
Abstract
Background:
Despite the improved access to health services in China, inadequate diagnosis and management of dementia are common issues, especially in rural regions.
Objective:
The Hubei Memory & Aging Cohort Study was designed as a prospective study in Central China to determine the prevalence, incidence, and risk factors for dementia and mild cognitive impairment (MCI) among urban and rural older adults.
Methods:
From 2018–2020, participants aged ≥65 years were screened, and data regarding their life behaviors, families, socio-economic status, physical and mental health, social and psychological factors, and cognition were collected. Diagnoses of MCI and dementia were made via consensus diagnosis using the Diagnostic and Statistical Manual of Mental Disorders fourth edition criteria.
Results:
Of 8,221 individuals who completed their baseline clinical evaluation, 4,449 (54.1%) were women and 3,164 (38.4%) were from remote rural areas (average age: 71.96 years; mean education period: 7.58 years). At baseline, 25.98%(95%confidence interval [CI]: 24.99–26.96) and 7.24%(95%CI: 6.68–7.80) of the participants were diagnosed with MCI and dementia, respectively. Prevalence showed a strong relationship with age. The substantial disparities between rural and urban regions in MCI and dementia prevalence and multiple dementia-related risk factors were revealed. Especially for dementia, the prevalence rate in rural areas was 2.65 times higher than that in urban regions.
Conclusion:
Our results suggested that public health interventions are urgently needed to achieve equitable diagnosis and management for people living with dementia in the communities across urban and rural areas.
INTRODUCTION
China has the largest population of older adults [1], and subsequently has the largest number of patients with dementia worldwide [2]. Despite the improved access to health services, inadequate diagnosis and management of dementia are still common issues, particularly in rural areas. It has been estimated that approximately 75%and 90%of urban of rural patients with dementia, respectively, do not receive timely diagnosis or treatment [2]. Instead, such patients reside at home and are cared by family members. Therefore, it is essential to develop a community-based study to fully understand the dementia burden and risk factors attributable to the cognition-specific aging process, to develop effective prevention programs, possible biomarkers, and future therapeutics.
In the recent decades, the inhabitants of the countryside across China are rapidly aging as the younger generations relocate to cities. This urban-rural disparity is well documented in China [3]; however, we still lack information concerning the changes in the prevalence, incidence, and risk factors for mild cognitive impairment (MCI) and dementia. Given that economic development is unevenly distributed across Eastern, Central, and Western China [4, 5], the primary prevention of dementia based on geographic region is essential; although several longitudinal aging studies have previously been conducted (Supplementary Table 1), no such study has evaluated the condition in the underdeveloped geographical area of Central China. Therefore, a longitudinal study of aging in Central China is necessary and has been endorsed. Additionally, it is important to trace the successive emergence of the clinical symptoms of dementia or Alzheimer’s disease, progressing from normal to subtle objective cognitive decline, MCI, and dementia [6, 7].
In response to this need for obtaining more sophisticated and multidisciplinary data concerning the trajectory of cognitive aging in less developed areas in China, the Hubei Memory & Aging Cohort Study (HMACS) was established. Hubei province is the hub and central region of Central China, with 58.5 million permanent residents [8]. Herein, we aim to describe the design, sampling, methodology, and participant characteristics of the baseline HMACS enrolled between 2018 and 2020.
MATERIALS AND METHODS
Study cohort
The HMACS was designed as a community-based cohort study with urban and rural settings. For the urban cohort, we randomly selected four districts in Wuhan metropolitan area, Hubei Province, and then selected 31 neighborhoods within these four targeted districts. For the rural cohort, four townships in Dawu county, a remote mountain area, were selected; then, 48 villages from these four targeted townships were randomly selected. All eligible residents living within the sampled neighborhoods and villages were identified from the electronic health records (EHR) maintained in the hospitals and health centers. China has established EHRs for citizens aged ≥65 years. Eligible residents were: 1) registered residents in these neighborhoods and villages with EHRs; 2) those aged ≥65 years; 3) those without dementia diagnosis; 4) those without diagnosis of schizophrenia, major depressive disorder, or life-threatening disease based on their medical records; and 5) those able to accept physical and cognitive examinations. Residents in nursing homes and psychiatric hospitals were excluded. This study was approved by the Medical Ethics Committee of Wuhan University of Science and Technology (protocol code: 201845; approved on October 22, 2018). Written informed consent or witnessed oral consent (in cases of illiteracy) was obtained from all participants after the nature of the procedures had been fully explained.
