
Abstract
Mild traumatic brain injury (mTBI) is the most prevalent type of TBI (80–90%). It is characterized by a loss consciousness for less than 30 minutes, post-traumatic amnesia for less than 24 hours, and Glasgow Coma Score of 13–15. Accurately diagnosing mTBIs can be a challenge because the majority of these injuries do not show noticeable or visible changes on neuroimaging studies. Appropriate determination of mTBI is tremendously important because it might lead in some cases to post-concussion syndrome, cognitive impairments including attention, memory, and speed of information processing problems. The scientists have studied different methods to improve mTBI diagnosis and enhanced approaches that would accurately determine the severity of the trauma. The present review focuses on discussing the role of biomarkers as potential key factors in diagnosing mTBI. The present review focuses on 1) protein based peripheral and CNS markers, 2) genetic biomarkers, 3) imaging biomarkers, 4) neurophysiological biomarkers, and 5) clinical trials in mTBI. Each section provides information and characteristics on different biomarkers for mTBI.
INTRODUCTION
Traumatic brain injury (TBI) is an acute brain damage that is caused by mechanical injury to the head from external physical forces due to motor vehicle accidents, neurotrauma and/or sport collisions [1, 2]. TBI incidence has been estimated worldwide with 69 million cases per year [3]. In 2014, ∼2.87 million TBI cases were reported in the USA, and from them, 837,000 were children [4, 5]. The severity of TBI is divided into three groups, based on clinical evaluation and the Glasgow Coma Score (GCS): severe, moderate, and mild [6]. The most common type of TBI is mild (mTBI) and very often is mentioned in the literature as concussion [3]. mTBI is defined as a trauma of head that affects normal function and physiology of the brain, causes loss of consciousness for less than 30 minutes, post-traumatic amnesia for less than 24 hours, and GCS 13–15 [7]. mTBI accounts for approximately 80–90% of all TBI cases [5, 9]. Other authors calculate that this may correspond only to the 10–25% of the total people suffering of mTBI; accordingly, estimated values may vary depending on the studies [10–12]. mTBI patients exhibit symptoms such as headaches, neck pain, nausea, dizziness, vomiting, and amnesia; symptoms that could be associated to the brain injury and upon further examination [6, 13]. The majority of the mTBI cases are uncomplicated; no visible lesions on non-contrast head computed tomography (CT) are found and the symptoms are only persistent for up to 3 months [14, 15]. A minority of mTBI cases have shown detectable brain damage that leads to other health complications [16, 17]. 5–10% of mTBI will progress to post-concussion syndrome (PCS) and will have several physical, cognitive, and behavioral symptoms, which can persist for months, years, or be permanent [18]. In these more severe mTBI cases, physiopathological changes such as inflammation, cellular injury, and cellular stress can be detected in the brain and could be responsible for further brain dysfunction [19]. Imaging studies have shown that PCS causes visible brain damage in both white and gray matter as well as metabolic changes [20, 21]. Children and adolescents are more susceptible to develop PCS after a mTBI [22]. The diagnosis of mTBI may differ among the studies but it is based on the following course: GCS values, loss of consciousness (LOC), post-traumatic amnesia (PTA), and brain imaging such as CT and magnetic response imaging (MRI), single photon emission computed tomography (SPECT), positron emission tomography (PET), and magnetic resonance spectroscopy (MRS) can provide very useful information [23–25]. An accurate diagnosis for mTBI has become a main focus in the healthcare community as it a risk factor that leads to post-concussion syndrome, cognitive impairments including attention, memory and speed of infor-mation processing problems and its relationship with neurodegenerative diseases like chronic traumatic en-cephalopathy (CTE), dementia, Parkinson’s disease, and amyotrophic lateral sclerosis are still under study [26–30]. Figure 1 reveals the classification of TBI based on the symptoms: mild (80%) with GCS ranging from 13–15; moderate (10%) GCS score 9–12, and severe (10%) with GCS < 8 [24–28]. Figure 1 also summarizes the diagnostic (history, measures, imaging), prognostic (biomarkers) and treatment (rest, medications, possible targeted approach) based on the stages of TBI. The appro-priate diagnosis and efficacious treatment still remains a challenge. Moderate to severe TBI can manifested by slurred speech; profound confusion; seizures, persistent headaches, and coma at times [24–28].
