
Abstract
Background:
Sleep appears to be a sensitive biomarker that facilitates early detection and effective intervention for Alzheimer’s disease, while subjective cognitive decline (SCD) is a risk factor for Alzheimer’s disease. Prefrontal cortex atrophy is associated with both sleep disruption and cognitive decline. Transcranial brain photobiomodulation (PBM) therapy can enhance frontal cortex oxygen consumption, increasing frontal cortex mediated memory function.
Objective:
This study aimed to test whether PBM therapy targeting the frontal cortex could improve sleep and cognitive function in SCD.
Methods:
Fifty-eight SCDs were divided into the PBM group (N = 32) in which real light therapy was administered and a sham light therapy group (N = 26). All the participants received either real light or sham light therapy for 6 days consecutively, while the sleep data were recorded. The n-back task was employed to measure each participant’s working memory.
Results:
We found no differences in sleep efficiency change (F = 211, p = 0.279), REM stage percent change (F = 420, p = 0.91), and wake-up time (F = 212, p = 0.277) between the two groups. The sleep efficiency and REM were improved within the true light group on the fifth day. The true light group perform better than the control group in the n-back test, the accuracy was higher in the 2-back test (88.6% versus 79.6%, p = 0.001), and the reaction time in 1-back was shorter (544.80±202.00 versus 592.87±222.05, p = 0.003).
Conclusion:
After five days of PBM therapy targeting the prefrontal cortex, sleep efficiency and N-back cognitive performance were improved on the fifth day.
INTRODUCTION
Alzheimer’s disease (AD) is the leading cause of dementia, which lasts for decades. It has been recognized that many treatments are likely to be more effective if given at the early stages [1]. Subjective cognitive decline (SCD) [2], which refers to an individual who perceives cognitive decline compared to the previous normal state subjectively while performing within the normal range in the objective neuropsychological tests, may be the earliest symptomatic manifestation of AD and it is associated with an increased risk of future cognitive decline and progression to AD [3–6]. Early detection and timely intervention for patients in the early stage may delay the onset of AD, reduce healthcare costs, and relieve socioeconomic burden [7, 8].
Sleep plays a critical role in memory consolidation, brain state refreshment, and brain plasticity regulation [9]. Sleep quality has been associated with objective cognitive performance in many studies, especially in the elderly population [10–14]. Specific sleep problems are significant risk factors for developing both mild cognitive impairment (MCI) and dementia, especially for AD [15–17]. Poor quality of sleep and severe daytime dysfunction are more prevalent in SCD [18]. Sleep problems are associated with complaints in all the cognitive subcategories of SCD [19–21]. Most sleep-related studies have focused on how sleep affects the cognitive function or aging effect on the connection between sleep and cognitive function [22–24]. Sleep problems co-existing cognitive complaints should be addressed timely [25, 26].
Given the irreversible nature of AD, there is an urgent need to identify modifiable risk factors to prevent or delay its onset. Sleep may present as a modifiable factor in the prevention of AD [27]. In particular, reduction in slow-wave activity (SWA), which is generated by the prefrontal cortex (PFC), and increased fragmentation are associated with memory impairment in the elderly [28–30], which have been identified as primary risk factors and potentially modifiable targets for neurodegenerative diseases. The PFC is relevant to memory encoding, particularly in encoding semantic information [28], and it is considered as an important mediator between SWA and encoding information [31, 32]. Several findings suggest that an excitatory stimulation pattern, particularly in the frontal lobe, may be effective for improving cognitive impairment [33, 34].
In the past twenty years, noninvasive sleep stimulation techniques such as transcranial electrical stimulation and transcranial magnetic stimulation (TMS) have emerged to enhance sleep quality [35]. Brain photobiomodulation (PBM) therapy using red to near-infrared (NIR) light is an innovative treatment for a wide range of neurological and psychological conditions such as stroke, Parkinson’s disease, brain trauma, depression, and insomnia [36–39].A few studies have investigated the use of NIR light as a form of neuromodulation for improving various cognitive domains in humans effectively [40–44]. However, those studies were limited by the small sample size and lack of objective outcome measures.