Power analysis showed that a sample size of 2,000 individuals would allow estimation of a typical dementia prevalence of 4.5%(standard deviation [SD]: 0.9%). Rural and urban samples of 1,000 each would provide a standard error of 1.2%. Missing data were handled by case-wise deletion, given the low proportion of missing data (0–4%) for all variables. We built a sample of 8,221 individuals, which can be used to estimate the prevalence in a certain area, and the statistical power was > 99%.
As shown in Fig. 1, we sampled 13,246 geriatric residents, but 2,109 were ineligible (257 were dec-eased; 536 refused any interviews; 908 were hospitalized, and 408 had other reasons). Of the remaining eligible 11,137 individuals, 2,916 did not participate (non-participants; 409 had severe hearing or vision impairments, 787 did not complete the cognitive screen, 785 did not finish the clinical examinations, and 935 had missing data). Eventually, 8,221 individuals completed their baseline cognition tests and clinical evaluation, and the response rate was 73.8%.
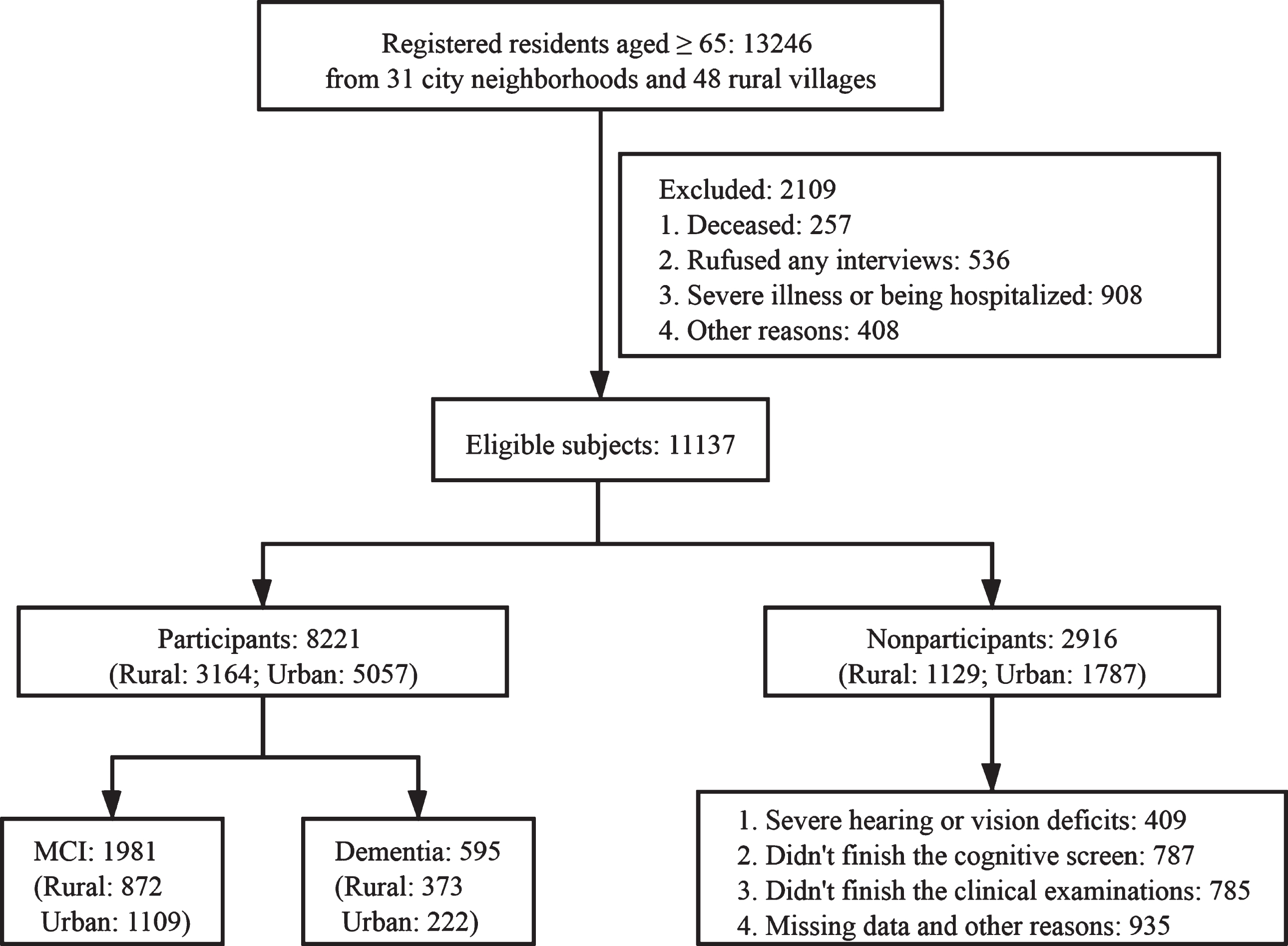
Study flow chart. MCI = mild cognitive impairment.