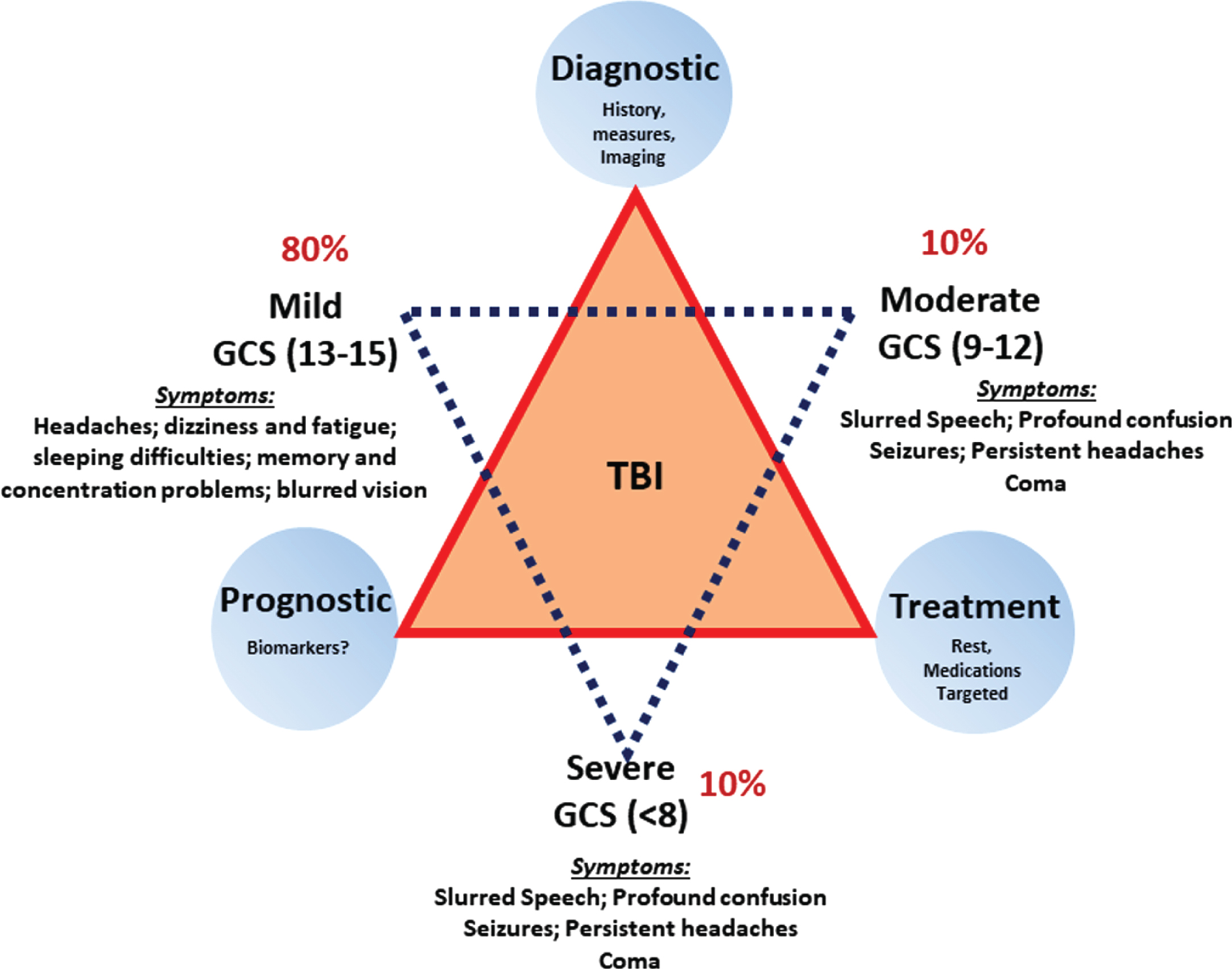
Classification of TBI based on the symptoms- mild (80%) with Glasgow Scale Score (GCS) ranging from 13–15; moderate (10%) GCS score 9–12; and severe (10%) with GCS < 8. Symptoms of mild to severe are listed based on the stages of the TBI; diagnostic (history, measures, imaging) and prognostic (biomarkers) to treatment (rest, medications, possible targeted approach) based on the stages of TBI.
The criteria used for classifying TBI into mild, moderate, and severe is based on structural imaging-normal in mild and normal to abnormal in moderate and severe; loss of consciousness (< 30 minutes in mild, 30 minutes to 24 hours in moderate, and > 24 hours in severe) and Glasgow Coma Scale (score of 13–15 for mild, 9–12 for moderate, and 3–8 for severe) [24–28] (Table 1). According to the literature, the screening of biomarkers is a promising way of diagnosis of mTBI [31]. Biomarkers such as proteins, microRNA (miRNA), and lipids as diagnostic/prognostic biomarkers have been reported in the literature using biological samples such as blood serum, plasma, cerebrospinal fluid (CSF), hair follicle, saliva, and urine as sample sources [31, 32]. In addition, miRNAs expressed in exosomes, are known to play an important role in regulating gene expression, and protein synthesis in mTBI [32]. Scientists believe that the combination of biomarker’s screening along with imaging studies could lead to an increase in the mTBI diagnosing accuracy [33–38]. While research on mTBI is highly relevant to understand the underlying pathophysiology that allow more consistent diagnosis of mTBI by the development of a suite of biomarkers that could lead to establish clinical tools for both diagnosis and prognosis. Hence, in the current review, we discuss about the mTBI biomarkers categorized as biological, imaging, and neurophysiological markers.
