
Abstract
Background:
Alzheimer’s disease (AD) and normal pressure hydrocephalus (NPH) commonly coexist.
Objective:
We aimed to characterize an overlapping syndrome of AD and NPH that presents with gait disturbance, ventriculomegaly on magnetic resonance imaging, and significant amyloid deposition on positron emission tomography (PET).
Methods:
Of 114 patients who underwent cerebrospinal fluid (CSF) drainage for a possible diagnosis of NPH between 2015 and 2020 in Samsung Medical Center, we identified 24 patients (21.1%) with the NPH patients with amyloid deposition on PET, which we referred to as hydrocephalic AD in this study. We compared their clinical and imaging findings with those of 123 typical AD without hydrocephalic signs/symptoms. We also investigated the frequency and potential predictors of the tap test response in hydrocephalic AD.
Results:
Evans’ index was 0.36±0.03, and a disproportionately enlarged subarachnoid space was present in 54.2% of the hydrocephalic AD patients. The mean age (75.2±7.3 years) and the APOE4 frequency (68.2%) did not differ from those of AD controls. However, the hydrocephalic AD patients showed better memory and language performance, and a thinner cingulate cortex. About 42% of the hydrocephalic AD patients responded to the tap test, of whom seven underwent shunt surgery. Cognition did not improve, whereas gait improved after shunt surgery in all.
Conclusion:
Hydrocephalic AD has different neuropsychological and imaging characteristics from typical AD. Future studies are warranted to further investigate the effect of CSF removal on their clinical course and to elucidate the pathophysiological interaction between amyloid and NPH.
INTRODUCTION
Normal-pressure hydrocephalus (NPH) is a clinical syndrome characterized by the classical triad of abnormal gait, cognitive impairment, and urinary symptoms with neuroimaging evidence of ventriculomegaly. Despite extensive clinical experience, it is still challenging to diagnose NPH because this clinical triad is nonspecific and could be attributable to other comorbidities in the elderly [1, 2]. What makes diagnosis more difficult is the possible coexistence with other neurodegenerative disorders that may be simply concurrent or the cause of both symptoms and ventriculomegaly [3].
Indeed, the presence of Alzheimer’s disease (AD), the most common neurodegenerative disorder, has been investigated in the NPH patients [4–6]. Previous studies have shown that the clinical response to cerebrospinal fluid (CSF) drainage or shunt surgery is poor in patients with concomitant NPH and AD [7–11]. Hypothetically, the common co-occurrence of AD and NPH is explained by the CSF circulation dysfunction shared between the two pathologies [12]; amyloid prevents CSF absorption [13], causing hydrocephalus, and the decreased CSF turnover in NPH leads to a failure of amyloid clearance [14]. Nevertheless, there has been scarce information on patients with concomitant AD and NPH.
In this study, we aimed to characterize AD patients who are positive for amyloid on positron emission tomography (PET) and present with NPH signs, including gait disturbance in early stage, which is atypical for AD. We compared cognition and cortical thickness between these patients and those with typical AD without hydrocephalic presentation and observed their clinical response to CSF drainage or shunt surgery. We hypothesized that amyloid positive hydrocephalus patients are more likely to have frontal dysfunction and frontal thinning (considered NPH-like characteristics), but less likely to respond to CSF drainage.
METHODS
Standard protocol approvals, registrations, and patient consents
The Institutional Review Board of Samsung Medical Center approved this study. Although the requirement for informed consent was waived for the use of clinical data, we obtained written informed consent from all patients before all clinical procedures after a detailed explanation. All processes were carried out in accordance with the Ethical Principles for Medical Research from the Declaration of Helsinki.
Participants
In this study, we referred to hydrocephalic AD (hydrocephalic variant of AD) as patients who develop both cognitive impairment and NPH-like symptoms associated with amyloid pathology. This is a hypothetically generated terminology to consider the association between AD and NPH, although definitive diagnosis of AD requires pathologic confirmation of significant amount of amyloid and neurofibrillary tangles. Therefore, our operational criteria for hydrocephalic AD is as follows: 1) presence of both gait disturbance and cognitive impairment with or without urinary incontinence; 2) clinical diagnosis of either NPH or AD with early presentation of gait symptoms; 3) presence of amyloid uptake on amyloid PET (we used amyloid PET instead of CSF amyloid as the inclusion criterion, because previous studies reported that CSF amyloid may be decreased in NPH [15, 16]; and 4) objective ventriculomegaly defined as Evans’ index (EI) > 0.30.
