
Abstract
Background:
Patients with amnestic mild cognitive impairment (aMCI) are usually at an initial stage of Alzheimer’s disease (AD). However, some patients with aMCI do not present biomarkers of amyloid pathology characteristic of AD. The significance of amyloid-negative aMCI is not presently clear.
Objective:
To know the etiology and prognosis of amyloid-negative aMCI.
Methods:
Patients who fulfilled criteria for aMCI and were amyloid negative were selected from a large cohort of non-demented patients with cognitive complaints and were followed with clinical and neuropsychological assessments.
Results:
Few amyloid-negative aMCI had evidence of neurodegeneration at the baseline, as reflected in cerebrospinal fluid elevated tau protein levels. About half of the patients remained essentially stable for long periods of time. Others manifested a psychiatric disorder that was not apparent at baseline, namely major depression or bipolar disorder. Remarkably, about a quarter of patients developed neurodegenerative disorders other than AD, mostly frontotemporal dementia or Lewy body disease.
Conclusion:
Amyloid-negative aMCI is a heterogeneous condition. Many patients remain clinically stable, but others may later manifest psychiatric conditions or evolve to neurodegenerative disorders. Prudence is needed when communicating to the patient and family the results of biomarkers, and clinical follow-up should be advised.
INTRODUCTION
As a consequence of population aging, the number of people affected by neurodegenerative disorders, particularly Alzheimer’s disease (AD), is increasing dramatically worldwide, representing a major public health issue [1]. For many years, a transitional state in AD from normal cognitive aging to a full-blown dementia stage was anticipated [2]. The possibility of diagnosing consistently AD at an early phase emerged about two decades ago, when the Mayo Clinic group proposed the concept of amnestic mild cognitive impairment (aMCI), characterized by subjective memory complaints, objective memory deficit, normal general cognitive performance, and maintained activities of daily living [3]. Indeed, patients diagnosed with aMCI in a clinical setting have about 10% annual progression rate of conversion to dementia, usually AD [4]. The concept of aMCI as a surrogate for early AD, however, was not entirely satisfactory, since it was recognized that a proportion of patients with aMCI may remain cognitively and functionally stable for more than 10 years, which would be hardly compatible with a neurodegenerative condition [5].
In recent years, a major breakthrough was the possibility of diagnosing AD reliably in vivo in patients that present with aMCI. Different diagnostic criteria with slight differences were advanced, namely prodromal AD [6–8] and mild cognitive impairment (MCI) due to AD [9], that rely on biomarkers reflecting pathological alterations of the AD continuum, namely the presence of amyloid in the brain [10], detected by measuring low amyloid Aβ1-42 concentrations in the cerebrospinal fluid (CSF) [11], and/or identifying brain deposits of Aβ with amyloid positron emission tomography (PET) [12]. Interestingly, when applying the AD biomarkers in research and clinical settings [13], the existence of a subset of patients with aMCI who do not harbor amyloid pathology and thus do not have AD was confirmed [14].
The etiology and prognosis of aMCI patients without amyloid pathology are not presently clear. A previous study found that amyloid negative patients with aMCI do not show cognitive decline over a period of 3 years [15]. On the contrary, in a large multicentric study, as much as 24% of the amyloid negative aMCI cases progressed to dementia within 3 years [16]. In several studies, some patients with amyloid negative aMCI were proposed to be at an initial stage of a neurodegenerative disorder other than AD, like frontotemporal dementia, primary age-related tauopathy, or the Lewy body disease [17–20]. Other patients may have masked depressive symptoms [21] or functional cognitive disorder [22] that might mimic the aMCI syndrome.
For sure, the absence of amyloid pathology is by no means a guarantee that patient with aMCI will not get worse and will not develop dementia in the future. As a consequence, the information that presently can be provided by the clinician to the individual patient and family is rather imprecise and certainly unsatisfactory. More should be known about the relevant and intriguing question of the etiology of aMCI cases that do not show AD pathology, and for this purpose a long follow-up might needed, so that to underlying clinical conditions might appear manifestly, and rates of progression might be estimated.