Criteria used to classify TBI into mild moderate and severe based on structural imaging (normal in mild and normal to abnormal in moderate and severe), loss of consciousness (< 30 minutes in mild, 30 minutes to 24 hours in moderate, and > 24 hours in severe) and Glasgow Coma Scale (score of 13–15 for mild, 9–12 for moderate, and 3–8 for severe)
Candidate protein biomarkers of mTBI, the table summarizes studies from the literature, with the type of injury specific to mTBI, type of method, study findings and the sample source
PERIPHERAL AND CNS BASED BIOLOGICAL BIOMARKERS IN mTBI
Biomarkers can be broadly classified based on the physiological, biological, and functional state of a subject at a given point of diseased state [39]. Biomarkers are also categorized as diagnostic, prognostic, and therapeutic to understand the state of the brain injury. In the present section, we will discuss both peripheral and CNS protein-based markers that are specifically expressed in mTBI. Table 1 summarizes the candidate protein biomarkers of mTBI, based on the studies conducted from the literature, with the type of injury specific to mTBI, type of method, study findings, and the sample source.
Astrocyte damage
S100β
S100β is a biomarker that belongs to a family of proteins known as S100. This protein requires to be a dimer to acts as a functional protein. S100β is a calcium-modulated protein of EF type; consequently, S100β is involved in regulating intracellular calcium homeostasis [40, 41]. The main role of S100β is in the glia proliferation [40, 41]. S100β has been studied as a biomarker for many types of TBI and its main role is in calcium homeostasis, cell survival, and differentiation [40, 43]. Most recently, studies have shown that S100β is a potential biomarker to determine mTBI in both adults and children [31, 44–50] due to the alteration in the levels of S100β in the blood serum. Several groups have studied blood plasma and urine as possible sources for the identification of S100β levels in mTBI patients [43–50]. In adults with mTBI, S100B levels in blood serum have been shown to be higher when compared to control [46]. Additionally, a study conducted by Vos et al., also confirmed increased levels of S100β in blood serum among adults with mTBI [51].
Glial fibrillary acid protein (GFAP)
GFAP, a protein marker for astrocytes and is only expressed by glia cells [52]. Studies from the literature support the hypothesis that GFAP is released in response to mTBI [51, 53–55]. Recently, studies have shown increase levels of GFAP in blood serum after mTBI in adults and in younger adults [56]. GFAP might serve as a great candidate for determining and diagnosing mTBI; however, additional studies with large number of samples are required to validate these findings
Myelin basic protein (MBP)
MBP is a key component of the myelin and it is only expressed in myelinated cells, such oligodendrocytes and Schwann cells [57]. Like other proteins, MBP has been studied as a possible biomarker for neuronal damage. In children with TBI, MBP levels were found to be elevated in the CSF samples [58]. Additionally, MBP levels in blood serum were also elevated in mTBI patients [59]. A large number of studies have shown MBP to be a promising biomarker in diagnosing patients with different types of TBI [34, 60].
Cytokines and inflammatory proteins
Inflammatory proteins, such as IL-6, IL-8, and IL-10, are known to be increased in the CSF following injury [61]. It still remains elusive if this immune response is an association between proinflammatory proteins and poor clinical outcome in mTBI. A pilot study on 16 pediatric mTBI patients showed increased concentrations of IL-6 and MMP9. Increased blood-brain barrier (BBB) permeability due to mTBI might be a causative factor for elevation of these proteins. Such damage leads to the elevation of a marinobufagenin (MBG), a cardiotonic steroid substance is released in response to renal artery stenosis in humans [62]. MBG initiates inflammation and also maintains the inflammatory response; therefore, MBG levels in the circulation have been suggested as a potential mTBI biomarker [63]. Urine MBG levels are elevated in concussed players, typically peaked between two and five days after injury, and correlated with neurocognitive symptoms. Additional studies are required to understand these inflammatory response molecules, to yield for potential biomarkers for mTBI [64].
Tau protein
The tau protein belongs to a group of proteins known as microtubule associated-proteins (MAPs) [65]. The main role of tau protein is to promote the polymerization of the microtubules during the axonal growth [65, 66]. Recent evidences have shown that the tau levels increased either in CSF or blood serum as a response to different types of neuronal damage [67–70]. The studies focusing on neural damage such as TBI have shown that significant levels of protein tau were elevated as a response to the trauma in both animal models and human [71–73]. Based on this evidence, tau protein might serve as a biomarker for different types of neural damage such as occur in mTBI [72–75].