Data collection
The dataset was designed and collected by a collaborating team of specialists. Neurologists from Tianyou Hospital, China Resources & WISCO General Hospital, and Dawu County Hospital of Traditional Chinese Medicine conducted physical and neurologic examinations of all participants. Nurses from four community health centers and four township hospitals conducted physical measurements and biological sample collections. Specially trained medical graduate students and junior physicians performed the interviews and neuropsychological tests. The information recorded for participants in the HMACS is summarized in Fig. 2. The face-to-face interview and neuropsychological tests took approximately 90 min, while the physical and clinical examinations took approximately 70 min to be completed. The complete study visit was carried out on day 1, with breaks.

Summary of data collected in the HMACS.
Face-to-face interviews included questions on demographics, socio-economic variables, social network size, health behaviors, personality, and health status. Social network size was quantified with standard questions regarding living arrangement, number of children and siblings alive and close friends, and frequency of interactions with neighbors and friends (Supplementary Table 2); the responses were summed and averaged to yield a total score. Ratings of 0–3, 5–7, and 8–9 indicated limited, appropriate, and good social connections, respectively [9, 10]. The participants rated their current frequency of eating fruits, fish and animal fat, and drinking tea. They rated their current frequency of participation in seven cognitively stimulating activities (such as reading books or newspapers; playing chess, cards, or games; calligraphy and painting; and other intellectual activities) on a 5-point scale, with 5 indicating participation in the activity every day or almost every day and 1 indicating participation once a year or less. Item scores were averaged to yield a summary measure of cognitive activity.
The individuals were asked if they had participated in each of the five activities (walking exercise, dancing, Taiji, ball games, other exercises) during the past 3 months; in such case, they were asked concerning the number of times and the mean time per session [10]. Minutes in each activity were summed and divided by 120 to yield a summary measure of hours per week of physical activity, as described elsewhere [11].
The presence of 24 self-reported chronic illness or medical conditions (i.e., hypertension, diabetes, coronary heart disease, hyperlipidemia, anemia, cerebral vascular disease, head injury, intracranial infection, facial infection, history of toothache and tooth extraction, thyroid disease, cervical spondylopathy, general anesthesia, and carbon monoxide poisoning) was determined from EHR only or EHR with examination. We preferred self-reported chronic illness or medical conditions, which were confirmed by EHR. If a chronic illness was not self-reported, we used the examination data. Physical measurements included blood pressure (taken twice with the second blood pressure value used in our analysis), height, weight, grip, vision, and hearing. The number of conditions present was used as a measure of chronic illness, as described elsewhere [11, 12].
Chronic constipation was assessed by asking participants regarding their bowel habits and the history of constipation [13] in the past 3 months. Insomnia was evaluated using the Athens Insomnia Scale (AIS). The AIS evaluates sleep during the past month using eight questions (Supplementary Table 2). Participants with AIS≥6 were clinically defined as having insomnia [14]. Subjective hearing and olfactory functions were reported during the interview [15–17]. For the description and scoring assignment of the above indicators, please refer to the Supplementary Table 2.
Neuropsychological tests
The neuropsychological battery used in the study included: 1) the Chinese version of the Mini-Mental State Examination [18, 19] and the Chinese version of the Montreal Cognitive Assessment-basic [20–21]; 2) the auditory verbal learning test [22]; 3) trail-making test A & B; 4) the forward and backward conditions of the digit span test; 5) the Boston naming test [23] and the animal fluency test; 6) the clock-drawing test; 7) the short version of the geriatric depression scale [24, 25]; 8) the Lawton and Brody activities of daily living (ADL) questionnaire [26]; and 9) the neurologist-administered clinical dementia rating (CDR) scale [27, 28]. All the above neuropsychological tests were administered to all the participants.
Quality control and follow up
All team members and interviewers underwent ex-tensive training, including the study objectives, face-to-face interviews skills, neuropsychological tests, anthropometrics, performance measurements, biolo-gical sample processing and blood-based measu-rements, and referrals to health facilities when indicated. After 2 weeks of training, the trainees had to pass a written examination and simulation of the interview to become qualified interviewers.