Figure 1 illustrates how we selected the hydrocephalic AD patients. We retrospectively reviewed 816 patients who underwent a CSF tapping on admission to Samsung Medical Center Memory Clinic between October 2015 to January 2020. Among them, we excluded patients with central nervous system infection, encephalopathy of any etiology, and other neurological disorders such as cranial nerve palsy, headache, or leukoencephalopathy (n = 509). Among the remaining 307 patients, we further excluded patients with the following conditions, resulting in the final 199 patients: 1) severe white matter hyperintensities (WMH) on brain magnetic resonance imaging (MRI) scans, defined as periventricular WMH≥10 mm and deep WMH≥25 mm, as modified from the Fazekas ischemia criteria; 2) a clinical diagnosis of Parkinson’s disease dementia or atypical parkinsonism, such as progressive supranuclear palsy, dementia with Lewy bodies (DLB), and multiple system atrophy, or other neurodegenerative disorder, such as frontotemporal dementia when followed up; 3) parkinsonism associated with use of any antipsychotics; 4) obvious preceding disease possibly causing ventricular dilation, including subarachnoid hemorrhage, meningitis, head injury, congenital hydrocephalus, and aqueductal stenosis; 5) EI < 0.3 and 6) Mini-Mental State Examination (MMSE) scores lower than 10 as advanced AD could lead to both gait disturbance and hydrocephalus.
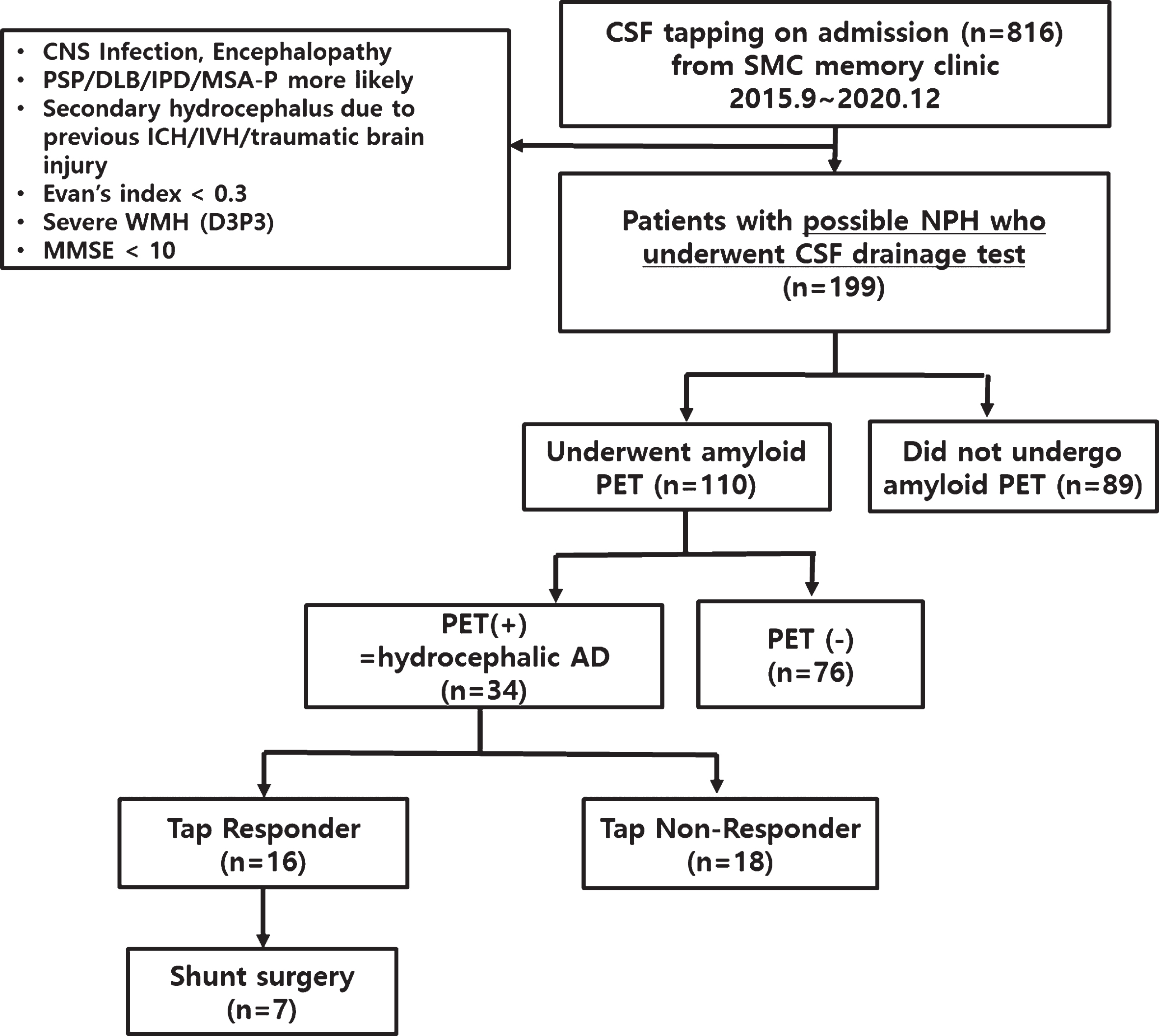
Selection of hydrocephalic Alzheimer’s disease patients. CSF, cerebrospinal fluid; SMC, Samsung Medical Center; NPH, normal pressure hydrocephalus; PET, positron emission tomography; AD, Alzheimer’s disease; CNS, Central nervous system; PSP, progressive supranuclear palsy; DLB, dementia of Lewy body; IPD, idiopathic Parkinson’s disease; MSA-P, multiple systemic atrophy-parkinsonism; ICH, intracranial hemorrhages; IVH, intraventricular hemorrhage; WMH, white matter hyperintensities; D3P3, deep WMH≥25 mm and periventricular WMH≥10 mm, as modified from the Fazekas ischemia criteria; MMSE, Mini-Mental State Examination.
The reason that these 199 patients underwent CSF drainage test (= a single CSF drainage test of 40–50 ml) was because of an objective gait disturbance and hydrocephalus (ventricular dilatation defined as EI > 0.3) seen on brain MRI, which led to clinical suspicion of isolated or combined NPH. Out of the 199 patients, 110 underwent amyloid PET and 30.9 % (34/110) turned out to have positive amyloid PET scans, fulfilling the hydrocephalic AD criteria as was described already. When we compared demographics between participants who underwent (110/199) and did not undergo (89/199) PET scans, age (p = 0.780), sex (p = 0.175), and MMSE score (p = 0.141) were not biased.
