
Abstract
Background:
Default mode network (DMN) dysfunction is well established in Alzheimer’s disease (AD) and documented in both preclinical stages and at-risk subjects, thus representing a potential disease target. Multi-sessions of repetitive transcranial magnetic stimulation (rTMS) seem capable of modulating DMN dynamics and memory in healthy individuals and AD patients; however, the potential of this approach in at-risk subjects has yet to be tested.
Objective:
This study will test the effect of rTMS on the DMN in healthy older individuals carrying the strongest genetic risk factor for AD, the Apolipoprotein E (APOE) ɛ4 allele.
Methods:
We will recruit 64 older participants without cognitive deficits, 32 APOE ɛ4 allele carriers and 32 non-carriers as a reference group. Participants will undergo four rTMS sessions of active (high frequency) or sham DMN stimulation. Multimodal imaging exam (including structural, resting-state, and task functional MRI, and diffusion tensor imaging), TMS with concurrent electroencephalography (TMS-EEG), and cognitive assessment will be performed at baseline and after the stimulation sessions.
Results:
We will assess changes in DMN connectivity with resting-state functional MRI and TMS-EEG, as well as changes in memory performance in APOE ɛ4 carriers. We will also investigate the mechanisms underlying DMN modulation through the assessment of correlations with measures of neuronal activity, excitability, and structural connectivity with multimodal imaging.
Conclusion:
The results of this study will inform on the physiological and cognitive outcomes of DMN stimulation in subjects at risk for AD and on the possible mechanisms. These results may outline the design of future non-pharmacological preventive interventions for AD.
Keywords
INTRODUCTION
The disruption of specific large-scale networks is implicated in the pathophysiology of Alzheimer’s disease (AD) [1]. Reduced default mode network (DMN) connectivity is a well-established feature in AD, showing topographical overlap with amyloid pathology and neurodegeneration [1]. The regions with the most consistent connectivity reduction are the posterior cingulate cortex (PCC) and the precuneus [2, 3]. These DMN areas together with the bilateral hippocampi are critically involved in episodic memory and self-referential thoughts, whose impairment represents a core clinical feature of AD [4]. DMN disconnection is observed in early AD stages, e.g., subjects with mild cognitive impairment [5, 6] and cognitively normal older adults at risk for AD due to the presence of amyloidosis [7, 8] or susceptibility factors such as the apolipoprotein E (APOE) genotype. The APOE ɛ4 allele is the strongest known susceptibility gene for AD and the inheritance of one copy confers a 3-fold increased risk of dementia [9]. APOE ɛ4 carriers show DMN abnormalities similar to those observed in AD patients, i.e., reduced connectivity in the PCC/precuneus [10, 11] and increased connectivity in frontal areas [11]. DMN abnormalities in cognitively healthy older adults APOE ɛ4 carriers might represent the earliest possible changes in the AD spectrum [12, 13] and thus represent a potential target for preventive interventions in AD.
Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive stimulation technique capable of modulating brain network dynamics through mechanisms of neural plasticity [14]. rTMS can induce long-lasting changes in network connectivity through the repeated delivery of a magnetic impulses over specific cortical areas. Stimulation of the target area generates neural activity that propagates to connected regions and that can be assessed through resting-state functional MRI (rs-fMRI) or concurrent registration of the electroencephalography (EEG) during the application of single pulses of TMS [15, 16]. The combination of rTMS with rs-fMRI and TMS-EEG has been successfully used to investigate connectivity properties within targeted functional networks in healthy populations [17] and AD patients [18].
There is preliminary evidence in healthy populations that rTMS applied to key nodes of the DMN can modify network connectivity and improve the associated cognitive functions. In healthy young adults, a number of studies applied high-frequency rTMS for five consecutive days over the lateral inferior parietal cortex (a key node of the DMN cortical-hippocampal connection), finding increased functional connectivity between the stimulated region and the hippocampus in the active group compared with the control group, as well as an improvement in associative memory [19–21]. These results were subsequently replicated with protocols of three or four days of stimulation [22]. Recent studies demonstrated the efficacy of rTMS in modulating DMN connectivity and episodic memory in healthy older subjects and early AD [23–25]. Interestingly, a study by Peña-Gomez and colleagues (2012) reported the effects of a single session of rTMS on DMN connectivity and memory in prodromal AD also accounting for APOE genotype [26]. While memory improved in both APOE ɛ4 carriers and non-carriers, only ɛ4 carriers showed functional changes in the DMN indicative of a normalization of its connectivity [26]. Whether rTMS can be used to modulate DMN connectivity at preclinical AD stages, however, remains largely unexplored. In principle, rTMS similarly to other interventions may be more effective if applied at earlier stages, when brain plasticity is higher and pathological changes are limited. A general aspect of AD pathophysiology is the impairment of plasticity mechanisms [27, 28] and the APOE ɛ4 allele is also known to affect synaptic dysfunction [29, 30]. Moreover, AD patients carrying the APOE ɛ4 allele show greater cortical plasticity impairment and worse clinical outcomes over time than non-carriers [31]. The application of rTMS at preclinical stages may therefore provide the optimal window to exploit relatively preserved plasticity processes and effectively modulate network dynamics.