In the present study, we selected from a large cohort of non-demented patients with cognitive complaints those who fulfilled criteria for aMCI and were amyloid negative at the baseline and followed them up with clinical and neuropsychological assessments.
METHODS
Participants
Participants were selected from the Cognitive Complaints Cohort (CCC), established in a prospective study conducted at Faculdade de Medicina da Universidade de Lisboa, approved by the local ethics committee, conducted according to the declaration of Helsinki and requiring the participants’ informed consent [23]. The CCC aimed to investigate the cognitive stability or evolution to dementia in patients with cognitive complaints, recruiting nondemented patients with cognitive complaints who underwent a comprehensive neuropsychological evaluation, as well as clinical history, neurological examination, laboratory evaluation, and brain imaging (CT or MRI). Patients with neurological, psychiatric, or medical disorders that might induce cognitive deficits, history of alcohol or recurrent substance abuse, or with dementia were excluded. For the purpose of the present study, participants recruited from 2008 to 2018 were selected. Although patients were followed on a routine clinical basis, when preparing this work they were systematically contacted for follow-up.
Diagnostic criteria
Inclusion criteria
Diagnosis of amnestic MCI, adapted from Petersen [3]. Memory complaints present at the clinical interview. Abnormal memory function. Performan-ces in at least two memory domain tests must fall 1.0 SD below norms for age and education, following the comprehensive criteria defined by Jak and coworkers [24]. Normal general cognitive function, determined by the Mini-Mental State Examination (MMSE) [25] within normal values for the Portuguese population [26]. No or a minimal impairment in activities of daily living, reflected in a score < 3 on the first part (items 1–8) of the Blessed Dementia Rating Scale (BDRS) [27]. Absence of brain amyloid pathology.
Exclusion criteria
The same exclusion criteria as used in the CCC (see above), that is, patients with neurological, psychiatric, or medical disorders that might induce cognitive deficits, history of alcohol or recurrent substance abuse, or with dementia were excluded.
Amyloid status
The absence of amyloid pathology was determined at baseline by measuring normal Aβ1-42 concentrations in the CSF and/or the absence of brain deposits of Aβ with amyloid PET scan. Whenever possible, patients had both CSF biomarkers and amyloid PET performed. A high agreement between Aβ1-42 concentrations in the CSF and amyloid PET scan findings was documented previously, supporting the strong correlation of these two measures [12].
Lumbar puncture and CSF handling followed established protocols [28]. The levels of Aβ1–42, total tau, and hyperphosphorylated tau were mea-sured using commercially available enzyme-linked immunosorbent assays (INNOTEST® Aβ42, INNOTEST hTAU Ag, and INNOTEST PHOSPHO-TAU (181P); Innogenetics, Ghent, Belgium). The positivity was determined using locally available cut-off values.
Amyloid positron emission tomography (PET) scans used the Pittsburgh Compound B ([11C]-PIB) and were performed in the same scanner (Philips PET/CT Gemini GXL), preceded by a low-dose brain computed tomography (CT) acquisition for attenuation correction (Institute of Nuclear Science Applied to Health, ICNAS, University of Coimbra). PiB-PET images were initially classified as amyloid positive or negative based on a support vector machines (SVM) local classifier, which uses the voxel wise brain grey matter standardized uptake value ratio (SUVR) and the cerebellar grey matter as reference region [29]. Final classification was confirmed by visual read from the same specialists, a nuclear medicine radiologist and a neurologist, experienced in the field.
Clinical diagnoses at follow-up
Clinical diagnoses at follow-up are based on international clinical criteria: 1) Presence of dementia according to the DSM-IV- TR [30]; 2) Alzheimer’s disease according to the Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease [31]; 3) Vascular dementia criteria of the National Institute of Neurological Disorders and Stroke (NINDS) and Association Internationale pour la Recherche et l’Enseignement en Neurosciences (AIREN) [32]; 4) Lewy body disease criteria by McKeith [33, 34]; 5) Dementia associated with Parkinson’s disease, criteria of the Movement Disorder Society [35]; 6) Frontotemporal dementia following Rascovsky [36]; 7) Primary progressive aphasia variants, criteria proposed by Gorno-Tempini [37]; 8) Major depressive disorder and bipolar disorder, according to the DSM-IV- TR [30].
