
Abstract
Background:
Dementia is one of the top causes of death worldwide, but individuals with dementia and their caregivers report that knowing what to expect, including regarding approaching end of life, is an unmet need.
Objective:
To identify predictors of death in individuals with Alzheimer disease (AD) dementia, Lewy body dementia (LBD), vascular dementia, and frontotemporal dementia.
Methods:
The study used data from National Alzheimer’s Coordinating Center participants with dementia and an etiologic diagnosis of AD, Lewy body disease, frontotemporal lobar degeneration (FTLD, with or without motor neuron disease), or vascular dementia. Analyses included median survival across dementia types and predictors of death at 5 years based on baseline demographics and clinical measure performance. Five-year survival probability tables were stratified by predictor values.
Results:
Individuals with AD had the longest survival (median 6 years), followed by FTLD (5 years), and vascular dementia and LBD (each 4 years). The strongest predictors of death for the full cohort were dementia type (higher risk with non-AD dementias), sex (higher risk with male sex), and race and ethnicity (higher risk with white and non-Hispanic participants). Age was associated with higher mortality risk across the non-Alzheimer dementias; other significant associations included worse cognitive status (FTLD, LBD) and more depression (LBD).
Conclusion:
Results can help clinicians counsel individuals with dementia and families regarding average dementia trajectories; findings regarding individual risk factors can aid individualizing expectations. Further research is needed to investigate drivers of mortality in the non-AD dementias to improve counseling and help identify potentially modifiable factors.
Keywords
INTRODUCTION
Alzheimer disease (AD) and Alzheimer disease-related dementias (ADRDs) are among the top ten causes of death worldwide. In 2019, AD and ADRDs were the third most common cause of death in Europe and the Americas [1]. Dementia quality measures recommend comprehensive counseling regarding ongoing palliation and end of life decisions within 2 years of initial diagnosis or assumption of care [2]. However, in one study of caregivers of individuals with dementia with Lewy bodies, only 22% of caregivers reported a helpful conversation with physicians regarding what to expect at the end of life [3]. In another study, only 35% of dementia caregivers said they received advice about what to expect in the future [4]. Across studies, individuals with dementia and caregivers reported that understanding what to expect in dementia was an unmet need [3–7] and over a quarter of families reported not knowing that dementia could lead to death [8]. However, awareness of dementia as terminal condition was associated with improved patient comfort at the end of life [8]. Unsurprisingly given these unmet needs, understanding dementia trajectories [9] and improving end-of-life care [10] are published dementia research priorities.
Recognizing approaching death in dementia is critical for patient and family counseling and for connecting patients and families to palliative care and hospice services. While interest in palliative care in dementia is increasing [11], most individuals with dementia do not access palliative care services [12]. When palliative care is used in dementia, it is commonly initiated only in the last weeks of life [3, 12], limiting the potential benefits that patients and families could receive from palliative care and hospice services. These delays may relate to the fact that recognizing the end of life in dementia can be challenging [13]. Additionally, in the United States (U.S.), Medicare guidelines for hospice eligibility in dementia had a sensitivity of only 0.20 (95% CI 0.13–0.28) for 6-month mortality in nursing home residents with dementia, though specificity was high (0.89; 95% CI 0.86–0.92) [14].
Sparse research provides tools for clinicians to counsel individuals with dementia and family members regarding life (and death) expectancy. In 2020, Haaksma and colleagues published prediction tables for 3-year survival in dementia based on age, diagnosis (AD versus frontotemporal dementia (FTD)/Lewy body dementia versus vascular dementia/mixed/other), Mini-Mental State Examination (MMSE) score, and comorbidities. These tables yielded c-indices of 0.70–0.72, with predictors of mortality including higher age, male sex, increased comorbidity burden, lower cognitive function at diagnosis, a diagnosis of a non-AD dementia, living alone, and using more medications [15]. However, this analysis did not include some potentially relevant clinical variables (e.g., psychiatric symptoms) and replication in non-Swedish cohorts is needed. Thus, the current study aimed to use data from the National Alzheimer’s Coordinating Center (NACC) to identify predictors of death in individuals with the most common dementias: AD dementia, LBD, vascular dementia, and FTD.