In summary, the effect of transcranial infrared laser stimulation through the forehead on sleep structure is an important research focus. However, there is no objective method to explore its effect. The purpose of this study was to explore the effect of short-term PBM treatment targeting PFC on sleep structure and cognition in SCD.
METHODS
Study design
A randomized double-blind, sham-controlled study was conducted at Xuanwu hospital in Beijing. This study consisted of three basic phases with an evaluation of eleven time periods: a) baseline sleep monitoring period of 1 day; b) a consecutive PBM 7 days treatment and sleep monitoring without weekend interruption; c) a follow-up period of 4 weeks with functional near infrared spectroscopy (fNIRS) and cognitive tests each week; d) to maintain blindness, participants were instructed not to communicate with other participants during their visits in any of the study phases.
Participants were randomly assigned to two groups in equal numbers, using the random number table generated by SPSS v23.0 before enrollment of the first participant.
Participants
We included 68 participants with SCD based on the inclusion and exclusion criteria below. The study protocol was approved by the central ethics committee at Xuanwu hospital. All participants provided written informed consent for research. The 68 SCD participants were randomly assigned to two groups, finally only 32 participants in the treatment group and 26 participants in the sham group completed the entire trial.
The inclusion criteria were as follows: 1) 50–79 years old, right-handed and Mandarin-speaking participants; 2) presence of self-perceived continuous cognitive decline compared with previous normal status and unrelated to an acute event; 3) concerns (worries) associated with memory complaint; and 4) failure to meet the criteria for MCI or dementia.
The exclusion criteria are as follows: 1) History of stroke or other neurological disorders that may influence the cognition; and 2) Current major psychiatric diagnoses such as severe depression and anxiety (Hamilton Anxiety Scale score greater than 14). Participants will not be excluded when mild or moderate symptoms of psychiatric disorders are suspected.
All participants and their informants will provide the following information: family history, vascular risk factors, occupation/retirement, socioeconomic status, cigarettes, alcohol use, and nutrition style. Additionally, the neuropsychological battery measures different cognitive domains including episodic memory (Auditory Verbal Learning Test-Hua Shan version, AVLT), language (Animal Fluency Test (AFT), 30-item Boston Naming Test (BNT), and speed/executive function (Shape Trail Test Parts A and B, STT-A and-B). The AVLT is a test of memory using the free recall of a list of 12 words. A higher score means recalling more words from the list and indicating better performance. BNT consists of 30 items to assess word retrieval and a higher score indicates better performance. The STT score is the total times taken to finish the test and the number of correct responses. A higher score indicates poorer performance. The Pittsburgh Sleep Quality Index (PSQI) containing a 19-item questionnaire was used to measure the subjective quality of sleep over the 4 weeks before. The PSQI distinguishes “poor” from “good” sleep by measuring seven areas: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleeping medication, and daytime dysfunction. Scoring was based on a 0–3 Likert scale and the sum of scores for these seven components yielded one total score ranging from 0 to 21. A score over 5 indicates poor sleep quality. Geriatric Depression Scale (GDS) is a 15-item self-reported questionnaire. In the analysis, GDS was used as a dichotomous variable, with a cut-off score of 6.
fNIRS
A wave near-infrared optical imaging system was used to measure the time course of oxyhemoglobin (HbO) and deoxyhemoglobin (HbR) concentrations at a rate of 25 Hz. The system includes 24 laser sources and 16 detectors, with each source including two wavelengths (690 and 830 nm) of near-infrared light. Sources and detectors were systematically positioned on the participant’s whole head, and the spatial separation between adjacent sources and detectors was set to be 2-3 cm. The configuration resulted in measurement channels that covered the cerebral cortex’s frontal, temporal, parietal, and occipital lobes.
