
Abstract
Background:
The olfactory system is affected very early in Alzheimer’s disease and olfactory loss can already be observed in patients with mild cognitive impairment (MCI), an early stage of AD.
Objective:
The aim of this randomized, prospective, controlled, blinded study was to evaluate whether olfactory training (OT) may have an effect on olfactory function, cognitive impairment, and brain activation in MCI patients after a 4-month period of frequent short-term exposure to various odors.
Methods:
A total of 38 MCI outpatients were randomly assigned to OT or a control training condition, which were performed twice a day for 4 months. Olfactory testing, comprehensive neuropsychological assessment, and a passive odor perception task based on magnetic resonance imaging were performed before and after training.
Results:
The results suggested that OT exhibited no significant effect on olfaction and cognitive function. Additionally, OT exhibited a positive effect on frontal lobe activation (left middle frontal gyrus and orbital-frontal cortex) but exhibited no effect on grey matter volume. Moreover, the change of olfactory scores was positively associated with the change of frontal activation.
Conclusion:
OT was found to have a limited effect on olfaction and cognition in patients with MCI compared to a non-OT condition but increased their functional response to odors in frontal area.
INTRODUCTION
Alzheimer’s disease (AD) is regarded as the most common type of neurodegenerative dementia. Currently, there are approximately fifty million patients with AD around the world, and this number may double every 5 years and increase to around 152 million by 2050. Additionally, with estimated global burden of 1 trillion US dollars annually, AD significantly affects individuals, families, and economic development [1]. Although there are available treatments which can slow down the disease progress and improve symptoms, there is no cure for AD [2]. Therefore, early intervention of the high-risk individuals of AD is of great significance for reducing its morbidity and disease burden. Patients with mild cognitive impairment (MCI) are considered as high-risk individuals for AD [3], with a prevalence of around 3%to 22%in the elderly population [4]. Previous studies suggested that the annual rate of progression to dementia in MCI (5%to 10%) is significantly higher than in the general population (1%to 2%) [5]. A number of studies in the past examined whether drugs (e.g., cholinesterase inhibitors [6], vitamins [7]) lifestyle modifications (physical exercise [8], Mediterranean diet [9]) and physicotherapeutics (transcranial magnetic stimulation and transcranial direct current stimulation) [8] might have therapeutic effects in MCI. However, these mentioned study results did not show beneficial effects on conversion rates of dementia which might be due to methodological reasons and patient pre-selection.
The olfactory system is a potential target for the early intervention in MCI. According to Braak stages, entorhinal and transentorhinal areas are the earliest regions to be affected by AD pathology [10], and amyloid-β and tau were found early in many other olfactory regions (olfactory neuroepithelium, olfactory bulb, piriform cortex, etc.) [11]. In AD pathological progression, olfactory dysfunction may emerge parallel to tau-mediated neuronal dysfunction and occurs earlier than memory impairment and clinical symptoms [12]. Clinical evidence suggested that olfactory dysfunction was associated with worse cognitive performance [13], reduced hippocampal and entorhinal volume [14], increased cortical amyloid burden [15], lower ratios of CSF t-tau and P181-tau to Aβ1–42 [10], faster cognitive decline and a higher rate of conversion to AD in community elderly and MCI [16, 17]. Because the olfactory map strongly overlaps with the cognitive map [12], it can be assumed that improving olfactory function may contribute to AD treatment. In fact, animal and human studies suggested that modulation of entorhinal-hippocampal circuitry improved cognitive function [18], and aromatherapy contributes to relieving behavioral and psychological symptoms of in AD [19, 20], suggesting that the olfactory system may be a promising target for early intervention in AD and MCI.
Olfactory training is a novel and, in ENT, generally recognized treatment method which improves olfactory function by frequent sniffing and/or exposure to robust odors [21]. Previous studies suggested that olfactory training significantly improved patients’ olfactory function [21], subjective well-being [22] and depressive symptoms [23], and increases olfactory bulb volume [24], cortical thickness [25], functional activation and connectivity [26–28] in olfactory regions. The possible mechanism of olfactory training is that repeated odor expose may cause synapse formation and spine sprouting, then increases cell genesis of glial or neuronal cells, leading to an increase of gray matter density and altered neural function [29, 30]. However, it remains unclear whether this peripheral chemical stimulation of the olfactory system may be beneficial to cognitive function. Our previous studies suggested that 5-month olfactory training can not only improve olfactory function, but also increases verbal fluency in elderly people [22], suggesting its potential therapeutic benefit in patients with cognitive impairment.
