
Abstract
Background:
Impaired cerebrovascular reactivity (CVR) and blunted cerebral hemodynamic recruitment are thought to be important mechanisms linking hypertension to cerebrovascular and cognitive outcomes. Few studies have examined cardiovascular or dietary correlates of CVR among hypertensives.
Objective:
To delineate associations between cardiometabolic risk, diet, and cerebrovascular functioning among individuals with resistant hypertension from the TRIUMPH trial (n = 140).
Methods:
CVR was assessed by examining changes in tissue oxygenation (tissue oxygenation index [TOI] and oxygenated hemoglobin [HBO2]) using functional near-infrared spectroscopy (fNIRS) during a breath holding test, a standardized CVR assessment to elicit a hypercapnic response. Participants also underwent fNIRS during three cognitive challenge tasks. Vascular function was assessed by measurement of brachial artery flow-mediated dilation and hyperemic flow response. Cardiometabolic fitness was assessed from peak VO2 on an exercise treadmill test and body mass index. Dietary patterns were quantified using the DASH eating score. Cognitive function was assessed using a 45-minute test battery assessing Executive Function, Processing Speed, and Memory.
Results:
Greater levels fitness (B = 0.30, p = 0.011), DASH compliance (B = 0.19, p = 0.045), and lower obesity (B = –0.30, p = 0.004), associated with greater changes in TOI, whereas greater flow-mediated dilation (B = 0.19, p = 0.031) and lower stroke risk (B = –0.19, p = 0.049) associated with greater HBO2. Similar associations were found for cerebral hemodynamic recruitment, and associations between CVR and cognition were moderated by duration of hypertension.
Conclusion:
Impaired CVR elevated cardiometabolic risk, obesity, vascular function, and fitness among hypertensives.
Keywords
INTRODUCTION
Cardiometabolic risk factors and vascular function are increasingly recognized as risk factors for cognitive impairment and dementia [1–3]. Hypertension among middle-aged adults, with or without obesity, is an especially common source of increased risk for Alzheimer’s disease and related dementias (ADRD) in later life [4–6]. Despite the substantially increased risk of cognitive impairment and ADRD among middle-aged adults with hypertension, few studies have attempted to delineate mechanisms linking elevated blood pressure to cognitive impairment in this vulnerable patient group [7].
An increasingly large body of evidence suggests that hypertension and associated cardiometabolic risk factors may adversely impact cognitive function through their overlapping associations with poorer aerobic fitness [8], obesity [9–11], and subclinical vascular endothelial function [12–15]. Lower levels of aerobic fitness and poorer endothelial function have been associated with poorer performance on clinical measures of executive functioning, working memory, and processing speed, after accounting for conventional confounders [16–18]. Lifestyle habits, such as dietary behaviors, have also been suggested to play an important role in the association between cardiometabolic risk and cognition, although few studies have examined these associations in middle-aged and older adults with elevated of ADRD [19, 20]. In addition, although the associations between lifestyle factors and brain health are heterogeneous may vary by background demographic and clinical risk factors, few studies have attempted to examine individual differences linking cerebrovascular health to cognitive functioning [21–24]. Increasing age, duration of exposure to the adverse effects of hypertension [25, 26], APOE genotype [27], and biological sex [28], have all been suggested to influence the association between cerebrovascular function and cognitive decline. Delineating mechanistic associations between biomarkers of cerebrovascular function and individual differences linking cerebrovascular and cognitive function therefore holds importance to advancing strategies to reduce the risk of cognitive decline.
Functional near infrared spectroscopy (fNIRS) is a non-invasive modality of assessing cerebrovascular functioning in outpatient settings among individuals with elevated cardiometabolic risk [29, 30]. fNIRS measures provide non-invasive indices reflecting cerebrovascular reserve and reactivity when changes in oxygenated hemoglobin and tissue oxygenation (TOI) are quantified during various provocative vascular challenge measures [29, 31]. A commonly used metric of cerebrovascular reserve is the breath holding index, during which changes in cerebrovascular indices are examined while a participant holds their breath [32–34]. Changes in oxygenated hemoglobin during cognitive challenges have also been explored as a mechanistic marker of cerebral efficiency [35, 36]. Blunted cerebrovascular reactivity (CVR) has been associated with increased risk of stroke, cognitive impairment, and ADRD [37, 38]. Moreover, poorer cerebrovascular functioning has been suggested as a plausible mechanism linking exercise training with cognitive decline [38]. fNIRS therefore provides a feasible and prognostic marker of cerebrovascular functioning that is ideally suited for use among middle-aged adults with preclinical levels of cognitive impairment and ADRD risk. Our goals in the present study were to delineate the associations between CVR, cardiometabolic health, and markers of vascular function among middle-aged and older adults with resistant hypertension. We also sought to explore the association between cerebrovascular function and cognitive function, as well as the influence of plausible moderators of this association (age, duration of hypertension, and biological).
