered approach using a risk factor management pathway to prevent cognitive decline. There is evidence that such programs are successful in other conditions, such as falls prevention. The RESPOND program was a telephone-based, patient-centered falls prevention program that was demonstrated to reduce falls, but not fall injuries, in older people presenting to the emergency department with a fall [20]. Program evaluation of RESPOND showed high acceptability among participants, and that the participant-centered approach, use of goal setting and motivational interviewing, positive health messaging, and leveraging technologies (e.g., telehealth), increased participant engagement [20].
Based on the same guiding principles as RESPOND, we have designed a program (BetterBrains) to prevent cognitive decline in middle-aged adults (40–70 years) through the delivery of a person-centered intervention that targets individual risk factors known to increase risk of cognitive decline and dementia (see Box 1 for an overview of the intervention). These risk factors relate to vascular health, low mood, poor sleep, and low social and cognitive engagement. BetterBrains adopts a risk factor management strategy where each targeted risk factor is dependent on individual goal prioritization and the presenting modifiable risk factor(s) for dementia (Box 1). This flexibility has been shown to increase participation, adherence and engagement [23].
Through these guiding principles, BetterBrains, an online, person-centered, risk factor management program aims to delay cognitive decline in Australian middle-aged adults with a family history of dementia. This program will incorporate five unique components: 1) remote assessment of outcomes via an online web platform (betterbrains.org.au), 2) screening to identify personalized risk factor profiles; 3) targeted risk factor management driven by participant preference and supported by motivational interviewing and goal-setting, 4) telehealth support (via phone or video call) by trained coaches to review and support behavior change, and 5) smartphone-app support to assist participants in undertaking their recommended strategies (e.g., notifications, weekly check-ins, assessment of barriers to engagement, alerts to coaches if participants’ indicate repeated disengagement).
TRIAL DESIGN
This is a prospective blinded endpoint 24-month randomized controlled trial (RCT) to test the effectiveness of BetterBrains, an online, person-centered, risk factor management intervention to prevent cognitive decline. We will compare the outcomes in the BetterBrains intervention group with those in a control group receiving standard health education.
Intervention (BetterBrains) Overview
Delivered by BetterBrains Coaches trained in motivational interviewing, behavior change strategies and risk factor management via telehealth Active intervention will last for 12 months from randomization Suggested strategies for intervention are dependent on risk factor management pathway, and driven by participant preference Risk factor management will target one or more of the following:
Medical management facilitation Psychology or counselling service referral (health literacy, education, and GP referral) Behavioral activation eTherapy (e.g., web and/or app-based programs) Smoking cessation Physical activity Dietary modification Responsible consumption of alcohol and/or caffeine Social engagement Continuing education/skill development Participation in cognitively stimulating activities Sleep psychoeducation Advanced sleep phase (light) therapy Risk factor management strategies map onto one or more of the common categories of modifiable risk factors for dementia (i.e., vascular risk, poor mood, low social and cognitive engagement, and poor sleep).
Aims and hypotheses
Primary aim
The primary aim is to test the hypothesis that the BetterBrains intervention program can prevent cognitive decline in middle-aged adults. We hypothesize that a higher proportion of participants randomized to the BetterBrains program will show a favorable cognitive outcome at 24-months than those randomized to the control group.
Secondary aims
Secondary aims are to determine whether participants randomized to the BetterBrains intervention program show changes in 1) cognitive function (complex attention, executive function, memory and learning), 2) subjective ratings of health and quality of life, and 3) dementia risk as measured by the Australian National University Alzheimer’s Disease Risk Index (ANU-ADRI) and the Cardiovascular Risk Factors, Aging and Incidence of Dementia (CAIDE) risk scores, compared to the control group.
Tertiary aims
Tertiary aims are to determine whether participants randomized to the BetterBrains intervention program show changes in 1) health literacy, 2) motivation to change health behavior, and 3) work productivity, compared to the control group.
Exploratory aims
Exploratory analyses will aim to identify variables that may moderate the efficacy of the intervention to prevent cognitive decline. Variables of interest include 1) the apolipoprotein E (APOE) ɛ4 allele (strongest genetic risk factor for sporadic AD), 2) the nature and number of dementia risk factors, 3) individuals’ readiness to change behavior, and 4) level of engagement with the intervention. A full program evaluation of this RCT will also be conducted. The program evaluation protocol will be published separately.
Participants and setting
Community-dwelling adults aged 40–70 years old (inclusive), living in Australia, who have a first- or second-degree family history of AD or dementia and meet the below defined 7 inclusion criteria will be eligible for recruitment. Exclusion and inclusion criteria for this study are detailed below. The BetterBrains intervention program and corresponding RCT will be conducted virtually via a website, smartphone application, and telephone coaching sessions.
Inclusion criteria
Aged between 40–70 years; Plans to reside in Australia for at least 2 years (irrespective of citizenship); First- or second-degree family history of dementia (AD, Parkinson’s disease, Lewy body dementia, or other known diagnosis of dementia); Fluent in the English language; Access to a tablet, desktop, or laptop computer with internet connectivity (to complete computerized cognitive tests via our online platform and engage in telehealth sessions with the BetterBrains coaches); Willing and able to provide informed consent; Willing and able to commit to undertaking a series of online assessments over 2 years; At least one modifiable dementia risk factor identified during the online screening process; Willing and able to provide a saliva sample for genotyping.