METHODS
Data source
This cohort study used data from NACC, a database with longitudinal data collection from over 40,000 participants at 41 Alzheimer Disease Research Centers (ADRCs) in the U.S. at the time of data request. Each study site obtains local institutional review board approval for conduct at their site. The University of Washington Human Subjects Division determined that the NACC database itself is exempt from IRB review/approval because it does not meet criteria for human subjects research. The University of Florida IRB confirmed that the current analysis met exempt criteria (IRB202102267). Prior publications described NACC recruitment and data collection [16–18]. Data for the current analysis represented uniform data set (UDS) participants as of the December 2020 data freeze.
Participants
NACC participants were eligible for the current analysis if their cognitive status was dementia and the primary etiology was AD, Lewy body disease (LBD), frontotemporal lobar degeneration (FTLD, with or without motor neuron disease), or vascular dementia. Because the focus of this analysis was on assessing predictors of mortality overall and as stratified by clinical diagnosis, neuropathological data were not requested or analyzed.
Measures
The current study used demographic variables including age, sex, race/ethnicity (self-report), education, marital status, living situation (alone or with others), and type of residence/living location (e.g., private residence, retirement community, assisted living, skilled nursing). Disease-related variables included primary etiologic diagnosis (of dementia), age at symptom onset, and whether multiple dementia diagnoses were recorded (primary and contributing dementia diagnoses). Medical history assessed included a cardiovascular risk index (0–4 score based on diabetes, obesity, hypertension, hypercholesterolemia) [19], smoking history, an approach to the Carlson Comorbidity Index adapted for NACC (0–4 score based on cardiac arrest, congestive heart failure, cerebrovascular disease, and diabetes) [20], and the number of medications reported at the most recent visit.
Cognition was assessed using the MMSE [21], Montreal Cognitive Assessment (MoCA) [22], and the CDR® Dementia Staging Instrument [23] Sum of Boxes (CDR-SB). MoCA scores were converted to MMSE scores using the NACC crosswalk [24]. The Neuropsychiatric Inventory –Question-naire (NPI-Q) [25] and Geriatric Depression Scale (GDS) [26] assessed behavioral and psychiatric symptoms. The NPI-Q queried the study partner regarding the presence of delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, elation/euphoria, apathy/indifference, disinhibition, irritability/lability, motor disturbance, nighttime behaviors, and appetite/eating [25]. The NACC Functional Activities Questionnaire [27] evaluated the degree of help needed with daily activities.
Statistical analysis
Alzheimer Disease Research Center visits occur annually. Variables were assessed at the first NACC visit with a diagnosis of dementia, considered the baseline visit for the purposes of this analysis. Survival time (year scale) was calculated as the duration from the baseline visit to death. Censoring occurred at the last visit for those participants who did not die in the study. For participants without follow-up after the baseline visit, censoring occurred at a half-year after the baseline visit. List-wise deletion was used throughout all analyses.
We applied the LASSO method for survival analysis [28] to select predictors for survival time and a Cox proportional hazards model [29] to estimate the effect of the predictors on survival time. The final prediction model was chosen by 10-fold cross-validation in LASSO. The model prediction performance was assessed by discrimination and calibration. The optimism-corrected Harrell C-index [30] was calculated by bootstrapping (B = 150) to assess the discrimination with adjustment of overfitting. This index ranges from 0 to 1, with higher values indicating a higher discrimination ability. The calibration plots were used to visually assess the calibration of the model, where the predicted and observed survival probabilities were compared. The proportional hazard assumption for Cox model was verified by scaled Schoenfeld residuals. Point estimate along with 95% confidence intervals (CI) and p-values for the effects of selected predictors were generated from the Cox model. Bonferroni correction was applied with a factor of 5 since there were 5 sets of analysis for the overall population and four subpopulations. Thus p-values≤0.01 were considered statistically significant.