As an active control group, we recruited age matched amyloid PET negative normal controls (NC, n = 91) who had normal cognition and age- and MMSE-matched AD dementia patients (n = 123) who were amyloid-positive on PET. All participants in the control groups underwent 3-T brain MRI and neuropsychological tests at Samsung Medical Center. These patients, referred to as NC and AD controls, respectively, had no hydrocephalus on MRI and no symptoms or signs of motor or gait disturbance. All participants in this study were assessed using clinical interviews, neurologic examinations, comprehensive neuropsychological tests, and detailed neuroimaging.
MRI acquisition and analysis
We acquired standardized T2-weighted, 3-dimensional T1-weighted turbo field echo, and 3-dimensional fluid-attenuated inversion recovery (FLAIR), and T2*-weighted gradient echo (GRE) images at Samsung Medical Center using a 3.0-T MRI scanner (Philips 3.0T Achieva; Philips Healthcare, Andover, MA, USA) as previously described [17].
Analysis of ventricular volume and cortical thickness
The CIVET anatomical pipeline (version 2.1.0) was used to extract ventricular volume and cortical thickness (http://mcin-cnim.ca/neuroimagingtechnologies/civet/). In brief, using a linear transformation, native MRI images were registered to the Montreal Neurological Institute ICBM 152 nonlinear symmetric (2009a) template. We used the N3 algorithm to correct the images for intensity-based non-uniformities caused by inhomogeneities in the magnetic field. The registered and corrected images were then divided into white matter, gray matter, CSF, and background using a 3D stereotaxic brain mask and the Intensity-Normalized Stereotaxic Environment for Classification of Tissues (INSECT) algorithm. We obtained the ventricular volume (lateral+third+fourth ventricle) and extracerebral CSF volume using Automated Nonlinear Image Matching and Anatomical Labelling parcellation on native space [18]. In addition, the inner and outer surfaces of the cortex were automatically extracted using the Marching-cubes algorithm to obtain cortical thickness which was defined as the Euclidean distance between the linked vertices of the inner and outer surfaces. The detailed explanation for cortical thickness analysis was described in our previous study [11]. Using these methods, we obtained the mean cortical thickness values for each lobe.