Based on this background, this study aims at testing the effects of DMN stimulation in cognitively normal older subjects at increased risk of AD due to the presence of the APOE ɛ4 allele. By combining neuroimaging with rTMS, we will identify the DMN individual targets based on resting-state fMRI data and will assess the effect of stimulation on network connectivity and cognition. Following stimulation, we expect to observe an improvement in DMN connectivity (as assessed with MRI and TMS-EEG) and memory performance (as assessed with a face-name associative memory task) in APOE ɛ4 carriers. APOE ɛ4 non-carriers will be included as a reference group to assess whether 1) rTMS effects will be similar between carriers/non-carriers or weaker in carriers, e.g., due to greater cortical plasticity impairment [30, 31]; 2) rTMS will normalize network abnormalities in carriers, i.e., if this protocol will restore a DMN connectivity pattern more similar to that of non-carriers at baseline, as in [26]. Finally, by taking advantage of MRI and TMS-EEG, we plan to unravel the mechanisms underlying DMN modulation by assessing associations with additional neuroimaging and neurophysiological measures.
METHODS
Participants
Sixty-four participants without cognitive deficits, both carriers (n = 32) and non-carriers (n = 32) of the APOE ɛ4 allele, will be enrolled from the IRCCS Saint John of God – Fatebenefratelli of Brescia (FBF-BS) memory clinic (relatives of patients with dementia, participants to ongoing research studies on the natural history of cognitive decline) and the community through public dissemination of the study (i.e., websites; information brochure).
Inclusion criteria will be age ≥60 years and ability to provide written informed consent. Exclusion criteria will be a Mini-Mental State Examination (MMSE) score ≤24 at the screening visit; pathological scores in at least two standardized cognitive tests administered during the screening visit; known carriers of an autosomal dominant genetic mutation associated to AD (APP, PSEN1, PSEN2); presence of any neurological, psychiatric or medical conditions not compatible with the study (history of psychiatric or neurologic diseases such as AD, frontotemporal dementia, Parkinson’s disease, multiple sclerosis, alcohol/drug abuse, epilepsy, headache); pharmacological therapy not compatible with the study (some classes of psychotropic drugs, antivirals, anticancer drugs, antihistamines, antibiotics); usual contraindications for MRI and rTMS [32]; any evidence of intracranial pathology which may affect cognition or rTMS procedures (brain tumors, aneurysm or arteriovenous malformations, stroke, cortical vascular lesions, severe cerebrovascular disease); concurrent participation in interventional trials.
Study protocol
Figure 1 summarizes the study design and Table 1 summarizes the protocol’s procedures at each visit. After the screening phase, in which the participants’ eligibility will be evaluated and a blood sample will be collected, enrolled subjects will be randomly assigned to one of two groups (active versus placebo rTMS). Then, they will undertake the baseline evaluation [T0], consisting of a cognitive assessment, a multimodal neuroimaging exam, and a TMS electroencephalography coregistration (TMS-EEG) exam. After T0, participants will undergo 4 daily sessions of rTMS. After the rTMS sessions, each participant will perform the follow-up visit [T1], carrying out the same procedures performed at T0 (cognitive, MRI, TMS-EEG assessment). Two months after the rTMS sessions [T2], participants will undergo the cognitive assessment again to evaluate potential delayed effects of rTMS on cognition.