To visualize the influence between the predictors and survival time for each dementia etiology, 5-year survival probability tables were created and stratified by combinations of predictor values. These predictors were chosen based on 1) variables selected by LASSO and 2) data that are available to most clinicians at dementia visits, regardless of clinician specialty type. The first five variables identified by the LASSO were dementia type, age, sex, MMSE, and CDR-SB. However, the CDR® requires training to do accurately and is often not completed outside dementia specialty clinics and research settings. Thus, race/ethnicity (black/African-American non-Hispanic, white non-Hispanic, and white Hispanic) was used as the final variable for making the survival probability tables.
RESULTS
The current study included data obtained through December 2020 and reflected data from 41 ADRCs. Demographic details and presentation characteristics (e.g., MMSE scores) of the 17,784 individuals meeting inclusion criteria are detailed in Table 1, stratified by diagnosis. Due to missing values, data were insufficient to include family history, APOE4 status, and the Functional Activities Questionnaire in analyses.
Characteristics of Eligible Participants by Diagnosis (n = 17,784)
Results presented as number (percent) or median (interquartile range). AD, Alzheimer disease; FTLD, frontotemporal lobar degeneration; LBD, Lewy body disease; NA, not available; CDR-SB, CDR – Sum of Boxes; MMSE, Mini-Mental State Examination; NPI-Q, Neuropsychiatric Inventory – Questionnaire; GDS, Geriatric Depression Scale. *At first visit with dementia diagnosis.
Survival
Of the 17,784 individuals eligible for the analysis, 7,745 (43.6%) were identified as deceased (5,799 AD, 1,064 FTLD, 680 LBD, 202 vascular dementia). Median survival for the full sample was 5 years (IQR 3–8). Individuals with AD had the longest survival (median [IQR]: 6 [3–8]), followed by FTLD (5 [3–7]), vascular dementia (4 [3–6]), and LBD (4 [2–6]). Participants identified as having AD had the highest probability of 5-year survival (Fig. 1, p < 0.0001). The unadjusted hazard ratio (HR) for death during follow up was 1.37 (95% CI 1.30–1.44, p < 0.001) in individuals with non-AD dementia (FTLD, LBD, vascular dementia) compared to AD dementia.
