
Abstract
Background:
Cerebral microbleeds (CMBs) are small round/oval lesions seen in MRI-specific sequences. They are divided in deep and lobar according to their location. Lobar CMBs (L-CMBs) are commonly associated with amyloid angiopathy. Although CMBs have been considered clinically silent for a long time, a growing body of evidence has shown that they could play a crucial role in cognitive functioning.
Objective:
The aim of this systematic review was to estimate the role of L-CMBs in cognitive performance.
Methods:
We selected, from the Cochrane Library, Embase, PubMed, and ScienceDirect databases, clinical studies, published from January 2000 to January 2020 and focused on the association between L-CMBs and cognitive functions. The inclusion criteria were: 1) participants grouped according to presence or absence of CMBs, 2) extensive neuropsychological examination, 3) CMBs differentiation according to topographical distribution, and 4) MRI-based CMB definition (< 10 mm and low signal in T2*/SWI). The impact of L-CMBs was separately assessed for executive functions, visuospatial skills, language, and memory.
Results:
Among 963 potentially eligible studies, six fulfilled the inclusion criteria. Four studies reported a greater reduction in executive performances in participants with L-CMB and two studies showed a statistically significant association between visuospatial dysfunction and L-CMBs. No association was found between hippocampal memory or language abilities and L-CMBs.
Conclusion:
Lobar CMBs are associated with a reduction of processing speed and visuospatial performances, thus suggesting the contribution of vascular amyloid deposition to this cognitive profile. This occurrence enables us to suspect an underlying Alzheimer’s disease pathology even in absence of typical hippocampal memory impairment.
Keywords
INTRODUCTION
Cerebral microbleeds (CMBs) are small circular or elliptical, homogeneous lesions with a size of 2 to 10 mm, visible in two MRI sequences: gradient-recalled echo (GRE) or susceptibility-weighted imaging (SWI). The prevalence of CMBs is highly variable: 3%–27% in the general population, 6%–80% in patients with vascular risk factors or vascular disease, and 16%–45% in patients with cognitive impairment [1]. In histological samples, CMBs are composed of hemosiderin accumulation surrounding the small, mainly arterial, blood vessels. Such accumulation appears hypointense on the aforementioned brain MRI sequences. To evaluate their number and location, visual scoring systems are currently the most widely used methods [2]. Among them, the Microbleed Anatomical Rating Scale (MARS) is usually preferred. In this scale, CMBs are scored according to their location, such as infra-tentorial, deep, or lobar (L-CMB), and side (right or left), for each of them.
CMBs are associated with aging [3], Alzheimer’s disease (AD), and cerebrovascular disease. CMBs localization differs according to the pathological substrate. Hypertensive arteriopathy is associated with CMBs in deep brain regions (basal ganglia, thalamus, and brainstem), whereas cerebral amyloid angiopathy (CAA) is usually characterized by the presence of L-CMBs [4]. These latter, in case of biomarker supported underlying amyloidoapthy, are nowadays defined as Amyloid-Related Imaging Abnormalities-Hemorrhage (ARIA-H). Although CMBs have been considered clinically silent for a long time, a growing body of evidence has shown that they could play a crucial role in cognitive impairment [5]. In fact, many studies suggest that CMBs likely affect specific cognitive functions and that the coexistence of mild cognitive impairment (MCI) and CMBs is a potential predictor of progression to AD [6–12].
MCI is a cognitive decline greater than expected for an individual’s age and education level but that does not interfere with activities of daily life. Two main clinical forms have been recognized: amnestic MCI (aMCI) and non-amnestic MCI (naMCI). If memory is the only impaired domain, diagnosis of amnestic MCI-single domain (aMCI-SD) can be made; alternatively, if other domains (e.g., language, executive functions, or visuospatial skills) are impaired, it could be defined as amnestic MCI-multiple domain (aMCI-MD). In a similar fashion, if the patient has a mild cognitive impairment without memory impairment (naMCI), we can distinguish between single or multiple domain based on the number of impaired cognitive domains [13]. The aim of the present review is to collect the available evidence about the existence of a peculiar neuropsychological pattern related to the presence of L-CMBs. We provide a review of the studies conducted in populations with a mean MMSE score above 24, including healthy elderly subjects or individuals affected by MCI [14], evaluating the association between cognitive performance and L-CMBs.