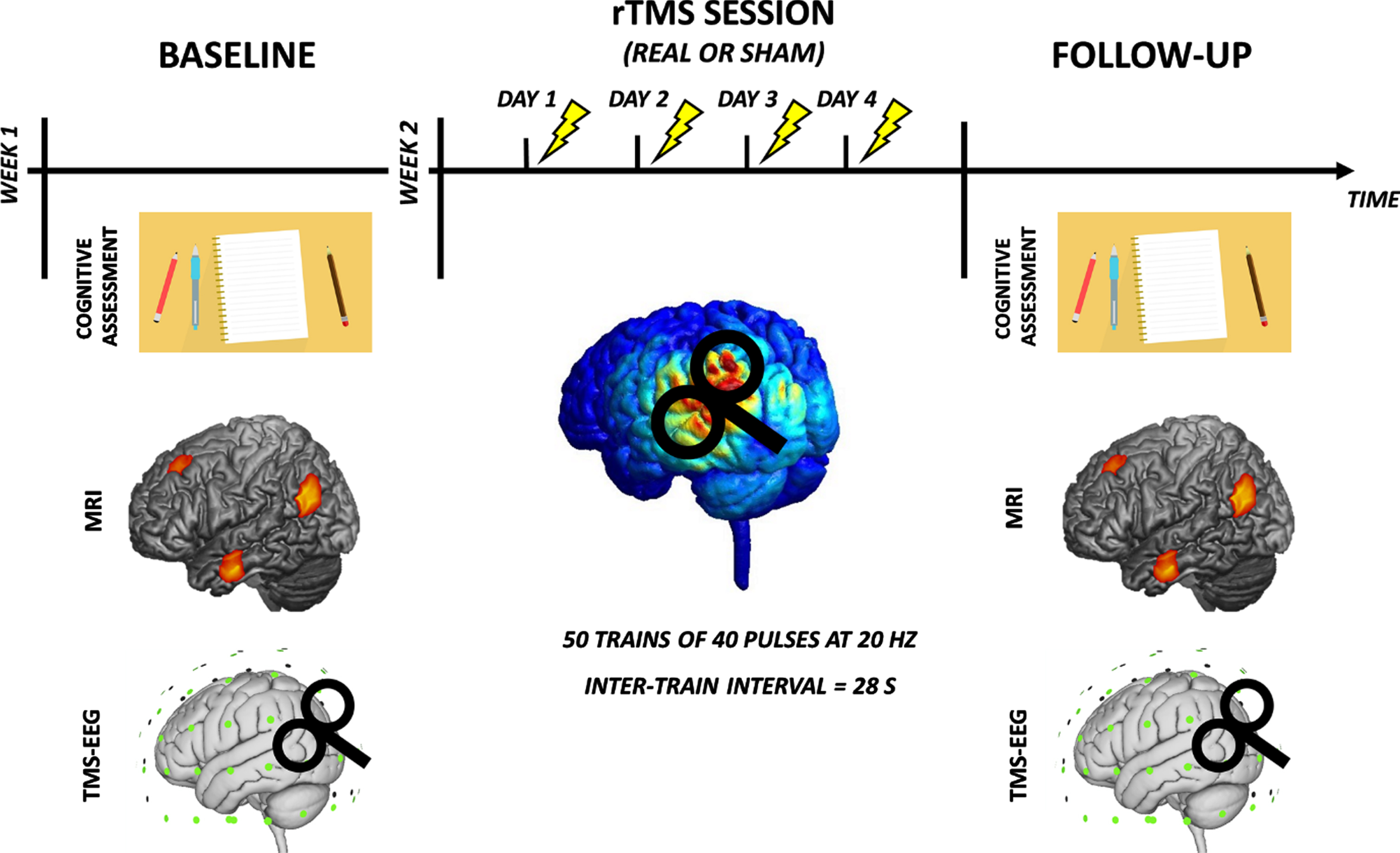
Study design: during the first week, the enrolled subjects will undertake the baseline evaluation including a multidomain cognitive assessment, multimodal neuroimaging (MRI) exam, and a transcranial magnetic stimulation - electroencephalography coregistration (TMS-EEG) exam. In the second week, the participants will undergo 4 daily sessions of repetitive TMS (real or sham, depending on the assignment) and a follow-up visit (multidomain cognitive assessment, multimodal MRI, and TMS-EEG exams).
Schedule of visits
The study has been approved by the Ethics Committee of the FBF-BS (approval date 15/05/2019; Number 41-2019).
Screening
During the screening visit, the study protocol will be discussed, and information will be given to subjects to allow them to decide whether to take part in the study or not. After signing the informed consent, the eligibility criteria will be examined. Sociodemographic and medical information will be collected, and a clinical and cognitive assessment will be done. Global cognition will be examined using the MMSE [33]; specific cognitive domains will be tested using a complete cognitive battery assessing verbal and visual memory, visuospatial/visuoconstructive abilities, attention, language, and executive functions. The presence of potential depressive symptoms will be evaluated with the Geriatric Depression Scale (GDS) [34], a 30 items self-report assessment used to identify depression in the elderly. Participants will also complete two questionnaires for evaluating any contraindication for MRI (Supplementary Material 1) and rTMS (Supplementary Material 2). For eligible subjects, a blood sample will be collected for APOE genotyping, when not already available, according to previously described procedures [35]. Briefly, we will use the quantitative polymerase chain reaction (qPCR) method using the StepOnePlus® equipment (ThermoFisher). Two ApoE single-nucleotide polymorphisms (SNPs), rs429358 (C___3084793_20) and rs7412 (C____904973_10), will be determined using TaqMan® Genotyping assays (Applied Biosystems; Thermo Fisher Scientific, Inc.), according to the manufacturer’s protocols. SNPs will be analyzed with TaqMan Genotyper Software (Applied Biosystems; Thermo Fisher Scientific), based on an algorithmic approach to automatically assign a genotype.