METHODS
Data for the present study were obtained as part of the TRIUMPH randomized controlled trial among adults with resistant hypertension [39]. TRIUMPH was a randomized controlled trial examining the efficacy of an intensive cardiac rehabilitation (CR)-based diet and exercise program in modifying lifestyle behaviors and lowering BP in resistant hypertension patients. The study is registered at www.clinicaltrials.gov (NCT03001427 and NCT03001427), and the trial methodology and principal results have been previously reported [40]. One hundred forty patients with resistant hypertension were randomized with 2:1 allocation to either a Center-based Lifestyle Intervention (C-LIFE) or Standardized Education and Physician Advice (SEPA). Data from the baseline assessments of trial participants are provided in the present report.
Patients with resistant hypertension, defined as treatment with 3 or more antihypertensive medications of different classes, including a diuretic, with clinic systolic blood pressure (SBP)≥130 mm Hg or diastolic blood pressure (DBP)≥80 mm Hg (modified from 140/90 mm Hg in November 2017), or the need for 4 or more drugs to achieve SBP≤130 mm Hg and DBP≤80 mm Hg, with SBP≥120 mm Hg were eligible. Additional inclusion criteria included body mass index (BMI)≥25 kg/m2, lack of regular moderate or vigorous physical activity, and age 35–80 years. Exclusion criteria included known secondary hypertension, estimated glomerular filtration rate (eGFR) < 40 ml/min/1.73 m2, moderate-severe ischemic heart disease, diabetes requiring insulin, and major psychiatric disorder or substance dependence, including alcohol consumption > 14 drinks/week.
Vascular risk factors
Framingham Stroke Risk Profile (FSRP)
The FSRP is a measure of 10-year stroke risk, with each 1-point increase associating with a 1% increased change of stroke. The FSRP is calculated separately for men and women and determines stroke risk based on antihypertensive medications, diabetes, heart failure, prior coronary disease, atrial fibrillation, and smoking. Because age was adjusted as a separate covariate, we did not include age in our calculation of the FSRP for the purposes of our reported regression models. For SBP, clinic-measured BP was determined according to standard clinical guidelines (The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure [JNC-7]), in which SBP and DBP are assessed in a quiet room with a standard rest period on multiple occasions in order to ensure validity [41].
Nutritional and weight assessment
An independent assessment of dietary and nutritional content was obtained by 2 separate self-report measures of diet: a retrospective food frequency questionnaire (FFQ) requiring participants to recall typical consumption during a 4-week period [42], and a 2-day (weekend/weekday) food diary [43]. The FFQ was analyzed by NutritionQuest (Berkeley, CA, USA), and the diary data were analyzed using the Automated Self-Administered 24-hour (ASA 24®) Dietary Assessment Tool (https://epi.grants.cancer.gov/asa24/). An overall Dietary Approaches to Stop Hypertension (DASH) eating plan score was quantified using a scoring algorithm used previously [44].
Aerobic fitness
Participants underwent a maximal graded exercise treadmill test in which workloads were increased at a rate of 1 metabolic equivalent per minute [45]. Expired air was collected by mouthpiece for quantification of minute ventilation, oxygen consumption, and carbon dioxide production with the Parvo Medics TrueOne measurement system (model 2400; Parvo Medics, Sandy, UT, USA).
Body mass index
BMI was calculated as height/weight2 (kg/m2). Body weight was determined by a calibrated digital scale (Detecto; Cardinal Scale Manufacturing Co, Webb City, MO, USA).
Vascular and microvascular endothelial function
Brachial artery flow-mediated dilation (FMD)
Our technique for assessing FMD followed procedures first described by Celermajer and colleagues [46]. FMD of the brachial artery was assessed following overnight fasting. Longitudinal B-mode ultrasound images of the brachial artery, 4–6 cm proximal to the antecubital crease, was obtained at end-diastole. Peak hyperemic flow and shear stress were derived by standard formulae based upon Doppler velocity measurements during the first 10 s following deflation of the occlusion cuff. Brachial artery diameter was assessed from 10–120 s post-deflation of the cuff using edge-detection software, with the peak arterial diameter quantified using polynomial curve fitting, and FMD was defined as the percent change in arterial diameter relative to pre-inflation baseline.
Microvascular endothelial function
Microvascular endothelial function was assessed by quantifying the % change in brachial artery flow with reactive hyperemia, which has been previously validated as a marker of microvascular function [47, 48]. Pulsed Doppler flow signals in the brachial artery were recorded at baseline and for up to 15 s after cuff release. The velocity-time integral for baseline and reactive hyperemia was based upon the mean of triplicate pulsed-Doppler flow tracings recorded at each of these phases. Hyperemic flow was calculated from hyperemic velocity and brachial artery cross-sectional area. In the present study, hyperemic velocity and flow demonstrated comparable associations and % change in flow was therefore used as our index of microvascular endothelial function.
