
Abstract
Background:
Pneumonia is an inflammatory condition induced by infection of the lungs and is frequently a cause of morbidity and mortality among patients with Alzheimer’s disease (AD). Some studies have shown an association between acetylcholinesterase inhibitor use and elevated pneumonia risk.
Objective:
The purpose of this study was to perform a comparative analysis of the number of reported pneumonia cases in individuals prescribed rivastigmine relative to the number of reported cases by patients using other therapeutics including over-the-counter drugs and other AD therapeutics, as reported to the FDA Adverse Event Reporting System (FAERS) database.
Methods:
A disproportionality analysis was conducted to investigate the association between using rivastigmine and risk of pneumonia. Age, gender, dosage, temporality, and geographic distribution of reported cases were also assessed.
Results:
Patients prescribed rivastigmine were more likely to report pneumonia as an adverse event than many drugs except galantamine. Males were found to be 46% more likely than females to report pneumonia as an adverse event while likelihood of pneumonia diagnosis increases 3–5-fold in patients older than 65 years of age.
Conclusion:
The observed elevated frequency of aspiration pneumonia in patients prescribed rivastigmine may be due to an induced cholinergic crisis that is selective for the medulla oblongata, resulting in gastrointestinal distress, impaired swallowing, heightened salivation, and labored breathing. The observed elevated frequency of infectious pneumonia in patients prescribed rivastigmine may also be linked to overstimulation of neurons in the medulla oblongata and downstream suppression of localized inflammatory responses.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a degenerative neurological condition that is defined as the slow escalation of cognitive impairment, memory decline, synaptic dysfunction, and inhibited social capabilities [1, 2]. In most clinical manifestations of the disease, progressive loss of both short and long-term memory, which results from neuronal loss and the shrinkage of hippocampal volume, are the initial symptoms [1]. Most cases of AD are diagnosed after the age of 65 and the prevalence of the disease increases as age increases, thus signifying a growing global medical problem as many populations are increasingly skewing older [3]. In the United States, approximately 6.2 million individuals aged 65 and older (11.3%) have been diagnosed and are currently living with AD, and that number is expected to double to approximately 12.7 million people by the year 2050 [3]. As a result of an aging global population and the lack of effective cures for the disease, AD is currently ranked as the 5th leading cause of mortality in individuals aged 65 and older in the United States [3].
Despite the absence of therapeutics that reverse the adverse cognitive effects induced by AD pathology, two classes of drugs are currently available that help to stave off and delay the onset of further cognitive decline. The first class of AD therapeutic agent includes the N-methyl-D-aspartate receptor (NMDAR) antagonist memantine, a non-competitive antagonist molecule that selectively inserts itself into NMDA glutamate channels and stifles NMDA receptor activity [4, 5]. While moderate levels of NMDAR function are required for synaptic plasticity and synaptic formation, overstimulation of NMDAR leads to excitotoxicity and neuronal damage. Thus, memantine’s role in the stalling of AD pathology is through modulation of NMDA receptor activity and reduction of excitotoxicity [4]. The second class of therapeutics used in AD treatment are a series of acetylcholinesterase (AChE) inhibitors, of which may be administered individually or as part of a combination therapy to patients with mild or moderate cases of the disease [6]. Drugs in this class include galantamine (Razadyne), donepezil (Aricept), and rivastigmine (Exelon) [6]. Cholinergic neurons, which play a significant role in memory and synaptic transmission, are stimulated by the chemical messenger acetylcholine, of which is primarily synthesized in the basal forebrain region of the brain [7]. Acetylcholine is generated by the conversion of acetyl-CoA and choline and is mediated by the enzymatic activity of choline acetyltransferase. Generated choline is then transported into synaptic vesicles via the vesicular acetylcholine transporter [6]. Subsequent calcium-mediated depolarization of the synaptic vesicles triggers the release of acetylcholine into the synaptic cleft, at which point acetylcholine can innervate neuronal activity through binding to muscarinic and nicotinic receptors [8]. Stimulation of these cholinergic neurons is then terminated as a result of AChE-mediated hydrolysis of the neurotransmitter, which results in the release of choline and acetate that can be recycled in presynaptic cells into new acetylcholine molecules [6]. As the cholinergic system is frequently disrupted in the early stages of AD, AChE inhibitors such as rivastigmine seek to restore proper cholinergic stimulation of neuronal activity and improve cognitive performance.
Frequent side effects of rivastigmine and other AChE inhibitors include vomiting, severe malaise, confusion, sleep disruption, increased aggression, difficulty swallowing, and aspiration pneumonia [9]. Of particular concern in the elderly afflicted with dementia-like symptoms is aspiration pneumonia, an inflammatory lung infection caused by entry of food, saliva, vomit, or stomach acid into the airways of the lungs as opposed to entry into the esophagus [10]. Infiltration of the respiratory system by food-derived microorganisms and acidic compounds can promote the development of lung abscesses, of which are pus-filled cavities containing necrotic lung tissue debris [10]. While some cases of aspiration pneumonia are induced by chemical exposure and thus do not require antibiotic treatment, most clinical cases are caused by commensal aerobic and anaerobic bacteria such as Staphylococcus aureus, Haemophilus influenzae, Streptococcus pneumoniae, and bacteroides [11]. As dysphagia is a common clinical side effect of both impaired cognitive function and AD treatment, further suppression of effective swallowing mechanisms may lead to an increased risk of aspiration pneumonia in some AD patients [12].