The present study aimed to explore the effect of olfactory training on olfaction, cognition, brain structure, and brain function in patients with MCI. Additionally, the relationships between changes of olfaction, cognition, and neuroimaging indicators were further explored. Based on the recent findings mentioned above, we hypothesized that a 4-month period of olfactory training consisting of frequent short-term exposure to various odors would significantly improve olfactory and cognitive function in patients with MCI, and that the changes of brain function and structure would be associated with changes of olfaction and cognition.
METHODS
Subjects
This study is a randomized, controlled, double-blind clinical trial. Initially, 42 subjects with MCI were recruited from the Memory Clinic at the University Hospital of the TU Dresden. All participants were supplied with a detailed information sheet, provided written informed consent, and received a moderate financial compensation. The study ran from May 2019 to May 2021. The study was conducted according to the Declaration of Helsinki and was approved by the Ethics Committee of the Medical Faculty Carl Gustav Carus at the Technical University Dresden (EK 136032015). This clinical trial was conducted following the guidelines of the Consolidated Standards of Reporting Trials (CONSORT) statement and checklist.
The inclusion criteria were: 1) Age: 45–80 years; 2) Voluntariness and cooperativeness; 3) German is the dominant language if there is multilingualism; and 4) Meeting of Peterson’s diagnostic criteria of MCI [31]. The exclusion criteria: 1) Lack of consent; 2) Significant further health impairments (e.g., chronic hypothyroidism, renal insufficiency) that can be associated with disorders of the olfactory function; 3) People with acute or chronic inflammation of the nose and sinuses; 4) People with relevant previous or concomitant diseases in the ENT area; 5) A history of any other neurological or psychiatric illness; 6) History of addiction; 7) A history of electro-convulsive therapy in the past 6 months; 8) Severe metabolic diseases with impaired brain performance; 9) Medication with impairment of brain performance, e.g., benzodiazepines; 10) Structural brain damage in the MRI, even without a clinical correlate (incidental finding); 11) Pacemakers, artificial heart valves, insulin pumps, or other implants metal in the body (prostheses, vascular clips, metal dust from work); 12) taking cognitive enhancement drug.
Procedures
A total of 38 participants completed the study as four participants had incomplete datasets. The participants were randomly assigned to a training group (n = 19) and a control group (n = 19). A randomization list was thus created by the investigator and the participants were assigned to this list chronologically. Participants and investigators were blind to the grouping and the treatment conditions. All subjects underwent assessments of olfactory function, cognitive function, depressive symptoms, as well as magnetic resonance imaging scanning. The same tests were applied again after 4 months.
For the training group, patients received four brown glass jars (total volume 50 mL) with one of the four odors in each (1 mL each, soaked in cotton pads to prevent spilling). The following odors were used: phenyl ethyl alcohol (PEA): rose, eucalyptol: eucalyptus, citronellal: lemon and eugenol: cloves (all odors from Sigma, Deisenhofen, Germany)). All jars were labeled with the odor name. Patients had to sniff each odor for approximately 15 s and repeat this exercise once. They were asked to train in the morning and in the evening, resulting in a total of four exposures per day. Moreover, a “smell diary” was used after the training to evaluate whether olfactory training was performed regularly.
The control group performed the same training plan by using four odorless jars. To make sure the participants in the control group will comply with the task, we told them these jars contain subliminal odors and describe the odors the exact same way as you do with the training group. Additionally, the odor containers and labels were the same as the ones used as for the training group. Therefore, the treatment expectancies of the two groups were controlled, and the only difference between the two groups was the presence of odor in cotton pads in the containers.
