
Abstract
Background:
Lutein (L), zeaxanthin (Z), and meso-zeaxanthin (MZ) are collectively called macular pigment. MZ can be converted from L in the macula. In the recent decade, many studies have been performed to investigate the effects for taking carotenoids, especially L and Z or L, Z, and MZ, as diet supplements on human health.
Objective:
We examined if diet supplements of L + Z or L + Z + MZ have effects on cognitive function in adults.
Methods:
A systemic literature search was performed in March 2021 with the following keywords: lutein, zeaxanthin, meso-zeaxanthin, cognition, cognitive, and macular pigment. The searched databases included Medline EBSCOhost, Scopus, Elsevier, Cochrane Library, ProQuest, and ClinicalTrials.gov. Findings from eight clinical trials were presented as the strongest evidence on the studied topic.
Results:
Most studies have found that macular pigments (L + Z) in blood or macula are positively correlated with cognitive performance. As an index of the amount of macular pigments in the brain, macular pigment optical density is related to cognitive performance in adults. In addition, there is an inverse relationship between a higher amount of macular pigment in the blood and lower risk of mild cognitive impairments or Alzheimer’s disease. Based on the findings from the clinical trials, diet supplements of L + Z or L + Z + MZ are associated with improved cognition in adults.
Conclusion:
The diet supplements of L + Z or L + Z+MZ are associated with better cognitive functioning, which may be via their beneficial effects on the vision.
INTRODUCTION
Lutein (L), zeaxanthin (Z), and meso-zeaxanthin (MZ) are three carotenoids existing in the human retina [1]. L, Z, and MZ are highly concentrated near the fovea, a small area in the center of the macula lutea of the retina [2]. These three carotenoids are collectively referred to as macular pigment [3–5]. From diet supplementation experiments performed in animal models, MZ can be converted from its precursor L in the macula [3, 6]. In addition, MZ is rarely found in the human diet although its presence has been confirmed in a few food resources [7–9]. Thus, some studies focused on the effects of L and Z while others investigated the effects of all three macular pigments L, Z, and MZ.
After their absorption into the blood circulation, L and Z ultimately reach and accumulate in the retina. The amount of retinal L, Z, and MZ can be indexed reliably by measuring macular pigment optical density (MPOD) [10, 11]. A heterochromatic flicker photometry is usually used to measure the MPOD [12]. The amount of macular pigment reflects their level in some brain regions but not others. For example, macular pigment (L, Z, and MZ) in the retina was significantly related to the combined concentrations of L and Z in the occipital cortex but not the hippocampus [4]. It is worthy to note that retinal L and MZ, but not Z, are significantly related to L in the occipital cortex [4]. In another study, MPOD was related to L concentration in the cerebellum, occipital cortex, pons, and frontal cortex [13]. Further, macular Z was related to its level in different brain regions [13]. In a cohort study of Centenarians, the amount of L and Z in the blood circulation was related to their levels in the brain as well [14].
In the recent decade, many studies have been performed to investigate the effects for taking carotenoids especially L and Z or L, Z, and MZ as diet supplements on human health. We are interested in knowing if these supplements have effects on cognition in the adult population. Our systematic review approached the topic by answering the following questions: 1) Is supplementing L and Z related to cognition?; 2) Is L and Z related to the risk of mild cognitive impairment (MCI) or Alzheimer’s disease (AD)?; 3) Could diet supplementation of L and Z improve cognition? An emphasis was placed on the evidence from double masked, randomized clinical trials with supplementing L + Z or L + Z+MZ as interventions for their effects on cognitive functions. At last, the possible underlying mechanism was discussed for the observed beneficial effects of macular pigment diet supplementation on cognition.
METHODS
A systemic literature search for relevant publications was performed during March 2021 using the following databases: Medline via PubMed (521 results); CINAHL Plus Full Text via EBSCOhost (89 results); Scopus (22 results); Embase via Elsevier (885 results); Cochrane Library (253 results); PsycINFO via ProQuest (36 results); and ClinicalTrials.gov (41 results).
Both keywords and database-specific controlled vocabulary terms were used in the search. The following search term combinations were used to find relevant literature: lutein and cognitive/cognition; zeaxanthin and cognitive/cognition; meso-zeaxanthin and cognitive/cognition; and macular pigment and cognitive/cognition. Exact search query translations for each of the databases are available upon request.