METHODS
We performed the systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (Supplementary Material). We searched for all clinical studies focused on the association between L-CMBs and cognitive functions. Studies were identified through the databases of Cochrane Library, Embase, and PubMed. The following terms were combined to yield our search outcome: (Alzheimer* OR Cognition* OR Cognitive OR Subjective OR Neuropsychological OR Dementia) AND (Microbleed* OR Small Vessel Disease* OR Small Vascular Disease* OR Amyloid Angiopathy). This search was restricted to articles published in English from January 2000 to January 2020. Moreover, by examining the reference list of relevant articles, additional papers were selected through cross-referencing.
Inclusion and exclusion criteria
Clinical research studies investigating CMBs and cognitive functions were considered eligible if they fulfilled the following inclusion criteria: 1) case-control, prospective or retrospective cohort, cross-sectional or experimental design, with respect to CMBs, i.e., participants had to be divided into two groups, with CMBs (CMBs+) and without CMBs (CMBs-); 2) detailed evaluation of cognitive functions including at least two domains among language, memory, visuospatial and executive/working memory/processing speed; 3) differentiation of CMBs according to their topographical distribution, at least deep and lobar; 4) definition of CMBs as homogeneous, round, or ovoid focal areas observed in the brain, with diameter < 10 mm and very low signal on MRI specific sequences (T2*GRE and/or SWI). Exclusion criteria were: 1) case reports, reviews, systematic reviews, meta-analyses, letters, and editorials; 2) participants with brain injury, infections, multiple sclerosis, epilepsy, or having taken drugs that affected cognitive function within 24 hours; 3) dementia or mean MMSE score of participants below 24; 4) studies with incomplete data. Age and gender of participants did not condition the study selection. These selection criteria were formulated to minimize statistical and sample heterogeneity.
Study selection
Two reviewing authors (L.C. and C.C.) examined all abstracts independently. Where it was arduous to make an adequate selection on the basis of the title and abstract alone, they retrieved the full article for screening. Full-text copies of articles deemed eligible by, at least, one of the reviewing authors were acquired for closer examination. At full-text level, the reviewing authors independently assessed each study for eligibility, according to the inclusion criteria.
Data extraction
Any measure of domain-specific cognitive performance was eligible for inclusion. Data on the presence, number, and location (lobar or not) of CMBs, as well as on mean, standard deviation, or linear regression coefficient of cognitive performances in the L-CMBs + and L-CMBs- groups, were extracted by the reviewing authors, independently. When the authors of the included studies made use of allocations in specific groups and categories (e.g., according to the L-CMBs load) and/or applied adjustments for multiple variables to reach statistical significance, we extracted the most “adjusted” data. Disagreements were resolved through consultations with a third reviewer (V.C.).
Study quality
Study quality was assessed using the Newcastle-Ottawa Scale (NOS). A score of up to 9 (NOS for case-control and cohort design) or 10 (NOS adapted for cross-sectional studies) points was assigned to each study based on the quality of group selection, comparability of groups and assessment of L-CMBs and cognitive functions [15, 16]. Both the NOSs are reported in the Supplementary Material.
Data synthesis
On account of the great heterogeneity of employed tests in assessing cognitive performances, we grouped results of cognitive performances in four main categories according to which cognitive domain was screened. When the included studies reported raw cognitive scores of the L-CMBs group, we converted these results in z-score setting the L-CMBs negative group as reference.