Functional near infrared spectroscopy
Cerebrovascular reserve (CVR)
CVR was assessed non-invasively using fNIRS. When assessed by fNIRS, the increase in cerebral blood flow (CBF) in the surface layers of the cortex during localized neural activity is seen as an increase in the total concentration of hemoglobin (total-Hb) and comparative decrease in deoxy-Hb, with both variables corresponding strongly with the functional MRI BOLD signal [49] An increasing number of pharmacological trials [50] have used this technique to infer localized brain activity, CBF, and tissue oxygenation from changes in hemoglobin concentrations. In addition, changes in the prefrontal cortex using this technique have been found to be quite sensitive to cerebrovascular changes associated with exercise [51, 52] and have been used as an outcome in an increasing number of randomized, double-blind, dietary supplementation trials [53, 54]. fNIRS has also been found to discriminate between healthy adults and those with mild cognitive impairment [35] as well as providing a non-invasive marker of cerebral microvascular health [55]. Therefore, CVR provides a reliable, reproducible, and inexpensive measure of CVR [56].
CVR was measured as the change in tissue oxygen saturation from baseline during a standardized breath holding index (BHI) [57, 58]. The BHI has been used extensively as a marker of CVR, has been shown to decrease with age [32], is impaired among individuals with cerebrovascular disease [59, 60] and cognitive impairment [33], and is predictive of subsequent stroke [61]. Consistent with standard methodology, changes in tissue oxygen saturation (TOS) during BH was measured using two, near-infrared optodes of the cerebral oximetry, each consisting of two light-source fibers and one light-collecting fiber. Sensors was placed in two symmetrical points on the forehead in symmetric areas of the frontal lobe of the two hemispheres (2 cm beside the midline and about 3 cm above the supraorbital ridge) and fixed with a headband. CVR was quantified as changes in TOS from baseline to BHI, divided by baseline TOS and total BHI time (BHI = [TOSBH – TOSBAS]×100/ TOSBAS/DBH) [55]. Voluntary breath holding was used to induce hypercapnia, with a duration ranging from 20 to 30 s. Assessments lasting less than 20 s were repeated.
Cerebral hemodynamic cognitive changes
In addition to the BHI, we also examined changes in oxygenated hemoglobin during cognitive tasks known to elicit a large cerebral hemodynamic response that included recruitment of cortical brain regions impacted in hypertension, such as the dorsolateral prefrontal cortex. In order to accomplish this, participants underwent three sequential cognitive challenge tasks for 1 min each. The average increase in oxygenated hemoglobin across all three tasks was used as our marker of interest. In order, cognitive challenge tasks included 1) semantic fluency, 2) mental arithmetic, and 3) phonemic fluency. Alternate forms were used in a counterbalanced order for all cognitive tasks.
Neurocognitive performance
In order to characterize the associations between CVR, task-based cerebral activation, and neurocognitive performance, we also examined the associations between neuropsychological performance within the domains of Executive Function and Learning (Trail Making Test Part B, Stroop Color-Word Section [62], Animal Naming [63], Controlled Word Association [64], California Verbal Learning Test (CVLT)-II Discrimination Index [65], Brief Visuospatial Memory Test - Revised Learning [66]), Processing Speed (Trail Making Test Part A, Stroop Word Section [63], Stroop Color Section, Digit Symbol [67], Ruff 2&7 Test [68]), and Memory (CVLT-II Total Recall, CVLT-II Free Recall, and CVLT Delayed Recall). Scores were aggregated into mean-rank domain scores for the purposes of analysis.
Data analysis
Results for the present analyses were carried out using SAS 9.4 and R 3.6.3. Analyses characterizing the associations between CVR, cardiovascular disease risk, and lifestyle behavior were conducted first using simple correlation and second using general linear models controlling for age, education, gender, race, and creatinine. For our primary analyses, hierarchical regression modeling was used to delineate the unique and overlapping associations between cardiovascular disease risk, aerobic fitness, BMI, DASH diet pattern, and CVR. These biobehavioral predictors were selected because of their conceptual importance linking lifestyle patterns to reduced risk of stroke and cognitive decline. Within each model, we controlled a priori for age, education, biological sex, race, and creatinine, with CVR as the outcome. We also controlled for baseline TOI levels to mitigate the influence of any differential starting level on subsequent CVR changes during breath holding or the cognitive challenge tasks. These demographic and medical covariates were selected based on their known influence on functional brain indices and potential to confound inferences between biobehavioral predictors of interest and cerebrovascular outcomes. We then entered each variable of interest as an independent predictor in sequential steps: 1) Framingham stroke risk profile, 2) brachial artery flow mediated dilation, 3) microvascular hyperemic flow, 4) DASH diet adherence score, 5) BMI, and 6) aerobic fitness (peak VO2 from an exercise treadmill test). In a final regression step, we entered all predictors simultaneously in order to determine which predictor(s) continued to demonstrate an association with CVR metrics. We used changes in TOI as our primary outcome metric of interest. However, because changes TOI reflect both increases in oxygenated hemoglobin (comparable to BOLD signal change from fMRI) and total-Hb changes sensitive to macrovascular compliance, we conducted supplementary analyses of oxygenated hemoglobin in parallel with our TOI analyses.