Brain photobiomodulation
NIR is nonionized electromagnetic radiation, that penetrates through the skin and skull into brain tissues in an invisible way. The mechanism involves the stimulation of it can stimulate complex IV of the mitochondrial respiratory chain (cytochrome c oxidase), decrease the viscosity and density of a nanoscopic layer of H2O molecules surrounding cells and increase adenosine triphosphate (ATP) synthesis [45]. Moreover, light absorption by ion channels results in the release of Ca2 + and leads to the activation of transcription factors and gene expression [46]. Brain PBM therapy enhances the metabolic capacity of neurons and stimulates anti-inflammatory, anti-apoptotic, and antioxidant responses. It is hypothesized that a signaling cascade is also activated by promoting cellular plasticity neuroprotection and reducing amyloid plaque burden, p-Tau, oxidative stress, apoptosis, and clearance of amyloid-β [47, 48]. The PBM treatment consisted of applying light of a specific wavelength (1064 nm) which excited cytochrome oxidase, using a laser apparatus supplied by Changchun New Industries Optoelectronics Tech. Co. The laser received approval from Xuanwu hospital and a standard operating procedure for the laser was also approved. Both participants and experimenters wore protective eyewear, through the administrators of the PBM were careful not to shine the light on the eyes. Participants sat relaxed on a chair with their hands spread flat on the legs.
The power density was 250 MW/cm2, the laser treatment was continuous, not pulsed. The PBM treatment occurred in a locked room with black walls and no reflective surfaces. The experimenter ensured that protective eyewear was worn by all individuals [38].
The stimulation site was the PFC. The laser was directly illuminated to the frontal pole area of the cerebral cortex, which was considered as the most anterior area of the prefrontal cortex (Brodmann areas 9 and 10), About the 10–20 system used for EEG electrode placement, the forehead stimulation site was centered on the PF2 point [40]. The entire procedure lasts for 12 min each day for 6 continuous days [43].
The control group underwent the same procedure as the treatment group but received a transient treatment to intend site on the forehead, followed by 11 min of no treatment. The participants in the control group received 1/12 of the light energy density of the treatment group. Light stimulation also was taken each day for 6 continuous days.
Sleep monitor
Sleep structure was monitored by Sleepart, which is a wearable device that can be used at home to ensure that participants stay in the real daily sleep state. Sleepart uses an accelerometer to track sleep conditions. Based on the changes in sleep data including total sleep time (TST), total bedtime (TBT), proportion, and hours spent in REM (rapid eyes movement), non-REM (NREM), and sleep efficiency (TST/TBT×100%).
Participants were also given written instructions on how to use the Sleepart device. Metrics collected from the sleep art were TST (the actual sleep time without awaking), TBT (time spent in bed), sleep onset latency (SL), sleep efficiency (SE; the ratio between TST and TBT), proportion and hours spent in REM, NREM, and SWS, wakefulness after sleep onset (WASO), as well as daily RMS HRV. Those data were recorded every day. During the days of the test, participants were instructed to wear the Sleepart device at all nights.
The first night served as an adaptation to the instrument and to screen for incidental sleep disorders, and the first day’s data was used as the baseline for subsequent data. All participants were not allowed to use alcohol, or a daytime nap during the entire process of the study. Participants kept habitual sleep-wake rhythms as normal.
The actigraphy data were used to obtain estimates of sleep parameters, including Minutes of total sleep time, percent of sleep spent in N1, N2, N3, REM sleep, and WASO (min).
Working memory
The n-back task was employed to measure each participant’s working memory updating ability. The task involves a series of random Arabic numerals being displayed one by one. In this study, the participants were required to judge whether each number was the same as the one or two preceding numbers and respond by pressing a computer key (pressing “4” indicated that the numbers were the same and pressing nothing indicated that they were not). The intervals between stimuli were 1000 ms with a 500 ms delay, during which the participants were required to respond. The entire test consisted of 3 blocks. Working memory performance was assessed using the accuracy AAC (%) and reaction time (RT; ms).