RESULTS
Study selection
The flowchart of the study selection process is illustrated in Fig. 1. We identified 13,977 potential studies from our initial electronic databases and reference lists, of which 5,689 were excluded after de-duplication. 574 articles were removed due to the unavailability of the abstract or because of non-working/non-existent links to the abstract. 7633 were removed based on their title and abstract. The full text of the remaining 81 studies was examined. Of these, 75 articles were removed due to the presence of one or more of the following factors: 1) neither the presence nor the location of CMBs was specified; 2) cognitive functions were not separately evaluated with an extensive neuropsychological assessment; 3) the exact sample size of L-CMB+ and L-CMB- groups were not properly specified; 4) participants suffered from Dementia or had a MMSE score under 24; 5) they did not compare cognitive functions with lobar CMBs. Also, at full-text analysis 3 articles were excluded due to overlapping data. None of the papers, selected through cross-referencing, were included. A total of six studies fulfilled the inclusion criteria. Concerning the study quality assessment, two studies were evaluated with the NOS for cohort studies [17, 20], receiving a score of 8 and 7, respectively; four articles were appraised with the NOS adapted for cross-sectional studies [9, 21], obtaining a quality score ranging from 8 to 9. The included works were qualified as observational, with a prospective [17, 20] or cross-sectional [9, 21] design. All the studies were conducted in elderly non-demented individuals except for the one by Valenti et al. [18]. This latter included a population of aged MCI. Three authors [17, 20] conducted a longitudinal study with follow-up cognitive testing over a mean period ranging from 4 to 6 years. Among them, Paradise et al. reported the association between L-CMBs and specific cognitive domains only at baseline, while showed the overtime impact of whole brain CMBs on cognitive performances without grouping according to CMBs location. Two studies [17, 20] created a subcategory of L-CMBs + subjects by defining a threshold of L-CMBs load, to reach statistical significance (Table 1).
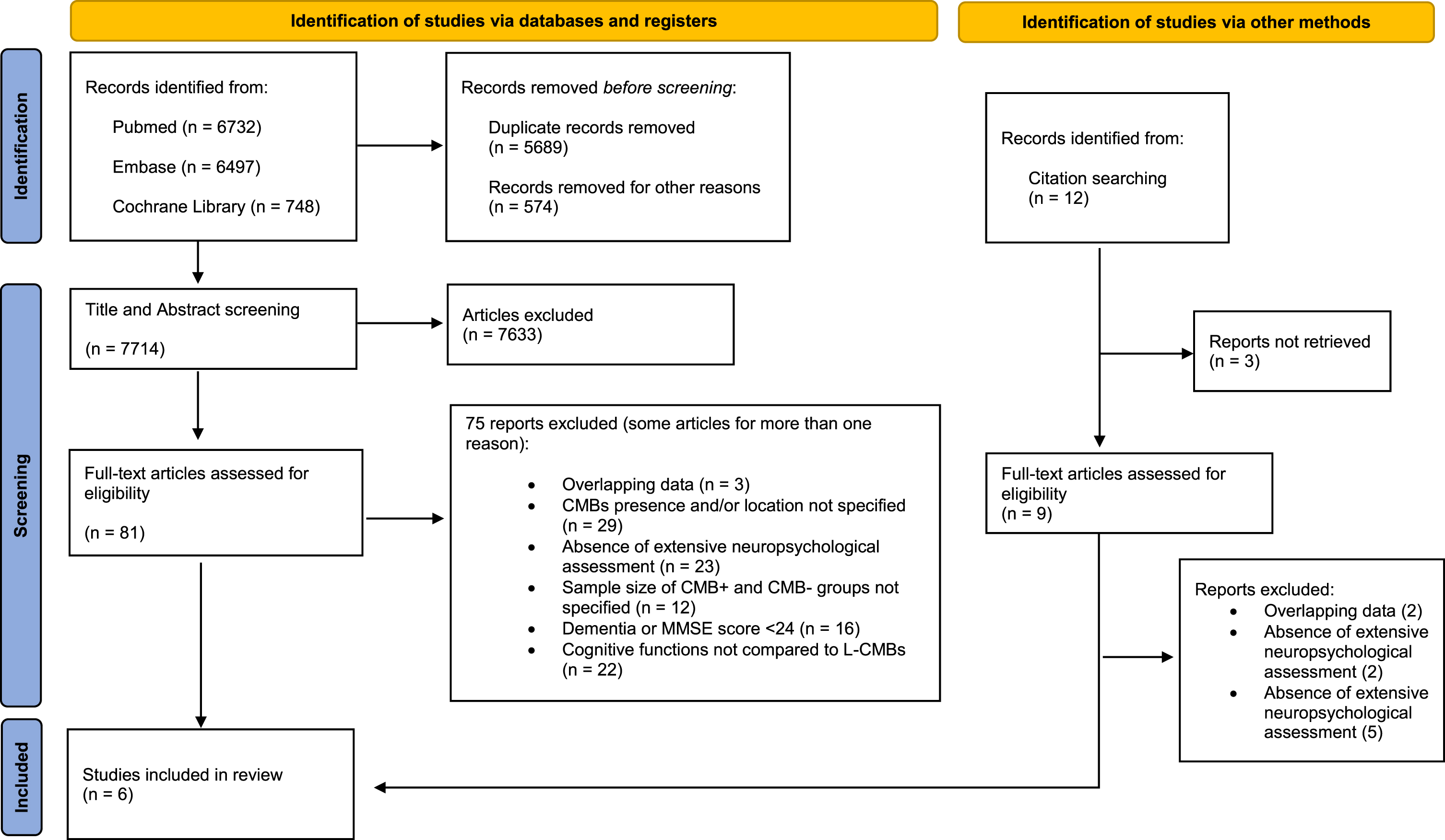
Flow diagram of search strategy and study selection.