Ubiquitin carboxyl-terminal esterase L1 (UCHL1)
UCHL1 is a small protein containing 76 amino acid residues and is a C-terminal hydrolase, a deubiquitinating enzyme that can cleave or remove the C-terminal esters and amines of ubiquitin in order to produce free ubiquitin monomers [76, 77]. An important aspect to consider is that the expression of UCHL1 is very restricted to neuronal cytoplasm, testis, and ovary [78]. UCHL1 has been studied as a possible biomarker for neuronal damage because it is a protein that can be released to the blood plasma in response to a neuronal damage, especially in the case mTBI. Furthermore, studies have shown that UCHL1 levels were increased in mTBI patients [79]. While UCHL1 can be used as a biomarker to potentially diagnose mTBI, a research study conducted by Puvenna et al. (2014) did not find any changes in levels of UCHL1 in response to neuronal damage [80]. Therefore, the use of UCHL1 as a biomarker needs to be used with caution [75].
Neurofilaments (NFLs)
NFLs are a group of proteins that are part of the cellular cytoskeleton and the intermediate filaments. NFLs are subdivided in three groups based on the molecular weight: neurofilament heavy chain (NFL-H), neurofilament medium chain (NFL-M), and neurofilament light chain (NFL-L) [81]. Several studies have shown that NFLs can be released into CSF or blood serum in response to an axonal injury [81–85]. Depending on the tissue used and the study’s focus, the NFLs can be used as biomarkers for axonal/neuronal damage and many other diseases. Current evidence has shown that all three NFLs levels increase in response to different types of neuronal damage including mTBI. Used as a biomarker, NFL-L levels in blood serum showed an increase in patients with mTBI in comparison to the control group [86–88]. Another study found that NFL-M levels were significantly higher in patients with mTBI in both CSF and blood serum [38]. Lastly, further studies using NFL-H as a biomarker, showed higher levels of phosphorylated NFL-H (pNFL-H) in mTBI patients in blood serum and CSF samples [82, 89].
Enolase 2 (NSE)
NSE is a phosphopyruvate hydratase neuronal-specific enzyme, and it is part of the glycolytic pathway [90]. A study conducted by Stålnacke (2004) showed an increase of NSE levels in blood serum from patients with mTBI [91]. However, another study showed that levels of NSE either did not significantly change in comparison to the appropriate control, or did not change [44]. The debate argues that NSE may not be used as a biomarker or by itself for the purpose of diagnosing mTBI; however, it is possible that in combination with other mTBI biomarkers, it may positively contribute to diagnosing mTBI more accurately [92]. Research studies using NSE as a biomarker for mTBI are scarce and more studies are needed to conclude its usefulness as brain injury biomarker.
Neutrophil gelatinase-associated lipocalin (NGAL)
NGAL, also known as Lipocalin-2 (LNC2), is a small protein of 25 kDa which is associated to the protein gelatinase lipocalin [93]. NGAL binds small lipophilic substances derived from bacteria and it is involved in immune system responses [94]. High levels of NGAL, both mRNA and protein levels, increased in response to brain injury, such severe TBI. However, this biomarker can also be increased in kidney damage, therefore abnormal levels should be examined closely [75]. Based on the literature, this protein can be used as a biomarker for certain brain injuries as NGAL levels can reflect the severity of neuronal damage; in other words, the more severe the damage, the higher the levels of NGAL in blood plasma. Overall, NGAL could be useful in determining the type and severity of mTBI [95].
Prions/plasma-soluble cellular prion (PrPC)
PrPC is a glycosylated membrane and soluble protein in blood plasma [96]. According to research studies in both rodents and humans, different types of brain damage produce a significant increase of PrPC in plasma samples compared to healthy subjects. This evidence indicates that PrPC could be a promising biomarker for the diagnosis of TBI [97, 98]. A recent study conducted by Pham et al., (2015) determined that PrPC was elevated in confirmed concussion cases, hence can be used as a biomarker to mTBI in humans [99]. However, studies using this biomarker in diagnosing mTBI are limited. A validated and reliable panel of diagnostic biofluid TBI biomarkers such as protein-small metabolites and amino acid markers can reduce the harm of radiations by imaging. A study conducted by Hajiaghamemar et al. (2020) utilized robust panel of biomarkers and multivariate logistic regression analysis, on several subsets of amino acids such as serum glycine, taurine, and ornithine with a high sensitivity and accurate prediction rate [100]. Refer to Table 1 for the complete list of protein biomarkers of mTBI.