Statistical analysis
Statistical analysis was performed with SPSS v23.0 software. A repeated measure ANOVA was used to analyze F scores among groups for comparison of baseline and follow-up data. Cohen’s d was reported as a statistical effect. We set the significance level at p < 0.05. The analysis made use of the open-source statistical programming language R and R studio (The R Foundation for Statistical Computing, Vienna, Austria Version 4.0.0). We calculated the difference between baseline data (first day) and follow-up data (2–6 days). N-back performance (ACC and RT) were analyzed using two independent sample t-tests and χ 2 tests to compare the continuous and categorical variables among groups, respectively.
RESULTS
Demographic and neuropsychological characteristics
There were no significant differences in gender, years of education, Hamilton Depression Rating Scale, Hamilton Anxiety Rating Scale, PSQI, and Montreal Cognitive Assessment-basic scores between the two groups. Detailed information is shown in Table 1. Table 1 shows the demographic and neuropsychological information of the treatment and control groups in detail. Overall, the comparison results were consistent with those in Table 1.
Demographic and neuropsychological assessments for all participants
Gender, Female/male; HAMA, Hamilton anxiety rating scale; HAMD, Hamilton depression rating scale; STT-A&B, Shape Trails Test A&B; AFT, Animal fluency test; BNT, Boston Naming Test; GDS, Geriatric Depression Scale; FAQ, Functional Activities Questionnaire; PSQI, Pittsburgh Sleep Quality Index; MoCA-B, Montreal Cognitive Assessment-basic; AVLT, Auditory Verbal Learning Test-HuaShan version.
Sleep quality
We first compared sleep quality between the true light and sham light groups. As shown in Fig. 1 and Supplementary Figures 1–3 repeated measures ANOVA revealed no significant effect of PBM on sleep efficiency (F = 211.18, p = 0.279), REM percentage (F = 420.53, p = 0.910), WASO (F = 212.29, p = 0.277), and deep sleep percentage (F = 179.82, p = 0.151).
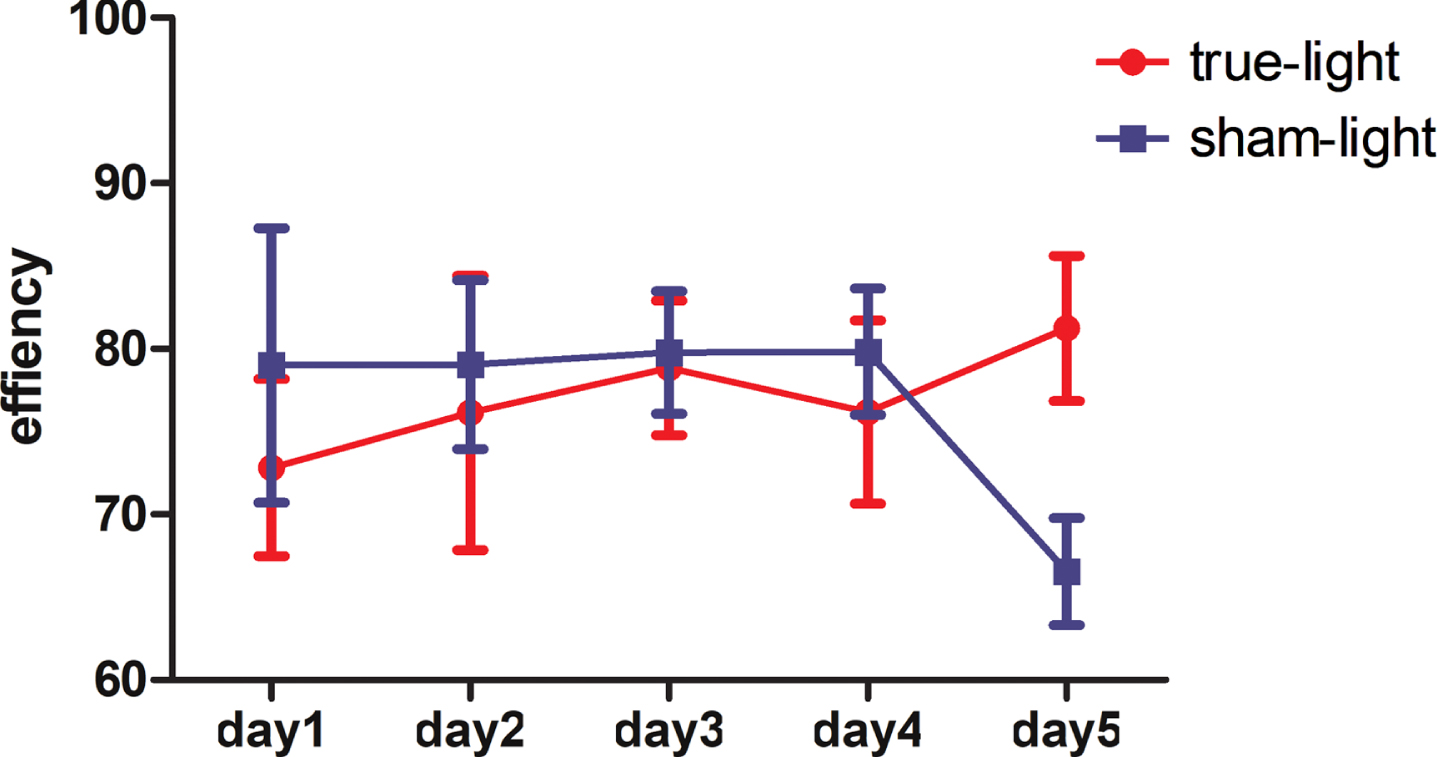