Amyloid PET acquisition and visual assessment of amyloid positivity
Participants underwent Florbetaben (FBB) PET or Flutemetamol (FMM) PET at Samsung Medical Center using a Discovery STe PET/CT scanner (GE Medical Systems, Milwaukee, WI, USA) in three-dimensional scanning mode that examined 47 slices, 3.3 mm-thick, spanning the entire brain. We used a 16-slice helical CT (140 KeV, 80 mA; 3.75 mm section width) for attenuation correction. According to the manufacturers’ protocols, a 20 min emission PET scan with dynamic mode (consisting of 4×5 min frames) was performed 90 min after injection of a mean dose of 311.5 MBq of FBB or 185 MBq of FMM. 3D PET images were reconstructed in a 128×128×48 matrix with a voxel size of 2×2×3.27 mm3 using the ordered subsets expectation maximization algorithm (FBB iterations = 4 and subset = 20; FMM iterations = 4 and subset = 20).
Quantitative analysis of amyloid PET imaging
For quantitative analysis of the FBB and FMM uptake, PET images were co-registered to individual MRI normalized to a T1-weighted MNI-152 template using SPM8 in a MATLAB 2014b environment (MathWorks, Natick, MA, USA). After standard space registration, the brain was divided into 116 gray matter regions using the Automated Anatomical Labeling (AAL) atlas [19]. In order to obtain FBB and FMM uptakes, we used standardized uptake value ratios (SUVR) calculated by dividing the mean activity in target volumes-of-interest (VOI) by the mean activity in the cerebellar gray matter. Global cerebral cortex amyloid retention ratios were assessed from the volume-weighted average SUVR of 28 bilateral cerebral cortical VOIs: bilateral frontal (superior and middle frontal gyri, medial part of superior frontal gyrus, opercular part of inferior frontal gyrus, triangular part of inferior frontal gyrus, supplementary motor area, orbital part of superior, middle, and inferior orbital frontal gyri, rectus and olfactory cortex), posterior cingulate gyri, parietal (superior and inferior parietal, supramarginal and angular gyri, and precuneus), lateral temporal (superior, middle and inferior temporal gyri, and Heschl’s gyri), and occipital (superior, middle, and inferior occipital gyri, cuneus, calcarine fissure, and lingual and fusiform gyri). To obtain the global amyloid uptake from FBB and FMM scans, we converted the SUVR values of the FBB-FMM cortical target VOI directly into Centiloid (CL) units using the direct comparison of FBB-FMM CL (dcCL) method based on the CL conversion equation [20, 21]. In order to compare regional amyloid uptake, we calculated the regional/global SUVR ratio.
Clinical assessments and CSF tap test
Functional disability was assessed using modified Rankin scale (mRS), and the triad of symptoms were evaluated using the idiopathic NPH grading scale (iNPHGS) [22], which rates the severity of gait disturbance, cognitive impairment, and urinary symptoms from 0 (normal) to 4 (severest) based on observations and interviews with patients and their caregivers, as in our previous study. Regarding objective evaluations, gait was assessed using the Timed Up & Go Test (TUG) [23]. Cognition was assessed using the MMSE and detailed neuropsychological tests. For imaging parameters, EI and the presence of the disproportionately enlarged subarachnoid space hydrocephalus (DESH) sign (both tight high convexity and enlarged sylvian fissure) were evaluated by two independent neurologists; any discrepancy was decided based on consensus.
All hydrocephalic AD patients were admitted and administered a CSF tap test to remove large volumes of CSF (40–50 mL). After CSF drainage, all patients were assessed for improvement in mRS, iNPHGS, MMSE, and TUG tests. A tap test response was defined as an improvement in any of the following five criteria: 1) ≥1 level on mRS; 2) gait disturbance≥1 level on the gait scale in iNPHGS or≥20% reduction in the time in the best performed TUG tests or 30 m walking test; 3) cognition≥1 level on the cognition scale in iNPHGS or≥4 points in the MMSE; and 4) urinary disturbance≥1 level on the urinary scale in iNPHGS.