GENETIC BIOMARKERS OF mTBI
A few genetic markers are being tested for applicability as mTBI biomarkers. Potential genetic variations affecting the pathophysiologic biomarkers could potentially contribute to the susceptibility of an individual to an injury and to the likelihood of developing secondary sequelae, such as PCS and CTE. Apolipoprotein E (APOE) and brain-derived neurotrophic factor (BDNF) are two important candidate markers for mTBI [101, 102]. The BDNFVal66Met allele is linked to a higher risk of experiencing memory deficits after mTBI [103, 104]. Also SNP rs1157659 could be a biomarker for a high risk of getting a neurodegenerative disease after mTBI [102]. The epsilon 4 allele of the APOE gene is one of the biggest risk factors for development of neurodegenerative diseases such as Alzheimer’s disease [105, 106]. The studies in the military population with mTBI and APOE4 genotype showed cognitive impairment with reduced memory and processing, APOE4 itself did not show any adverse effect in the military population based studies [107]. In other studies, APOE4 in combination with mTBI have showed an impairment of verbal memory [108] and increase of getting a neurodegenerative disease such Alzheimer’s disease [109].
The microRNA is an emerging biomarker that has shown promise with clinical applications for mTBI. Johnson et al. (2018) showed that salivary microRNAs may be a useful biomarker for the prediction of post-concussive syndrome in children, allowing clinicians to offer patients more informed management options [110]. For these potential candidates, the effect and sample sizes were quite small. Much larger samples are required to validate and replicate these findings for spurious results. However, the falling costs of sequencing and the increasing availability of deep-sequencing methods make genetic biomarkers attractive candidates for future inquiry. Di Pietro et al. (2017) described decreased levels of two miRNAs in patients with mTBI and extracranial injuries that allowed them to clinically distinguish these patients from those with severe TBI [111]. Additionally, LaRocca et al., (2019) revealed that certain miRNAs derived from blood serum and saliva showed associations with the outcomes of cognition and balance following TBI, which has potential for further research and clinical applications [112].
IMAGING BIOMARKERS OF mTBI
mTBI may be caused by a variety of mechanisms, such as motor vehicle accidents (MVAs), falls, assaults, and more. Despite efforts to reduce the frequency of TBI due to MVAs, TBI remains a common chief complaint in emergency department (ED) visits particularly due to a rise in incidence of older adult fall-related TBIs [113]. A study conducted by Lagerstedt et al. (2018) aimed to discover a novel diagnostic biomarker of mTBI utilizing broad range of inflammation biomarkers in CT-positive and CT-negative patients (total of 133 mTBI patients). Interestingly they found IL-10, as one of the clinically useful markers with 100% sensitivity, to differentiate CT-positive and CT negative mTBI patients [114].
Head computed tomography (CT)
Head CT without contrast is done to rule out processes that may require urgent medical attention or surgical intervention, and also to rule out subsequent sequelae and assess short-term and long-term prognosis in mTBI [115]. Recently, studies have suggested the value of simultaneous facial and head CT scans in patients with suspected TBI as patients with TBI have higher frequency of facial fractures. These fractures may be overlooked in a routine head CT and may require surgical intervention [116]. A study conducted by Lagerstedt et al. (2018) showed that levels of interleukin-10, an anti-inflammatory protein, could help predict whether or not a patient with a mild TBI would have a positive finding in a head CT [114].
Magnetic resonance imaging (MRI)
A brain MRI is usually not indicated for mild TBI; however, in the setting of a patient with a normal head CT and persistent or worsening neurological deficits without cause, a brain MRI may be used [117]. The studies have shown that brain MRI abnormalities are occasionally found in patients suspected of mild TBI with a normal head CT; these abnormalities are described as lesions “consistent with axonal injury”. [118]. Recent studies have attempted to increase the sensitivity and specificity of these studies by investigating how the diffuse axonal injury (DAI) locations in TBI cases may be affected future prognosis. A study conducted by Mittl et al. (1994) concluded that DAI findings in the brainstem, substantia nigra, and mesencephalic tegmentum have been correlated with a worse neurocognitive prognosis [118]. Furthermore, the number of cortical contusions found in brain MRI and head CT scans may be a potential predictor of patient outcomes in cases of moderate TBI [119]. This is further supported by Abu et al. (2017) which found that increased number of lesions in the substantia nigra and mesencephalic tegmentum is correlated with a poor long-term outcome in DAI [120]. There have also been investigations in regards to white matter changes in the brain which occur after mTBI. A recent study found that out of 104 mTBI subjects, 27% were found to have white matter changes via MRI unrelated to age and 26 of these findings were unrelated to acute trauma [121]. Cortical thickness on MRI is another potentially useful biomarker, as studies revealed that patients who suffered an mTBI revealed cortical thickness in the right superior parietal and left middle temporal areas. The thinning of the cortex was observed with different treatment groups, indicating these could be possibly tracked in patients with mTBI [122].