In addition to our analyses examining correlates of CVR, we conducted ancillary analyses to better understand the association with CVR and cognitive functioning. We have previously published data from the present cohort demonstrating that greater stroke risk, poorer vascular function, greater obesity, and lower aerobic fitness all associated with cognitive performance [16]. In the present analyses, we therefore limited our array of potential predictors by examining the association between CVR and cognitive functioning, with exploration of plausible moderating factors: age, biological sex, and duration of hypertension history. These associations were conducted using a mean-rank, global score for each cognitive domain (Processing Speed, Executive Function, and Memory), adjusting for the same covariates as in our primary analyses above (age, education, sex, race, and creatinine). TOI changes during the breath holding challenge were used as the variable of interest and we included the interaction terms between BHI and age, sex, and duration of hypertension history as interaction terms within the same model in order to mitigate the effects of multiplicity. Power for the present study was determined based on the primary trial [40], which was designed to assess treatment-related changes in blood pressure and metabolic function. A post hoc power analysis demonstrated that we would have had 80% power to detect a correlation of 0.20 between our predictors of interest and outcomes based on the following assumptions: a sample size of 140, an alpha of 0.05, and an R-square of 0.30 between our covariates. Assumptions regarding linearity, independence, and homogeneity of model residuals were inspected and found to be acceptable prior to analysis. Several of our CVR outcome variables were found to be positively skewed and were log-transformed prior to inclusion within our regression models, including TOI and oxygenated hemoglobin indices.
RESULTS
One hundred forty individuals with resistant hypertension were enrolled in the study. Participants tended to be older (62.5 years [SD = 8.9]), African American (59%), overweight/obese (mean BMI = 36.0 [SD = 5.7]), and were at high risk of stroke (mean 10-y stroke risk = 10.2 [SD = 3.4]). Participants reported a history of hypertension lasting several decades (mean = 22.2 years [SD = 11.8]).