Assessment of olfactory function
Olfactory function was measured using the extended “Sniffin’ Sticks” test [32] which is based on odor-containing felt-tip pens. This test consists of three subtests: odor threshold, odor discrimination (OD), and odor identification (OI) test. For each subtest, the pen’s cap was removed, and its felt-tip was presented about 2 cm in front of both nostrils of the subject for about 3 s. The testing procedure began with the odor threshold part in a triple-forced choice paradigm where participants had to discriminate the odor (PEA) from 2 blanks (filled with solvent propylene glycol). Starting with the lowest PEA concentration, a staircase paradigm was used where 2 correct or 1 incorrect answers led to a decrease or increase of concentration, the so-called turning point. The resulting threshold score was the mean of the last 4 turning points in the staircase. The next subtest performed was the OD test, where 2 pens had the same odor while the other one had a different scent, which had to be identified. The last task was the OI test, where the subject was asked to choose the object that describes the odor the best using a 4-alternative-forced choice from flash cards that had both the picture and name of the object. The scores of the olfactory subtests were then summed up building the overall TDI (threshold, discrimination, and identification) score.
Assessment of cognitive function and depression
A comprehensive neuropsychological test battery was carried out in all subjects by researchers. The global cognitive function was assessed by Mini-Mental State Examination (MMSE), and the higher scores represent better global cognitive function [33]; the premorbid intelligence level was assessed by a vocabulary test (WST), and the higher scores represent higher premorbid intelligence [34]; the short-term memory skills was assessed by Wechsler memory test-Revised (WMSR) [35], which included the following aspects: word list recall and delayed recall, digit span forward and backward, and the higher scores represent better memory; the word fluency was assessed by the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) Animal Naming Test [36], a higher score represents superior verbal fluency; the naming ability was assessed by Boston Naming Test (BNT), and the higher scores represent better language function [37]; the planning ability was assessed by Nuremberg age inventory (NAI) Labyrinth-Test, and the higher scores represent better planning ability [38]; the executive functions was assessed by the Trail-Making-Test B (TMT-B), and the shorter time represent better executive functions [39]; the subjective impairment was assessed by the Questionnaire for cognitive complaints (FLei) [40], including subjective measurement of attention, memory and executive function, and the higher scores represent more cognitive complaints.
The symptoms of depression were assessed by the German version of the Beck Depression Inventory (BDI), a self-reported scale.
Assessment of brain activation when perceiving odor
A passive odor perception task [41] which has been successfully used in healthy individuals was used to assess brain activation of MCI patients. The peach odor (FREY&LAU, Germany, Product code P0606040) was delivered using a computer-controlled olfactometer and presented with an “ON-OFF” block design. The task lasted 228 s, which includes one run with seven blocks, and each block lasted 36 s, which consisted of a 12 s “ON” period for peach odor delivery, followed by a 24 s “OFF” period for odorless air delivery. The last block only included the “ON” period (Fig. 1).
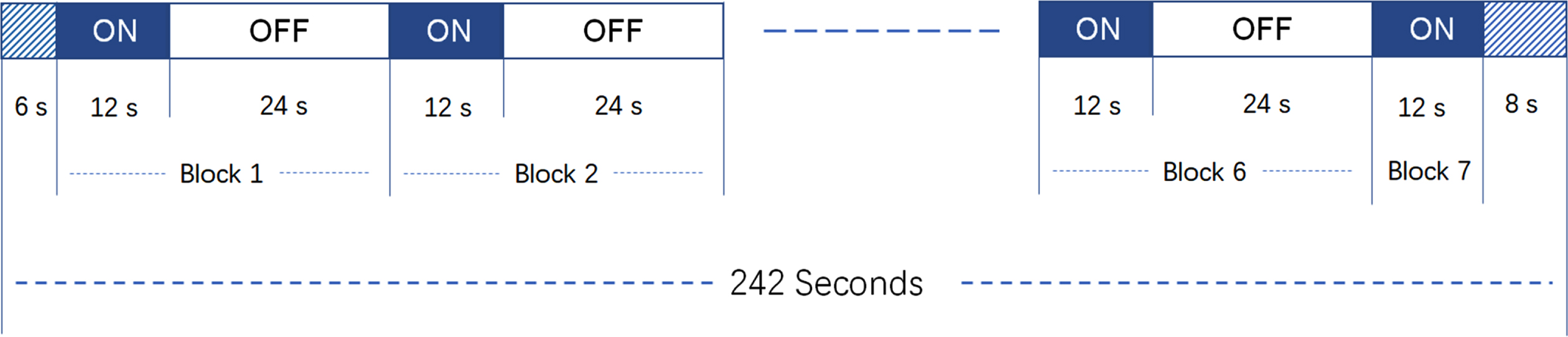
Design of the passive odor perception task. The task lasted for 228 s, which included one run with seven blocks, and each block lasted 36 s, which consisted of a 12 s “ON” period for peach odor delivery, followed by a 24 s “OFF” period for odorless air delivery. Particularly, the last block only included the “ON” period. The whole scanning lasted for 242 s, and the first 6 s and the last 8 s were not included in the analyses.