The study team analysts produced weekly and monthly field check tables to support the field-based teams for continuous progress and data-quality monitoring. The field sites were periodically inspected by the responsible investigators every season, and a routine callback interview for quality control and reliability was performed for approximately 5%of the enrolled participants by random selection. Internal checks were embedded in the document system to ensure data completeness and accuracy.
The primary mode for follow-up examinations will be face-to-face interviews at community health centers every 4 years. Additionally, follow-up examinations will include data linkage to social and national health administrative databases and a survey through a mobile phone app each year.
Cognitive diagnoses
Two board-certified neurologists, two neuropsychologists, and two experts in dementia from the Brain Science and Advanced Technology Institute formed the expert panel. After the study visit was completed, the expert panel reviewed the participants’ functional, neurological, and cognitive abilities, as well as other pertinent data, and subsequently reached a consensus regarding the presence or absence of dementia using the DSM-IV criteria [29]. Only those who were not diagnosed with dementia were considered for a diagnosis of MCI, which was defined according to Petersen’s criteria [30]: 1) Concern of a cognitive change by the participant, informant, or clinician based on information obtained during the clinical interview, with CDR = 0.5; 2) Objective impairment for any neuro-psychological test within a cognitive domain (i.e., performance falling > 1.5 SD outside the age-adjusted normative mean); 3) Essentially normal functional activities (determined from ADL evaluation); 4) Absence of dementia (by the DSM-IV criteria).
Statistical analyses
SPSS version 26.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Continuous variables are expressed as means (SDs) or medians (interquartile ranges), and categorical variables are presented as frequencies (%). Student’s t-tests or one-way analyses of variance were performed for comparisons of continuous variables. The Chi-squared test was used for comparisons of categorical variables. Logistic regression models were used to further ascertain possible risk factors for MCI or dementia by concomitantly entering variables using forward stepwise methods.
Echoed with previous studies, we incorporated gender, age, education level, living arrangements, cigarette smoking, drinking, and social connections into the main logistic regression model to identify potential risk factors for MCI and dementia. Based on our main model, we also performed a series of sensitivity analyses to verify the robustness of our findings, including further adjusted for chronic disease, physical exercise, food patterns, insomnia, and constipation, respectively. All p-values and 95%CIs were estimated in a two-tailed fashion. Differences between the groups were considered statistically significant when the p-value was < 0.05.
RESULTS
Characteristics of study participants
The characteristics of 8,221 participants and 2,916 non-participants are presented in Table 1. Of the 8,221 individuals who completed their baseline cognitive and clinical evaluation, 4,449 (54.1%) were women and 3,164 (38.4%) were from remote rural areas (average age: 71.96 years [SD: 5.895]; mean education period: 7.58 years [SD: 5.359]). Of the 2,916 non-participants, 55.2%were women, the average age was 71.38 years (SD: 5.522), and the average education was 7.57 years (SD: 5.222). There was no statistical difference between the participants and non-participants by region, sex, education, and smoking and drinking habits. The average age of participants was higher than that of non-participants (p < 0.001) because of the high proportion (45.7%) of non-participants aged 65–69 years, and the low proportion (10.9%) of non-participants aged 80 years. Compared with non-participants, the participants were more likely to have hypertension (66.2%versus 56.7%), cerebral vascular disease (17.5%versus 14.2%), and heart disease (14.5%versus 13.5%), but less likely to have diabetes (16.6%versus 38.4%) and obesity (10.2%versus 12.6%).
Comparison of HMACS participants and nonparticipants
HMACS, The Hubei Memory & Aging Cohort Study; BMI, body mass index.
Comparison of the characteristics of urban and rural cohorts
The participants from rural regions were similar to those from urban areas in terms of sex distribution, and the frequency of depression and heart diseases. There were large rural/urban-related gaps in education (p < 0.001), social connections (p < 0.001), cognitive activities (p < 0.001), and diet pattern (p < 0.001) (Supplementary Table 3). The participants aged 65–69 years (43.2%versus 39.7%) and those aged > 80 years (13.9%versus 10.6%) were more common in urban cohorts than in rural ones (Supplementary Table 3). Rural participants were more likely to be underweight (6.7%versus 3.6%), unmarried (32.5%versus 18.3%), and living alone (23.4%versus 10.4%). They were less likely to engage in physical exercise (72.7%versus 86.8%) or perform cognitive activities (40.9%versus 72.2%), but drank (29.0%versus 22.5%) and smoked (30.0%versus 27.2%) more frequently than their urban counterparts. Rural participants reported higher frequencies of olfactory decline (43.4%versus 19.0%), hearing decline (63.7%versus 41.9%), hypertension (68.8%versus 64.5%), and insomnia (56.3%versus 45.1%) (Supplementary Table 3).