Background characteristics and cerebrovascular reactivity
Examination of unadjusted associations between CVR and other variables of interest demonstrated longer duration of hypertension, lower levels of fitness, lower FMD, and higher levels of obesity all associated with poorer CVR (Table 1).
Correlations with cerebrovascular reactivity measures across background characteristics, clinical factors, and markers of lifestyle factors. Correlations are adjusted for average
**p < 0.01; *p < 0.05; †p < 0.10. TOI, tissue oxygenation index; HBO2, oxygenated hemoglobin; SBP, systolic blood pressure; DBP, diastolic blood pressure; DASH, Dietary Approaches to Stop Hypertension; FSRP, Framingham Stroke Risk Profile; ASCVD, atherosclerotic cardiovascular disease.
Vascular function, lifestyle factors, and cerebrovascular reactivity
Examination of hierarchical regression models for TOI changes are presented in Table 2. Results demonstrated that greater DASH diet compliance (B = 0.19, p = 0.045), lower levels of obesity (B = –0.30, p = 0.004) (Fig. 1), and greater levels of aerobic fitness (B = 0.30, p = 0.010) (Fig. 2) associated with greater changes in TOI. As shown, individuals with lower levels of obesity and higher levels of aerobic fitness showed greater CVR compared to their more obese and less aerobically fit counterparts. In a final model including all variables of interest, only obesity and DASH diet compliance tended to show an association with TOI changes.
Hierarchical regression analyses examining correlates of TOI changes during the breath holding task. Values represent standardized betas
**p < 0.01; *p < 0.05; †p < 0.10. TOI, tissue oxygenation index; FSRP, Framingham Stroke Risk Profile; FMD, Flow-mediated dilation; DASH, Dietary Approaches to Stop Hypertension; BMI, body mass index.
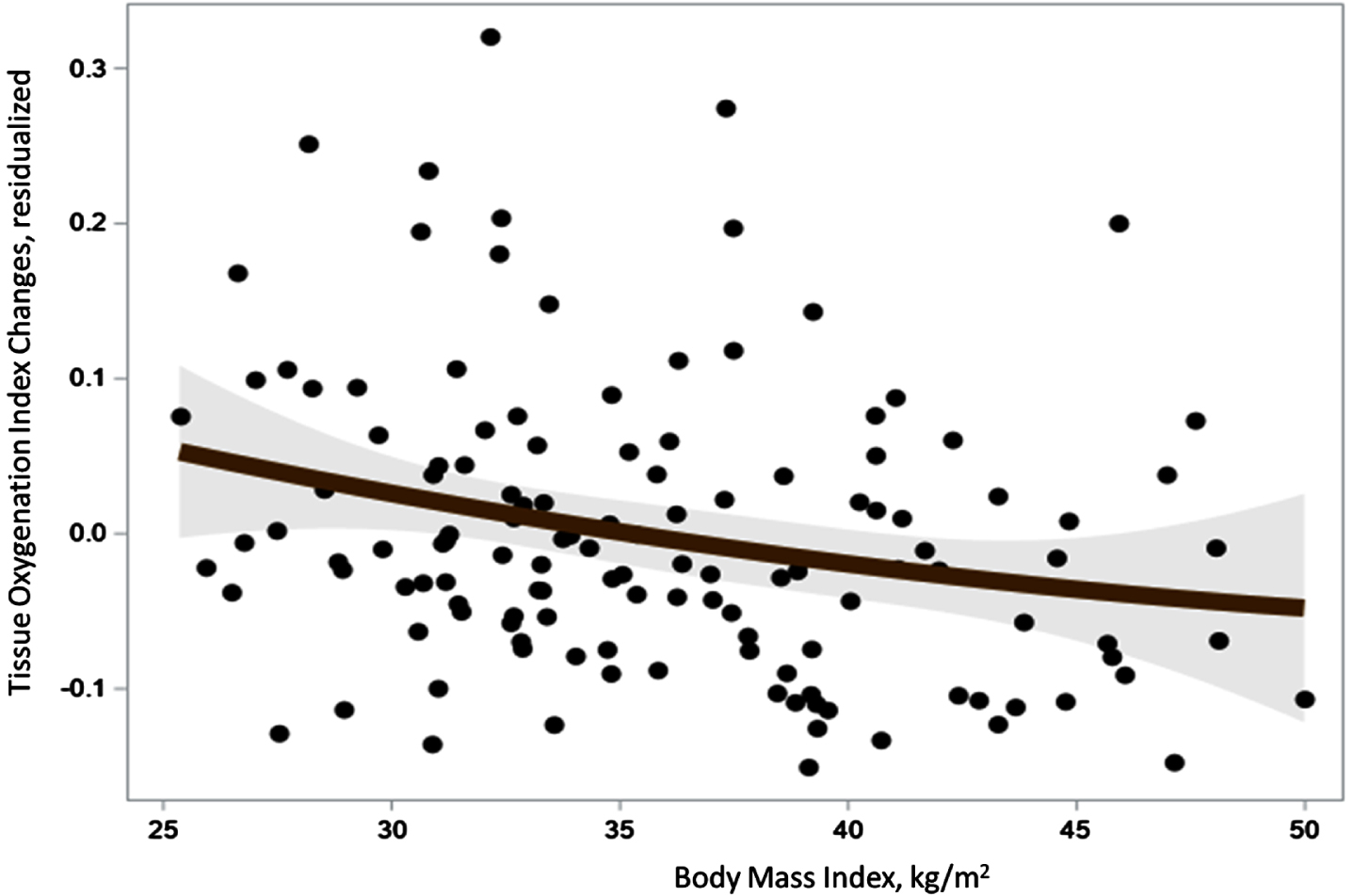
Body mass index and tissue oxygenation index cerebrovascular reactivity during the breath holding task.
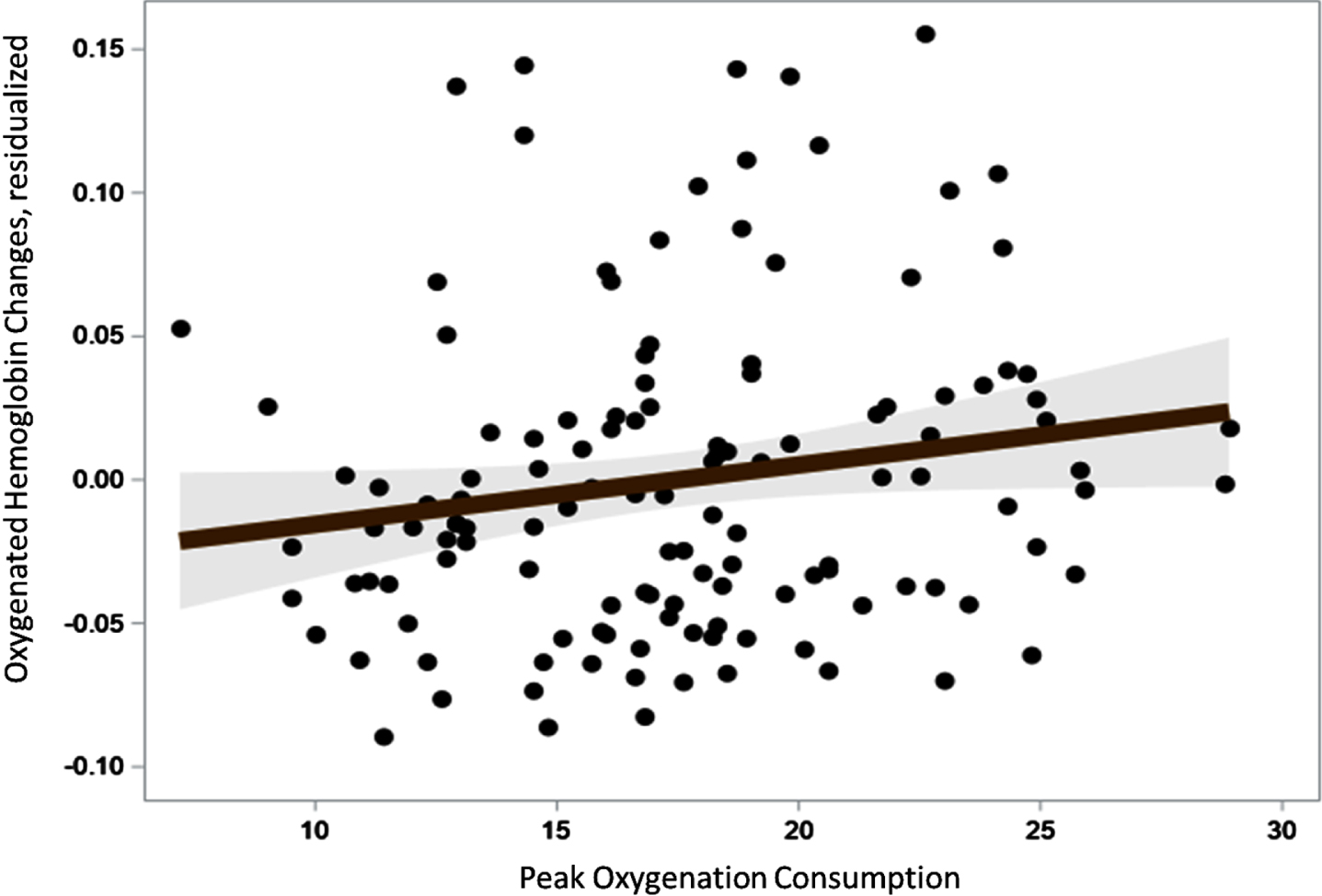
Peak VO2 and oxygenated hemoglobin changes during the breath holding task.