MRI data acquisition and image processing
A 3-Tesla MRI scanner (Siemens Sonata, Erlangen, Germany) with an 8-channel head coil was used for image acquisition. A total of 121 functional images were collected per individual using a T2 single-shot echo-planar imaging (EPI) sequence: TR = 2000 ms, TE = 30 ms, 90° flip angle, voxel size 2.97*2.97*3.00 mm, no interstice gap 10 %, 220×220 mm Field of view. T1 image was acquired using a 3D magnetization prepared gradient rapid acquisition gradient echo (MPRAGE) sequence (TR = 2300 ms, TE = 3.43 ms, 256×256 mm Field of view, voxel size 1×1×1 mm).
MRI scans were pre-processed and analyzed using SPM12 (Statistical Parametric Mapping, Functional Imaging Laboratory, Wellcome Trust Centre for Neuroimaging, Institute of Neurology, UCL, London, UK) [42] implemented in MATLAB (Version 2016b for Windows; The Mathworks Inc., Natick, MA). The first 6 seconds and the last 8 seconds of the functional data were discarded. The pre-processing steps were oriented by the default settings in SPM 12 and included realignment and unwarping, co-registration of functional with anatomical images, normalization to the Montreal Neurological Institute (MNI) space (by using the segmentation analysis of T1 images) and smoothing of functional images with a Gaussian kernel of 8×8×8 mm3 FWHM (full width at half maximum). The T1 images were preprocessed using the toolboxes CAT 12. Briefly, each T1 image was segmented into the cerebrospinal fluid, white matter, and grey matter, and then normalized to the MNI template. A Gaussian kernel filter of 8×8×8 mm3 was used to smooth the modulated image.
MRI data analyses
For the functional data, the statistical evaluation used restricted maximum likelihood algorithms on two levels. At the first level, the contrast odor “ON versus OFF” was modeled for each subject, and the movement related realignment parameters were included as repressors of no interest. The first-level contrasts were entered into second level random-effects analyses to address the following statistical model: 1) one-sample t-test for brain processing of odor in control group and training group in baseline and follow-up, respectively; 2) repeated-measures analysis of covariance (ANCOVA) was used to analyze the group effect (control groups versus training group), time effect (baseline versus follow-up) and the interactive effect of group*time for brain activation, controlling variable included age, sex, and years of education. The same design of repeated-measures ANCOVA was applied to the analysis of grey matter volume (GMV).
For functional and structural data, regions of interest (ROI) analyses were carried out following by whole brain analyses. First, analyses were focused on five ROIs based on the olfactory-related regions, including the piriform cortex, entorhinal cortex, hippocampus, thalamus, and orbital-frontal cortex. These ROIs were defined with the WFU PickAtlas software. Second, the Anatomical Automatic Labeling 116 template was defined as the mask to explore functional and structural change of the whole brain. Multiple comparisons correction was performed using a Gaussian random field (GRF) at voxel p < 0.005 and cluster p < 0.05 for functional analyses, and a voxel false discovery rate (FDR) at p < 0.05 for structural analyses. The blood oxygenation level dependent (BOLD) of the significant area was extract by using WFU PickAtlas software.
Statistical analyses
Statistical Package for Social Sciences version 23.0 (IBM SPSS 23.0, Chicago, IL, USA) was used to perform the statistical analyses. Demographic variables between training group and control group were evaluated with χ2 analysis (sex) and two-sample t test (age and years of education). The effect of olfactory training on change of olfactory scores and cognitive scores was analyzed by performing repeated-measures ANCOVA, with “group” (control groups versus training group) and “time” (baseline versus follow-up) as factors, and control variables included age, sex, and years of education. Least Significant Difference (LSD) post hoc analysis was used for multiple comparisons. Partial correlation analysis was used to explore the relationship between change of olfactory scores, cognitive scores and neuroimaging indicators, and control variables included age, sex, and years of education.