Neuropsychological assessment
The baseline and follow-up comprehensive neuropsychological assessments were carried out by the same team of trained neuropsychologists, following a standard protocol and comprised the following instruments: MMSE [25]. The MMSE is a brief screening instrument to assess global cognitive performance. The Portuguese version was applied, and normative data was > 27 for more than 11 years of education and > 22 for 11 or less years of education [26]. Battery of Lisbon for the Assessment of Dementia (BLAD) [38, 39]. The BLAD is a comprehensive neuropsychological battery that includes some tests from the Wechsler Memory Scale [40] and has been validated for the Portuguese population. This battery includes tests for the following cognitive domains: attention and executive functions (Cancellation Task, Digit Span Backward and Clock Draw); initiative (Semantic Fluency, Motor and Graphomotor initiatives); reasoning (Raven Colored Progressive Matrices and Interpretation of Proverbs); orientation (Personal, Spatial, and Temporal Orientation); calculation (Basic Written Calculation); visuo-constructional abilities (Cube Copy); language (Token Test); memory and learning (Visual Reproduction Test, Digit Span Forward, Word Recall, Logical Memory immediate and delayed recall, Verbal Paired-Associate Learning). Trail Making Test (part A and part B) [41, 42]. This task measures sustained attention, visuomotor processing speed (part A), visuospatial working memory and cognitive flexibility (part B). Part A consists of 25 circles numbered 1–25 distributed over a sheet of paper and the patient should draw lines to connect the numbers in ascending order. In Part B there are 25 circles as well, but the circles include both numbers (1–13) and letters (A –M) and the patient has to draw lines to connect them all in an ascending pattern with the added task of alternating between the numbers and letters (i.e., 1-A-2-B-3-C, etc.). California Verbal Learning Test (CVLT) [43, 44]. The CVLT measures verbal learning and assesses constructs such as repetition learning, serial position effects, semantic organization, intrusion, and proactive interference. The word lists (List A and List B) are made up of 16 items from 4 different categories of “shopping list” items. The trial of interest (better discriminating ability for different stages of cognitive decline) [45] considered for the present study was the total number of words from List A correctly recalled on the first 5 learning trials (CVLT 5 Trials Total Recall). Geriatric Depression Rating Scale (GDS) –short version (15 items) [46–48]. The GDS is a self-report instrument used specifically to identify depressive symptomatology in the elderly. Subjective Memory Complaints Scale (SMC) [49, 50]. The SMC scale comprises 10 individual questions for the assessment of subjective memory complaints, with total scores ranging from 0 (absence of complaints) to 21 (maximal complaints score). Blessed Dementia Rating Scale (BDRS) [51, 52]. The BDRS is a brief behavioral scale based on the interview of a close informant. This scale is composed of 22 items that address daily life activities, habits, and changes in personality. Changes in everyday activities and habits were assessed by the first part of the scale [27].
Statistical analysis
The neuropsychological assessments were standardized according to the age and education norms for the Portuguese population [26, 38], and z scores were calculated.
RESULTS
From the 79 amyloid-negative aMCI patients selected from the CCC as much as 39 were excluded for various reasons shown in Fig. 1. Demographic and clinical data of the 40 amyloid-negative aMCI patients that entered the study are reported in Table 1. The amyloid status was based on normal Aβ1-42 concentrations in the CSF (13 patients), normal brain amyloid PET scan (9 patients), or both (18 patients). The values of CSF biomarkers were Aβ1-42 883±224 pg/mL, total tau 277±119 pg/mL, and hyperphosphorylated tau 45±19 pg/mL (31 patients that underwent lumbar puncture).