Exclusion criteria
Diagnosis of mild cognitive impairment (MCI), AD, Parkinson’s disease, Lewy body dementia, or other known diagnosis of dementia; Current use of any Therapeutic Goods Administration (TGA) approved medication for the treatment of AD (e.g., donepezil, galantamine, rivastigmine, memantine, or other newly approved medication); Current use of any TGA approved medication for the treatment of Parkinson’s disease (e.g., Sinemet, amantadine, bromocriptine, pergolide, selegiline, or other newly approved medication) History of severe traumatic brain injury or other significant neurological disease or insult (e.g., multiple sclerosis, stroke, epilepsy); Uncontrolled major depressive disorder or another Axis I psychiatric disorder as described in DSM-IV-TR within the past year, psychotic features, agitation, or behavioral problems; History of alcohol or substance abuse or dependence within the past 2 years; Regular (daily) use of narcotics or antipsychotic medications; History of myocardial infarction in the past year or unstable severe cardiovascular disease including angina or congestive heart failure with symptoms at rest; Respond “no, and I have no intention to make changes” in response to the question “have you made any changes to your lifestyle during the past year to actively reduce your risk of dementia (e.g., increasing physical activity, engaging in cognitively stimulating activities, lowering stress)?”; No modifiable dementia risk factors identified during the online screening process; Participant does not complete their risk factor assessment within a 4-week period (2 attempts will be provided, see Fig. 1).

Study procedure flowchart.
Outcomes
The primary outcome is favorable cognitive performance at 24-months, defined as the absence of decline (rate of change over 24-months that is less than 0.5SD) on one or more of the following cognitive tests: (a) Cogstate Detection test (speed), (b) Cogstate One Card Learning test (accuracy), (c) Cogstate One Back test (speed), and (d) total score on the Cognitive Function Instrument.
Secondary outcomes are as follows: Change in cognitive function (complex attention, executive function, memory, and learning) assessed by the Cogstate Brief Battery, Cogstate IDSST-Medicines, and the Online Repeatable Cognitive Assessment (ORCA) battery; Change in subjective ratings of general health and quality of life, as measured by the RAND Change in health literacy, assessed by the Health Literacy Questionnaire (HLQ); Change in motivation to change health behavior, assessed using the Motivation to Change Health Behaviour for Dementia Risk Reduction questionnaire; Change in work productivity (absenteeism and presenteeism), assessed using the Valuation of Lost Productivity questionnaire.
All measures will be collected at baseline, 12- and 24-months.
Primary estimand
For intercurrent events that may potentially modify cognitive outcomes (e.g., stroke, traumatic brain injury) and for events relating to the prescription of concomitant medications which are listed in the exclusion criteria and/or likely to impact on trial outcomes (e.g., donepezil, memantine), a team of medical monitors (Yassi, Brodtmann, Bush) will assess in a fully-blinded manner, the nature of the event, and determine whether the event is likely to have sufficiently modified cognitive outcomes. If the team identify an intercurrent event that is cognitively modifying, the participant in question will still be included in the primary outcome analysis, but the classification of the primary cognitive outcome for that participant will be automatically classified as negative (i.e., presence of cognitive decline), irrespective of their actual cognitive performance. For intercurrent events that influence intervention participation (e.g., motor vehicle accident with no head injury), intervention discontinuation, prescription of rescue medications/alternative therapies not listed in the exclusion criteria, or death, no a priori amendments will be made to any outcomes.
Sample size
Sample size calculations were based on unpublished data from 800 participants enrolled in the Healthy Brain Project, an observational study on individuals with similar characteristics as the BetterBrains trial (i.e., participants are aged 40–70 years, have a family history of dementia, have undergone cognitive testing using the same outcome measures and the same remote, unsupervised, web-based mode of assessment) [24]. Of this group, 680 participants were classified as having at least one modifiable risk factor for dementia (120 participants had no modifiable risk factors for dementia). Participants were classified as having an “unfavorable” cognitive outcome (slope estimate of > 0.5 SD decline) or a “favorable” cognitive outcome (slope estimate of < 0.5 SD decline). Change over time for each participant was estimated using linear mixed models, with random slopes and intercept. We found that over 24 months, ∼78%of individuals with at least one modifiable risk factor presented with no cognitive decline, defined using the cognitive tests that make up our primary outcome. Conversely, ∼88%of individuals with no modifiable risk factors presented with no cognitive decline.
We have conservatively estimated that the BetterBrains intervention program will result in a 7%absolute increase in the proportion of participants with a favorable cognitive outcome in the intervention compared to the control group. Recruiting 1,510 participants (755 per group) would yield 90%power to detect at least a 7%increase in the proportion of participants achieving a favorable cognitive outcome in the intervention group compared to the control group (78%in control, 85%in intervention, total n = 1,290 (645 per group), two-sided p = 0.05), allowing for potential 10%loss-to-follow-up.