RESULTS
Demographic variables
There was a drop-out in two subjects in the training group and in 3 subjects in the control group in the follow-up period, respectively. The information of age, sex, and year of education in control group and training group who completed the training was listed in Table 1, and there was no significant difference in the demographic data between the two groups (all ps > 0.05).
Demographic information in patients with MCI
The effect of olfactory training on olfactory and cognitive scores
The control and training groups’ olfactory and cognitive tests scores (baseline follow-up) are listed in Table 2. The repeated-measures ANCOVA demonstrated that there was a group effect on the MMSE scores (training group > control group) (p < 0.05). Additionally, there were interaction effect of time*group on the scores of WMSR memory numbers backward (p < 0.05) (Table 2). Specifically, the control group but not the training group exhibited increased scores of WMSR memory numbers backward (p > 0.05). No significant effect of time nor time*group was found on other olfactory and cognitive score (p > 0.05).
The effect of olfactory training on olfactory and cognitive function in patients with MCI
TDI, olfactory sum score (threshold, discrimination, identification); MMSE, Mini-Mental State Examination; WMSR, Wechsler memory test range of numbers; BNT, Boston Naming Test; NAI, Nuremberg age inventory; TMT, Trail-Making-Tes; FLei, Mental performance questionnaire. *p < 0.05.
The effect of olfactory training on brain function and structure
The ROI analyses revealed no significant activated cluster in the one-sample t test and the repeated measures ANCOVA in the passive odor perception task (GRF correction at voxel p < 0.005 and cluster p < 0.05). In the whole brain analyses, a significant cluster (covering left middle frontal gyrus, left orbital-frontal cortex, left insula) was found in the whole sample in the one-sample t test (Table 3 and Fig. 2A). Additionally, the repeated measures ANCOVA demonstrated time*group exhibited an interactive effect on a cluster (covering left