Repeated measure ANOVA modal revealed no significant effect of PBM for sleep efficiency between true-light and sham-light group (F = 211.18, p = 0.279). On the fifth day, there is a significant improvement in the true-light group.
However, compared to the sham light group, the sleep efficiency of the true light group on the fifth day was significantly higher (81.24±4.39% versus 66.54±3.24%, p < 0.001).
Within the treatment group, we defined the first day as the baseline and calculated the t value and Cohen’s d between 2–5 days and the first day. As shown in Table 2, compared to the baseline, deep sleep percentage (t = 0.30, p = 0.023) and REM percentage (t = 0.09, p = 0.016) showed significant improvement on the fifth day.
The sleep quality in the PBM process compared to the first day
Efficiency, the ratio between total sleep time and total bedtime; Deep sleep, deep sleep percentage in total sleep; REM%, REM stage percentage in total sleep time; WASO, wake after sleep onset; *p < 0.05.
Working memory
Secondly, we compared the working memory represented by the n-back test between the baseline and 6 continuous days after true light PBM. As shown in Supplementary Table 2, there was no improvement in the sham light group both RT and accuracy. Within the true light group, the accuracy of 2-back was significantly improved (83.6% versus 88.8%, χ2 = 5.161, p = 0.023) (Supplementary Table 1, Fig. 2). Meanwhile, the RT was shorter than the baseline, but without any statistical significance (Supplementary Table 2, Supplementary Figure 4). After 6 days PBM, the true light group perform better than the sham light group (Table 3 and Fig. 4), the accuracy was higher in 2-back test (88.6% versus 79.6%, χ2 = 10.788, p = 0.001), and the RT in 1-back was shorter (544.80±202.00 versus 592.87±222.05, t = –3.002, p = 0.003). Working memory improved effectively after 6 days of PBM, while sleep illustrated an improvement trend, especially on the fifth day. For all participants throughout the entire process of treatment, the PBM was well tolerated without any adverse events.