To allow for a trial run-in period in which operational and procedural difficulties can be identified and rectified as needed, the first 10 participants enrolled in the trial will be excluded from the primary outcome analyses. The number of participants to be included in primary outcome analyses is therefore 1500. Sample size estimates were obtained using G*Power 3.1.9.2, using z-tests to determine the difference between two independent proportions.
Recruitment
Recruitment will consist of two approaches. First, a small number of invitations (e.g., n = 15) will be sent to a randomly selected group of participants from the Healthy Brain Project (healthybrainproject.org.au) via email, from which we anticipate enrolling 10 participants. The first 10 participants will complete consent, registration, risk factor assessment, baseline and randomization before a broader invitation is extended to the rest of the Healthy Brain Project cohort. This will be done via email, study newsletters and social media announcements. The Healthy Brain Project is an online observational cohort study that has enrolled 7,000 participants aged 40–70 years at study entry [24]. Participants from the Healthy Brain Project have been recruited through the community. Should existing Healthy Brain Project participants consent to be a part of this trial, their participation in the Healthy Brain Project will be suspended for the duration of their participation in the trial. They will have the opportunity to re-engage with the Healthy Brain Project at the conclusion of this trial. Second, community dwelling middle-aged adults will be invited to take part in this trial via a variety of sources, including newspaper and radio advertisements, through social media, consumer organizations and public lectures.
Study procedure
Figure 1 provides an overview of the study procedure.
Pre-screen
Interested individuals will be directed to access the study website at betterbrains.org.au. Participants will be able to access an explanatory statement on this website. This statement forms part of the Participant Information and Consent form and will provide participants with a summary of the trial, its aims, the requirements of participation and a participant’s rights as a volunteer in the BetterBrains trial. Participants will also be able to download and save a PDF copy of the explanatory statement for their reference. After indicating that they have read the explanatory statement, prospective participants will then be directed to complete pre-screening, by confirming that they meet the criteria outlined in Supplementary Table 1. They will do this by answering a series of questions. Prospective participants will be required to select “yes” to each of these questions in order to proceed to the medical screen.
Medical screen & readiness for change
Participants will be required to tick a box to indicate their consent for the study team to collect information pertaining to their medical history. Once participants have indicated their consent, they will be required to respond “Yes” or “No” to a series of prompts based on the inclusion and exclusion criteria for the study (Supplementary Table 1) to determine further eligibility. Participants will also be presented with a single Likert-scale question to determine their readiness for change (Supplementary Table 1).
Informed consent
Upon completion of the pre-screen and medical screen sections, participants will proceed to undergo the informed consent process. Given the online nature of this trial, we have presented the consent form in an interactive manner, whereby participants will be presented with selected key components of the study that they will be required to consent to by selecting “Yes” or “No”. Once the participant has completed this, they will be asked to provide their full name in lieu of an electronic signature.
Online profile creation
After providing informed consent, participants will create an online profile by entering the following information: first name, last name, email address, contact phone number, handedness, date of birth, sex, residential address, postcode, and state. Participants will also be asked to indicate whether they are enrolled in the Healthy Brain Project, whether they have a smartphone (iPhone or Android), and to provide details of their general practitioner (GP).
Risk factor screening
Participants will then be directed to complete a risk factor screening assessment. This comprises of 10 questionnaires (∼30 min) which map onto 4 risk domains: (a) Hearts (vascular risk), (b) Mood (depressive, anxiety or stress symptoms), (c) Sleep (extent of sleep disruption), and (d) Minds (level of social and cognitive engagement) (Table 1). Participants will be encouraged to complete these risk factor surveys within four weeks. If a participant does not complete the risk factor assessment within 4 weeks, they will be provided with an opportunity to re-take the assessment in its entirety. This is to ensure that the most accurate information regarding participants’ lifestyle risk factors for dementia are collected. If the participant does not complete their risk factor assessment within 4 weeks on their second attempt, no further opportunities to re-take the assessments will be offered, and the participant will be excluded from the trial. Participants will be sent several notifications and reminders. If no risk factors across the four domains are identified during the risk assessment, the participant will be notified of their ineligibility to take part in the trial via the BetterBrains website and offered participation in the Heathy Brain Project instead. If one or more risk factors are identified, participants will be informed via the BetterBrains website that at least one lifestyle risk factor has been identified, which makes them eligible for enrolment in the trial. In participants for whom elevated depressive and/or anxiety symptoms have been identified, a letter to their nominated GP will be sent, irrespective of whether the participant is randomized to the intervention or control group. Upon completion of the risk factor screen, participants will be directed to complete the baseline assessment.
Schedule for Pre-Baseline Risk Factor Screen (RFS), and Baseline Assessment
Baseline assessment
Participants have 4 weeks (28 days) from the completion of their risk factor assessment to complete their baseline assessment. As part of the baseline assessment, participants will be asked to complete approximately 110 min of cognitive testing, with the Cogstate Brief Battery, the Cogstate iDSST-Medicines test, and the ORCA battery that has recently been shown to be sensitive to subtle cognitive dysfunction in preclinical AD [25, 26]. Participants will also be required to complete several detailed questionnaires evaluating several medical, lifestyle, health, and work productivity factors (33 min total). Participants will also be asked if they are currently taking medications. Participants who respond ‘yes’ will be instructed to take a photo of their medication packaging and label and to upload this to their BetterBrains profile. An RA will then be responsible for data entry and coding of the medications uploaded. If the reason for the prescription is not ascertainable from the photo provided by the participant, then a study RA will contact the participant via phone call or internal message to clarify reasons for taking each medication provided. Given the comprehensive testing, we have organized the baseline assessment into seven 20 min blocks of testing (Table 1). Participants have the option of completing all 7 blocks consecutively in one day or across 4-weeks. This design is similar to what has been implemented in the Healthy Brain Project [24], and has been designed to reduce assessment fatigue and to provide maximum flexibility for participants, while collecting a comprehensive set of key outcome variables.