Cognitive assessment
We will investigate the participants’ global cognition and specific cognitive domains using the MMSE, the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) [36], and the Free and Cued Selective Reminding Test (FCSRT) [37]. The RBANS is a brief and complete neuropsychological battery, composed of multiple forms of identical difficulty, each divided into 12 subtests to be administered individually. It evaluates five different cognitive domains: attention, language, visuospatial/visuoconstructive ability, immediate memory, and delayed memory. The FCSRT is an episodic memory test that evaluates immediate and delayed free-recall and cued-facilitated immediate and delayed recall. Briefly, in the learning phase, participants will be asked to provide the name of 16 simple pictures with a semantic cue; in the recall phase, participants will be asked to recall (spontaneously and through a semantic cue for those items not retrieved) the 16 pictures three times, interspersing the trials with a 20-s interference task. After a delay of 30 min, participants will be asked to recall the 16 pictures without any cues. We will administer a different form of the RBANS and the FCSRT to avoid practice effects during each visit. Some of the above tests (the total recall score from the FCSRT, the delayed recall score of the logical memory and the symbol digit substitution subtests from the RBANS battery, the MMSE total score) will be used to compute the preclinical Alzheimer cognitive composite (PACC) score [38], a composite measure that has been proposed to be sensitive to early disease-related changes in preclinical populations.
Participants will also undergo two tests of the CANTAB battery [39] before TMS-EEG coregistration: the Paired Associative Learning test (PAL), which measures episodic memory, to assess cognitive correlates of DMN activity, and the Spatial Working Memory test (SWM), which assesses executive functions, to assess cognitive correlates of the frontoparietal network (FPN). The two tests take about 15 min to administer.
Participants will also be asked to complete the Cognitive Reserve Index questionnaire (CRIq) [40] and the Cognitive Reserve Scale (CRS) [41] to assess the cognitive reserve accumulated by individuals through their lifespan. CRIq and CRS will be administered during the baseline visit only.
Neuroimaging protocol
MRI scans will be acquired on a 3T Siemens Skyra scanner equipped with a 64-channels coil at the Neuroradiology Unit of the Spedali Civili Hospital in Brescia, Italy. The MRI protocol will include the following sequences: 1) resting-state fMRI (rs-fMRI) scan to assess DMN functional connectivity (TR = 1000 ms, TE = 27 ms, flip angle = 60°, voxel = 2.1 mm isotropic, 70 slices, 600 volumes); 2) fMRI with an associative memory task (task-fMRI) to analyze memory performance and neural activity (TR = 1000 ms, TE = 27 ms, flip angle = 60°, voxel = 2.1 mm isotropic, 70 slices); 3) diffusion tensor imaging (DTI) for the study of structural connectivity (TR = 4100 ms, TE = 108 ms, voxel = 1.8 mm isotropic, 75 slices, b0 = 0 s/mm2, b = 1200 s/mm2, 64 directions); 4) MPRAGE (TR = 2300 ms, TE = 2 ms, flip angle = 9°, voxel = 1 mm isotropic, 176 slices; 5) 3D FLAIR (TR = 5000 ms, TE = 393 ms, voxel = 1 mm isotropic, 192 slices).
fMRI face-names associative memory task
Memory performance will be assessed on MRI using a face-name associative memory task. The associative memory task will consist of a series of images associated with words (face-name pairs), and the participant will be requested to memorize the associations. Memory performance will be assessed with a mixed block and event-related face-name association paradigm adapted from previous paradigms [42, 43]. As visual stimuli, we will use a series of novel faces (i.e., faces that are unfamiliar to the subject) randomly paired with fictional first names. The faces will be taken from a public dataset, the Park Aging Mind Laboratory Face Database [44] and will be chosen based on direct gaze, white ethnicity, and neutral facial expression. The age range will be 19 to 93 years and an equal number of males and females will be selected. First names will be chosen from a list of the most popular Italian names drawn from the web. Names will be randomly paired with faces. We will create two separate sets of stimuli, one for baseline (T0) and one for follow-up (T1). Names and faces will be uniquely assigned either to the baseline or follow-up experiment to avoid practice effects. fMRI task will be divided into 12 separate blocks of face-name encoding pairs, each followed by a block of face-name recall pairs. Between each trial, task instructions for encoding or recall will be displayed. Each encoding block will comprise 8 faces (4 females and 4 males, randomly selected), with a fictional first name underneath the face in white letters. Each face-name pair will be presented for 5000 ms against a black background and separated from the subsequent face-name pair by a randomized fixation trial (a white crosshair on a black background) of 1000 –2000 ms (mean inter-trial interval = 15007 ms). Each encoding block will be followed by a recall block, during which the same faces will be presented again in random order for a 5000 ms duration each (inter-trial-interval of 1000–2000 ms), with two names presented below each face (correct name versus distractor). Via button press, participants will select the correct name associated with the face during the encoding block using two fingers of their dominant hand. No feedback regarding accuracy will be given. The correct and distractor names will be presented in random order. Half of the recall tasks will include a new distractor name (i.e., a name not previously seen). In contrast, the remaining half will include a distractor name associated with another face in the same block. For each recognition block, the choice of associating a face with a new name or a name already shown in that block will be made at random. Correct responses during the recall block will be classified as successful recall, incorrect responses as incorrect recall. Based on responses during the recall block, the corresponding encoding trials will be classified as successful encoding or incorrect encoding, respectively. Task accuracy will be measured as the number of successfully recalled face-name pairs relative to the total number of face-name pairs shown. Overall, the subjects will see 96 different faces and 144 names with balanced male/female face and name frequencies. Before fMRI scanning, all subjects will be trained for the task on a local notebook using face-name pairs not included in the fMRI task.