Neuropsychological tests
All participants underwent a standardized neuropsychological battery (the Seoul Neuropsychological Screening Battery [SNSB]) [24–26]. In this study, we generated a summary score for the following five cognitive domains as below: 1) attention domain, digit span forward and digit span backward; 2) language domain, Korean version of the Boston Naming Test (KBNT); 3) visuospatial domain, Rey-Osterrieth Complex Figure Test (RCFT) copy score; 4) memory domain, Seoul Verbal Learning Test (SVLT) (immediate recall, delayed recall, and recognition) and RCFT (immediate recall, delayed recall, and recognition); and 5) frontal domain, Controlled Oral Word Association Test (COWAT) animal, and COWAT phonemic score.
CSF analysis for AD biomarkers in hydrocephalic AD patients
CSF samples were collected from patients who agreed to further laboratory tests, and Aβ1–42, total (t)-tau, and phosphorylated (p)-tau levels were measured using commercial enzyme-linked immunosorbent assay (Innogenetics ELISA) kits.
Statistical analysis
Comparison of neuropsychological test results between hydrocephalic AD, NC, and AD controls was performed using analysis of covariance (ANCOVA) after adjusting for age, sex, and education. Comparison of ventricular volume and cortical thickness was performed using ANCOVA after adjusting for age, sex, education, and ICV. Comparison of the CL (amyloid) and regional/global PET SUVR ratio was performed using ANCOVA after adjusting for age and sex. Comparison of potential predictors between tap test responders and non-responders was conducted using Student’s t-test or Pearson’s chi-squared test. As a sensitivity analysis, we also conducted the same analyses between tap test responsive NPH (n = 16) and AD controls, to minimize the possibility of including other underlying etiologies in the NPH group. All analyses were conducted using STATA 15. A p-value < 0.05 was considered to indicate statistical significance.
Data availability
Anonymous data are available to qualified investigators upon requests addressed to the corresponding author.
RESULTS
Clinical characteristics of hydrocephalic AD
The mean age of the 34 hydrocephalic AD patients was 76.6±7.5 years, and the female patients comprised 41.2% (14/35). The prevalence of APOE4 carriers among the hydrocephalic AD patients was 51.5% (17/33 tested). All participants reported gait disturbance and cognitive impairment, and 29 out of 34 patients reported urinary symptoms as well.
In terms of cognitive impairment and gait symptoms, six patients reported gait disturbance as the first symptom and eight patients reported gait disturbance and cognitive impairment at the same time, whereas the remaining 20 patients reported cognitive impairment as the first symptom. In these 20 patients, the median interval between cognitive impairment and gait disturbance was 3.0 years. The mean EI of participants was 0.35±0.03, and 15 patients (44.1%) had positive DESH signs on MRI. Finally, levels of CSF Aβ1–42, t-tau, and p-tau were 469.5±163.8, 402.9±386.0, and 58.5±52.3 pg/ml, respectively (Table 1). Figure 2 illustrates MR images from representative cases out of the six patients who underwent shunt surgery.
Clinical characteristics of hydrocephalic AD
AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; CSF, cerebrospinal fluid; DESH, disproportionately enlarged subarachnoid space hydrocephalus; MRI, Magnetic resonance imaging; APOE4, Apolipoprotein E4; Aβ, amyloid-β peptide.

Representative cases of hydrocephalic Alzheimer’s disease who underwent shunt surgery. MMSE, Mini-Mental State Examination; VP, ventriculoperitoneal.
Neuropsychological characteristics, cortical thickness, and amyloid uptake of hydrocephalic AD
Compared to the NC group, both hydrocephalic AD patients and AD controls had worse performance on all cognitive domains and thinner cortex in all regions except the occipital cortex. Also, both AD groups had larger ventricular volume and higher ratio of ventricular to extracerebral CSF volume compared to the NC group (Table 2).
Comparison in cortical thickness and neuropsychological characteristics between hydrocephalic AD, NC, and typical AD
Values are expressed as means±standard deviations. ap value from analysis of covariance (ANCOVA) after adjusting for age, sex, and education, bp value after adjusting for age, sex, education, and total intracranial volume, cp value after adjusting for age and sex; *p < 0.05 for comparison with NC; §p < 0.05 for comparison with AD controls. NC, normal controls; AD, Alzheimer’s disease; CSF, cerebrospinal fluid; PET, positron emission tomography; SUVR, Standardized uptake value ratio.
When hydrocephalic AD patients were compared with AD controls, the mean age, prevalence of female sex, and years of education did not differ. In neuropsychological tests, however, the hydrocephalic AD group performed better on language (35.9±12.6 versus 30.4±12.7, p = 0.006) and memory (52.3±13.5 versus 45.8±10.7, p = 0.039) tests than the AD controls (Table 2).