A maximum of five reminder notifications will be sent to participants when each assessment is due, provided it is yet to be undertaken. If the participant fails to complete all baseline surveys and tests in the specified time interval (i.e., 4 weeks), they will not progress in the trial (i.e., no further participation).
Randomization
Upon the completion of all baseline assessments, participants will be asked to upload a photo of their ID (e.g., driver’s license, Medicare card). This ID will then be verified by a research assistant. After ID verification, participants will be randomly assigned into the intervention (BetterBrains) or control groups in a 1:1 ratio based on the following stratification variables: (a) age (< 55 years versus≥55 years), and (b) rurality (i.e., urban versus rural/regional based on classifications from the Australian Bureau of Statistics). Age and rurality were selected as stratification variables as they were considered to have a substantial impact on the primary outcome and community/health resources available to participants in the intervention group. Computer-generated allocation as a part of the electronic Case Report Form (eCRF) will be conducted using permuted blocks of variable sizes (not disclosed in the protocol due to its public availability) after the baseline assessment. Participants will be notified of group allocation automatically via the BetterBrains platform. Depending on their allocation, participants will receive the relevant procedures outlined below.
Blinding
Outcome assessments will be conducted entirely online and will be assessor blinded. A research assistant will monitor completion of all primary, secondary, and exploratory outcomes, and follow-up with participants if necessary. As genetic analyses will only be conducted at the end of the trial, participants, investigators, coaches, and research assistants will remain blinded to participants’ APOE status for the entire trial duration.
Intervention (BetterBrains)
The intervention (BetterBrains) will be delivered by trained psychologists, physiotherapists, dieticians, nurses, or occupational therapists with expertise in motivational interviewing, behavior change strategies, and risk factor management (henceforth referred to as ‘BetterBrains Coaches’). The 12-month intervention will commence from the completion of the participant’s baseline assessment. Key risk factors and associated evidence-based management strategies will form the basis of the intervention. Intervention group participants will nominate which risk factor they intend to address, in consultation with their BetterBrains coach. During the first call, the BetterBrains coach will engage the participant in a discussion about their risk factor(s) and explore barriers and enablers to addressing them. Suggested strategies are dependent on the risk factor management pathway, which have been developed to map onto four common risk factor categories of dementia (Table 2): BetterHearts, which targets cardiovascular risk factors, including physical inactivity; BetterMind, which targets social and cognitive engagement; BetterMood, which targets depressive, anxiety or stress symptoms; and BetterSleep, which targets symptoms of insomnia, advanced sleep phase disorder, sleep apnea, and overuse of sleep medications.
Summary of BetterBrains risk factor management strategies
Suggested strategies within each risk factor pathway are dependent on participant access to healthcare services and their financial position (e.g., Medicare or Private Health Insurance). Coaches will encourage participants to address multiple risk factors across the 12-month intervention. BetterBrains Coaches will provide education and coaching to participants in the intervention group via telehealth during the active intervention phase (Table 3). Intervention group participants will receive a minimum of 6 scheduled calls from their coach (Fig. 2). Coaching in these telephone calls will focus on person-centered care to optimize participant engagement. Motivational interviewing will be used to support the participant to understand the findings of their risk assessment and to facilitate goal-setting based on the participant’s identified risk factors for cognitive decline. Anticipated barriers to engagement (e.g., work and/or family commitments) will also be identified, and coaches will assist participants to find solutions to barriers identified. Further, coaches will also assist intervention group participants by recommending action strategies to meet goals and assist with finding appropriate support services and resources local to the participant’s residential area (community linkages). Should intervention group participants require additional support, they will be able to schedule a phone call (as needed) with their BetterBrains coach. Based on the evaluation of the RESPOND program [23], we estimate that intervention group participants will receive an average of 8 hours of intervention delivery (4 hours every 6 months). Participants assigned to the intervention group will also receive monthly updates on general news about dementia and general psychoeducational health material about dementia risk reduction for as long as the trial is active (i.e., at least 24 months).