The following filters were applied for the literature search process: 1) reports written in English; 2) abstracts or full text articles available; 3) date range from 2006– 2021 (based on when the first RCT was conducted on this topic); 4) study design had to be randomized clinical trials; and 5) original research reports with adult humans only.
In total, 1,847 articles from all the databases were imported into Covidence for screening. Once imported into the Covidence, 271 duplicates were automatically removed. Then two primary reviewers screened the title and abstracts of the remaining 1,576 studies, and a third reviewer resolved any disagreements. Upon the first round of screening 1,497 studies were removed due to irrelevancy, with 79 studies assessed during the full-text stage. Of these, 71 studies were excluded due to: 9 had the wrong patient population (i.e., children instead of adults), 35 being the unmatched study design (specifically, they were not randomized controlled trials); 6 were irrelevant; 4 had wrong outcomes (e.g., cognition is not the outcome); and 3 were abstracts only. From this, eight randomized controlled trials were extracted for being presented as the strongest evidence. (See Fig. 1. A PRISMA 2020 flow chart was generated for the literature search process [15]).
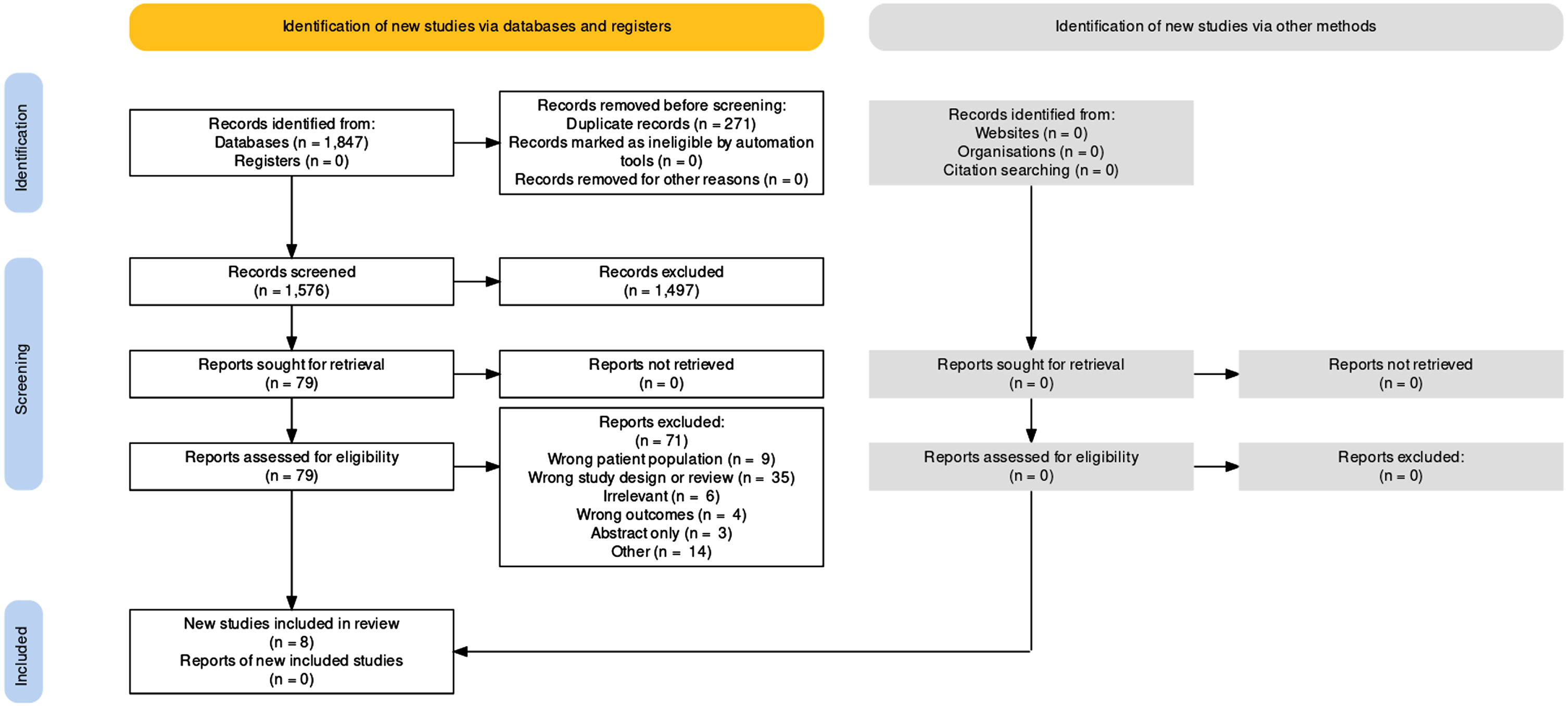
PRISMA flow chart of the literature search process.