We failed to obtain the ventricular volume from three (8.8%) hydrocephalic AD patients; additionally, cortical thickness and intracranial volume (ICV) could not be successfully obtained from nine (26.5%) hydrocephalic AD and 17 (13.8%) AD without hydrocephalus patients due to preprocessing errors. We found that ventricular CSF volume (110656.6±42127.9 versus 49,636.0±20,996.7 mm3, p < 0.001) and the ratio of ventricular to extracerebral CSF volume (0.17±0.06 versus 0.07±0.03, p < 0.001) were larger in the hydrocephalic AD patients than in the AD controls.
In terms of cortical thickness, we found that the hydrocephalic AD patients had a thinner cingulate cortex (3.04±0.14 versus 3.08±0.15, p = 0.009), but thicker or better preserved occipital cortex (2.91±0.18 versus 2.81±0.16, p = 0.006) compared to the AD controls. However, frontal, temporal, or parietal cortical thickness did not differ between the two groups (Table 2).
We also compared global amyloid PET uptake using CL units, and the two groups did not differ in terms of the amount of amyloid uptake. In terms of amyloid distribution assessed by FBB and FMM scans combined, the temporal/global uptake ratio was lower (p = 0.002) in the hydrocephalic AD than in the typical AD group (Table 2).
The analyses we performed so far between hydrocephalic and AD controls were repeated between tap test responsive hydrocephalic AD and AD controls. Overall we found similar results such that tap test responsive hydrocephalic AD patients had or tended to have better memory (p = 0.028) and language performance (p = 0.061), and a thinner cingulate cortex (p = 0.005) and a tendency to have a thicker occipital cortex (p = 0.073) (Supplementary Table 1).
Tap test responses and shunt surgery in the hydrocephalic AD patients
Among 34 participants, 16 patients were tap test responders according to our clinical criteria. We then compared clinical and imaging characteristics, and levels of CSF biomarkers between the two groups to find the potential predictors for a tap test response in the hydrocephalic AD patients. As shown in Table 3, age, sex, years of education, presence of APOE4 genotype, and MMSE scores were not significantly different between the tap test responders and non-responders. In addition, the presence of the DESH sign, EI, initial presentation with gait disturbance, and levels of CSF biomarkers (Aβ1–42, t-tau, and p-tau) were not significantly different between the two groups.
Comparison between tap test responders and non-responders
MMSE, Mini-Mental State Examination; DESH, disproportionately enlarged subarachnoid space hydrocephalus; CSF, cerebrospinal fluid. Values are expressed as means±standard deviations or frequency (%). p value from Student’s t-test or chi-squared test, as appropriate.
Among 16 tap test responders, seven underwent shunt surgery after receiving a detailed explanation of their amyloid status and expected cognitive trajectory in the future. The clinical course of these patients are described in Table 4. Five patients did not report significant cognitive improvement except for the one patient who showed an immediate 10-point improvement in MMSE score. Gait improvement following shunt surgery was found in all patients, of whom three demonstrated persistent improvement until the final follow-up. The maximum period of gait improvement was 4 years. Finally, five out of seven patients reported secondary deterioration in gait, which called for shunt pressure adjustment, shunt function testing, and/or imaging follow-up. One patient experienced shunt malfunction, another developed increased lateral ventricles on follow-up CT waiting for shunt revision, and the remaining three patients underwent shunt pressure adjustment, of whom only two improved again. The last two patients who underwent surgery in 2019 are being followed-up with a currently improved state.
Description of hydrocephalic AD patients who underwent shunt surgery
AD, Alzheimer’s disease; DESH, disproportionately enlarged subarachnoid space hydrocephalus; EI, Evans’ index; C, cognition; G, gait; U, urinary symptom, VP, ventriculoperitoneal; LP, lumbar-peritoneal; iNPHGS, idiopathic normal pressure hydrocephalus grading scale; TUG, timed-up and go; MMSE, Mini-Mental State Examination. Values are expressed as means±standard deviations or frequency (%).
DISCUSSION
In this study, we referred to amyloid positive patients with early NPH presentation as hydrocephalic AD and described their clinical characteristics in detail. The major findings of our study are as follows. First, we found that 30.9% of patients with NPH-like presentation had amyloid positivity. Second, the hydrocephalic AD patients demonstrated better cognitive scores, especially in the language and memory domains, thinner cingulate cortex, and thicker occipital cortex than the AD controls. Finally, approximately 47% of the hydrocephalic AD patients responded to the tap test despite amyloid positivity, but the long-term prognosis of shunt surgery and potential predictors for good prognosis remained unanswered.