Intervention description as per TIDieR [47]
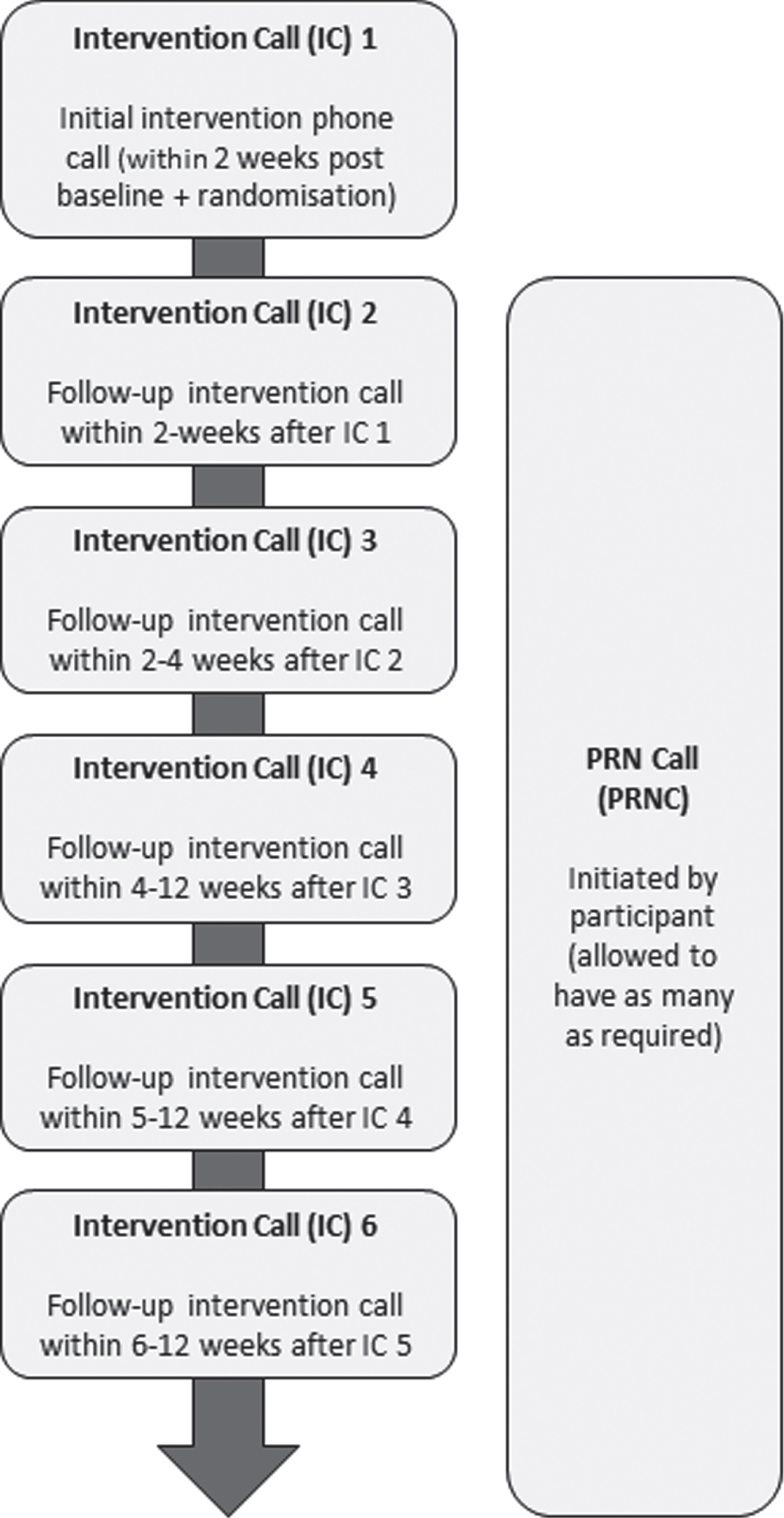
Call schedule for intervention participants.
By leveraging existing community services and tailoring the intervention to each participant, we ensure that we maximize the likelihood for engagement, that lifestyle modifications undertaken have the highest chance of long-term adherence, and that ultimately, cognitive function will be preserved for at-risk individuals.
Control
Participants assigned to the control group will receive monthly updates on general news about dementia, and general psychoeducational health material about dementia risk reduction for as long as the trial is active. Material will simultaneously be available on the BetterBrains website and smartphone app. Control group participants will not receive personalized information about their risk profile or personalized intervention recommendations including phone calls with the BetterBrains coaches. After completing their risk assessment at baseline, they will only receive mention of the number of risk factors for dementia that apply to them, based on their responses.
Follow-up assessments
Twelve and 24 months after baseline, all participants, irrespective of group allocation, will be notified to complete follow-up assessments (surveys and cognitive testing). The assessment schedule for the follow-up visits is outlined in Table 4. At each follow up visit (i.e., 12 and 24 months), participants will repeat the risk assessment completed at screening and the baseline questionnaires and cognitive testing undertaken at sign up (i.e., all questionnaires, apart from the inclusion/exclusion screening specific questions, presented to the participant up until the point of randomization). A total of 5 reminder notifications will be sent to participants when each assessment is due, provided it is yet to be undertaken.
Assessment Schedule for 12- and 24-month Follow-Up Assessments
BetterBrains smartphone application
All participants with a smartphone will also be asked to download the BetterBrains smartphone application. This is an optional study component that will provide a smoother experience. Participants without a smartphone will still be able to participate, and all notifications and assessments sent through the app will be made available through the website. The BetterBrains app will be used to provide psychoeducational material about dementia risk reduction, supplement intervention participants’ contact with their BetterBrains Coach, and to enhance the overall trial experience. For both groups, participants will have access to psychoeducational material about dementia risk reduction. In the intervention group, participants will also be sent regular notifications and reminders to check-in on their recommended intervention, whether they have experienced any barriers to engaging in their recommended intervention, and whether they would like to schedule a call with their BetterBrains Coach. Participants will receive these notifications weekly from their first intervention phone call up until week 52 of the intervention. From Months 12–24, these notifications will be sent monthly (option to speak with a coach will no longer be available from Month 12 onwards).