Administration of rivastigmine can occur either orally or transdermally, with doses ranging from 3–12 mg/day for oral capsules and 4.6–13.3 mg/day for transdermal patches [13]. Capsules are approved for mild and moderate cases of AD while the transdermal patch is approved for all AD patients with mild to severe cases [13]. Multiple reports have demonstrated an association between AChE inhibition and risk of pneumonia in AD patients. For example, a case report describes a fatal case of aspiration pneumonia in an 83-year-old white male who transitioned from a donepezil regimen to a 3 mg/day rivastigmine regimen without a washout period. The patient was presented to the emergency room with severe respiratory distress and was eventually intubated due to worsening respiratory function. Bronchoscopy results indicated infiltration of food particles into the lower airways and blood cultures indicated Haemophilus influenzae infection [14]. A small-scale study from the geriatric department of the Bertinot Juel Hospital in France has also shown a correlation between the use of cholinesterase inhibitors and pulmonary disorders. Of the 183 patients (131 males, 52 females) in the study, 55 patients were diagnosed with a respiratory disorder either before hospitalization or after admittance into the hospital, of which 37 patients had pneumonia. After univariate and logistic regression analyses, an adjusted relative risk of 1.98 was calculated for pulmonary disorders in patients administered cholinesterase inhibitors [15].
Despite these reported cases, there is currently no systematic analysis that has assessed the differences in pneumonia risk for patients prescribed each AD therapeutic individually as well as determined whether or not there is a difference in pneumonia risk for AD patients administered the rivastigmine patch relative to the oral capsule. Utilizing data from the FDA Adverse Event Reporting System (FAERS), a large repository of reported adverse drug events (ADE) from patients [16], medical professionals, and drug manufacturers, the frequency of pneumonia incidence was compared. In this study, we performed a comprehensive analysis assessing the association between the use of AChE inhibitors and frequency of reported pneumonia cases. In particular, we compared the number of reported pneumonia cases in individuals prescribed rivastigmine exclusively with individuals prescribed another commonly utilized AD drug as well as over the counter (OTCs) drugs. In addition, confounding factors such as gender, age, and dosage were also assessed as it pertained to pneumonia risk.
METHODS
FAERS records from 2000 to 2020 were downloaded from the public FAERS dashboard. Records derived from the FAERS database contain seven distinct tables including drug information (DRUG), drug reactions (REAC), patient outcome for the reported adverse event (OUTC), patient demographic information (DEMO), source of the reported adverse event (RPSR), start and end dates for drug therapy (THER), and the indications for use (INDI). The DRUG, REAC, and DEMO tables were selected for this analysis. The people who took a drug of interest were extracted by searching the DRUG table using both generic names (for example rivastigmine) and brand name (such as Exelon or Exelon patch) of the drug. The adverse drug events of these patients who had taken the drug were identified from the REAC table. Demographic information including age, sex, reporting date, and country of origin for reported cases was extracted from the DEMO table in the FAERS database. To avoid duplicate reports, each case ID that reported pneumonia as an adverse event was counted as one case, regardless of the number of reported adverse events per ID.
In order to compare the risk of pneumonia between different groups, a disproportionality analysis was performed. The reporting odds ratio (ROR), of which compares the proportion of pneumonia reports between the experimental group and the control group, was calculated. The 95% lower bound of the confidence interval greater than 1.0 indicated that the association between rivastigmine drug and pneumonia in the exposed group is significantly higher than the risk of pneumonia in the control group. In addition, age, gender, and dosage were assessed as possible confounders. Data analysis was performed using R statistical software.
RESULTS
The association between rivastigmine and pneumonia in patients prescribed rivastigmine exclusively
Most individuals in the FAERS database that have reported adverse events are prescribed multiple therapeutics. Consequently, it can prove difficult to determine whether or not pneumonia occurrence was attributed to rivastigmine, another prescribed therapeutic, or was the result of drug-drug interactions. Thus, patients that were prescribed exclusively rivastigmine for AD treatment were included in this study. The top 12 most frequently reported adverse events for patients prescribed exclusively rivastigmine were reported as counts and presented in Table 1. The most frequently reported adverse event was death. Additional adverse events that comprised the top 12 list included pneumonia, cerebrovascular accidents, and vomiting.
This table shows the top adverse events (frequency > 200 cases) reported by patients prescribed rivastigmine only. The most frequently reported adverse event was death. Additional adverse events that comprised the top 12 list included pneumonia, fall, vomiting, cerebrovascular accidents, dementia Alzheimer’s type, confusional state, nausea, malaise, drug ineffective, product adhesion issues, and dizziness. Pneumonia was among the top 2 most frequent adverse events associated with rivastigmine use
*including terms “pneumonia” (376), “pneumonia aspiration” (70), “pneumonia bacterial” (2), “pneumonia klebsiella” (1), “pneumonia pseudomonal” (1), “pneumonia viral” (1).
The temporal and geographic distribution of reported pneumonia cases
Figure 1 details the temporal distribution of reported pneumonia cases from 2000–2020 for patients prescribed exclusively rivastigmine for AD treatment. The peak of reported pneumonia cases occurred between 2011 and 2015, particularly in 2013 (approximately 120 cases), while the nadir of the reported pneumonia cases was in the early 2000s. In general, the number of reported cases of pneumonia by patients prescribed rivastigmine decreased between 2016 and 2020. In contrast, the number of reported cases increased significantly between 2008 and 2013.