Prevalence of MCI and dementia
The crude prevalence rates of MCI and dementia in HMACS were 25.98%(95%CI: 24.99–26.96) and 7.24%(95%CI: 6.68–7.80), respectively (Table 2). After standardization for age and sex using data from the 2010 population census in Hubei Province, the prevalence rates of MCI and dementia were 26.28%and 6.98%, respectively (Table 2). However, significant differences in MCI and dementia prevalence rates were observed between the rural and urban cohorts. The rates of MCI and dementia in the rural cohort were 1.33 (32.13%versus 24.14%) and 2.65 times (12.68%versus 4.83%) than those of urban areas, respectively (Table 2). These results indicated that MCI and dementia were more prevalent in rural than in urban areas.
The prevalence of MCI and dementia in HMACS by residential areas
MCI, mild cognitive impairment; HMACS, The Hubei Memory & Aging Cohort Study; 95%CI, 95%confidence interval; PR, standardized prevalence ratio.
In both rural and urban cohorts, the prevalence of dementia increased significantly with age, reaching 23.2%(95%CI: 18.7–27.8) and 16.1%(95%CI: 13.3–18.8), respectively, among individuals aged≥80 years. It was also higher in women; in patients with chronic diseases, such as diabetes (rural: 12.1%versus 11.7%; urban: 6.0%versus 4.0%) and cerebrovascular disease (rural: 14.7%versus 11.3%; urban: 6.1%versus 4.0%) (Table 3); and in those who tended to live alone and have poor social connections or a lower education level. The same trend that was observed for dementia in subgroups with variable characteristics, except for education, was also observed for MCI (Table 3).
Prevalence and 95%CI for MCI and dementia in HMACS by selected factors
*p < 0.05; **p < 0.001; MCI, mild cognitive impairment; HMACS, The Hubei Memory & Aging Cohort Study.
Logistic analysis for selected risk factors
As shown in Table 4, the risk of dementia increased significantly with age in urban and rural cohorts and increased with the decrease of education only in urban cohorts (odds ratio [OR]: 2.614; 95%CI: 1.393–4.905; p < 0.001). Nevertheless, it was lower in women only for the rural cohort (OR: 0.650, 95%CI: 0.458–0.921, p < 0.001). Limited social connection increased the risk of dementia in urban (OR: 6.376; 95%CI: 2.231–18.255; p < 0.05) and rural cohorts (OR: 22.473; 95%CI: 9.772–51.683; p < 0.001).
Logistic regression analysis of the selected risks for MCI and dementia in rural and urban residents
*p < 0.05; **p < 0.001; OR, odds ratio; MCI, mild cognitive impairment. We set up one logistic regression model to ascertain the risk factors associated with MCI or Dementia considering the effects of gender, age, education level, living arrangements, cigarette smoking, drinking, and social connections concomitantly. The analysis for MCI in rural and urban regions were based on a sample size of 2,791 (rural) and 4,835 (urban), including MCI patients and cognitively normal individuals. And the analysis for Dementia in rural and urban regions were based on a sample size of 3,164 (rural) and 5,057 (urban), including patients with Dementia and nondementia individuals.
Similar to the trend observed for dementia cases, the risk of MCI increased significantly with age in the urban and rural cohorts. Those with poor education (OR: 1.756; 95%CI: 1.386–2.224; p < 0.001) or limited social connection (OR: 4.688; 95%CI: 2.108–10.426; p < 0.001) presented increased risk of MCI among the urban cohorts, but not among the rural cohorts. The sensitivity analysis results showed that our main logistic regression model was stable, and the results were reliable. The changes in the results were very subtle when we adjusted the logistic regression model (Supplementary Table 4–6).