Adverse and serious adverse event reporting
Any unexpected, untoward event that occurs during the trial will be recorded in an SQL database and reported in line with the National Health and Medical Research Council (NHMRC) guidelines on safety monitoring and reporting. An adverse event is defined as any untoward medical occurrence. A serious adverse event is defined as any untoward medical occurrence that 1) results in death, 2) is life-threatening, 3) requires inpatient hospitalization or prolongation of existing hospitalization, 4) results in persistent or significant disability/incapacity, or 5) is a congenital anomaly/birth defect.
When a participant reports an event to a BetterBrains coach or research assistant, the reporting process begins (see Fig. 3 for a flow-chart of the adverse/serious adverse event reporting process). A rostered doctor within the medical management team (Yassi, Brodtmann, or Bush) will review the event, including 1) the date of the report, 2) details of the event, 3) a description of the adverse event, and 4) relevant medical history and medications. The medical management team are blinded to participant group and will be notified of the event by a research assistant, rather than a BetterBrains coach. Finally, an emergency protocol is in place should a participant report an urgent medical or mental health crisis, advising them to attend their GP or local emergency department, or, if not possible, to ring 000 (emergency services) immediately.
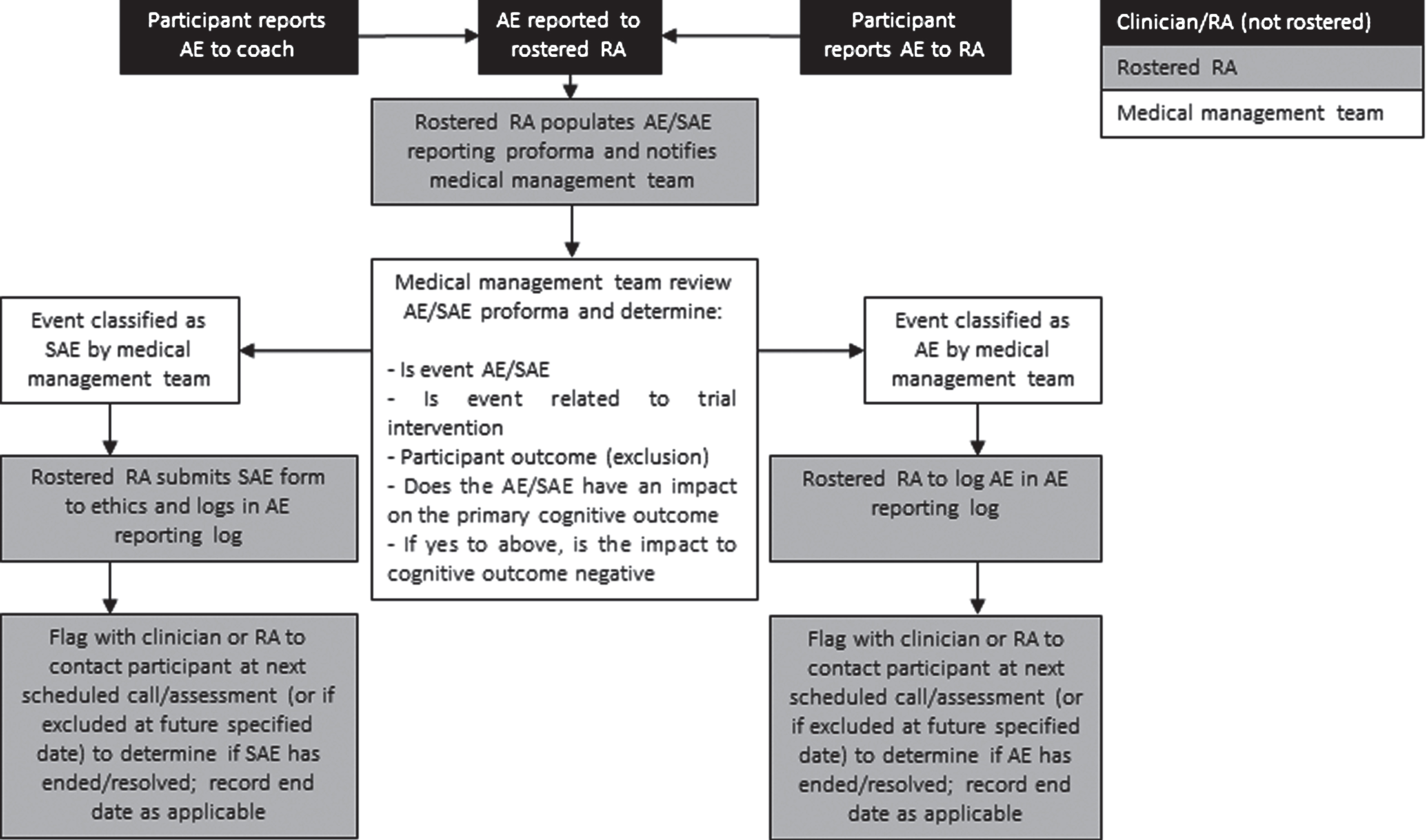
Adverse and Serious Adverse Event Reporting Process.