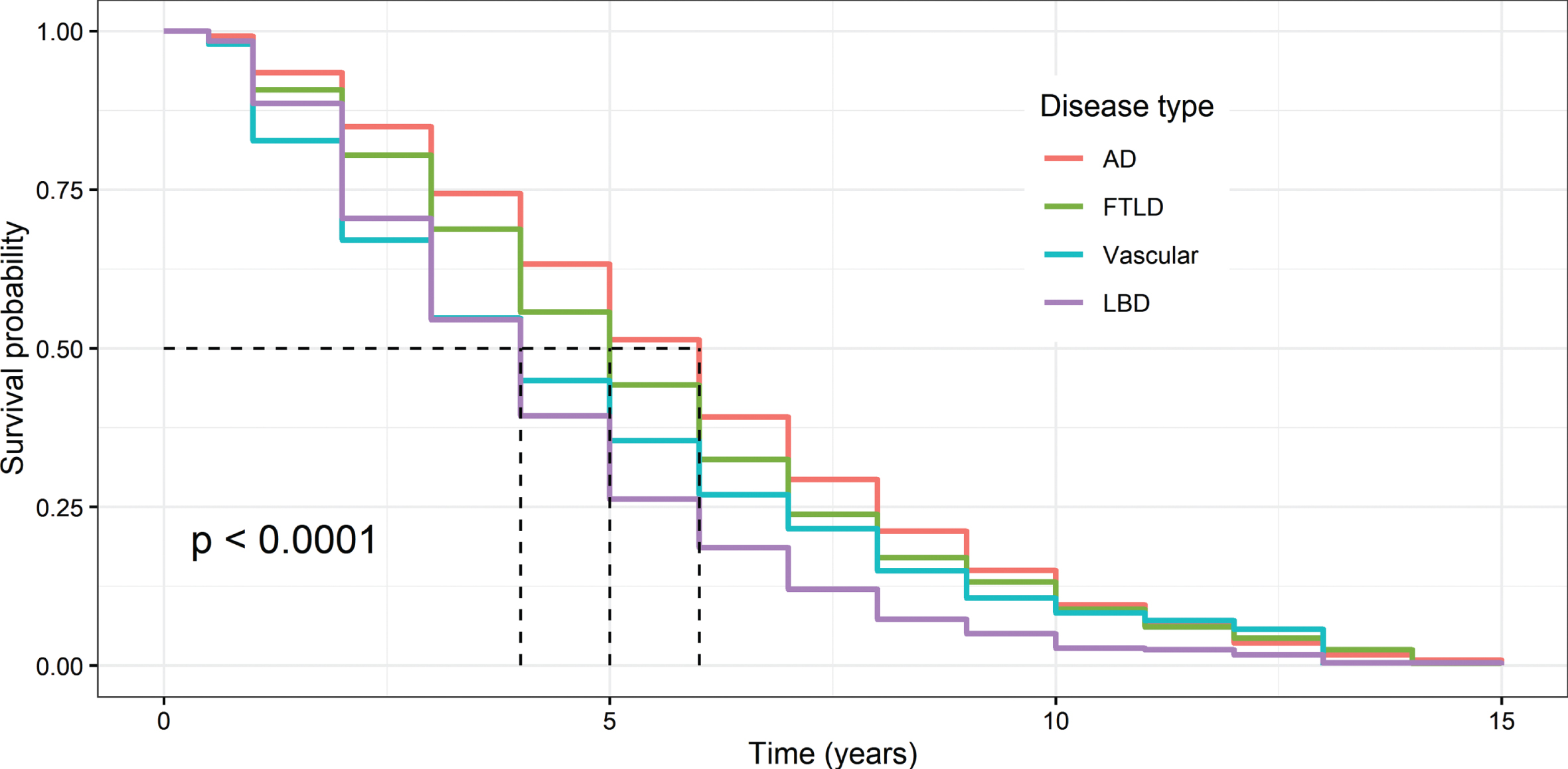
Unadjusted 5-Year Survival Probability Across Dementia Types. N = 17,784. Kaplan-Meier plots. The dashed lines indicate median survival: 4 years for vascular dementia and Lewy body dementia (LBD), 5 years for frontotemporal lobar degeneration (FTLD), and 6 years for Alzheimer’s disease dementia (AD). p value is for log-rank test with a null hypothesis that all groups have the same failure distribution.
Predictors of mortality
After excluding participants with missing data needed for the predictor analysis, data from 11,338 participants were used for the models predicting death during follow up (Table 2). Significant variables included age at symptom onset, sex, race, ethnicity, dementia type (AD versus non-AD), having multiple dementia diagnoses (primary and contributing dementia etiologic diagnoses), type of residence (private versus not private), comorbidity score, cardiovascular risk index, years of smoking, number of medications, MMSE, CDR-SB, NPI-Q, and GDS (variables assessed at first NACC visit) (Table 2). The strongest predictors of death for the full cohort were dementia type (higher risk with non-AD dementias), sex (higher risk with male sex), race (higher risk for white participants), and ethnicity (higher risk for non-Hispanic participants).
Predictors of death during follow up by dementia diagnosis based on multivariable Cox regression models
The n of 11,338 reflects all participants from the full cohort (n = 17,784) who had all the data for the variables included in the models. Data are from first visit, presented as hazard ratios (95% CIs). p-values < 0.01 are bolded. NR indicates not relevant; this analysis was for the full cohort only and compared AD to the non-AD groups combined. N/A indicates that the variable was not selected by the LASSO for the analysis for the individual population reported. Variables with insufficient sample size not included. AD, Alzheimer disease; FTLD, frontotemporal lobar degeneration; LBD, Lewy body disease; NACC, National Alzheimer Coordinating Center; MMSE, Mini-Mental State Examination; CDR-SB, CDR® Dementia Staging Instrument Sum of Boxes; NPI-Q, Neuropsychiatric Inventory –Questionnaire; GDS, Geriatric Depression Scale. *At first visit with dementia in NACC.