Examination of hierarchical models for oxygenated hemoglobin (HBO2) changes are presented in Table 3. Results demonstrated that lower stroke risk (B = –0.19, p = 0.049), higher FMD levels (B = 0.19, p = 0.031) (Fig. 3), greater DASH diet compliance (B = 0.16, p = 0.045), lower levels of obesity (B = –0.19, p = 0.027), and greater levels of aerobic fitness (B = 0.22, p = 0.049) were associated with changes in HBO2. Individuals with better dietary quality, vascular function, fitness, and lower obesity showed greater capacity for cerebrovascular changes while completing cognitive challenge tasks. For example, individuals with greater FMD levels, as indicated by brachial artery dilation in response to reactive hyperemia, showed greater cerebrovascular responsivity while performing cognitive challenge tasks. In a final model incorporating all variables of interest, only BMI continued to remain associated with HBO2 changes.
Hierarchical regression analyses examining correlates of oxygenated hemoglobin changes during the breath holding task. Values represent standardized betas
**p < 0.01; *p < 0.05. TOI, tissue oxygenation index; FSRP, Framingham Stroke Risk Profile; FMD, Flow-mediated dilation; DASH, Dietary Approaches to Stop Hypertension; BMI, body mass index.
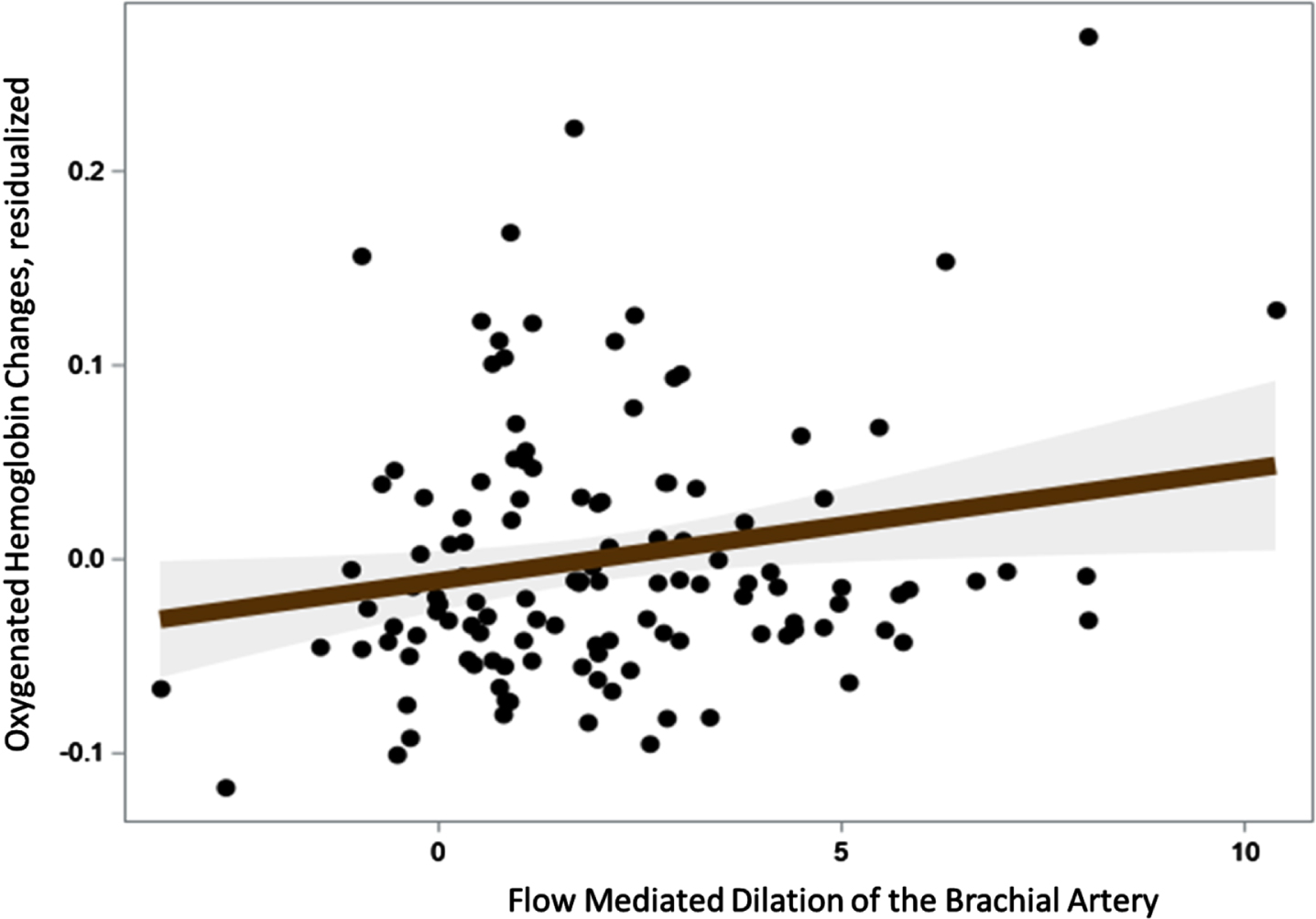
Flow-mediated dilation of the brachial artery and oxygenated hemoglobin changes during cognitive challenge tasks.