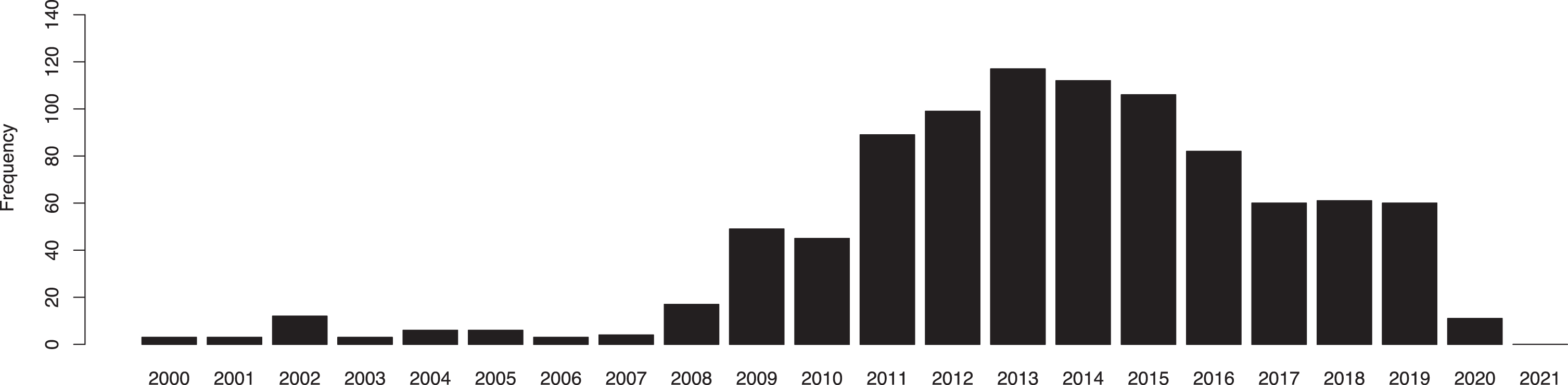
The temporal distribution of reported pneumonia cases from 2000–2020 for patients prescribed exclusively rivastigmine for AD treatment. The peak of reported pneumonia cases occurred between 2011 and 2015, particularly in 2013 (approximately 120 cases), while the nadir of the reported pneumonia cases was in the early 2000s.
In Fig. 2, the geographic distribution of reported pneumonia cases between 2000 and 2020 were included. Approximately 50% of all reported pneumonia cases by AD patients treated with a rivastigmine regimen originated from Brazil. In addition, a large percentage of pneumonia cases were sourced from Japan, Mexico, Argentina, and the United States.
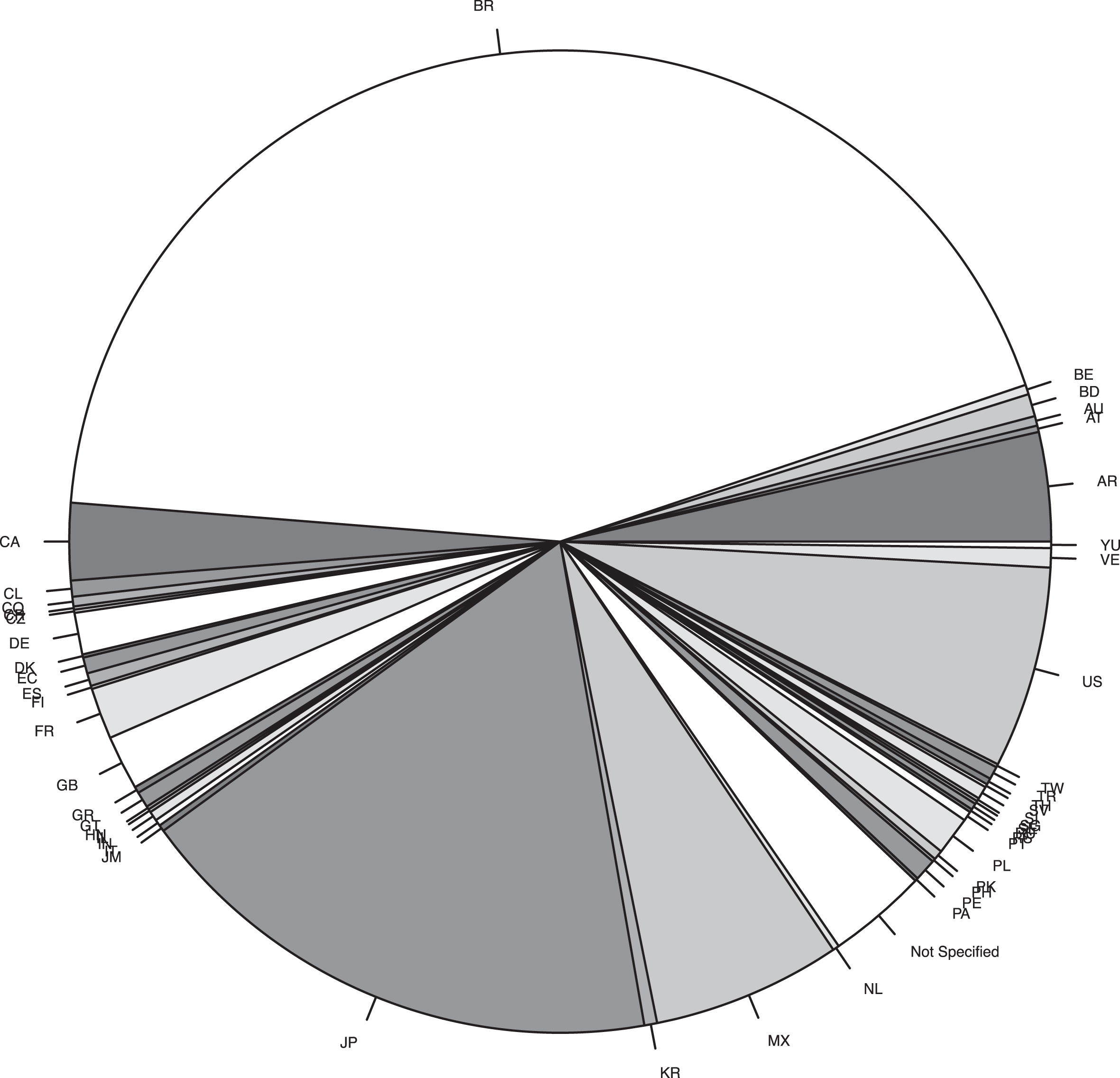
The geographic distribution of reported pneumonia cases between 2000 and 2020. Approximately 50% of all reported pneumonia cases by AD patients treated with a rivastigmine regimen originated from Brazil. In addition, a large percentage of pneumonia cases were sourced from Japan, Mexico, Argentina, and the United States.