Studies characteristics and employed tests in cognitive assessment
BNT, Boston Naming Test; BVRT, Benton Visual Retention Test; CDT, Clock drawing test; CVLT, California Verbal Learning Test; CVVLT, Chinese Version of the Verbal Learning Test; CMB, cerebral microbleeds; COWAT, Controlled Oral Word Association Test; DSB, Digit Span Backward; DSST, Digit symbol substitution test; LDST, Letter Digit Substitution Test; PVF, Phonemic Verbal Fluency; ROCF, Rey–Osterrieth complex figure; SDMT, Symbol Digit Modalities Test; SVF, Semantic Verbal Fluency; VSAT, Verbal Series Attention Test; WFT, Word Fluency Test. Test results represent the mean difference in the z score in patients CMB+ compared with those CMB-. *Number of patients with > 4 L-CMB+. ** Number of patients with≥3 L-CMB+. § see the text.
Qualitative analysis of cognitive functions
In all selected studies L-CMBs were identified by T2*GRE and/or SWI MRI sequences. Cognitive functions were evaluated using an extensive neuropsychological examination to study each cognitive domain. Most of these studies used multiple linear regression to investigate the association of microbleeds with specific cognitive domains [9, 19–21]. Valenti et al. performed a Spearman’s rho test to assess the association between count and location of L-CMBs and neuropsychological performances. Two studies reached statistical significance applying a L-CMBs load cut-off [17, 20]. The results in the L-CMB + groups are listed (Tables 2–5) as deviations from the mean value of the reference population (L-CMD- groups).
Frontal lobe functions
CMB, cerebral microbleeds; COWAT, Controlled Oral Word Association Test; DSB, Digit Span Backward; DSST, Digit symbol substitution test; LDST, Letter Digit Substitution Test. Test results represent the mean difference in the z score in patients CMB + compared with those CMB-. *Statistically significant. §encompass TMT-B and COWAT.
Visuospatial functions
CDT, clock drawing test; CMB, cerebral microbleeds, ROCF, Rey–Osterrieth complex figure; TCF, Taylor Complex Figure. Test results represent the mean difference in the z score in patients CMB + compared with those CMB-. *Statistically significant.
Language
BNT, Boston Naming Test; CMB, cerebral microbleeds; PVF, Phonemic Verbal Fluency; SVF, Semantic Verbal Fluency; WFT, Word Fluency Test. Test results represent the mean difference in the z score in patients CMB + compared with those CMB-. *Statistically significant.
Memory
CMB, cerebral microbleeds; CVLT, California Verbal Learning Test; CVVLT, Chinese Version of the Verbal Learning Test; RAVLT, Rey Auditory Verbal Learning Test. Test results represent the mean difference in the z score in patients CMB + compared with those CMB-. *Statistically significant.