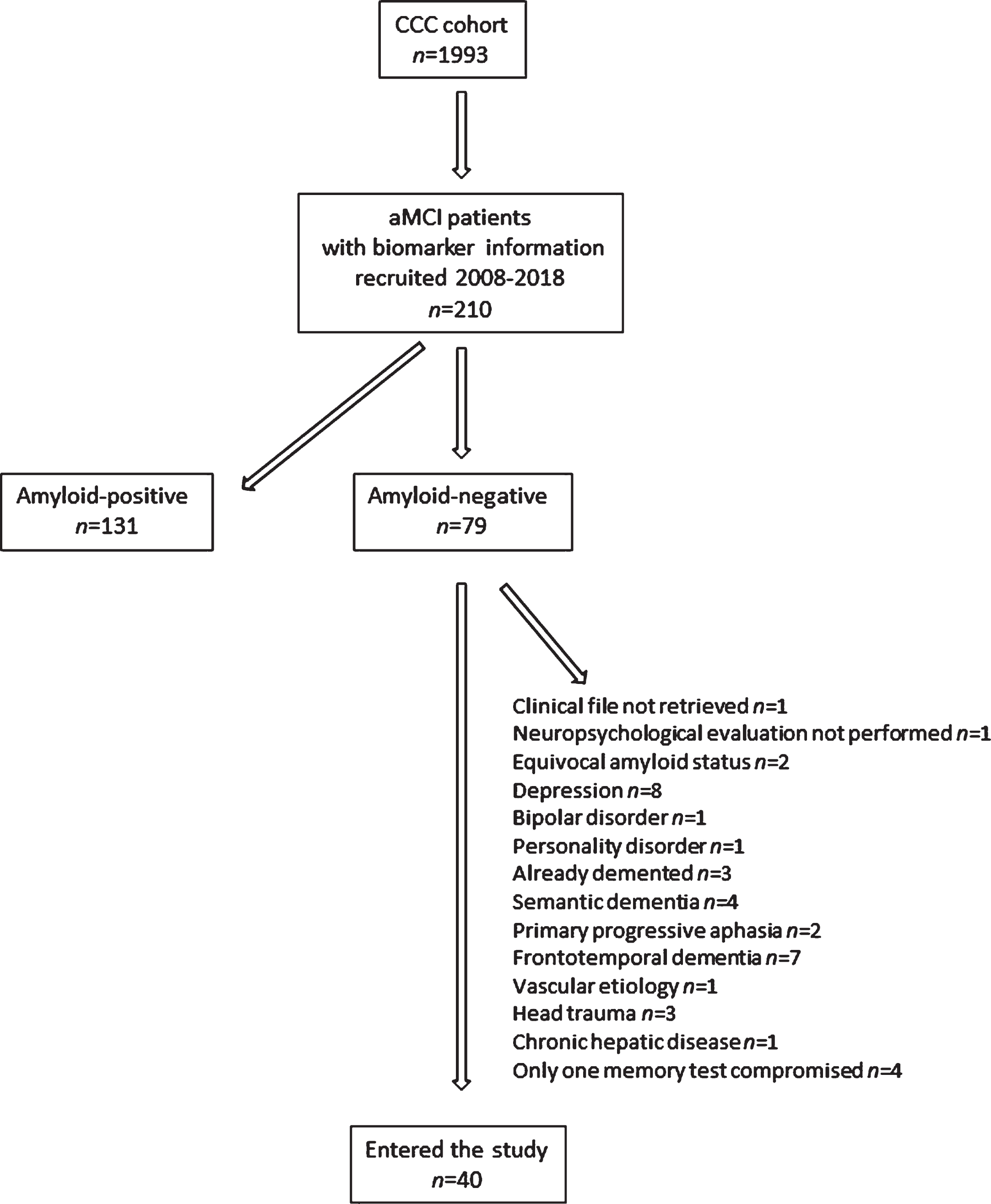
Flow-chart of patient selection for the study.
Baseline demographic and clinical characteristics of patients with amyloid-negative aMCI
The results of the baseline neuropsychological assessment are shown in Table 2. Patients were impaired (z score < –1) in measures of memory (Logical Memory), learning (CVLT) and orientation, as well as in executive functions (Trail Making Test B).