rTMS target extraction
The baseline rs-fMRI sequences will be used to extract individual DMN spatial maps and identify individual target coordinates for rTMS. The target for DMN stimulation will be the left inferior parietal lobe (IPL) node of the DMN, in line with previous studies [19–22]. The procedure for target coordinates extraction is described in detail elsewhere [45]. Briefly, the DMN will be extracted with the MELODIC software [46] through an independent component analysis (ICA). The DMN will be identified using a template matching procedure with a published DMN template [47]. The DMN spatial map will be decomposed into clusters and the largest cluster in the left IPL cortex will be identified. The IPL cluster local maxima will then be extracted as candidate targets. Within the pool of extracted local maxima, the optimal target for rTMS will be selected after excluding points shared with adjacent networks (i.e., the FPN) and falling outside the gray matter (i.e., in the white matter or the cerebrospinal fluid). This procedure will ensure accuracy when targeting the DMN meanwhile minimizing the risk of off-target stimulation [45]. Finally, the following coordinates will also be extracted as control areas for TMS-EEG recordings (see ‘TMS-EEG protocol’ section): the right IPL node of the DMN, the left and right DLPFC nodes of the FPN. The FPN will be extracted following the same procedure described above but using the executive control network as the template [47]. FPN targets will be selected after excluding points falling outside the gray matter or shared with the DMN.
TMS-EEG protocol
Measures of functional connectivity will be collected by recording the propagation of the cortical activation induced by single-pulse TMS on EEG, i.e., TMS-EEG coregistration, as done in previous AD studies [18, 24].
TMS will be delivered as “standard biphasic” pulses using a figure-of-eight coil (MagVenture C-B60 coil) of the MagVenture MagPro X100 incl. MagOption. The coil will be positioned by means of a stereotaxic neuronavigation system (SofTaxic, EMS, Italy) over five areas of interest: 1) the target of the stimulation in the rTMS sessions (left parietal DMN node); 2–5) four control areas: the contralateral DMN node, the left and contralateral DLPFC node of the FPN, the vertex (where sham stimulation will be applied to control for possible sensory confounds associated with the TMS). In this condition the coil will be separated from the EEG cap by a 3 cm spacer. Except for the vertex, all the targets will be individually defined from rs-fMRI data, as described in the ‘rTMS t arget extraction’ section. For every participant, the optimal coil position and orientation for the target coordinates will be assessed using the software SimNIBS [48] and the ‘auxiliary dipole method’ optimization procedure [49]. For each target area, 80 single-pulse TMS will be administered at 110%of the resting motor threshold (RMT) with inter-stimulus interval of 1500–3000 ms and recharge delay at 1000 ms. RMT will be defined as the minimum stimulus intensity producing low-intensity responses (≥50 mV) of the first dorsal interosseous muscle of the right hand employing an adaptive staircase procedure [50]. To reduce sensory stimulation associated with TMS, a thin layer of foam will be placed between the TMS coil and the EEG cap and white noise will be played through noise-canceling earphones [51].
A TMS-compatible EEG system (BrainAmp, Brain Products GmbH, Munich, Germany) will be employed to record EEG from 67 electrodes placed on the scalp according to the 10-10 international system, and vertical and horizontal electrooculogram (EOG). To minimize possible artifacts, previously described procedures will be used [52]. Reference and ground will be placed on the tip of the nose and on FPz, respectively. EEG will be recorded with sampling rate at 5 kHz, online bandpass filter at 0.1–1000 Hz and impedance below 5 kΩ.
Data analysis
Analysis of MRI data
Functional connectivity will be assessed in the network of interest (DMN) using ICA. Resting-state scans will be pre-processed according to standard procedures (i.e., motion correction, distortions correction, registration to standard space, bandpass filtering, nuisance regression, smoothing). The DMN will then be extracted with group-level ICA. DMN connectivity will be assessed with voxel-wise analysis [53]. Moreover, ROI-based analysis will be conducted to measure connectivity between core DMN nodes.