Multiple variables were associated with death at the p≤0.01 level in the AD dementia cohort (Table 2), largely overlapping with findings for the full cohort. In the smaller non-AD cohorts, older age at symptom onset was associated with in-creased risk of death across diagnoses. In the FTLD group, the only other variables associated with death at the p≤0.01 level were MMSE and CDR-SB scores. In the LBD group, ethnicity (higher risk for non-Hispanic participants), CDR-SB (higher scores associated with higher risk of death), and GDS scores (higher scores associated with higher risk of death) were associated with mortality. In vascular dementia, not living alone was the only variable that significantly associated with a higher risk of death (Table 2). Point estimates for hazard ratios were generally similar across groups but with wider confidence intervals in the non-AD dementia cohorts.
To help clinicians visualize the influence of these predictors on survival, risk tables were created for male and female participants stratified by diagnosis, age at symptom onset, sex, MMSE score, and race/ethnicity (Fig. 2).
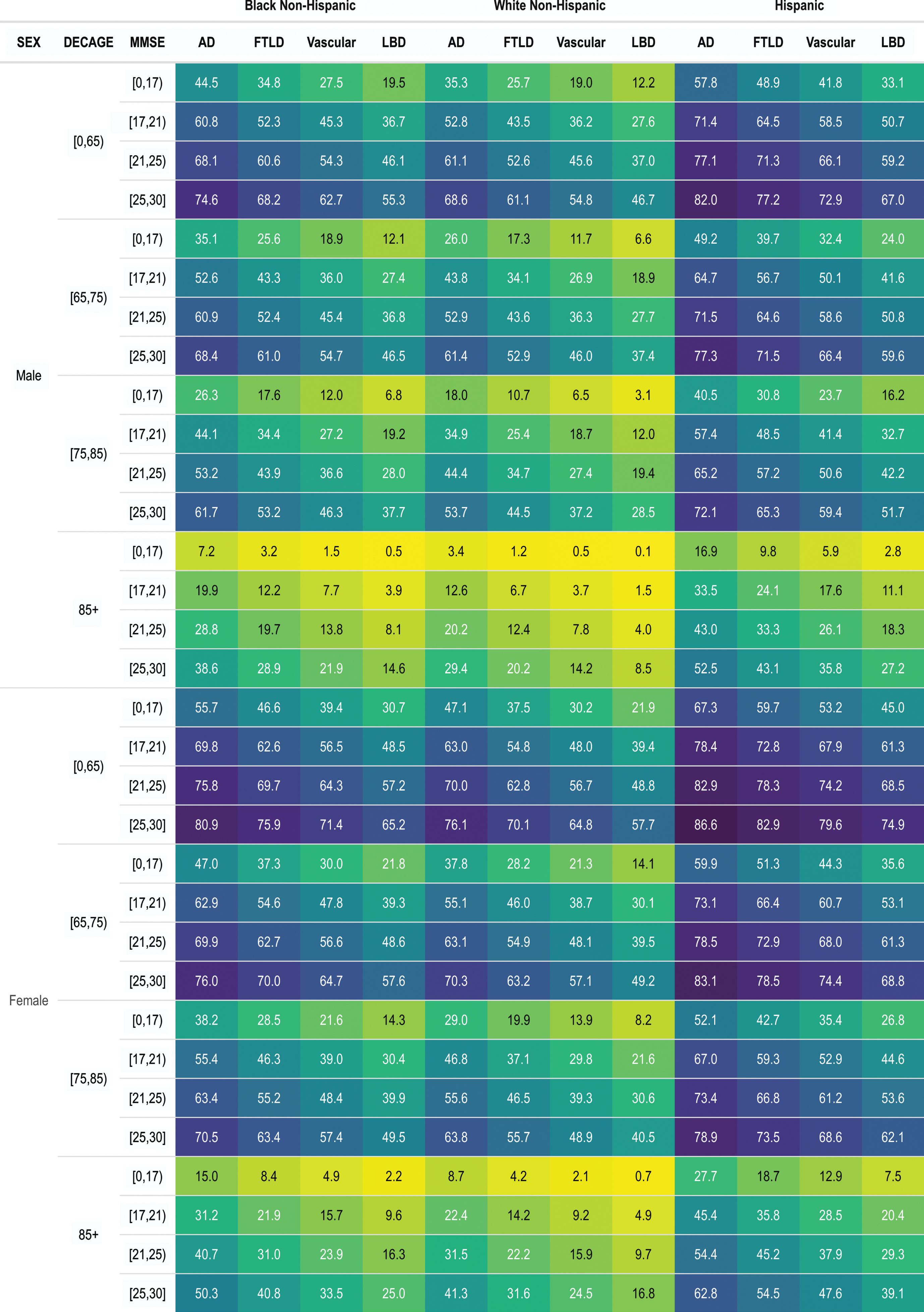
Probability of 5-Year Survival at Time of First NACC Visit with Dementia. N = 16,186 (male: 7,806, female: 8,380) reflects all participants from the full cohort (n = 17,784) who had all the data for the variables included in the models (1,598 participants were missing the Mini-Mental State Examination (MMSE). The bracket indicates that the value is included, and the parentheses indicates that the value is excluded (i.e., [0,17] is equivalent to the range of 0 to < 17).
Model performance
The optimism-corrected Harrell C-index was calculated to evaluate the models (Table 2) selected by LASSO for the full cohort and each dementia type (full cohort: 0.70, AD: 0.70, FTLD: 0.64, LBD: 0.70, vascular: 0.74). Typically, a Harrell C-index between 0.6 and 0.7 indicates a good model [31]. The calibration plots for our models also revealed strong agreement between obtained predicted and observed survival probabilities (Supplementary Figure 1). The C-index (both training and testing C-index) of the Cox model used for Fig. 2 was 0.68, also demonstrating a good model without overfitting.