Within the true light group, after PBM treatment, RT was shorter than before (551.16±193.17 versus 544.80±202.00 in 1-back, p = 0.619; 745.68±309.29 versus 726.70±302.19 in 2-back, p = 0.360; 820.96±324.20 versus 834.33±335.31 in 3-back, p = 0.566), but not statistically significant.
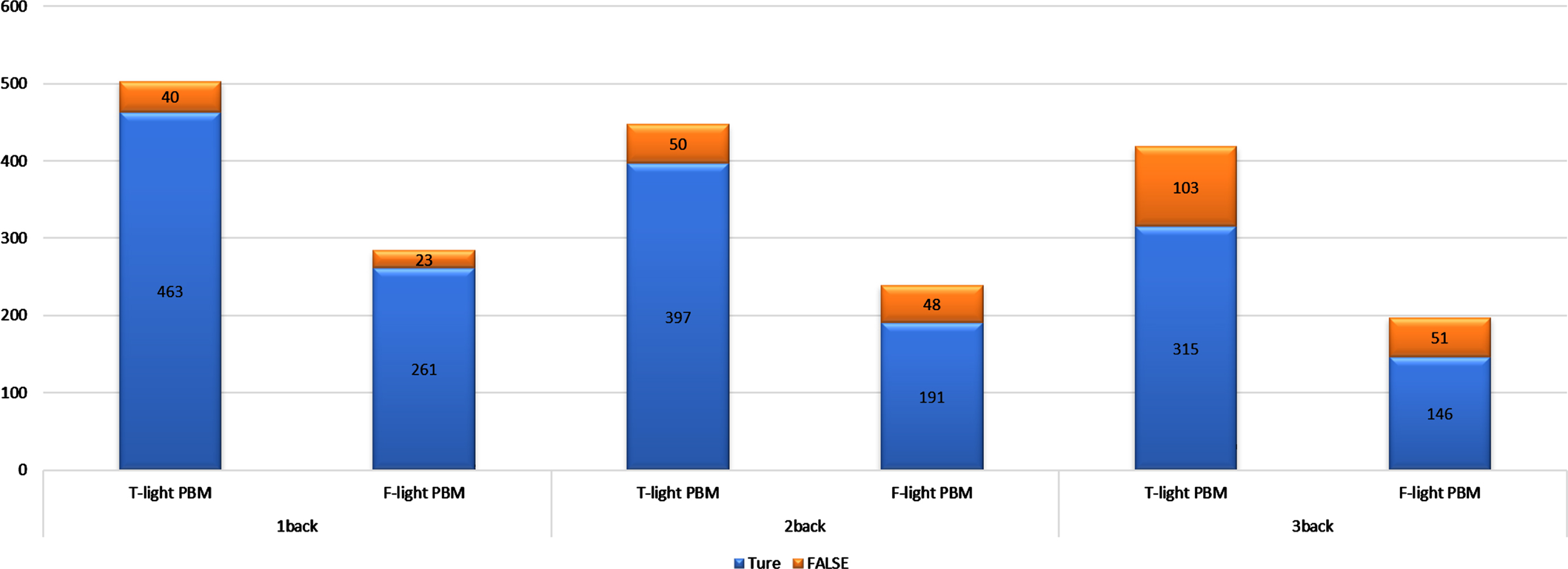
n-back accuracy between the true light group and sham light group. TRUE = times of press the correct number in the n-back test. FALSE = times of did not press the number in the n-back test. The treatment group was significantly higher than the sham group in 2-back (88.8% versus 79.6%, p = 0.001).
n-back test between true light intervention and sham light group
T-light baseline, before true light intervention; F-light PBM, one week after sham light PBM. Compared to the sham light group, the treatment group was more accurate and had shorter reaction times, but only 2-back ACC and 1-back RT were statistically significant. *p < 0.05; **p < 0.01.