Baseline neuropsychological performance of patients with amyloid-negative aMCI
Means of z scores calculated according to the equation [z = (x-mean)/SD]. z score values below 1 SD of the mean are marked in bold. CVLT, California Verbal Learning Test.
It was possible to obtain follow-up data in all but 2 patients. The global follow-up time was 5.5±3.3 years (Table 1), and 6.5±3.5 years in patients who remained stable during the study. The individual outcomes are detailed in Table 3, showing that amyloid-negative aMCI represents a rather heterogeneous group of patients. About half of the patients (#1 to #19) remained essentially stable for long periods of time. Of these, only one (#8) admitted to becoming free from memory complaints. Other patients (#20 to #24) manifested a psychiatric disorder that was not apparent at baseline, namely major depression or bipolar disorder, showing no evidence of cognitive decline. Importantly, about a quarter of the patients (#25 to #34) developed a neurodegenerative disorder other than AD, mostly frontotemporal dementia or Lewy body disease. Finally, some patients (#35 to #38) suffered from serious intercurrent medical disorders affecting cognition, as would be expected in this aged population (Table 3).
Follow up of patients with amyloid-negative aMCI
F, female; M, male; DaTscan, single photon emission computed tomography with ioflupane; aMCI, amnestic mild cognitive impairment; MMSE, Mini-Mental State Examination; NPS evaluation, neuropsychological evaluation; N, normal; NA, not applicable; ND, not determined.
Regarding the 4 patients who had evidence of neurodegeneration at the baseline, as reflected in CSF elevated tau protein levels, one developed depressive syndrome, another was apparently cognitively stable suffering stroke a few years later, and the remaining two progressed to Lewy body disease (Table 3).
DISCUSSION
First, the majority of patients fulfilling criteria for aMCI who had biomarkers performed were amyloid positive, as would be expected from a condition designed to identify patients at early stages of AD. A second point is that, in patients with aMCI who were amyloid-negative, the review of the clinical files could often identify at the baseline a presumable cause for the memory deficits. Several patients were followed by the psychiatrist with the diagnosis of major depressive disorder, presenting concurrently substantial memory complaints. Others showed prominent behavioral symptoms suggestive of an initial phase of frontotemporal dementia, or language deficits indicating a primary progressive aphasia disorder. The patients where a presumable cause for memory decline might have been suspected at the baseline were excluded from the present study.
We observed that patients with amyloid-negative aMCI had deficits in memory, learning, and orientation tests at the baseline. Deficits in executive functions were also observed. Recent studies emphasized the presence of executive dysfunction in patients with aMCI [53], namely involving difficulties in inhibitory and interference control, cognitive control, and cognitive flexibility [54].
The main finding of the present study is that amyloid-negative aMCI represents a rather heterogeneous group of patients. As a consequence, classifying simply the patients with amyloid-negative aMCI as converters and non-converters [55] might conceal the diversity of distinct clinical entities. About half of the patients remained essentially stable, as found in previous studies [19, 56]. We now show that this stability may be observed for remarkably lengthy periods of time, more than a decade. Even though, cognitive complaints and memory deficits generally persisted. Although patients with high levels of depressive symptoms or psychiatric diagnoses were excluded, some manifested at the follow up a psychiatric disorder that was not apparent at baseline, namely major depressive disorder or bipolar disorder, showing no evidence of cognitive decline. In these cases, we may assume that the memory complaints and memory deficits observed at the baseline could be prodromal manifestations of an insidious psychiatric condition that would later become apparent. Other amyloid-negative aMCI patients developed a neurodegenerative disorder, mostly frontotemporal dementia or Lewy body disease, as reported by other authors [18, 56]. Two patients progressed to a non-specified form of dementia.