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI)
Damage to the BBB due to mTBI is a secondary molecular mechanism. This disruption can alter the regulation of interstitial fluid microenvironment and therefore cause improper function. Identifying the severity that BBB has undergone as a result of trauma is a critical step in the process of developing therapeutic treatments in order the ameliorate and address the possible repercussions of the injury. DCE-MRI is a neuroimaging tool that provides sequential images during the passage of a contrast medium. DCE-MRI has been used in determining BBB dysfunction in stroke survivors and animal models [123]. Currently, there is no test that assesses BBB damage following a brain injury. Identifying the baseline and any abnormalities of the BBB following mTBI would allow for the improvement of more accurate test in diagnosing mTBI as well as developing new therapeutic treatments. A study conducted by Winter et al. (2015) tested the use of DCE-MRI and SPECT in TBI patients; their results suggest that either one of these neuroimaging tools can be a significant tool in determining BBB alterations [123].
Susceptibility weighted images (SWI)/quantitative susceptibility maps (QSM)
Other modalities such as SWI/QSM have been investigated to effectively classify the severity of TBI as well as assess neurocognitive outcomes. These methods are used to measure the brain venous volume above the lateral ventricle, which was found to be significantly increased in patients with mTBI compared to controls [124]. Other studies have shown that SWI should be also implemented in the diagnostic steps as it can provide information regarding possible cerebral microbleeds, aid with determining the severity of the injury and treatment development [125, 126].
Diffusion kurtosis imaging (DKI)
DKI has also been considered as a possible diagnostic tool in the assessment of TBI. It has been speculated that TBI may result in changes in brain microstructure, one study found significant white matter changes in patients with acute TBI and at three-months post-injury. More evidence is need to ascertain the value of DKI to detect these changes [127]. A study conducted by Karslen et al. (2019) showed that patients with TBI are also at risk of developing post-concussional syndrome, which has been associated with microstructural alterations [128]. With the use of DKI, these abnormalities can be detected with DKI. In another study conducted by Grossman et al. also identified structural alterations in patients with mTBI using DKI [129]. Overall, studies have shown the potential of DKI as a tool to identify and track physiological changes as a result of mTBI [130].
Diffusion tensor imaging (DTI)
DTI is a more sensitive neuroimaging tool that can detect microstructural axonal injury in mTBI. New techniques have allowed for the analysis of specific brain regions affected as a result of a brain injury [131]. Regular neuroimaging tests often do not reveal any visible damage; consequently, the sensitivity of DTI may show the white matter microstructural alterations and, therefore, indicate the damage caused as a result of mTBI [131]. Aoki et al. (2012) conducted a study to assess if DTI can detect white matter damage in mTBI patients via systematic review and meta-analysis. In this study, 28 DTI studies were considered for the meta-analyses, only 13 independent DTI studies of mTBI patients were eligible for the data analyses [131]. The random effect model demonstrated significant fractional anisotropy reduction in the corpus callosum and a significant increase in mean diffusivity. Furthermore, from Aoki et al. (2012), the meta-analysis revealed the posterior part of the corpus callosum was more vulnerable to mTBI than the anterior part suggests the potential effectiveness of DTI to detect white matter damage in the corpus callosum of mTBI patients [131]. Madaan et al. (2021) conducted the study on neurocognitive outcomes, and their DTI correlates in children aged 6–16 years with mTBI. The prospective analysis included 74 children with mTBI. 17% of children with mild TBI had internalizing behavioral problems in comparison to 4% of controls [132]. There was a positive correlation between right arcuate fasciculus mean diffusivity and vascular cognitive impairment.
Traumatic cerebrovascular reactivity injury (TCVI)
TBIs can cause functional deficits and disabilities that affect day to day activities. One of the mechanisms believed to be related to TBI is TCVI [133]. TCVI has been a focus of treatment development after TBI due to the high cerebral vasculature of the brain. A study conducted by Amyot et al. (2018) tested the spatial distribution of TCVI in TBI using MRI and determined the possible use of cerebral blood flow and cerebrovascular reactivity (CVR) as biomarkers for TCVI. Their results showed that CVR corresponded better with TBI symptoms and therefore may have high potential in becoming a biomarker for TCVI [133]. Another study by Kenney et al. (2016) showed that measuring the cerebral microvascular dysfunction after a TBI can not only expand the understanding of the pathophysiology of TCVI, but also give more insight into developing more specific treatments after a TBI has occurred [134]. All in all, TCVI has shown to be related to impaired cognitive behavior as a result of a TBI. Even though these studies focused on other TBI severities, it focuses on a potential biomarker that could also be used in diagnosing and treating mTBI.
NEUROPHYSIOLOGICAL BIOMARKERS
Electrical biosignals in the nervous system have the potential to serve as neurophysiological biomarkers for the diagnosis and treatment of mTBI. There are several methods to measure electrical biosignals, two of which include electroencephalograms (EEG) and magnetoencephalograms (MEG). An EEG measures the electric current between two electrodes, while a MEG measures the magnetic field that is created by the electric current in the brain.