middle frontal gyrus and left orbital-frontal cortex) (GRF correction at voxel p < 0.005 and cluster p < 0.05) (Table 3 and Fig. 2B). In both ROI analyses and whole brain analyses, no significant effect of time, group nor time*group was found on the change of GMV in the repeated measures (FDR correction at p < 0.05).
Whole brain analyses of passive odor perception task in MCI patients with and without olfactory training
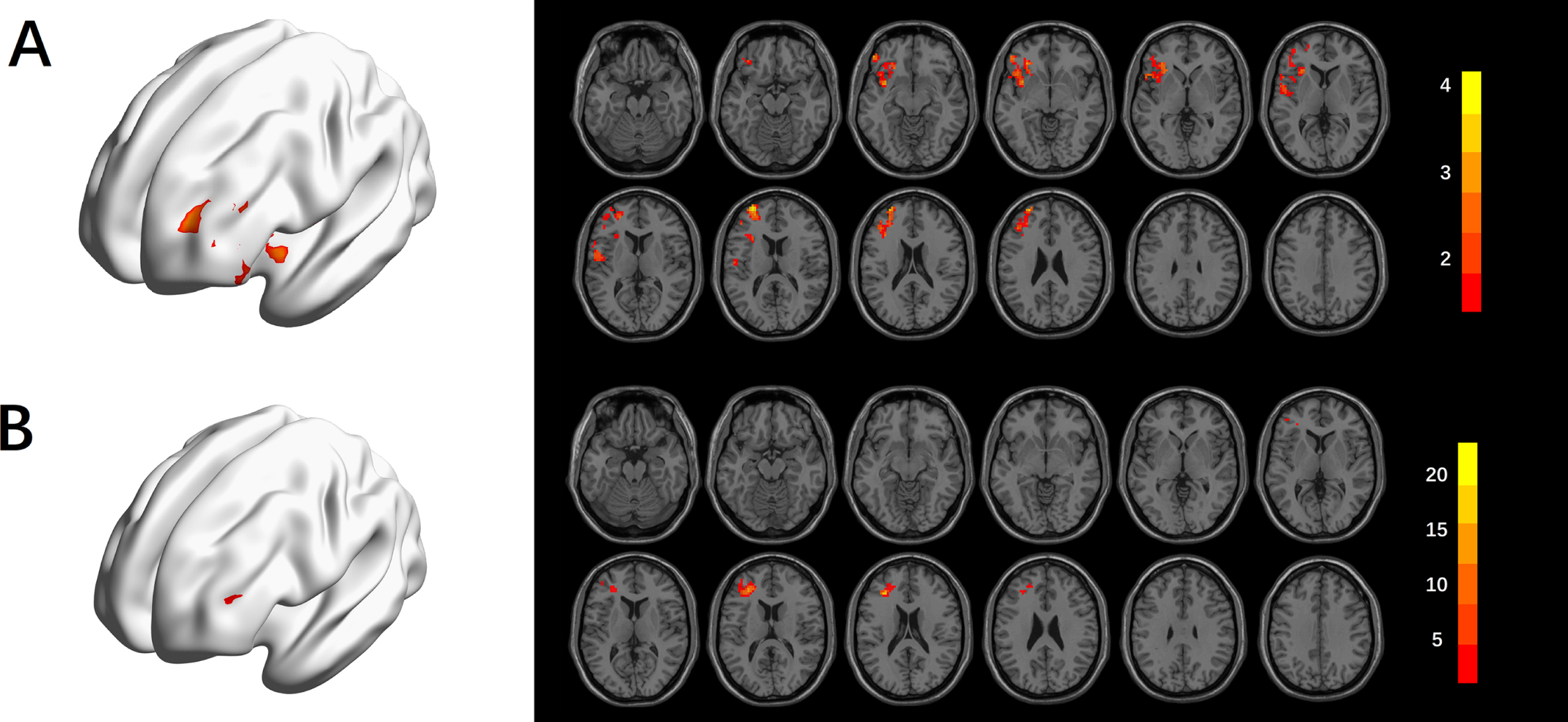
Activated regions of passive odor task in MCI patients. A) One-sample t test of the whole sample of MCI patients in follow-up. B) Interactive effect of group*time in repeated measures ANCOVA.
Correlation analyses
Across all subjects, the change of TDI scores (follow-up scores minus baseline scores) was positively correlated with change of BOLD response frontal area (extracting from the significant regions of the effect of group*time, follow-up values minus baseline values) (r = 0.470, p = 0.015) (Fig. 3). No significant correlation between change of BOLD response frontal area and change of cognitive score was found (p > 0.05).
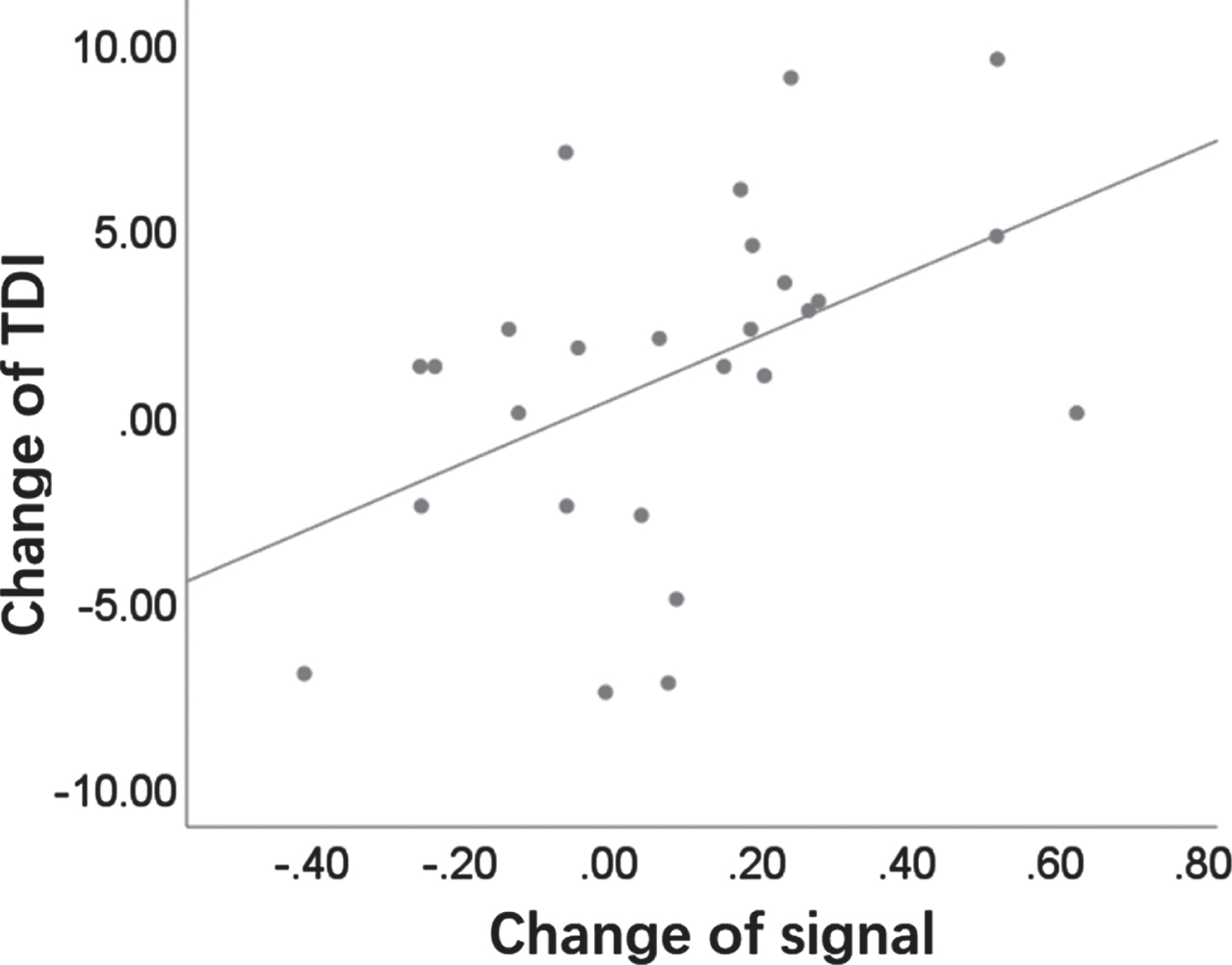
Correlation analyses in the relationships between olfaction and brain response to odor in patients with MCI.
DISCUSSION
Our study examined the effects of olfactory training on patients with MCI, and the following main results were found: first, olfactory training exhibited no significant effect on the change of the scores of olfaction, depression and most cognitive tests (except from the WMSR memory numbers backward); second, olfactory training exhibited a positive effect on the BOLD response to odor in frontal area (left middle frontal gyrus and orbital-frontal cortex), but exhibited no effect on GMV; third, the changes of TDI scores was positively correlated with BOLD response of frontal area (extracted from the fMRI analyses).