Vascular function, lifestyle factors, and cerebral hemodynamics during cognitive challenges
Examination of hierarchical models for cerebral hemodynamic changes are presented in Table 4. Results demonstrated that lower FSRP levels (B = –0.19, p = 0.031), higher FMD levels (B = 0.23, p = 0.014), greater brachial hyperemic flow response (B = 0.24, p = 0.015), and higher VO2 (B = 0.22, p = 0.030) all associated with greater cerebral hemodynamic recruitment during cognitive challenge tasks. In a final model including all predictors (excluding microvascular function due to high collinearity with FMD), we found that higher FMD was the strongest correlate of higher cerebral hemodynamic recruitment (B = 0.18, p = 0.040) with a similar trend for lower FSRP levels (B = –0.17, p = 0.065).
Hierarchical regression analyses of cerebral hemodynamic responses to cognitive challenge tasks. The mean increase in oxygenated hemoglobin across a semantic fluency, mental arithmetic, and phonemic fluency task was used as our measure of cerebrovascular hemodynamic response. Values represent standardized betas
**p < 0.01; * p < 0.05; †p < 0.10. TOI, tissue oxygenation index; FSRP, Framingham Stroke Risk Profile; FMD, Flow-mediated dilation; DASH, Dietary Approaches to Stop Hypertension; BMI, body mass index.
Cerebrovascular reactivity and cognitive function
Examination of TOI changes and cognitive function revealed no association between CVR and Processing Speed (B = 0.02, p = 0.784), Executive Function (B = –0.03, p = 0.787), or Memory (B = –0.5, p = 0.568) as a main effect. However, we found that the associations between cerebrovascular activity cognitive functioning was moderated by duration of hypertension history for both Processing Speed (p = 0.046) and Executive Function (p = 0.017) (Fig. 4). Explanatory analyses by tertiles of hypertension history duration revealed that the strength of association between CVR and cognitive function increased with longer durations of hypertension. For Processing Speed, the magnitude of association varied from B = –0.32, p = 0.07 among individuals with < 15 years of hypertension, B = 0.11, p = 0.399 for individuals with 15–25 years of hypertension, and B = 0.30, p = 0.023 among individuals with < 25 years of hypertension. A similar pattern was evident for Executive Function, with B = –0.40, p = 0.017 among individuals with < 15 years of hypertension, B = 0.11, p = 0.390 for individuals with 15–25 years of hypertension, and B = 0.22, p = 0.142 for individuals with < 25 years of hypertension.

Cognitive performance on tests of Processing Speed and Executive Function with cerebrovascular reactivity measures (tissue oxygenation index [TOI]) from the breath holding test grouped by duration of hypertension history. Values represent residualized estimates from fitted regression models. As shown, individuals with longer history of hypertension showed stronger associations with cognitive performance. Individuals with shorter hypertension histories (< 15 years; black lines) showed weaker, slightly negative associations between cerebrovascular reactivity and cognition, whereas individuals with moderately long hypertension histories (15–25 years; purple lines) and individuals with the longest hypertension history (> 25 years; green lines) showed the strongest associations.