The gender and age differences of reported pneumonia cases
Gender and age were assessed as confounders with regards to the possible link between rivastigmine and elevated pneumonia risk. With regards to gender, 214 female patients that were prescribed rivastigmine for AD treatment reported pneumonia as an adverse event to the FAERS database. In contrast 221 males (ROR = 1.46; 95% CI: 1.20–1.77) reported pneumonia as an adverse event after being administered rivastigmine. Thus, male AD patients prescribed rivastigmine were 46% more likely to report pneumonia as an adverse side effect relative to female AD patients. Gender assessment as a confounder is presented in Table 2.
The role of gender in the reporting of pneumonia as an adverse event by AD patients prescribed rivastigmine is presented above. Male AD patients were 46% more likely (ROR = 1.46; 95% CI: 1.20–1.77) than female AD patients to report pneumonia as an adverse event after being prescribed rivastigmine
Age was also evaluated as a possible confounding variable with regards to the association between rivastigmine and elevated likelihood of reporting pneumonia as an adverse event (Table 3). Relative to the 50–65 age demographic, patients aged 66–80 that were prescribed rivastigmine for AD treatment were 225% more likely (ROR = 3.25; 95% CI: 1.18–8.96) to report pneumonia as an adverse event. In addition, AD patients older than 80 years of age had a 4.5-fold greater likelihood (ROR = 4.50; 95% CI: 1.65–12.26) of reporting pneumonia as an adverse event after being prescribed rivastigmine.
The role of age in the reporting of pneumonia as an adverse event by AD patients prescribed rivastigmine is presented above. AD patients aged 66–80 were 225% more likely (ROR = 3.25; 95% CI: 1.18–8.96) to report pneumonia as an adverse side effect relative to patients in the 50–65 age group. Patients older than 80 that were prescribed rivastigmine for AD treatment were 350% more likely (ROR = 4.50; 95% CI: 1.65–12.26) than the 50–65 age demographic to report rivastigmine as an adverse side effect
The clinical outcomes of pneumonia cases
The resulting outcome of rivastigmine administration and its severity was assessed. AD patients that were prescribed rivastigmine and developed pneumonia had a 29-fold increase (ROR = 28.98; 95% CI: 7.21–116.46) in likelihood of being classified as having a serious outcome than rivastigmine users that did not develop pneumonia (Table 4). Of the 450 patients prescribed rivastigmine that ultimately developed pneumonia, 285 (63.39%) were hospitalized, 241 (53.50%) subsequently died, and 5 (1.11%) were in life-threatening condition. In contrast, of the 7,524 patients prescribed rivastigmine that did not report pneumonia as an adverse event, 1,749 (23.24%) were hospitalized, 2,704 (35.94%) subsequently died, and 140 (1.86%) patients were in life-threatening condition. Table 5 summarizes the outcome classifications for patients that developed or did not develop pneumonia after being prescribed rivastigmine for AD treatment.
The degree of severity was compared between AD patients prescribed rivastigmine that developed pneumonia with patients that did not develop pneumonia after rivastigmine use. Patients that developed pneumonia after being prescribed exclusively rivastigmine had a 29-fold greater likelihood (ROR = 28.98; 95% CI: 7.21–116.46) of having a clinically serious outcome than patients prescribed rivastigmine that did not develop pneumonia
Clinical outcomes were compared between AD patients prescribed rivastigmine that went on to develop pneumonia with patients that did not develop pneumonia. Among patients that developed pneumonia, 285 (63.39%) were hospitalized, 241 (53.50%) subsequently died, and 5 (1.11%) were in life-threatening condition. Among patients that did not develop pneumonia, 1749 (23.24%) were hospitalized, 2704 (35.94%) subsequently died, and 140 (1.86%) were in life-threatening condition
The dosage effects of pneumonia cases
In addition to age and gender, dosage was assessed as a possible confounding variable for the association between prescribed rivastigmine use and elevated likelihood of developing pneumonia. The two primary routes in which rivastigmine can be administered include oral ingestion or through the use of a transdermal patch. Due to the inaccessibility of data in prior years, data for dosage and route was assessed from 2012 4th quarter to 2020. In patients that utilized the transdermal patch, no statistically significant association was found between likelihood of pneumonia development and dosage at 9.5 mg (ROR = 1.28; 95% CI: 0.93–1.77) and 13.3 mg (ROR = 1.28; 95% CI: 0.80–2.03) was found between likelihood of pneumonia development and dosage with 4.6 mg as the referent group (Table 6). However, when assessing all patients regardless of administration route, a statistically significant increase in risk of pneumonia with respect to an increase in dosage was observed. When using a dose ≤5 mg as the referent group, patients prescribed a dose from 5–10 mg were 33% more likely (ROR = 1.33; 95% CI: 1.02–1.77) to report pneumonia as an adverse event. In addition, patients prescribed a dose greater than 10 mg were 70% more likely (ROR = 1.70; 95% CI: 1.20–2.40) than patients prescribed a dose ≤5 mg to report pneumonia after rivastigmine use.