Comparison of frontal lobe functions
A total of 7,479 participants (818 L-CMB + and 6,661 L-CMB-) from the 6 studies were eligible for analyses. Executive functions, attention, and processing speed were evaluated using one or more of the following tests: Stroop test [9, 20], digit span backward [21], Trail Making Test (TMT) [18, 19], Letter-Digit Substitution test [17], Digit Symbol substitution test [9, 18–20], Figure comparison test [20], Paper-Pencil Memory Scanning task [9], Verbal series attention test [9]. Paradise et al. included the Controlled Oral Word association test (COWAT) in the executive functions assessment [19]; the results of this assessment were expressed as mean of the scores obtained in the following tests: COWAT and TMT B. Only one of the six studies (Table 2) reported lower performances in executive function tests (evaluating attention, working memory, mental flexibility and/or sensibility to interference) in L-CMB + individuals compared to L-CMB- subjects [9]. On the contrary, five out of the six included studies (Table 2) reported a reduction in processing speed performances in the L-CMB + group compared to the L-CMB- one.
Comparison of visuospatial functions
We found 113 L-CMB + and 1,304 L-CMB- eligible subjects from three studies. These studies investigated visuospatial functions with the copy of the Taylor or Rey–Osterrieth complex figure (TCF-copy; ROCF-copy) [9, 21], the Clock drawing test [21] or the Block Design test [19]. Chung et al. (Table 3) showed a statistically significant association between lower visuospatial performances and the presence of L-CMBs [9, 21]. A worsening trend was disclosed by the other two works, but they did not reach statistical significance.
Comparison of language domain
A total of 5,044 subjects (512 L-CMB + and 4,532 L-CMB-) were eligible. Five of the six studies performed the Word fluency test [9, 21], comprehensive of both phonemic and semantic fluency. Paradise et al. performed the Boston naming test and the semantic fluency test [19] to assess the language but included the phonemic fluency test into the executive functions assessment (see above). Two studies (Table 4) revealed a statistically significant positive correlation between fluency performances and L-CMBs presence [17, 18].
Comparison of memory function
A total of 7,479 subjects (818 L-CMB + and 6,661 L-CMB-) were eligible. Memory functions were tested with 15-Word Rey Auditory Verbal Learning Test (RAVLT, often split in immediate and delayed recall) [9, 17–19], Chinese version of the Verbal Learning test [21], California Verbal Learning test [20], Benton Visual Retention test [19], and the Short Story test [18]. Two studies evaluated memory involvement also with the ROCF recall test [9, 18]. Three studies [9, 20] calculated memory performances as a compound of the mean of two scores deriving from immediate and delayed recall. Only two studies [9, 17] (Table 4) found a significant association between memory performances and L-CMBs presence. The first [9] did not split immediate and delayed recall while the second one [17] found a relationship only between L-CMBs load and RAVLT immediate recall.
DISCUSSION
Cerebral microbleeds are small, circular, hypointense lesions observed in specific T2-weighted MRI sequences, well-demarcated from the surrounding tissue. They reflect a chronic accumulation of hemoglobin degradation byproducts in the brain parenchyma. Depending on location, CMBs are usually related to two different vascular pathologies: hypertensive vasculopathy and CAA. When CMBs are located in lobar regions they are commonly associated with CAA. Previous cross-sectional studies in healthy adults demonstrated that CMBs are associated with a lower MMSE score [7, 23]. Specifically addressing the question about the role of CMBs in MCI, recent studies reported a higher prevalence of CMBs, especially in lobar regions, among individuals with MCI compared to healthy controls [18, 25].
In this review, we report the current knowledge about the association between performances in specific cognitive domains and L-CMBs in healthy elderly subjects and MCI patients, showing a reduction in processing speed and visuospatial performances.