DISCUSSION
Main findings
This study identified that individuals in NACC with AD had the longest survival after their first NACC visit with a diagnosis of dementia (median 6 years), followed by FTLD (5 years), and vascular dementia and LBD (each 4 years). In the total cohort, the strongest predictors of death during follow up were dementia type (higher risk with non-AD dementias), sex (higher risk with male sex), and race and ethnicity (lower risk with non-white races and with Hispanic ethnicity). Results in the total cohort were likely driven by the AD cohort given its much larger size compared to the other cohorts. In the FTLD, LBD, and vascular dementia cohorts, older age at symptom onset was associated with increased risk of death across diagnoses. Worse cognitive status (FTLD, LBD) and more depression (LBD) were also associated with an increased risk of death.
Survival time
Survival time in the current study was calculated from time at the first NACC visit with a dementia diagnosis, thus potentially underestimating survival for individuals with a pre-existing dementia diagnosis. Despite this, median survival time from the baseline dementia visit in this cohort (5 years, IQR 3–8) was similar to the estimated median survival time from dementia diagnosis in the recently published Swedish registry (median 4.8, IQR 2.6–7.6) [15]. The finding that non-AD dementias had a more rapid progression than AD is also consistent with Swedish registry findings [15] and a 2012 review [32]. There are multiple potential reasons for this, including differing progression rates between pathologies and the fact that there are often delays in diagnosing non-AD dementias.