The effects of dosage were assessed for the two primary routes of rivastigmine administration: oral and transdermal patch. No statistically significant association was observed across all dosages for the transdermal patch. However, patients prescribed a dose from 5–10 mg were 33% more likely (ROR = 1.33.; 95% CI: 1.02–1.77) to develop pneumonia relative to patients prescribed a dose > = 5 mg. In addition, patients that were prescribed a dose > 10 mg were 70% more likely (ROR = 1.70.; 95% CI: 1.20–2.40)
The comparison of rivastigmine with other drugs
Finally, the frequency of reported pneumonia cases was compared between patients prescribed exclusively rivastigmine, OTC drugs which are not known to increase pneumonia risk (negative controls), drugs that have been shown to elevate the probability of pneumonia development (positive controls), and other commonly administered AD therapeutics. As shown in Table 7, the negative controls selected for analysis included acetaminophen, ibuprofen, omeprazole, cetirizine, and aspirin. Of the 35,693 individuals taking exclusively acetaminophen, 176 individuals (ROR = 0.083; 95% CI: 0.070–0.099) reported pneumonia as an adverse event. 203 individuals (ROR = 0.078; 95% CI: 0.066–0.093) taking ibuprofen reported pneumonia as an adverse event while 36 individuals (ROR = 0.0982; 95% CI: 0.070–0.14) utilizing omeprazole developed pneumonia. The number of individuals who reported pneumonia after use of cetirizine and aspirin were 0 (ROR = 0.0087; 95% CI: 0.00050–0.14) and 68 (ROR = 0.1221; 95% CI: 0.095–0.16) respectively.
The frequency of reported pneumonia cases was compared between patients prescribed exclusively rivastigmine, over-the-counter (OTC) drugs (negative controls), drugs that have been shown to elevate the probability of pneumonia development (positive controls), and other commonly administered AD therapeutics
Next, the frequency in which pneumonia was reported as an adverse event to the FAERS database was compared between individuals prescribed rivastigmine and individuals that took one positive control exclusively; diphenhydramine (antihistamine), oxybutynin (bladder relaxant), and doxepin (antidepressant). These drugs were selected as positive controls as their use has been previously shown to be correlated with elevated pneumonia risk, particularly aspiration pneumonia (Table 7). Of the 2,356 individuals taking exclusively diphenhydramine, 7 individuals (ROR = 0.050; 95% CI: 0.024–0.11) reported having pneumonia after use. Finally, 5 individuals (ROR = 0.020.; 95% CI: 0.0067–0.039) taking oxybutynin reported pneumonia as an adverse event while 4 individuals (ROR = 0.18; 95% CI: 0.066–0.47) prescribed the antidepressant medication doxepin reported pneumonia as an adverse side effect.
Finally, frequency of pneumonia was compared between individuals prescribed rivastigmine exclusively for AD treatment and individuals prescribed 1 of the other commonly administered AD therapeutics (Table 7). Of the 2,561 individuals taking memantine, 25 individuals (ROR = 0.16; 95% CI: 0.11–0.25) reported pneumonia as an adverse event while no statistically significant difference was observed between users of rivastigmine and galantamine (ROR = 0.88; 95% CI: 0.68–1.14) in reporting pneumonia to the FAERS database after taking galantamine. Finally, 34 patients (ROR = 0.22; 95% CI: 0.16–0.32) prescribed donepezil reported pneumonia as an adverse side effect. Thus, AD patients prescribed exclusively rivastigmine were approximately 5 times more likely to report pneumonia than patients prescribed other AD therapeutics except galantamine.
DISCUSSION
Multiple studies have shown an association between the use of AChE inhibitors and elevated occurrence of pneumonia cases in AD patients [17, 18]. However, the mechanism in which rivastigmine confers elevated pneumonia risk in AD patients is still largely unclear. The observed gender differences in which males were 46% more likely to report pneumonia as an adverse event may be explained by differences in the swallowing mechanism between males and females. Males have been shown to have higher swallowing volume, greater swallowing velocity, and a longer inter-swallow interval than females [19]. As a result, men may be more susceptible to entry of food particles, saliva, or vomit into the trachea and eventually the lungs than females, thus promoting an environment conducive to pneumonia development. With regards to age differences, elderly individuals older than 65 years of age are not only more likely to have AD, but they are also more likely to have progressed to the later physiological stages of neurological decline. Later stages of AD are characterized by impaired swallowing mechanisms, breathing difficulties, loss of appetite, and an increase in susceptibility to infections such as pneumonia [20].