The first major finding of our study was that among 110 patients with NPH-like presentation and ventriculomegaly, about 31% (34/110) demonstrated amyloid positivity, which is similar to previously reported rates (30–45%) based on neuropathological studies using cortical samples at shunt implantation [4, 27]. In these patients, we investigated the order of symptom development; the majority (30/34) develop cognitive impairment before gait disturbance. Nevertheless, it is hard to delineate the causality between AD and NPH based on our observations because the order of symptoms may not correlate with the order of pathologies. It is known that there is a time lag between amyloid deposition and cognitive impairment [28]; therefore, cognitive symptoms in our hydrocephalic AD patients may not be attributable to amyloid deposition.
Regarding the causal relationship between NPH and AD, we suggest two hypotheses (Fig. 3). The first hypothesis is the NPH first account where NPH affects amyloid clearance leading to AD for multiple reasons: this includes decreased CSF turnover in NPH resulting in decreased Aβ clearance; based on glymphatic MRI showing that the NPH patients have delayed clearance of tracer from the CSF and brain parenchyma [29], it is plausible that Aβ clearance may be decreased in NPH; dilated ventricles in NPH place pressure on brain parenchyma, causing arterial pulsatility restriction and venous congestion, which would subsequently affect glymphatic system clearance of brain waste, such as Aβ [30].The second hypothesis is the amyloid first account where amyloid pathology in AD may lead to NPH. Aβ accumulates in the vessels in the process of being cleared from the AD brain. Vascular Aβ may then decrease arterial pulsatility, causing glymphatic dysfunction followed by increased retrograde transventricular flow, leading to ventricular dilatation [31]. Alternatively, given that Aβ strongly binds to cell membranes [13] and generates increased intracellular calcium levels and subsequent cell damage [32, 33], it is reasonable to expect that soluble Aβ may cause toxicity in the ventricular ependymal cells, choroid plexus, and arachnoid villi, resulting in decreased bulk flow to the CSF outlet. If the NPH first hypothesis is true, we would expect the amount and distribution of amyloid uptake to be significantly different between the hydrocephalic and typical AD groups. However, with the same global uptake, the two groups did not differ in all VOIs except in a few brain regions, suggesting that the amyloid first account may be the most plausible explanation. However, to clarify this causal relationship, future studies are warranted to follow up amyloid-negative hydrocephalus patients to see whether they develop amyloid pathology, and conversely AD patients without hydrocephalic presentations to see whether they develop NPH-like symptoms and ventriculomegaly.

Possible hypotheses for the interaction or causal relationship between normal pressure hydrocephalus and Alzheimer’s disease. Red boxes and lines represent pathogenesis of “NPH-first hypothesis”, whereas blue boxes and lines represent pathogenesis of “Alzheimer’s-first hypothesis”.
The second major finding of our study was that the hydrocephalic AD patients had better cognitive scores and different cortical thickness (thinner cingulate and higher occipital cortex) than the AD controls. Particularly, the hydrocephalic AD patients had better scores in language and memory tests, which are typically affected in AD, whereas frontal function was similar between the two groups. This cognitive pattern is partially consistent with previous findings that patients with idiopathic NPH have preserved memory, but poorer frontal function than those with AD [34–36]. In line with these neuropsychological findings, we found that the hydrocephalic AD patients had a thinner cingulate, which is supported by a previous study that demonstrated that ventricular dilatation in NPH could affect perfusion in the cingulate cortex due to compression [37]. Interestingly, the hydrocephalic AD patients had thicker occipital cortex than the AD controls. These areas may be the least affected by ventricular dilatation, but further research on the meaning of this difference is needed.
The typical regions of neurodegeneration in AD, such as the temporoparietal cortex, did not differ between two groups. Given a significantly larger ventricle/extra-cerebral CSF volume in the hydrocephalic AD patients than in the AD controls with a similar level of AD’s signature cortical thinning, we consider that a simple compensatory process due to cortical atrophy (= ex vacuo) does not explain the ventricular enlargement in hydrocephalic AD.