Previous studies have demonstrated that L-CMBs are mainly associated with CAA. In fact, the deposition of the amyloid-β (Aβ) protein is prevalent in cortical and leptomeningeal vessels in CAA [26] and neuroimaging evidence suggests that L-CMBs occur in areas of amyloid deposition [27]. Although Aβ is unanimously considered the main component of both neuritic plaques and CAA-related vessel deposits, several studies have shown that the length of Aβ peptides differs between these two neuropathological entities. Fragments with 42 amino acids (Aβ42) are mainly found in neuritic plaques, whereas shorter fragments, i.e., Aβ40, are the most frequent peptides reported in the walls of leptomeningeal and cortical vessels [28–30]. Even if this distinction is generally true, some clarifications should be made. Aβ42 is anyway an essential component of the wall vessel deposits, but the Aβ40:Aβ42 ratio inside them is higher than in neuritic plaques [31]. Moreover, this is not the same in all vessels: although it is persevered in arterial and, to a lesser extent, venous deposits, the Aβ40:Aβ42 ratio in capillary walls is rather like that in neuritic plaques [31, 32]. The most intriguing mechanism that explains such preferential deposition of Aβ40 in arterial and venous walls and Aβ42 in neuritic plaques and capillaries is based on differences in fragment solubility. Aβ42 is less soluble and more prone to aggregation and accumulation than shorter Aβ peptides [33], whereas Aβ40, due to its greater solubility can diffuse along perivascular drainage pathways until it accumulates in the vessels.
The difference in location of Aβ deposits seems to influence the pathophysiological process that induces toxicity and neuronal death in CAA and AD. Although both the pathologic mechanisms are intimately linked to Aβ accumulation, different sites of Aβ deposition (in its turn influenced by the Aβ peptide length) activate different downstream events, leading to neuronal injury. Aβ42 triggers the tau hyperphosphorylation and, therefore, neurofibrillary tangles formation (strictly related to neuronal death and AD clinical severity) whereas some recent evidence has suggested that CAA-related brain damage could result from a reduced blood flow. In this context of amyloid-induced impaired cerebral blood supply, CAA-related perivascular hyperphosphorylated tau is supposed to enhance the vascular damage. In line with this assumption, some studies have reported an increase of blood-brain barrier permeability associated to tau oligomers vascular accumulation in human patients with progressive supranuclear palsy [34, 35] as well as a strong impact on the integrity of the brain’s microvasculature following tau perivascular accumulation [36, 37]. All this might explain the widespread reduction in resting-state cerebral blood flow and hypomethabolism in the same brain areas where CMBs are located [38, 39]. Hypothetically, this condition could determine chronic hypoperfusion, which, in turn, results in reduced cortical thickness that affects cognitive performances. In this regard, the pattern of cortical thinning in CAA does not completely overlap with that of AD, as greater thinning in the occipital and medial frontal cortex can be observed in CAA compared to AD [40, 41]. We could hypothesize that this pattern of CAA-associated hypoperfusion and atrophy affects processing speed and visuospatial functions performances in subjects with L-CMBs. Moreover, this blood supply dysfunction is supposed to be the cause of the recently reported reduction in structural connectivity, in CAA patients [42].
The last note should be made on the CAA and AD relationship. Almost all the previous neuropathological studies focused on CAA prevalence in AD, reporting a mean prevalence of CAA in AD brains of 85–95% [43, 44] and a strong relationship between CAA severity and AD neuropathological staging. A large autopsy study showed that the pathological grade of CAA grew along with the degree of AD pathology: CAA moderate-severe had a prevalence of 5.3% in absence of neuritic plaques, 16.1% in brains with mild neuritic plaques, 31.7% in presence of moderate neuritic plaques, and 45.3% in brains with severe neuritic plaques. This latter was the only work that also investigated the AD prevalence in CAA subjects: of more than 2,500 CAA, less than 300 cases had no/low AD pathology (11%) whereas the remaining 89% showed a co-existence of significant AD neuropathologic changes [45]. Based on these results, it seems that the “AD-independent” CAA quota could amount to nearly 1 : 10 of CAA; if it is true a notable percentage of CAA-related CMBs could be related to underlying AD pathology. This would allow to considerably increase the sensitivity in AD detection.