When considering specific dementia diagnoses and survival, a meta-analysis of survival in FTLD phenotypes identified that survival was shortest in frontotemporal dementia-amyotrophic lateral sclerosis (FTD-ALS; mean 2.5 years) and longer in behavioral variant FTD (mean 8.17 years), compared to 6.86 years’ mean survival in AD dementia [33]. A more recent study reported median survival from FTLD symptom onset to death of 10.8 years [34]. The meta-analysis range is consistent with the survival of the FTLD cohort in the current analysis (median 5 years), which included multiple FTLD types. The median survival of individuals with dementia due to LBD in the current analysis (4 years) is also consistent with studies showing that individuals with clinically-diagnosed dementia with Lewy bodies live a median of 3–4 years after diagnosis [3, 35–37]. Prior research consistently shows shorter survival in both clinically-diagnosed and pathologically-confirmed dementia with Lewy bodies versus AD [38, 39]. Reported survival is also shorter in vascular dementia compared to AD, with median survival in vascular dementia ranging from 3.3 to 9.1 years [40–42], consistent with current findings.
Predictors of mortality
Apart from dementia type, the strongest predictors of death during follow up in the current analysis were male sex, white race, and non-Hispanic ethnicity. Male sex (and gender, though sex is more frequently assessed) tends to be a predictor of increased mortality/decreased survival in dementia studies [15, 43–45], though this is not fully consistent across studies [32, 44]. Many studies— largely performed in AD— suggest that white non-Hispanic race/ethnicity is associated with increased mortality versus African-American and Hispanic/Latino race/ethnicity, but this finding also has some inconsistency [44, 47].
Other predictors of mortality in the current analysis are consistent with prior studies, including age at onset [15, 48], worse cognition [15, 48], increased comorbidity burden [15, 48], using more medications [15, 45], and multiple dementia diagnoses [42, 49]. Few prior studies include residence as a variable, but the suggestion that requiring assisted living or skilled nursing care could signify a more severe dementia and increased morality has face validity. Additionally, this likely at least partly reflects impaired functional status, which was associated with increased mortality in prior studies [44, 45]. We could not assess this in the current study due to missing Functional Activities Questionnaire data. Results regarding an association between neuropsychiatric symptoms and mortality in dementia are inconsistent, but numerous studies suggest that the presence of neuropsychiatric symptoms (e.g., depression, psychosis) associate with increased mortality risk [38, 51]. Prior studies examining antipsychotic administration and mortality in dementia are mixed but generally supportive of increased mortality risk with antipsychotic use [36, 52]. Specific medication use, including antipsychotic administration, was not assessed in the current analysis.
In FTD, worse survival is associated with path-ogenic FTD mutations, certain phenotypes (e.g., early motor symptoms), age at onset, behavioral symptoms such as apathy and psychosis, and autonomic dysfunction [34, 53]. In vascular dementia, older age, male sex, worse baseline cognition, dementia temporally related to a stroke, strokes in bilateral gray matter structures, a family history of stroke, and absence of hypertension may be risk factors for mortality [40, 41]. Studies of mortality in LBD have generally mixed dementia with Lewy bodies and Parkinson’s disease dementia populations. In these populations, dementia at onset, older age, worse cog-nitive performance, fluctuating cognition, and hallucinations at onset associate with shorter survival [37, 49]. The current analysis was limited by sample size, but apart from older age at symptom onset (which was associated with higher mortality across groups), data suggested that worse cognitive function was associated higher mortality risk in FTD and LBD, as well as non-Hispanic ethnicity and depression in LBD. It is possible that the NPI-Q is not the ideal measure to assess for an association between neuropsychiatric symptoms and mortality in dementia given that it assesses 12 different behaviors as present or absent and mild, moderate, or severe [25]. Symptom-specific scales (e.g., for psychosis, apathy) could be more likely to identify an association, if present. Surprisingly, the only variable other than age that associated with mortality in vascular dementia was not living alone.