Task fMRI data will be analyzed to assess increases and decreases in the BOLD signal in response to the associative memory task. The condition of interest will be the recall of name-face pairs. Data will be analyzed using the Statistical Parametric Mapping software [54].
Structural connectivity will be analyzed on DTI images by assessing traditional microstructural integrity indices (fractional anisotropy, mean diffusivity, axial diffusivity, radial diffusivity) [55]. A ROI analysis will be used to measure diffusivity within the WM tracts connecting the major DMN nodes (i.e., the WM tracts connecting the IPL to the posterior cingulate cortex, the cingulum tract, and the parahippocampal tract).
Analysis of TMS-EEG data
Amplitude and latency of the TMS-evoked potentials (TEPs) in the first 80 ms after TMS will be analyzed as measures of effective connectivity. Indeed, TEPs reflect the secondary activation of remote regions connected to the stimulated area [56]. Accordingly, the amplitude and latency of TEPs are associated with measures of structural and functional connectivity between the stimulated area and the sources of the secondary activation [16, 57]. The transmission of the generated cortical signal is fast so that it is possible to record secondary remote responses in the contralateral hemisphere around 15 ms after stimulation [58]. Therefore, the first 80 ms after the TMS stimulation are highly informative for effective connectivity. Moreover, they are less prone to sensory artifacts [51].
First, TEPs will be extracted through a preprocessing pipeline that combines independent component analyses (ICA), SOUND [59], and SSP-SIR [60] to minimize artifacts [18]. Then, TEP components will be individuated with the collapsed localizer strategy [61]. Finally, latency and amplitude will be extracted for the individuated peaks for each participant and for each condition. Moreover, the time-frequency response induced by TMS will be analyzed in the natural frequency of the target area. Previous studies have shown that TMS stimulation produces local oscillatory responses that tend to have a specific frequency depending on the stimulated region [62]. Specifically, parietal areas resonate in low beta oscillations (13–20 Hz) and prefrontal areas resonate at higher frequencies (21–50 Hz) [63]. Here, we will individuate the natural frequency for each stimulated area and measure its power after TMS for each participant and for each condition. This measure is an index of cortical excitability and connectivity of the stimulated area.
rTMS stimulation sessions
Participants will be randomized to two study arms (1:1 ratio) - high-frequency (active) or placebo (sham) rTMS - using a covariate-adaptive randomization [64] procedure to ensure balance between sub-groups for relevant confounds (APOE ɛ4 status, age, sex).
The randomization will be performed by a statistician at the FBF-BS. Participants and researchers involved in the cognitive, imaging, and TMS-EEG assessment will be blind to group assignment upon the conclusion of follow-up. Only the researcher responsible for rTMS sessions will be aware of group assignment. Participants will be blinded to the rTMS protocol through the use of a sham coil.
Each patient will undergo 4 consecutive daily rTMS sessions, each one lasting about 25 min, in an outpatient setting at the FBF-BS. The rTMS sessions will be performed with a cooled figure-of-eight coil integrated with a neuronavigation system (NBT System 2, Nexstim Plc., Helsinki, Finland) and delivering biphasic pulses. The stimulation parameters will consist of 50 trains at 20 Hz lasting 2 s (40 pulses/train) interleaved by intervals of no stimulation (28 s), for a total of 2000 pulses per session, according to safety recommendations [32].
The target of stimulation will be the left IPL node of the DMN, as defined from individual rsfMRI (see ‘rTMS target extraction’ section). The sham condition will involve the same parameters, but a 3 cm spacer will be positioned under the coil to avoid the cortex’s stimulation while matching auditory sensations. The neuronavigation system will be exploited to define and monitor the position of the coil throughout each rTMS session. Coil orientation will be the same used in the TMS-EEG recording session and defined through the software SimNIBS (see ‘TMS-EEG protocol’ section). The intensity of the stimulation will be set based on the real-time determination of the mean intracranial electric field (V/m) value induced by a TMS pulse in the target area as estimated in the adopted neuronavigation system. Specifically, the electric field induced in the motor area at resting motor threshold will be calculated in the first rTMS session following an adaptive staircase procedure (see TMS-EEG coregistration); then this value will be applied as cutoff when setting the rTMS intensity for the left IPL area. Following previous studies adopting a similar procedure, we expect that the induced electric field within M1—and thus IPL—will be of about 90 V/m (e.g., [65–67]). This will allow us to better account for the variability of the scalp-to-cortex distance between brain regions and between different subjects, which is a potential confounding variable for TMS effectiveness [68, 69].
Side effects will be monitored through a structured questionnaire [70]. The questionnaire will be administered at the end of each rTMS session to monitor the perceived discomfort induced by the rTMS procedure (Supplementary Material 3).