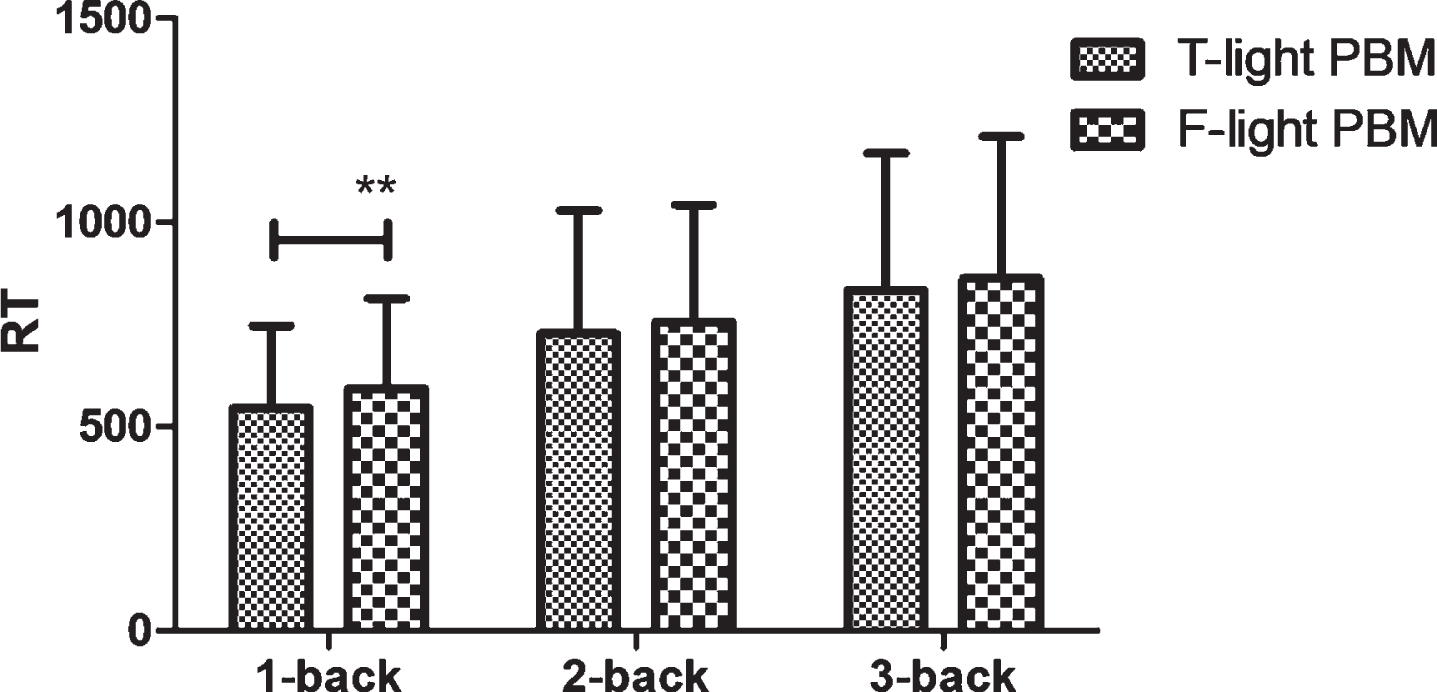
Compared to the sham light group, the treatment group had shorter reaction times in the 1-back test (544.80±202.00 versus 592.87±222.05, p = 0.003), **p < 0.01.
DISCUSSION
The study explored the effects of five-day consecutive PBM therapy targeting PFC on sleep situation and cognition in SCD elderly. The results indicated that deep sleep percentage and REM percentage showed significant improvement on the fifth day after the true light therapy. Compared to the sham light group, participants completing the true light therapy showed higher accuracy in the 2-back test and shorter RT in 1-back test.