Electroencephalography
EEG has shown potential for use as a clinical biomarker for TBI. In response to stimuli, the brain creates event related potentials (ERPs) that can be classified as either event-related synchronization or event-related desynchronization (ERD). The changes in brain oscillations are measured can be measured with EEG. A study conducted by Arakaki et al. (2019) examined working memory processing in 13 patients with a history of mTBI. When compared to 7 control patients who had a history of mild peripheral trauma, the mTBI patients displayed a marginally greater power of alpha ERD on quantitative electroencephalogram (qEEG) during a low workload task (the qEEG measurements were taken within 5 days of the injury). The study also found the induced alpha ERD did not return to baseline in the mTBI patients when compared to the control patients. Additionally, it was found that parietal evoked alpha ERD/event-related synchronization was greater in mTBI patients when compared to mild peripheral trauma patients after 2 weeks from the onset of injury [135].
EEG abnormalities within a population of 71 service members were performed, all of whom had a history of mTBI and continual post-concussive symptoms [136]. Approximately 39% of the participants displayed baseline slowing on EEG [136]. An observational, prospective validation trial was performed in 11 U.S emergency rooms on 720 patients who had a history of TBI with a Glasgow Coma Scale (GSC) of 12–15. The study was designed to assess the validity of using a quantitative brain electrical activity algorithm named AHEAD 300 to determine whether or not the patient received a head CT. All measurements of brain electrical activity were taken within 72 hours of the injury. The study found that the AHEAD 300 Algorithm showed potential use as an EEG-based biomarker for TBI with a sensitivity of 92.3% (95% [CI] = 87.8% –95.5%) and a specificity of 51.6% (95% [CI] = 48.1% –55.1%).
Magnetoencephalography
MEG also has proven to hold the possibility for future use as a clinical TBI biomarker. A study conducted on 26 patients with mTBI found abnormal theta band MEG activity in 7 of the patients. The authors also found that the abnormal MEG activity was only found during their initial recordings, 6–26 days after the mTBI, for some participants. These findings suggest the need for further evaluation of the clinical use of MEG promptly after injury in symptomatic patients with mTBI [137]. Another study performed on 30 patients with a history of mTBI analyzed the interactions between oscillations at different frequency bands, also known as cross frequency coupling. The study compared the mTBI patients with 50 controls and found that controls had a higher functional integration of neural networks [138]. It has also been discovered that phase locking value, a complex measurement of phase interactions in the brain is reduced in patients with mTBI when compared to controls. A study was done on 9 patients with a history of mTBI and persistent post-concussive symptoms. The reduction took place predominately in the delta band; however, the alpha and beta phase locking also showed reduction. In addition, most of the phase locking value reduction occurred in the parietal and occipital lobes [139].
In a retrospective study on 30 mTBI patients from MEG programs at the University of Utah and the Albuquerque Veterants Affair Medical Center (VAMC), it was found that a fifth of the patients displayed intermittent epileptic spikes on MEG despite none of them reported having clinical seizures. From a pool of 30 patients, only 19 had abnormal dipolar slow wave activity. In addition, 10 of the patients showed no abnormalities on MRI or SPECT, but still showed EEG abnormalities [140].
CLINICAL IMPLICATIONS OF BIOMARKERS AND CLINICAL TRIALS
Basic science research has uncovered a vast array of biomarkers of mTBI that are being utilized to diagnose, predict clinical outcomes, track recovery, and guide therapeutic interventions. Given the high incidence and disease burden of mTBI, the development of clinical applications from biomarker research stands to have a significant impact on public health. The use of biomarkers in the management of TBI is expanding, including the recent approval of a test utilizing GFAP and UHCL1 in blood to help rule out the need for head and brain imaging in the case of mTBI (https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-blood-test-aid-evaluation-concussion-adults).
Beyond discovery of a biomarker, whether through hypothesis-driven or unbiased methodology, further work must be done to validate the biomarkers and assess their clinical utility in mTBI. The goal of the mTBI study is determine if the blood biomarkers drawn during the transit to the hospital in patients who have suffered head trauma can be used to decrease the need for extensive workup by ruling out intracranial pathology (NCT02867137).
For mTBI, the relative impracticality of CSF collection has led to investigations of blood, saliva, and urine-based as biomarkers of management and prognosis [141]. The current clinical trials are investigating the effects of therapeutic interventions based on prognostic and diagnostic biomarkers of mTBI. One ongoing study is looking at the effect of pulsed electromagnetic fields on TBI (NCT03654014). Another study is looking at the effect of repetitive transcranial magnetic stimulation on performance of memory tasks and how this correlates to the biomarker of functional connectivity between brain regions in individuals with TBI (NCT03050801). As biomarkers are discovered and their relationship to the pathophysiology of mTBI is elucidated, researchers will be better at determining targets for intervention design therapies.