Outcome measures
The main neuroimaging outcome measure will be the change in DMN connectivity on rs-fMRI following active rTMS compared to placebo in APOE ɛ4 carriers. The main neurophysiological outcome will be the changes in amplitude and latency of TEPs following active rTMS compared to placebo in APOE ɛ4 carriers. The main cognitive outcome will be the change in associative memory performance on task fMRI following active rTMS compared to placebo in APOE ɛ4 carriers. The magnitude of rTMS effects will be assessed testing the changes in the above measures following active rTMS in APOE ɛ4 carriers compared to non-carriers. Finally, exploratory cognitive outcomes will be the change on global cognition (MMSE), standard cognitive tests (RBANS and CANTAB batteries), and PACC score following active rTMS compared to placebo in APOE ɛ4 carriers.
To elucidate the mechanisms underlying DMN modulation, we will collect measures of neuronal activity/excitability and structural connectivity and we will investigate the following outcomes: changes in neuronal activity (task-fMRI), cortical excitability and connectivity (TMS-EEG), axonal integrity (DTI) following active rTMS compared to placebo.
Study power and planned statistical analysis
Sample size
The minimum sample size to ensure a sufficient power for the defined aims of this study was determined by taking into account previously published stimulation studies in healthy populations. In particular, Wang et al. [19] reported an increase in IPL-hippocampal connectivity following active rTMS stimulation in a sample of 16 young subjects (evaluated twice, both in active and sham rTMS condition), while Antonenko et al. [71] reported an increase in DMN connectivity following active electrical stimulation in a total sample of 40 young and older subjects (20 per experimental group) analyzed with a repeated measures ANOVA model.
In our case, the sample size is higher than the previous studies (n = 64 subjects; n = 32 per experimental group), so we expect to detect similar or even higher effects using a repeated measures ANOVA model. In particular, Antonenko et al. [71] reported an arm x time interaction effect equal to F (1,34) = 4.86, p = 0.034. With these parameters, assuming a power of about 0.8 and a correlation between repeated measures equal to 0.5, the effect size is approximately 0.26. With our sample size (n = 64, with two arms and two time points), with the same effect size of 0.26 we would obtain a power of 0.98. Consequently, assuming for our study a power of 0.8, we could get as significant an even lower effect size (equal to about 0.19, i.e., a 27%reduced effect size) than the one found in Antonenko et al. [71], and using a more powerful technique (i.e., magnetic versus electrical stimulation). This computation ensures thus both feasibility and good power of our study.
Statistical analysis
The variables of interest (imaging, neurophysiological and task-related cognition) will be analyzed with repeated measures ANOVA models or Linear Mixed model (LMM), including APOE status (ɛ4 carrier versus non-carrier), timepoint (T0 versus T1), and arm (active versus sham) as factors. Exploratory cognitive outcomes will be analyzed with the same model but including three time-points (T0, T1, T2). To assess the effect of rTMS on the variables of interest, we will test the timepoint x arm interaction stratifying by APOE. To assess the magnitude of active stimulation in APOE ɛ4 carriers, we will test the timepoint x APOE interaction stratifying by arm. For the outcomes investigating the mechanisms underlying DMN modulation, we will test for timepoint x arm interaction in the whole study group. Finally, generalized linear models will be used to identify potential predictors of alterations in DMN connectivity, including the imaging and neurophysiological variables as independent variables (exploratory analysis).
Data management and storage
After signing the informed consent, participants will be assigned an alpha-numeric code in progressive order. All data acquired will be labeled with the participant’s code, and only the research staff will be able to link the name and the code of each participant.
Data will be kept both in paper and electronic form. Electronic data will be kept within a dedicated password-protected database; hard copy study material will be held within closets closed with a padlock. Electronic data and hard copy documentation will be accessible only by the research study personnel.
Expected results
In line with previous studies in elderly non demented populations [23, 26], we expect that the rTMS protocol will be effective in modulating DMN connectivity in APOE ɛ4 carriers and to observe a normalization of their connectivity to the level of non-carriers. From a biological/mechanistic perspective, we expect to identify the specific elements (neurons versus axons) and mechanisms (neuronal activity versus excitability versus connectivity) affected by rTMS using multimodal imaging and neurophysiological measures. Specifically, it is expected that rTMS will primarily affect neuronal activity and excitability and to a lesser degree axonal integrity. Moreover, some factors are known to influence the response to rTMS (e.g., the level of baseline plasticity and connectivity), thus we expect to observe significant relationships between these measures and rTMS effects on DMN connectivity. Finally, at the cognitive level we expect that changes in DMN connectivity will be associated with a selective improvement in memory performance.