The present study suggested that the four months’ olfactory training exhibited no significant effect on olfactory performance in patients with MCI compared to control training. Although olfactory function was improved in both groups, the repeated measures ANCOVA exhibited no effect of olfactory training on the change of olfactory scores. Similarly, most of the cognitive scores (except from the WMSR numbers backward) as well as the depressive score were not influenced by the olfactory training. These results were somehow contradictory to our hypothesis, especially regarding the fact that olfactory training has a positive effect on olfactory function in other neurodegenerative diseases [43].
There are several possible reasons for this inconsistency. First, both groups had to perform a training task. Even the control group had to sniff odorless bottles regularly which can be considered a daily exercise. In view of the fact that both groups improved their olfactory ability slightly after 4 months, a (motor) training effect can be assumed in both groups which is also reflected by the fMRI results. According to recent findings [44], physical exercise is associated with better olfaction in elderly individuals. Second, although the olfactory training was supervised by relatives, some of the patients may have forgotten the daily training which restricted the effect, because amnestic deficits are a major symptom in MCI patients [31]. Since only half of the MCI patients returned the smell diary, we do not have enough evidence of whether the olfactory training was performed over the entire period. Third, the relatively small sample size may have limited the results and might not be sufficient for demonstrating the effect of olfactory training. Forth, the improvement of olfaction and cognition may occur beyond the 4 months’ training (delayed effect), or even before and then fade away (temporary effect). With the present follow-up assessment, however, this possible dynamic changing could not be captured. Last, MCI represents various etiologies, and a heterogeneous spectrum of patients which might further weaken the therapeutic effect. The MCI patients in the present study belong to different subtypes (amnesic/non-amnesic, single/multiple domain), and olfactory training might only be effective in certain subtypes.