Data collection
Questionnaires and self-report surveys
The assessment schedule for this study is outlined in Tables 1 3 and consists of a set of validated questionnaires which assess participants’ motivation to change, depression, anxiety, and stress levels, subjective ratings of cognitive function, social engagement, general health, sleep quality, engagement in physical activity, work productivity, health literacy, menopausal symptoms (for women), resilience and perceived risk of dementia. The questionnaires will be presented to participants in their published and validated forms.
Self-report data will also be collected from participants in the form of demographic and health and family history surveys. The following
Cognitive testing
Unsupervised cognitive testing will be carried out using the Cogstate Brief Battery (CBB), the Cogstate iDSST Medicines, and the Online Repeatable Cognitive Assessment (ORCA) battery. Instructions and delivery of these tests have been designed and optimized for unsupervised, online assessment [36, 51], and have demonstrated sensitivity to AD-related cognitive change [25, 52].
The CBB has a game-like interface which uses playing card stimuli and requires participants to provide “Yes” or “No” responses. The CBB consists of four tests: Detection (DET), Identification (IDN), One Card Learning (OCL), and One-Back (OBK). These tests have been described in detail previously [34, 52]. Briefly, DET assesses psychomotor function, and IDN assesses visual attention. The primary outcome for both DET and IDN was reaction time in milliseconds (speed). OCL assesses visual learning, and OBK assesses working memory and attention. The primary outcome measures for OCL and OBK was proportion of correct answers (accuracy).
The Cogstate International Daily Symbol Substitution Test (IDSST) Medicines is a measure of complex attention (processing speed) and simple executive function. In this test, a key is provided at the top of the screen. This key shows nine pairs, each consisting of a single medicine (capsule, tablet, pill) and calendar date and month (e.g., FEB 1, FEB 2, FEB 3, FEB 4, FEB 5, FEB 6, FEB 7, FEB 8, and FEB 9). Each medicine has a unique shape and color, and each corresponds to a different date (e.g., a round red tablet may be allocated to FEB 3). In the middle of the screen, an empty pill box is presented, and a date is shown at the top of the pill box. At the bottom of the screen, the same medicines as those shown in the key are presented. The participant/subject is asked to select the medicine form the set at the bottom of the screen that corresponds to the date highlighted on the pill box in the center of the screen based on the correct pairing between medicine and date shown in the key (e.g., if FEB 3 is the label on the empty box in the middle of the screen, the subject should select the red tablet). At any decision, the four previous and four upcoming trials are also displayed, on either side of the current date. The software records each selection as correct or incorrect, and once a response is made it cannot be changed. The medicines are selected randomly from a repository of 100 stimuli. Their position in the key showing pairings of medicine and date is also randomized. After the practice, the subject is allowed 120 s to make as many correct responses as possible. The primary outcome for the IDSST-medicines is the total number of correct responses made in 120 s.
ORCA is a paired associate learning task that involves learning the correct pairing of a visually presented Chinese character (e.g., 莓) and the audio English translation of the word (i.e., berry) [25, 36]. The presentation of “correct” pairings will occur over the course of 6 training blocks (one per day) ten times more often than “incorrect” pairings (e.g., chair and 莓). Each trial will consist of a visually presented Chinese character, presented for 1000 ms after the onset of the auditory presentation of the English word. After the characters are presented, participants will have to press one of two keys on a laptop to indicate whether the pairing was correct or not. The instruction will be to “decide if the English word and Chinese characters match or not”. Through this process, participants will have the opportunity to learn a range of commonly used Chinese characters. This task will take a maximum of 15 min to complete. Participants will be required to complete 6 blocks of testing (90 min in total). In order to do this test, participants should not be proficient in Chinese (i.e., intermediate level onwards). In order to account for this, we will ask “How proficient are you with Chinese characters?” The responses will be multiple choice: “Not at all”, “Beginner level”, “Intermediate level”, “Advanced level”, or “I am fluent/It is my first language”. If the participant selects “Intermediate level”, “Advanced level”, or “I am fluent/It is my first language”, the participant will not complete the ORCA task. Based on HBP estimations [24], we anticipate that ∼90%of participants will be eligible to undertake this task. In addition to the five reminder emails sent as part of the baseline, 12- and 24-month assessment protocol, participants with low adherence rates on the ORCA task (e.g., < 80%) will also be sent an additional reminder email and SMS at 21 days. This will allow participants an additional 7 days to complete the task prior to the 28-day cut-off.
Saliva sampling
All participants that proceed to randomization will also be asked to provide a sample of saliva for genetic testing. After randomization, participants will receive via post at their residential address a Genotek Oragene (OG-500) 2 mL saliva kit in a pre-paid envelope. The DNA tubes will be coded (deidentified) at the Turner Institute before being sent to the participant in the post. Participants will be instructed to return the saliva sample via pre-paid Registered Post to our research team at the Turner Institute for Brain and Mental Health. Samples will be temporarily stored at the Turner Institute. At the end of the trial, a commercial vendor will be identified to conduct genotyping. All samples will be deidentified before being sent for analysis. SNPs for APOE (rs429358, rs7412) and those identified to be associated with risk of AD or dementia will be analyzed [53, 54].