About language and memory, it is necessary to make a few considerations. Two studies [17, 18] considered WFT as a standalone parameter without formally including it in the language domain, Van Norden et al. linked fluency to the executive domain while Chung et al. employed the WFT to assess language. To date, there is not a consensus in the literature regarding the exact categorization of verbal fluency in executive or language domain, but it is undeniable that both phonemic and semantic fluencies are strongly influenced by “frontal” functions [46]. Several studies described the impact of processing speed on verbal fluency performances [47–49]; so, it is plausible that the slower processing speed in L-CMBs patients is responsible for the lowering of the WFT score. In support of this theory, a significant association between naming tests and the presence of L-CMBs did not emerge. On the other hand, memory does not seem to be significantly affected in the L-CMBs+group, at least not in the earliest cognitive evaluations (in those studies that performed a follow-up testing). Almost all the studies investigated memory using the RAVLT, a test composed of two subsets, immediate recall and delayed recall. The latter is a measure of delayed retrieval of information, reflecting the CA1 hippocampal subfield and subiculum integrity [50], and whose deficit is an early indicator of AD [51]. While RAVLT delayed recall is expression of hippocampal functions, immediate recall reflects, at least partially, the functioning of frontal lobes, as the word-list learning creates an overload condition, sensitive to attentional capacities and to processing speed. Therefore, immediate recall is not considered to be only dependent on the hippocampal function, but also related to the fronto-parietal attentional circuit [52]. In addition, a slowing in processing speed was found to be an important contributor to lower performance in verbal memory tests, especially affecting immediate recall [53, 54]. Among the selected articles of this review, a reduction in memory performances was shown in immediate recall alone [17] or, when the authors reported memory performances as a summation of immediate and delayed recall scores. Therefore, even here, it is quite likely that these results depend on the impact that processing speed has on memory recall tests.
This review highlights the importance of always performing a GRE/SWI integration in MRI studies in elderly subjects with low performances in multiple domains but preserved episodic memory. The presence of L-CMBs could raise the suspicion of un underlying amyloid pathology in absence of typical memory impairment and, in turn, legitimize the searching for AD pathophysiological biomarkers, leading to earlier diagnoses of AD. The goal of an early diagnosis should be always pursued for both to improve quality of patient care and let the enrollment of prodromal or early symptomatic subjects in clinical trials aiming at testing novel therapeutic approaches.
However, in the absence of effective disease modifying treatments, the relationship between vascular impairment and AD pathology could suggest alternative approaches. Vascular dysregulation was found to initiate and sustain amyloid deposition [55] and also act synergistically with amyloid pathology in increasing tau burden [56]. Therefore, the strong impact of vascular dysfunction on underlying amyloid and tau pathologies could influence the therapeutic strategy to adopt in L-CMBs patients, justifying stronger cardiovascular prevention, with probable benefit on disease progression.
The present review has some limitations. First, there was no perfect correspondence, within the included studies, of the adopted methods in cognitive assessment: 1) not all the studies assessed visuospatial and/or language domains; 2) different studies evaluated cognitive functions making use of different tests, determining a minimal heterogeneity in scoring. This lack of uniformity was partially overcome by grouping the cognitive tests in one of the four correspondent cognitive domains. Second, several limitations concern the methodological approach used to demonstrate the association between L-CMBs load and cognitive involvement: 1) most of the studies did not offer information about the lobar position of the L-CMBs making difficult an anatomo-functional correspondence; 2) different studies have set different L-CMBs cut-off, arbitrarily employed to gain statistical significance; 3) only two of the studies provided a longitudinal evaluation of L-CMBs and cognitive domains association [16, 19]. A further shortcoming, that was common in all the included studies, was the absence of a biological definition of amyloidopathy (assessable by CSF Aβ dosage and/or amyloid PET). So, although L-CMBs are more frequent in diseases with an underlying amyloidopathy, the absence of biological confirmation did not allow the authors to state with certainty that a patient with L-CMBs was affected by an amyloid-related disease.
In conclusion, patients with L-CMBs show lower cognitive performances with a distinctive involvement of processing speed and visuospatial functions. Conversely, the episodic memory seems to be quite preserved. This emphasizes the importance of looking for L-CMBs in elderly subjects with subtle reduction in cognitive performances (and in naMCI individuals) that could hide an underlying Aβ pathology in the very early stage. It is important to emphasize that the presence of these cognitive deficits associated with specific CMBs (L-CMBs) must surely place AD or MCI due to AD among the main diagnostic hypotheses. In addition, early diagnosis increases the therapeutic efficacy of the new disease-modifying treatments.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-5323r2).