DISCUSSION
Impact
The modulation of aberrant neuronal networks has been proposed as a possible therapeutic target for AD [72]. A growing body of literature suggests the possibility to modulate brain networks in vivo with rTMS [15] and promising results have been reported in AD patients [24]. With the AD field progressively focusing on pre-clinical stages [73], there is an urgent need to test whether these approaches can be translated to earlier phases. A long prodromal phase characterizes AD and targeting early network dysfunction before irreversible neuronal damage has occurred might indeed increase the chance of success. The NEST4AD study will target a process affected early in AD (DMN dysfunction) with rTMS and will test the effectiveness of this strategy in at-risk persons (APOE ɛ4 carriers). Evidence of effective manipulation of DMN connectivity will represent a step forward towards the development of innovative and targeted interventions for early AD. The focus on APOE ɛ4 carriers as a model for early AD is well in line with the view that APOE may be a promising target for AD prevention [74, 75] and with ongoing interventions focused on APOE ɛ4 carriers [76].
NEST4AD results will also inform on the mechanisms underlying DMN modulation. According to theoretical and experimental studies, rTMS effects are not restricted to neuronal elements but may also involve axons in the white matter [14, 77]. By collecting neuroimaging and neurophysiological markers, we will identify the specific elements and mechanisms affected by rTMS. Specifically, 1) changes in task fMRI BOLD signal will provide evidence for an activity-related neuronal mechanism, 2) changes in TMS-EEG will support excitability- or connectivity-related neuronal mechanisms, and 3) changes in diffusivity measures will support axonal-related mechanisms. Moreover, these markers may be useful as surrogate measures in clinical trials, as demonstrated by a recent investigation using TMS-EEG to monitor treatment’s effect on functional activity in AD patients [78].
At the cognitive level, NEST4AD will fully characterize the pattern of rTMS-induced cognitive effects. We expect that our protocol will enhance memory as reported in previous rTMS studies in cognitively healthy populations [19, 26]. Demonstrating this effect would provide direct support to the notion that the DMN supports memory [79]. Moreover, evidence that these effects are specific for memory and do not involve other cognitive domains would further strengthen this argument. Finally, in an exploratory analysis we will assess cognition two months after the rTMS sessions to monitor whether memory effects persist after stimulation.
In the longer term, the clinical impact of the proposed rTMS protocol may be relevant at the individual, economical, and social level. Preserving the cognitive abilities for as long as possible in persons at risk of decline would preserve a person’s quality of life, with positive effects on their caregiver and the broader health system. The estimated cost of dementia is about US$1 trillion annually, a figure that is estimated to rise to US$ 2 trillion by 2030 [80]. Some researchers estimated that a future intervention to delay the onset of dementia might reduce the total costs by 33–40%[81].
Strengths
Strengths of the study are the inclusion of a population at risk of AD, the focus on a pathophysiologically and cognitively relevant target (DMN dysfunction), and the multimodal approach. The combination of neuroimaging and neurostimulation techniques will enable to capitalize on their respective strengths (i.e., the high spatial resolution of MRI and the high temporal resolution of TMS-EEG). Moreover, the collection of rs-fMRI data will enable to extract the individual targets. One limitation of other stimulation protocols is the difficulty in determining the exact target. Previous studies in cognitively normal subjects or AD patients used different strategies to define the targets of stimulation, ranging from anatomy-derived coordinates of parietal or DLPFC targets [24, 82] to fMRI-derived individual coordinates of the DMN [19–23]. However, anatomical coordinates do not ensure the stimulation of functional networks, and stimulation of the DLPFC region can variably result in targeting the DMN or FPN network [83]. Conversely, rs-fMRI data can provide subject- and network-specific targets of stimulation. Finally, the results of this study may be relevant not only for APOE ɛ4 carriers but also for other groups at risk for AD, e.g., amyloid positive cognitively normal elderly, since DMN dysfunction is observed in these persons as well [8].
Limitations
Limitations of the study are the small sample size and the monocentric design, which may limit the generalizability of the results. Another limitation is that we will not differentiate between homozygous and heterozygous APOE ɛ4 carriers; thus, we could miss potential gene-dose effects. Similarly, we may miss the impact of APOE variants protective for AD (i.e., APOE ɛ2) [84]. However, we expect that the impact of these variants (APOE ɛ4 homozygotes and ɛ2 carriers) will be negligible in this sample given their low frequency (<5%). Finally, the design of this study will only enable to assess the short-term effects of rTMS. Future protocols collecting neuroimaging, neurophysiological, and cognitive markers over longer periods will enable to investigate whether rTMS can induce long-term effects.
CONCLUSIONS
The results of this study will inform on the feasibility of modulating DMN connectivity in persons at risk for AD and will provide novel insight into the neurobiological mechanisms underlying DMN modulation. These results may serve to develop non-invasive interventions for persons at risk of AD in the longer term.
ACKNOWLEDGMENTS
This project was funded by the Italian Ministry of Health (“Bando della ricerca finalizzata 2018 - Giovani ricercatori” grant n° GR-2018-12368250 and Ricerca Corrente)
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0659r1).