The effort to discover and understand the clinical implications of biomarkers in mTBI is active and expansive. These abundant findings need to be collected and organized to be used for the clinicians in their daily practice. The TRACK-TBI effort is currently developing a directory for all types of biomarkers in order to hone the guidelines for diagnosis and care of TBI patients (NCT02119182). The continued investment in clinical trials that are aimed at correlating the appearance, dynamics, and response to therapy of biomarkers of mTBI will bolster this endeavor and lead to the development of novel clinical tools. Clinical trial related to mTBI studies and the reference numbers are extracted from http://www.clinicaltrials.gov.
CONCLUSION AND FUTURE PERSPECTIVES
In the US, it is estimated that millions of people are affected every year by TBI, the great majority being mTBI. According to the literature, patients with mTBI exhibit symptoms for up to three months; however, no visible brain damage is seen in most of them. It is estimated that 5–10% of mTBI cases present with detectable brain damage that can lead to post-concussion syndrome with physiopathological changes, and the risk of developing health issues such as neurodegenerative diseases [6, 26–30].
Many scientists have studied the aftermath effects of an mTBI. They have found that as a result of the injury, there is a release of molecules into the blood serum. Using these molecules as biomarkers may aid in the diagnosis of mTBI and possibly give light into the severity of the injury [31, 33–38]. While some biomarkers are useful for diagnosing TBIs, they can oftentimes not be used for mTBI patients. For instances CSF would not be useful for mTBI as the CSF/serum albumin ratio would not provide any significant insight for the disease [142, 143]. In contrast, glia-derived biomarkers such as S100β, MBP, and GFAP have been extensively studied as biomarkers for mTBI. Based on the literature, all three have strong evidence that they can be useful in diagnosing mTBI patients [31, 60].
Additionally, another idea considered is that a group of proteins are released as a result to neuronal damage/injury. To expand, these proteins are expressed in neurons, therefore any damage will lead to a release of these proteins into the serum. However, based on the literature, there are certain proteins that have been considered for biomarkers mTBI, such as tau, but the data has not shown a strong enough to support diagnosing of mTBI [72–75]. Furthermore, contradictory data on two other proteins, UHCL1 and NSE, have also made it difficult to consider these as biomarkers [6, 91]. Another study showed that on prions, PrPC is a very promising biomarker candidate, but not enough evidence has suggested that it can be used as a biomarker, specifically for mTBI [98, 99]. While many proteins have been considered but not fully supported by their data, two protein genes have shown to be useful biomarkers in diagnosing mTBI, APOE and BDNF. While these may be useful as diagnosing biomarkers, they are also implicated in neurodegeneration [102, 109]; which could shed light into developing a technique to use these as a potential biomarker, in determining possible future neurodegeneration as a result of mTBI. Testing for biomarkers can be done through the use of different samples such as blood serum, blood plasma, or CSF [33–38]. In 2018, the FDA allowed the first blood test to be used in evaluating mTBI based on the GFAP and UCHL1 levels. The results take 3–4 hours and can help in determining if a patient has intracranial lesion and will need a head CT scan.
Point of care (POC) devices are a great tool that have greatly improved health concerns such as diabetes and heart disease. The development of these devices is important because it allows for inexpensive access to diagnostic tools that could potentially save a life. These devices are defined as diagnostic instruments that allow the patient to obtain fast results without the need for additional medical staff at the time of the testing [144]. While these devices may be incredibly helpful, the disease specific POCs are somewhat limited. Nevertheless, the development of new devices targeting other diseases in underway. Taking this into consideration, developing a POC instrument that would aid with the diagnosis of an mTBI would be groundbreaking, especially in the athletic and military settings as rapid diagnosis would be greatly beneficial. Identifying the specific biomarkers for mTBI would allow for the development of a specific POC device that would test for irregularities in these biomarkers after an injury has occurred [144]. This form of diagnostic tool would give insight to the patient to determine if further medical attention is critical. Nevertheless, it is important to point out that this has yet to be developed and the biomarkers for mTBI are not concrete and more research is needed.
Overall, a lot of literature has put focus on the use of biomarkers as a diagnosing technique for mTBI. However, many do not have strong enough evidence to be used for mTBI specifically. We believe that more data is needed in order to accurately use these as determining biomarkers. It is also hypothesized that testing for a combination of biomarkers may be more accurate than one itself. Lastly, accurately diagnosing mTBI and potentially identifying irreversible damage and its effect on the individual’s health at an early stage, may give an opportunity to treat and/or try to prevent diseases to have a better quality of life.
Footnotes
ACKNOWLEDGMENTS
Bharathi S. Gadad would like to thank Edward G. and Margaret N. Marsh Foundation and Robert E. and Evelyn McKee Foundation for their support. Bharathi S. Gadad would like to thank Brain Behavior Research Foundation (BBRF)-NARSAD young investigator grant for their support.