AChE inhibitors such as rivastigmine, galantamine, and donepezil are thought to impede the progression of AD through acetylcholine-induced innervation of neuronal activity and inhibition of TNF-mediated apoptosis [21, 22]. In contrast, memantine is a low-infinity inhibitor of N-methyl-D-aspartate (NMDA) receptors that selectively blocks overstimulation of glutamate ion channels [5]. A previous comparative study has shown elevated pneumonia risk in AD patients prescribed either memantine (HR = 1.59; 95% CI: 1.48–1.71) or the rivastigmine patch (HR = 1.15; 95% CI: 1.04–1.27) relative to AD patients prescribed donepezil [18]. However, as memantine is typically reserved for AD patients in the later stages of AD pathology, the observed elevated risk may in part be related to residual confounding by age as it was not adjusted for in this study. In addition, this study represents a more homogenous population as it consisted of community-dwelling individuals exclusively derived from a previous study (MEDALZ) in Finland [18]. In contrast, the FAERS database encapsulates all reported pneumonia cases for each drug across multiple distinct communities and populations all over the world. The aforementioned study did find a statistically significant difference in pneumonia risk between patients prescribed the oral form of rivastigmine and the transdermal patch. However, the MEDALZ study did not assess dosage as a possible confounder and only assessed risk between all dosages concurrently. In contrast, our study assessed the dose response and found no statistically significant difference in pneumonia risk for all dosages of the rivastigmine transdermal patch but did determine an increase in risk in patients taking a dose greater than 10 mg in all patients. Thus, the heterogeneity of results suggest that multiple underlying factors ultimately contribute to pneumonia risk in AD patients.
Two characteristics of rivastigmine and galantamine may explain this observed elevated risk in AD patients beyond the heightened baseline risk observed in all patients with AD. First, rivastigmine and galantamine have greater selectivity for tissue of the central nervous system (CNS) than tissue of the peripheral nervous system (PNS) [23]. In particular, they are selective for the monomeric G1 isoform of AChE [24]. Monomeric AChE localizes to several clinically relevant regions of the brain including the cerebral cortex, hippocampus, and the medulla oblongata [25]. The medulla oblongata is the lowest portion of the brain that is responsible for the regulation of the autonomic nervous system including salivation, digestion, breathing, swallowing, heart rate, and urination [26]. Damage to the vagus nerve in the medulla oblongata, which is common in the later stages of AD, or overstimulation of motor neurons by prolonged acetylcholine-mediated signaling leads to dysfunction of the tongue, increased salivation breathing complications, impaired swallowing mechanisms (dysphagia), inhibited coughing and sneezing, gastrointestinal distress, and vomiting [27]. In the case of rivastigmine and galantamine, inhibition of AChE activity at synaptic junctions in the medulla oblongata induces a cholinergic crisis that exacerbates autonomic dysfunction and increases the risk of aspiration pneumonia due to impairment of mechanisms that would otherwise impede entry of food particles and vomit into the lungs (Fig. 3) [27, 28].
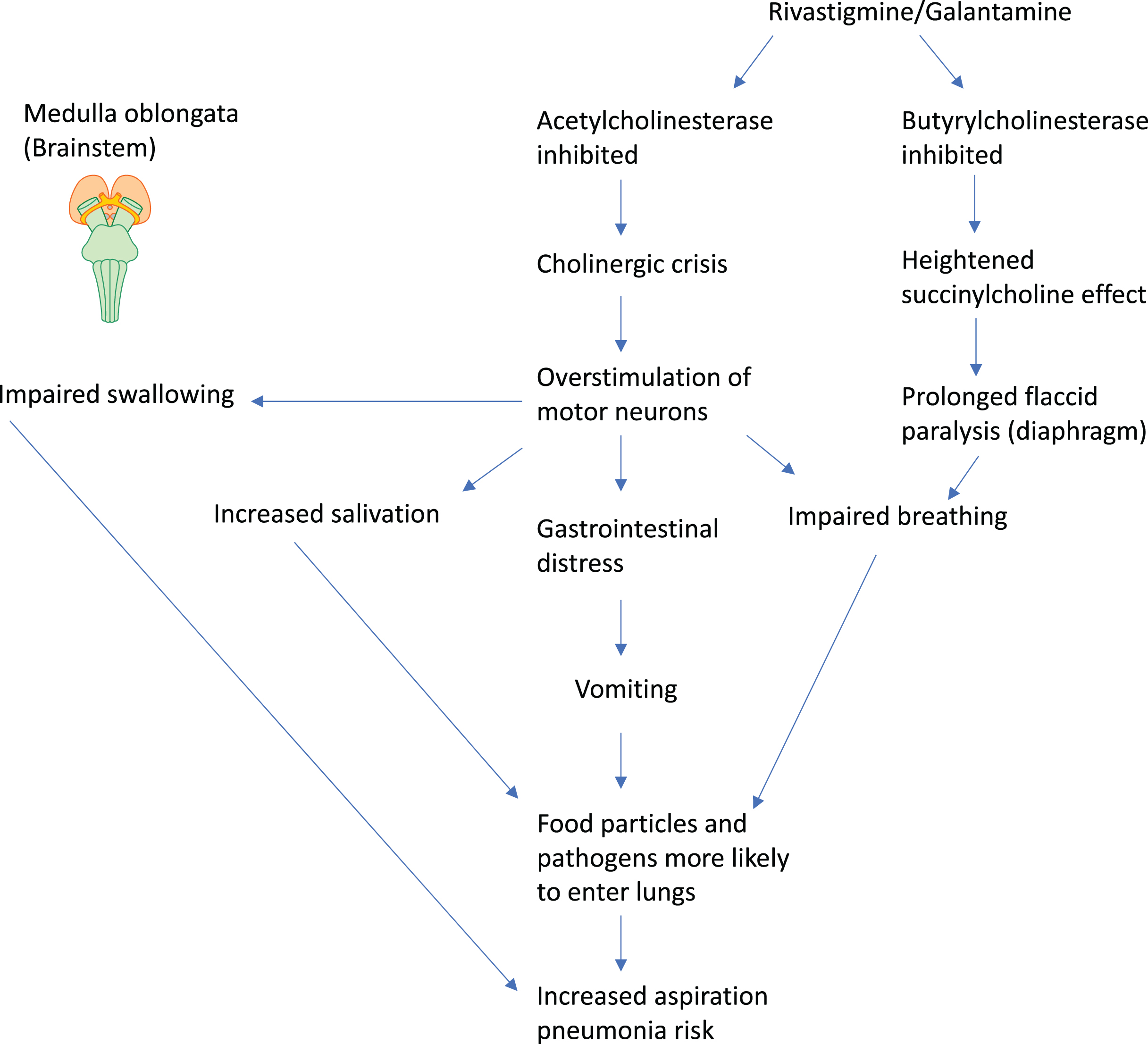
Mechanism for elevated aspiration pneumonia risk.