Model performance
One of the goals of the current analysis was to use the NACC cohort to investigate, replicate, and expand the prediction tables for 3-year survival in dementia developed from the Swedish Dementia Registry [15]. Despite using a U.S.-based co-hort and having additional variables, the current study found similar primary drivers of mortality in dementia–AD/ADRD type, age, sex, and MMSE score. This replication further supports these features as key predictors of dementia survival and mortality. The current analysis expanded on prior findings by incorporating variables relating to neuropsychiatric symptoms (NPI-Q, GDS), which were significantly associated with mortality in the AD, LBD, and total cohorts, though with hazard ratio point estimates near 1. Current findings also incorporate race and ethnicity into the survival tables, of particular relevance for U.S. clinics. Analysis of individual ADRDs was limited by sample size, however. Future research should use larger samples, potentially by combining cohorts, to develop similar risk tables using models specific to individual ADRDs where factors such as neuropsychiatric symptoms may play a particular role.
Study limitations
Strengths of the current analysis include use of a large dementia cohort available through NACC and analyses performed at the group level but also by AD/ADRD type. Use of NACC is also a limitation, however, as NACC is referral- and volunteer-based and does not reflect a population-based sample of the U.S. This affects generalizability to other U.S.-based populations and to individuals with dementia outside the U.S. The frequency with which ADRCs notify NACC regarding deaths and drop-outs varies, so caution is warranted when assessing death using NACC data. Prior research also suggests that ADRC enrollment-related factors may confound differences in progression in individuals with mild cognitive impairment identifying as non-Hispanic white or black [54]. It is possible that enrollment factors also affect other NACC analyses using race and ethnicity. NACC has missing and incomplete data and investigators and participants may take different approaches to some variables, such as age at symptom onset. Many of the associations had hazard ratio point estimates very close to 1, suggesting that these variables may play a limited role in mortality despite statistical significance. Despite these limitations, the findings of the current analysis are generally consistent with prior research, supporting that current findings can add to the literature regarding mortality in dementia.
Clinical implications and conclusions
Despite cited research regarding mortality and survival in dementias, individuals with dementia and dementia caregivers commonly report receiving insufficient guidance regarding what to expect, including relating to mortality and end of life [3–8, 55], with implications for end of life experiences [8, 55]. Based off a large database of Alzheimer’s Disease Center programs in the U.S., current results can help clinicians counsel individuals with dementia and their families regarding what to expect for average trajectories. Findings regarding individual risk factors (e.g., age, sex, MMSE score) can aid individualizing expectations. Study findings are particularly relevant for counseling individuals with dementia and their families at diagnosis and early in the disease course regarding what to expect for average survival and probability of 5-year survival. This can help individuals with dementia, families, and clinicians with long-term planning, including informed completion of advance directives. This study investigated predictors of mortality using assessments at the first dementia visit; further studies are needed to identify what changing variables over time may herald approaching end of life. However, better knowledge of average disease trajectories can alert clinicians regarding when they should be monitoring for palliative care needs and engaging palliative care and hospice services. Further research is needed to investigate drivers of mortality in AD/ADRDs, both to counsel individuals and families living with the different ADRD types and to identify factors (e.g., neuropsychiatric symptoms) that might be potentially modifiable.
Footnotes
ACKNOWLEDGMENTS
The NACC database is funded by NIA/NIH Grant U01 AG016976. NACC data are contributed by the NIA-funded ADRCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P50 AG005134 (PI Bradley Hyman, MD, PhD), P50 AG016574 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Thomas Wisniewski, MD), P30 AG013854 (PI Robert Vassar, PhD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennett, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P50 AG005131 (PI James Brewer, MD, PhD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russell Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG053760 (PI Henry Paulson, MD, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P30 AG049638 (PI Suzanne Craft, PhD), P50 AG005136 (PI Thomas Grabowski, MD), P50 AG033514 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD), P50 AG047270 (PI Stephen Strittmatter, MD, PhD). This study also used data from the Alzheimer’s Disease Genetic Consortium (NIA U01 AG032984). This project (M. Armstrong, Z. Li) also received support from NIA R01AG068128. Research support also occurred through the University of Florida Dorothy Mangurian Headquarters for Lewy Dementia and the Raymond E. Kassar Research Fund for Lewy Body Dementia.