DISCUSSION
Cardiometabolic risk factors have been associated with increased risk of cognitive impairment and ADRD risk. The present study extends prior work linking midlife cardiometabolic risk to cerebrovascular functioning by demonstrating that markers of subclinical vascular function associate with cerebrovascular markers from fNIRS assessments. In addition, markers of aerobic fitness, obesity, and dietary patterns associated with fNIRS measures, further underscoring the potential relationships between lifestyle behaviors and cerebrovascular functioning among middle-aged adults at risk for late-life cognitive decline. Finally, we found that the association between cerebrovascular and cognitive functioning was moderated by duration of hypertension history, which extends prior work demonstrating individual differences in demographic and clinical background characteristics that may influence the role of cerebrovascular function on brain health [69, 70]
Previous data have suggested that cerebrovascular functioning may be altered among middle-aged [71, 72] and older adults with hypertension [73–75]. Individuals with a longer duration of hypertension exhibit blunted CVR, as well as increased risk of cognitive decline, stroke, and dementia compared to their healthy counterparts [74]. Despite the widely replicated association between hypertension and poor cerebrovascular function, the mechanisms linking hypertension to impaired CVR have not been widely studied [76]. A recent study among middle-aged adults found that greater levels of obesity were associated with poorer cerebrovascular functioning, largely paralleling the present results [76]. Prior studies have also demonstrated associations between blunted vascular endothelial cell functioning and impaired cerebrovascular autoregulatory function among older adults [77–79] and patients with known vascular disease [80]. Our findings that aerobic fitness and dietary health were associated with CVR are novel and have not previously been reported outside of animal studies [81], to our knowledge. These findings are consistent with prior work demonstrating that better dietary health, such as higher Mediterranean diet scores [82], and greater aerobic fitness [83, 84], are associated with better cerebrovascular functioning across multiple different clinical samples of varying ages and levels of cognitive dysfunction [85–87]. Our findings therefore parallel existing work among older adults with known vascular dysfunction and extend these previously demonstrated associations to middle-aged and older adults with resistant hypertension.
Our finding that vascular endothelial function was the strongest correlate of cerebrovascular changes during cognitive challenge tasks is novel and warrants additional replication. Our work parallels that by Haley and colleagues, among others [88, 89], demonstrating that fMRI changes during cognitive tasks associate with peripheral markers of endothelial functioning in healthy middle-aged adults. In addition, peripherally-assessed endothelial functioning has been robustly associated with other markers of cerebrovascular health, including degree of white matter hyperintensities [90], small vessel disease burden [91], and cerebral angiography [92, 93]. Moreover, the degree of change in BOLD fMRI signal during cognitive challenges, which is conventionally interpreted as approximating neuronal activation, has been shown to associate strongly with BOLD changes during CVR challenges [94, 95]. Taken together with findings demonstrating that the relationship between cerebrovascular risk factors and cognitive performance may be substantially mediated by endothelial dysfunction [18], our findings suggest that fitness, obesity, and vascular risk may increase ADRD risk through overlapping impacts on cerebrovascular function and task-based oxygenation changes.
Our findings suggest several important extensions from prior work linking lifestyle factors, cerebrovascular function, and cognitive function. First, our findings suggest that multiple risk pathways, including diet, obesity, and vascular risk, may have convergent effects on worsening cerebrovascular functioning. We noted that multiple, overlapping individual risk factors were associated with cerebrovascular functioning and that when modeled together the majority of their associations were explained by obesity and diet. This is potentially important as it suggests that, even among individuals with elevated vascular risk, both diet and obesity have an important influence on brain health. This parallels prior intervention work demonstrating that dietary, cardiovascular, and metabolic factors [96–98] may act in parallel to improve cognitive functioning, whereas reductions in vascular risk do not fully mediate the effects of lifestyle changes on cognition. Second, our findings suggest that cerebrovascular functioning may serve as a protective buffer against cognitive decline that worsens with greater exposure to the adverse effects of hypertension. This finding extends prior work demonstrating a complex interplay between chronological age, hypertension history, and cognition, with uncoupling of the neurovascular unit occurring as part of a cascade of systemic changes [23, 26]. As noted elsewhere [22], the associations between CVR and cognition have been inconsistent, with large variations between middle-aged and older cohorts. Our results, if replicated, suggest that greater systemic exposure to the adverse effects of hypertension may partially explain these individual differences, with cerebrovascular function serving as an important buffer among individuals with a longer history of hypertension.
Limitations
The present findings must be viewed with several limitations in mind. First, the present data is based on a relatively small clinical sample of individuals with resistant hypertension and therefore requires replication. Indeed, although we were able to demonstrate associations between multiple biobehavioral predictors of interest and cerebrovascular function, many of our analyses we were likely underpowered. Second, inferences regarding cerebrovascular and cortical changes in the present study are somewhat limited by our use of fNIRS, which is limited by its derivation of cerebrovascular changes using non-invasive measurements from the scalp. However, our use of this accessible, non-invasive assessment modality likely increased the generalizability of our findings by allowing us to deploy these measurements in a representative clinical cohort of individuals with resistant hypertension. Indeed, our assessment of individuals with resistant hypertension was one to carefully examine cerebrovascular mechanisms of cognitive function [99]. Finally, our analyses of hypertension history are limited by the inherent difficulty with accurately demarking the onset of hypertension, which may often go undiagnosed. In the present study, we relied on a careful clinical interview with verification using medical records whenever available, which helps mitigate potential confounds from self-report bias. Secondary analyses within longitudinal cohort studies, and future prospective cohort studies, should attempt to replicate the present findings.
Conclusions
Our findings suggest that aerobic fitness, obesity, and endothelial function all associate with different aspects of cerebrovascular health and cognitive function among individuals with resistant hypertension. These findings extend prior work among adults with hypertension and older adults with small vessel disease by demonstrating that non-invasive measures of cerebrovascular function associate robustly with markers of vascular risk and task-based cerebral hemodynamic changes.