The second unique characteristic of rivastigmine and galantamine is the additional inhibition of plasma butyrylcholinesterase, a non-specific cholinesterase that can hydrolyze acetylcholine and succinylcholine [29]. Succinylcholine is a potent agonist of nicotinic acetylcholine receptors that is commonly administered as part of anesthesia in clinical settings and will bind to its corresponding receptors for longer than acetylcholine molecules, resulting in sustained muscle depolarization [29]. Succinylcholine In patients with either acquired and hereditary butyrylcholinesterase deficiency, prolonged binding of succinylcholine causes severe flaccid paralysis of the diaphragm and other skeletal muscles for several hours, further compounding existing breathing complications [27, 29]. As many of the pneumonia cases observed in this study were serious in nature and required hospitalization, the interaction between rivastigmine and medical intervention may have led to a greater risk of respiratory distress and subsequent higher mortality. In addition, some cases of aspiration pneumonia may have arisen in the clinical setting due to the administration of succinylcholine for the purposes of another medical procedure. Thus, the inhibition of two enzymes that regulate the parasympathetic nervous system (AChE and butyrylcholinesterase), as opposed to donepezil which only inhibits AChE activity, may work in a cooperative manner to greatly reduce autonomic function and muscle control.
In addition to the role of rivastigmine and galantamine in promoting aspiration pneumonia either before or after hospital admission, elevated acetylcholine activity may also modulate infectious pneumonia risk. Although more pneumonia cases from the FAERS database were classified as aspiration pneumonia, the large number of reported non-specific pneumonia cases necessitated the positing of a mechanism in which rivastigmine and galantamine may suppress the immune response and elevate likelihood of infectious pneumonia. The vagus nerve, which is the longest nerve in the human body and modulates functions of visceral organs through efferent and afferent fibers, plays a central role in maintaining homeostasis and fine-tuning localized inflammatory states [30]. In what is referred to as the vago-parasympathetic reflex or cholinergic anti-inflammatory pathway, the expression of proinflammatory cytokines can be reduced, stifling the immune response against localized infections [30]. The efferent fibers of the vagus nerve extend from the brainstem to the lungs, spleen, and gastrointestinal tract among other regions of the body [27]. The nerve endings of efferent fibers are in close proximity to memory T cells that express β2-adrenergic receptors, of which are stimulated by norepinephrine. Stimulation of the vagus nerve subsequently leads to downstream release of norepinephrine that can then bind to β2-adrenergic receptors located on resident T cells. Binding of norepinephrine triggers the upregulation of choline acetyltransferase, an enzyme that catalyzes the synthesis of acetylcholine from coenzyme acetyl-CoA and choline [31]. The released nascent acetylcholine can then bind to alpha 7 nicotinic ACh receptors (α7nAChR) located on macrophages and other resident cytokine-producing immune cells such as microglial cells [28, 31]. Binding of acetylcholine inhibits the downstream TLR4/MyD88/NF-κB signaling axis as well as promotes the phosphorylation and dimerization of the transcription factor signal transducer and activator of transcription 3 (STAT3) [28, 32]. Activated STAT3 then migrates to the nucleus and upregulates genes responsible for inhibiting the production of pro-inflammatory cytokines such as IL-6, TNF, IL-10, and IL-1β [28, 33]. Thus, overstimulation of the vagus nerve leads to release of norepinephrine, increased release of acetylcholine, and suppressed localized inflammation due to inhibition of pro-inflammatory cytokines. Figure 4 illustrates the mechanism of action in which rivastigmine elevates risk for infectious pneumonia.