The third major finding of our study was that 47% (16/34) of the hydrocephalic AD patients responded to tap test despite amyloid positivity. We tried to investigate predictors for tap test responders in this group, but none of the clinical or imaging characteristics were found to be associated with tap test responses in the hydrocephalic AD patients. Although the DESH sign has been considered the most useful imaging characteristic suggesting idiopathic NPH, and more importantly predicting shunt response [38, 39], the frequency of the DESH sign was not different between the tap test responders and non-responders in hydrocephalic AD patients. Our study findings suggest that this is less valuable as a predictor for tap test response in the amyloid-positive patients. A possible reason could be that DESH signs may not reflect disorders of CSF dynamics in the atrophied brain.
Another interesting finding was that levels of CSF biomarkers did not differ between the tap test responders and non-responders. This is inconsistent with our previous study [11] that demonstrated significantly lower t-tau, p-tau, and p-tau/Aβ42 ratio in the tap test responders with idiopathic NPH than in the non-responders. This discrepancy may be explained by the different study populations. In other words, CSF t-tau and p-tau levels may not be closely associated with disease severity or degree of neuronal injury in the already amyloid-positive AD patients. This is in line with the idea that CSF biomarkers may be able to accurately diagnose AD but may not be sufficiently sensitive to act as progression markers [40, 41].
Among 16 tap-test responders, seven patients underwent shunt surgery. In fact, many studies, including our previous report, demonstrated that amyloid positivity itself is a strong predictor for tap test non-response [11]. Nevertheless, the tap test or surgery benefitted the gait, not the cognitive impairment, of our patients; only one patient reported objective cognitive improvement as expected. Considering that gait impairment in the elderly can lead to frequent falls and trauma, improvement in gait could improve quality of life. Therefore, in patients with NPH characteristics, amyloid positivity should not be regarded as an absolute criterion to be excluded from treatment of NPH. Another interesting finding was that five out of the six patients experienced secondary deterioration and required shunt adjustment and/or shunt function testing. This higher rate of secondary deterioration in this group (compared to a reported rate of 20% in a previous study [42]) is noteworthy and may suggest a distinct pathogenesis in the hydrocephalic AD brain. For example, not only a decrease in CSF absorption, but a concomitant decrease in CSF production may have a role in the development of hydrocephalic AD, i.e., decreased intraventricular pressure may require further shunt pressure adjustment. Therefore, the CSF dynamics in hydrocephalic AD remains to be further investigated. Alternatively, it is also possible that a deterioration in gait symptoms may be attributed to underlying neurodegeneration instead of hydrocephalus, although two patients demonstrated improved gait following shunt adjustment.
There are several limitations of this study. First, the pathologic confirmation was unavailable. Therefore, clinically diagnosed NPH with amyloid deposition, especially the tap test unresponsive group, might have other co-morbid neurodegenerative diseases such as DLB, although we tried to exclude these at the first place. Also, although we used the terminology of hydrocephalic AD to suggest a new subtype of AD, a diagnosis of AD cannot be made when there is no pathologic confirmation or additional information on the neurofibrillary stage. Second, we could not explain the pathophysiological interactions between AD and NPH, and especially regarding which triggers the other. It also remains uncertain which AD patients are susceptible to ventricular enlargement disproportionately greater than atrophy. In fact, a recent genetic study showed that a gene causing ciliary abnormality causes NPH [43]. Therefore, further studies using genomic and preclinical data are required. Third, cautious interpretations might be needed for our imaging analyses, as the ventriculomegaly in the NPH group might have led to inaccurate measurement of cortical thickness, CSF volume or PET uptake values (because of registration issue). Finally, we used EI instead of ventricular volume as an inclusion criterion; therefore, we may have missed more patients considering that EI is not a sensitive measure of ventricular enlargement [44, 45]. Considering that ventricular volume is more closely related with cognition or gait [46], further studies using a ventricular volume-based cutoff instead of EI-based is needed, although ventricular volume is not as simple to measure as EI.
Patients with biomarker evidence of AD can commonly present with early gait disturbance with hydrocephalus. This overlapping syndrome of AD and NPH may be a consequence of a unique variant of AD (referred to as hydrocephalic AD in this study), characterized by preserved memory and a similar level of cortical thinning compared to that in AD controls. Despite amyloid positivity, 47% of patients with hydrocephalic AD demonstrated gait improvement following the tap test, although the long-term prognosis of shunt surgery and potential predictors for good prognosis remain unclear. Further research about the pathogenesis and treatment of this condition is required.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HI19C1132 and HR21C0885) and the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (NRF-2020R1A2C1009778).