In the fMRI analysis, all MCI patients exhibited significant activation (left middle frontal gyrus, orbital-frontal cortex insula) in follow-up rather than in baseline, though no significant activation was found when analyzing the training group and control group separately. Additionally, there was a positive effect of group*time on the activation of the left middle frontal gyrus and orbital-frontal cortex. Therefore, we deduced that the four month’s olfactory training significantly improved the activation of frontal area when perceiving peach odor, but this improvement was not sufficient to be shown in the one-sample t test because activations in MCI patients are rather low. Future studies including healthy controls could clarify whether MCI patients exhibit lower activation when processing olfactory information and might reflect the effect of olfactory training more clearly. Moreover, because AD pathology starts from secondary olfactory regions, fMRI tasks which focus more on high-level functions of the olfactory system (olfactory function which involving cognitive processing, such as odor identification and odor discrimination [45, 46]) rather than the passive odor perception may provide a deeper understanding about the brain functional change in MCI patients.
In the present study, the BOLD responses to odor in the frontal area (left middle frontal gyrus and orbital-frontal cortex) were significantly affected by olfactory training, which is consistent with the results of a previous study showing that olfactory training altered functional connectivity of the orbital-frontal cortex [27]. The orbital-frontal cortex is an important part of secondary olfactory areas, and it regulates planning behavior associated with sensitivity to reward and punishment [47]. For the middle frontal gyrus, it participates in the control and initiation of voluntary movements along with the primary motor cortex and is involved in memory recognition, working memory, categorization, drawing, and planning of strategies [48]. The effect of olfactory training on the activation of orbital-frontal cortex and middle frontal gyrus might be explained by the repeated sniffing of odors during the four months’ olfactory training, and the need to judge odor intensity and pleasantness for many times, which requires a cooperation of olfactory processing, cognitive processing, and motor coordination, resulting in an activation of the orbital-frontal cortex and middle frontal gyrus. Additionally, previous studies suggested that olfactory training may initially stimulate olfactory receptors and then induce neurogenesis [30], which may also be involved in the change of BOLD responses to odors in the frontal area.
The present correlation analyses suggested that the change of BOLD responses in the frontal area was positively correlated with the change of TDI scores. Although the olfactory training exhibited no effect on TDI on group level, significant change of scores can be observed in a portion of individuals. These results suggested that olfactory training may be only useful in some MCI patients, and future studies with a large sample size could further explore which MCI patients exactly are more responsive to the olfactory training.
Previous studies demonstrated that olfactory training may increase the volume of brain structures, such olfactory bulb [49], inferior frontal gyrus, entorhinal cortex, and fusiform gyrus [25]. This might be due to the repeated odor-exposure induced synapse formation and spine sprouting which increases cell genesis of glial or neuronal cells, and finally results in an increase of gray matter density or thickness [30]. However, no significance was found for the effect of olfactory training on GMV in the present study. Olfactory training may confer limited effect on brain structure because many MCI patients are suffering from AD pathology and therefore, an abnormal neurogenesis [50]. Moreover, voxel-based analysis may not be sensitive enough to reflect minor effects of olfactory training. Al et al. [25] also found that olfactory training exhibited no effect on the voxel-based analysis, but significant change was observed in their analyses of cortical thickness in healthy young individuals. Future studies with a larger sample size and the use of cortical thickness analysis methods are needed to explore the effect of olfactory training on brain structure in MCI patients.
Conclusion
Training with odors exhibited limited effect on the olfactory and cognitive function in patients with MCI compared to odorless training, but it increased their response to odors in the frontal area. Future studies with a larger sample size, non-intervention and healthy control groups, more time points of follow-ups, and a stricter supervision could provide a better understanding about the effect of olfactory training on patients with MCI.