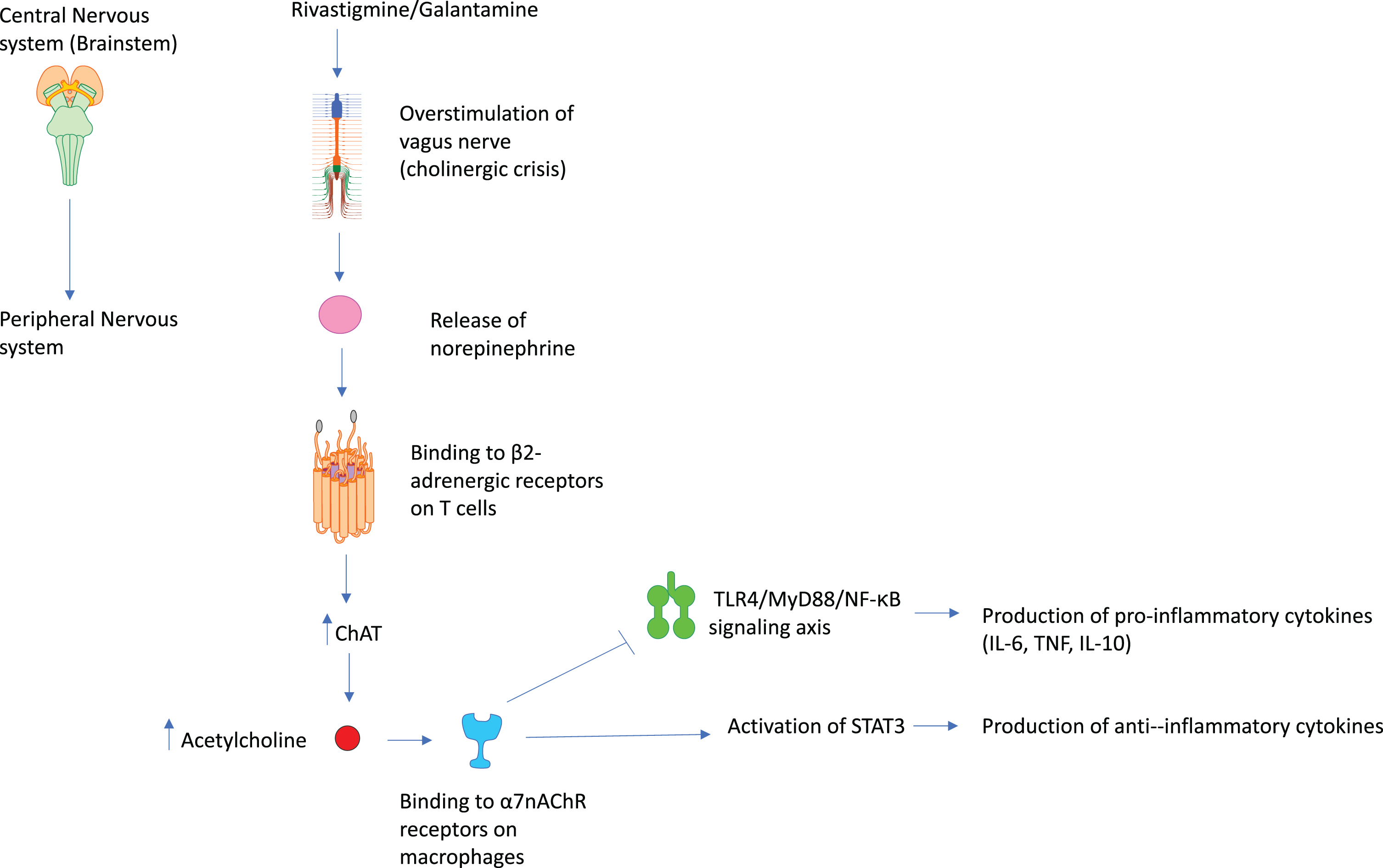
Mechanism for elevated infectious pneumonia risk.
Despite this, the current study has some limitations. First, despite having appropriately large sample sizes, more data should be collected concerning dosage as other studies have shown elevated pneumonia risk for the transdermal patch relative to the oral form. In addition, the proposed mechanisms are largely theoretical based on existing literature and thus, require further biological validation. Finally, the FAERS database does not contain possible covariate information including drinking frequency, smoking frequency, and physical activity levels. Further studies will focus on drug-drug interactions and how they influence pneumonia risk in AD patients as this study assessed pneumonia risk in patients that only took rivastigmine.
CONCLUSION
One of the most commonly reported adverse events to the FAERS database for individuals prescribed rivastigmine is pneumonia. Males were more 46% likely than females to report pneumonia as an adverse event after taking rivastigmine and individuals older than 65 were 3–5 times more likely to report pneumonia than individuals aged 50–65. The observed gender differences may be a result of inherent biological differences in which males have higher swallowing volume, greater swallowing velocity, and a longer inter-swallow interval. Individuals prescribed rivastigmine were approximately 5 times more likely to report pneumonia as an adverse side effect compared to individuals prescribed memantine (ROR = 0.16; 95% CI: 0.11–0.25) and donepezil (ROR = 0.22; 95% CI: 0.16–0.32). However, no statistically significant difference in reported pneumonia frequency was observed between users of rivastigmine and galantamine. An increase in dose was associated with elevated likelihood of pneumonia diagnosis for individuals prescribed the oral capsule while this was not observed for the rivastigmine patch. Despite these findings, further biological validation is required to confirm the proposed mechanism in which rivastigmine confers elevated pneumonia risk. Future studies will examine the role of drug-drug interactions in pneumonia risk by assessing pneumonia risk in patients prescribed different drug combinations.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0662r1).