Although it was proposed that declining amyloid-negative aMCI patients might develop AD [19, 56], this hypothesis does not seem plausible taking into account the very long preclinical phase of AD, amyloid biomarkers being present for about 20 years before symptoms appearance [57]. In other words, if the cognitive symptoms were due to AD, the biomarkers should be present at the baseline. According to the recent biological AT(N) definition of Alzheimer’s disease, amyloid-negative aMCI patients should be considered outside the AD continuum [10]. The possibility that some aMCI cases considered as amyloid-negative might show insufficient amyloid accumulation to be detected by PiB-PET or have borderline levels of CSF Aβ1-42 might be considered. The use of CSF Aβ42/Aβ40 ratio was proposed as a normalization procedure and may provide a more accurate measure of the amyloid status in some patients [58]. In the present study, we would argue that the patients were truly amyloid negative, since the amyloid status was concordant between CSF measures and PiB-PET in all but two cases, that were excluded from the study. The clinical evolution of the amyloid-negative aMCI patients does not seem compatible with AD either, since the patients remained essentially stable or developed psychiatric or other neurodegenerative disorders. One might argue that the two cases that progressed to dementia not otherwise specified could have had AD to start with. This might be the case with #27, since the patient’s PET scan showed substantial PiB binding, although in an exclusively subcortical (nonspecific) topography. On the contrary, patient #28 had a completely normal value of CSF Aβ1-42 (858 pg/mL) at the baseline. The possibility that these two cases might have Limbic Predominant Age-associated TDP-43 Encephalopathy (LATE) [59] might also be considered, but LATE is for the time being essentially a neuropathological diagnosis.
The presence of biomarkers for neurodegeneration was associated with progression to dementia in healthy people and in patients with cognitive decline [60]. A previous study reported that amyloid-negative aMCI patients with high CSF tau, as a biomarker of neuronal injury, may have a high risk of progressing to dementia [61]. On the contrary, other studies found that amyloid-negative and tau-positive aMCI patients have a low risk for progression [62, 63]. As a matter of fact, amyloid-negative and tau-positive MCI patients might be included in distinct but overlapping diagnostic categories, namely suspected non-Alzheimer’s pathophysiology (SNAP), primary age-related tauopathy (PART), or even other primary tauopathies [64]. In the present study, only few participants had abnormal CSF tau levels (both total tau and phospho-tau), and they did not show a particularly negative outcome.
The present study has limitations regarding the small number of participants, and replication of the present findings in future studies is needed. A further limitation to consider is that part of the cohort had no CSF or imaging biomarkers of neurodegeneration available. The lack of MRI data should also be recognized as a limitation. The major strengths of the present study are the long follow-up time, and the fact that only two patients were lost to follow-up. We anticipate that methodological issues, such as the specific clinical setting, the definition of aMCI, the extent of exclusion criteria, the use of CSF or PET measures to establish the amyloid status, and the selection of biomarkers of neurodegeneration might assume a critical relevance for the characterization and prognosis of amyloid-negative aMCI patients.
As practical consequences, when communicating to the patient with aMCI and the family the results of biomarkers, a negative amyloid status reflecting the absence of AD is usually acknowledged as good news [65] but must be moderated by the information that some cases may later manifest psychiatric conditions or evolve to neurodegenerative disorders. For sure, clinical follow-up should be advised.
The present study shows that it may not be possible to classify individuals based on cognitive performance at initial stages of the neurodegenerative disorder. This emphasizes the importance of continuing developing cognitive outcome measures that correlate with biomarkers of disease and neurodegeneration and that can detect changes at the MCI stage or even before. Future studies should focus on how to distinguish the different types of amyloid-negative aMCI and to provide reliable prognostic information to the individual patient. Adding advanced neuroimaging techniques, more extensive mood and personality assessments, and other CSF biomarkers like neurofilament light might be of interest. Large collaborative studies with amyloid-negative aMCI would allow the use of machine learning techniques, namely feature selection ensemble approaches, to automatically choose the best predictors of future outcome, as was already done for MCI patients without amyloid status information [66].
In conclusion, amyloid-negative aMCI is a heterogeneous condition, many patients remain clinically stable, but others may later manifest psychiatric conditions or evolve to neurodegenerative disorders, so that prudence is needed when communicating to the patient and family the results of biomarkers, and clinical follow-up should be advised.