DISCUSSION
In this study, we established the HMACS, a community-based, longitudinal cohort. It is the first large-scale community-based cohort in Central China including both rural and urban participants, with comparable study design, procedures, and diagnostic criteria for dementia to previous cohort studies in developed regions. The inception cohort exhibits many of the common chronic diseases typical of community-based epidemiologic studies. Unlike most previous aging cohort studies, such as the well-established Shanghai Aging Study [31], the Mayo Clinic Study of Aging [32], and the Sydney Memory and Aging Study [33], HMACS offers a unique opportunity to examine aging in less developed Central China, sampling residents from both metropolitan and remote rural areas; indeed, nearly 41.7%of the study participants had less than a middle-school degree. All participants received comprehensive epidemiologic and neurologic in-person assessments at community health centers and township hospitals. Consensus diagnostic criteria were applied to all participants. It should be noted that this study used a standardized procedure of cognitive screening to provide sufficient evidence to simultaneously diagnose MCI and dementia. In addition, the HMACS collected a large variety of individual, family, social, mental, and physical health variables, which enabled more complex analyses of the interplay between these factors and cognitive aging indicators in later life. A large team of community family physicians was recruited to participate in HMACS. These clinicians had well-established histories with the participants and were familiar with their personal and family situation.
The baseline data for the HMACS revealed the marked urban-rural disparity. There was a notably higher prevalence of MCI (32.13%versus 24.14%) and dementia (12.68 %versus 4.83%) in rural than in urban areas, and education may be an important reason for the rural-urban differences. There was a clearly higher proportion of poorly educated individuals in rural (75.2%) than in urban areas (20.7%), and the notably higher prevalence of dementia among those who were less educated supported this observation. Surprisingly, with the improvement of education level, the prevalence of MCI gradually increased in rural participants, although only 70 participants from rural areas had a high level of education, and they could not find jobs in cities because of various personal issues; therefore, they had to live in rural areas. The age-specific prevalence of MCI and dementia in HMACS shows a strong relationship with chronological age. The HMACS reveals large residential area-related differences in multiple dementia-related risk factors to the disadvantage of rural participants, especially in education, social connections, cognitive activities, and diet pattern. Good social connections were associated with reduced rates of MCI and dementia. These findings were consistent with the results of previous studies [34, 35].
Compared with the most recent epidemiological studies on dementia [31, 37], the prevalence of dementia in our study was estimated in an older population, with a higher proportion of participants with low education (47.1%), occupations involving “heavy labor” (46.5%), poor economic level (84.8%people earned <1,000 Chinese Yuan per month), and ordinary living environment (30.6%of participants had limited social connections). In this study, we excluded individuals who could not communicate or those who were living in institutions, such as nursing homes and psychiatric hospitals. Thus, we could have missed some potentially severe dementia cases and, therefore, we could have underestimated the prevalence of dementia. Interestingly, we had excluded the people who already had dementia from the study population, which might also lead to a lower prevalence rate than the actual prevalence rate. However, 48.5%of our participants reported some degree of hearing impairment, such that scores may be affected by the hearing decline. In addition, it should be noted that HMACS is an area-specific, not nation-wide study. By its nature, the study is confined to Hubei province, although efforts are underway to establish parallel studies in other provinces of China. Therefore, the calculated prevalence could not be generalized to the entire Chinese population.
Participants will be followed-up via face-to-face interviews every 4 years to examine the progression of disease states, and to identify risk factors and biomarkers for preclinical detection of incipient cognitive disorders. Attrition is an ongoing issue. The estimated rate of dropouts from this ongoing follow-up examination was 20%. It is necessary to refresh the sample to maintain an appropriate proportion of participants and to facilitate cross-cohort comparisons. First, HMACS will be entering successive age cohorts of targeted community residents into the study, as they attain 65 years of age. Second, a random cohort of non-participants will be selected and followed alongside participants using the same national databases.
In conclusion, the HMACS was designed as a prospective community-based study of cognitive impairment in older Chinese adults. The baseline data showed that the prevalence rates of MCI and dementia were notably higher in rural than in urban areas, and that the risk factors for dementia differed between urban and rural populations. This study provides a better understanding of most patients with dementia who receive care at home in China by enrolling a large and representative sample of the community-dwelling population.
Footnotes
ACKNOWLEDGMENTS
We thank all the study participants and all the graduate students for their participation. We also thank the physicians, nurses, and clinical supervisors for their contributions, and the field coordinators at the Qinglinjie, Gangduhuayuan, and Liyuan community health centers and Dawu Chinese traditional medicine hospital.
Financial support for the present study was received from National Natural Science Foundation of China (No. 81870901 and 82071272 to Y.Z., No. 81771488 to H.X.D., No. 71774127 to D. L) and Ministry of Science and Technology of China (No. 2020YFC2006000 to Y.Z.). The financial contributors had no role in the design, analysis, or writing of this article.