There is no effect of improvement in sleep efficiency, REM percentage, or WASO contrast to the baseline within the treatment group. However, the sleep efficiency and the percentage of REM sleep on the fifth day were improved, which suggests that PBM has some subtle improvement in sleep quality in SCD participants. Lauriola and colleagues found that SCD participants suffered decreased sleep efficiency [7]. The medial prefrontal cortex is identified as the generator of NREM slow waves, the extent of atrophy is negatively correlated to the ability of NREM SWA generation [49]. Age-related reductions in SWA may be associated with impaired long-term memory retention and working memory in elderly individuals [29, 50]. PBM showed the effect of cognitive enhancement by improving cerebral oxygenation [50]. Branger and colleagues found a link between Aβ levels in prefrontal regions and the longer sleep latency [12]. PBM targeting PFC may affect sleep quality based on the mechanism described above.
Our results showed that the N-back accuracy rate was higher and N-back RT was significantly shorter than before, which is consistent with previous studies [38]. Several studies have found the interaction between sleep and cognition in AD. AD patients often experience different sleep disorders, such as decline in sleep quality. On the other hand, sleep disorders also accelerate the progression of dementia [24].
The interaction may be associated with Aβ accumulation, inflammation [51], and regulation of circadian rhythms [52–55].In our single-blind setting, we found that sleep quality and n-back performance were improved on the fifth day. In contrast to irreversible pathology in AD, sleep was presented as a modifiable factor, thus a potentially treatable target. Therapies targeting sleep offer several treatment possibilities [56, 57]. Previous studies have shown that NREM sleep enhancement could increase Aβ clearance, and enhance cellular restitution processes to alleviate oxidative stress, while NREM sleep could improve overnight hippocampus-dependent long-term memory consolidation [28, 49], which may efficaciously reduce AD risks [58]. Although the association between sleep and cognitive performance was not explored in this study, it could be a research point for future exploration.
In the future, large samples and long-term tests are still needed to further explore the effect of PBM and its mechanism. The present data suggest that we may need to employ optimal stimulation parameters and target position. Although positive effects only showed on the fifth day, this study still had strengths as follows: 1) SCD participants who are more likely to suffer sleep problems and developing to AD were chosen; 2) Rigorous research design that participants were randomly divided into treatment group and sham groups were set; 3) PBM therapy targeting PFC was a novel and effective intervention method based on prior studies. Our results may give us more information about dementia prevention in the future.
There are still some limitations in this experiment: 1) Positive effects were only shown on the fifth day, which indicated that the appropriate dosage and treatment duration of the PBM on sleep is still uncertain, and long-term studies are needed in the future; 2) Our study used wearable biosensor devices that may not be as accurate as gold standard PSG for evaluating SWS and REM sleep. However, many previous studies proved this technique is reliable and reproducible; 3) Aβ burden is associated with cognitive decline and sleep disorders [55, 59]. However, many participants could not provide Aβ information in our study. Whether PBM could influence the association between Aβ and sleep quality or cognition may serve us more information; 4) Sleep-related nucleus was observed in the suprachiasmatic nucleus [15], which is deep in the brain, maybe not suitable for PBM. We speculated that there may be some correlation between the frontal cortex and suprachiasmatic nucleus, which may need to be explored in the future.
Conclusion
After five days of PBM therapy targeting PFC, sleep efficiency and N-back cognitive performance were improved on the fifth day.
Footnotes
ACKNOWLEDGMENTS
This article was supported by the National Natural Science Foundation of China (Grant 61633018, 82020108013).
Colleagues of Xuanwu Hospital, Capital Medical University who have made contributions to build the SILCODE cohort are Yuxia Li, Jun Wang, Mingyan Zhao, Liu Yang, Yu Sun, Xuanyu Li, Guanqun Chen, Qin Yang, Can Sheng, Taoran Li, Jiachen Li, Xiaoqi Wang, Li Lin, and Yang Zhan.