Clinical information
Information about intervention group participants’ engagement in behavior change strategies related to their goals will be collected from two sources: 1) coach phone calls and 2) the BetterBrains smartphone app. Coaches will complete an eCRF during their scheduled phone calls with intervention participants which will capture relevant behavior change information including: whether the participant has made progress in meeting their goal, barriers and facilitators related to goal progress, and strategies used to affect behavior change. The BetterBrains smartphone app will send participants ‘prompts’ in the form of notifications weekly (first 12-months of the trial) and monthly (second 12-months of the trial) with questions asking about goal progress, barriers and facilitators.
Participant’s engagement in behavior change will also be captured through their responses to questionnaires and surveys administered at the outcome assessments.
Statistical analysis
Outcome analyses will be conducted following intention-to-treat principles. All outcomes and analyses are prospectively categorized as primary, secondary, or exploratory. Differences in all endpoints between the two study groups will be tested independently at the two-tailed 0.05 level of significance. All estimates of treatment effects will be presented with 95%confidence intervals (CIs). No formal adjustments will be undertaken to constrain the overall Type I error associated with the secondary, tertiary, and exploratory analyses. Their purpose is to supplement evidence from the primary analysis to more fully characterize the treatment effect. Results from the secondary, tertiary, and exploratory analyses will be interpreted in this context. Descriptive statistics will be generated for each of the measures used in the study.
The primary outcome will be analyzed using an adjusted logistic regression model with the achievement of a favorable cognitive outcome at 24 months (yes/no) as the dependent variable and the treatment group as the independent variable.
Secondary, tertiary, and exploratory endpoints will be analyzed using appropriate regression models. Exploratory longitudinal analyses will be conducted using linear mixed models (LMM) with random slopes and random intercepts to determine any between-group differences in rates of change in objective and subjective cognitive function, subjective ratings of general health and quality of life, health literacy, motivation to change behavior for dementia risk reduction, and perceived risk of dementia. We will also explore the moderating effects of APOE ɛ4, the nature and number of risk factors, and participants’ readiness to change on cognitive outcomes. The details of the statistical analysis will be summarized in a separate Statistical Analysis Plan prior to the lock of the trial data.
COVID-19 related considerations
To ensure the safety and wellbeing of our research participants and to preserve trial integrity in the context of the COVID-19 pandemic, consideration has been given to intercurrent events related to COVID-19 as well as any adequate provisions that may be required to mitigate the potential impact of COVID-19 on trial outcomes (Table 5 details these considerations).
COVID-19 Impact
DISCUSSION
This RCT is, in its entirety, a remote clinical trial through its use of web-, smartphone-, and telephone-based platforms to assess, monitor, and deliver the intervention to participants. The aim is to test the hypothesis that the BetterBrains intervention program will prevent cognitive decline in community-dwelling, middle-aged adults with a family history of dementia. The BetterBrains program targets known modifiable risk factors for cognitive decline and dementia through a person-centered, risk factor management online intervention. As modifiable risk factors rarely present in isolation, our multi-risk factor approach has the potential to maximize the anticipated benefits of modifying lifestyle variables on reducing risk of cognitive decline.
The online nature of the trial reduces the burden on participants as attendance at a clinical research facility is not required and completion of cognitive tests and surveys can be completed at a time of convenience over several days. It also facilitates the recruitment and participation of regional and rural participants who are often underrepresented in clinical research due to geographic barriers. As a substantial proportion of Australians aged 40–70 years have access to the Internet via a computer, tablet or phone, this mode of assessment will allow us to reach a wide demographic of individuals. We have successfully utilized this method of recruitment and assessment in the Healthy Brain Project [24]. If successful, there will be an opportunity to apply the testing and intervention methods more broadly as part of clinical care for other patient groups such as chronic disease.
TRIAL STATUS
The trial plans to recruit from June 2021 to June 2022.
Footnotes
ACKNOWLEDGMENTS
This trial is funded by a National Health and Medical Research (NHMRC) Boosting Dementia Research Initiative grant (GNT1171816). YY Lim is supported by an NHMRC Career Development Fellowship (GNT1162645). D Ayton is supported by an NHMRC Investigator Grant (GNT1195357). M Pase is supported by a Heart Foundation Future Leader Fellowship (GNT102052). R Buckley is supported by a National Institutes of Health K99-R00 award (K99AG061238). Participants will be recruited from the Healthy Brain Project (healthybrainproject.org.au) and from the community. The Healthy Brain Project is managed by YY Lim, M Pase, N Yassi and R Buckley, and is funded by the National Health and Medical Research Council (GNT1158384, GNT1147465, GNT1111603, GNT1105576, GNT1104273), the Alzheimer’s Association (AARG-17-591424, AARG-18-591358, AARG-19-643133), the Dementia Australia Research Foundation, the Bethlehem Griffiths Research Foundation, the Yulgilbar Alzheimer’s Research Program, the National Heart Foundation of Australia (102052), and the Charleston Conference for Alzheimer’s Disease.