If L and Z are related to cognitive functions?
Many studies on the effects of L and Z supplements [16–22] indicated that L and Z in serum or plasma were related to cognitive performance. Higher plasma L and Z were independently associated with better composite scores across the domains of global cognition, memory, and executive function [16]. In addition, higher plasma Z, but not L, was associated with better processing speed [16]. In another study, both serum L and Z concentrations correlated significantly with semantic (animal) fluency cognitive scores for participants with age-related macular degeneration (AMD), while serum L concentrations also correlated significantly with verbal recognition memory learning slope scores in the participants with early AMD [17]. One study showed that serum L was consistently associated with a wide range of cognitive measures including executive function, language, learning, and memory [18]. However, serum L was significantly related to cognition from a cohort study with octogenarians [18]. In addition, L level in the brain was associated with a range of cognitive measures in a group of centenarians [18].
The amount of macular pigment in the retina can be indexed effectively by the MPOD measurement. Significant correlations were found between MPOD and various measures of cognition [17]. For example, higher MPOD was significantly related to faster executive processes and better brief intellectual ability [19]. Higher MPOD was also significantly related to faster reaction time and better balance ability in the older adults [20]. Further, higher MPOD was significantly related to faster fixed and variable position reaction time, as well as coincidence anticipation errors, at high speed [20]. As expected, lower MPOD was associated with poorer performance on the Mini-Mental State Examination and the Montreal Cognitive Assessment [5].
Some studies investigated the relationship between both MPOD or plasma L + Z and cognitive performance. For instance, both higher MPOD and plasma L + Z concentrations were significantly associated with better cognitive performance [21]. Higher MPOD levels were significantly associated with better global cognition, verbal learning and fluency, recall, processing speed, and perceptual speed, whereas serum L + Z was significantly related to only verbal fluency [22].
If L and Z are related to the risk of MCI or AD?
MCI is a prodromal stage of dementia, in which the person has noticeable cognitive changes that does not affect ability to carry out daily activities [23]. By contrast, AD is the most common type of dementia [23]. There are some studies on the relationship between plasma levels of L and Z or MPOD and the risk of MCI or AD [24–28]. Plasma levels of L and Z and activities of antioxidants were similarly lower in MCI and AD patients as compared to healthy control participants [24]. Another study also found that serum levels of L and Z were significantly lower in patients with AD compared with cognitively intact controls [25]. Higher intake of L + Z was associated with substantially lower hazard of AD [26]. The amount of L + Z was inversely associated with AD diagnostic score, neuritic plaque severity, and neurofibrillary tangle density and severity [26]. On the other hand, AD patients were observed to exhibit significantly less macular pigment, lower serum concentrations of L and Z, poorer vision, and a higher occurrence of AMD when compared to healthy control participants [27]. Finally, a higher plasma L concentration was consistently significantly associated with a decreased risk of all-cause dementia and AD [28].
Could supplementation of L and Z improve cognition?
Corn and corn products were found to be major contributors of dietary Z whereas green leafy vegetables were rich sources of dietary L and Z [29, 30]. By contrast, egg yolk is a highly bioavailable source of both L and Z [31]. In a representative sample of the older United States (US) population, a high consumption of vegetables, fish and seafood, legumes, eggs, and fruit was associated with a higher intake of L + Z among older adults [32]. However, neither L nor Z were detected in either fish or seafood [33]. In eggs from the US, L + Z levels ranged from 1.0 to 1.6 mg/100 g per yolk, with L levels being 1.3– 1.6 times higher than that of Z [33]. In a study with the National Health and Nutrition Examination Survey 2003– 2004 data, dietary intake of L is consistently higher than Z despite of sex, age, and ethnicity in the US population [34]. Higher dietary intake of L and Z was associated with higher scores on the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) Word Learning sub-test, Animal Fluency test, and Digit Symbol Substitution test [35]. Unfortunately, fewer than 1 in 10 Americans meet their calorie-specific MyPyramid fruit or vegetable recommendations [36].
L and Z supplementation was able to significantly increase concentration of L in serum, prefrontal cortex, and cerebellum [37]. In addition, supplementation of L [38, 39] and Z [38] could increase their level in serum or macula of the eye. MPOD was directly related to dietary intake of L and Z but even more strongly to serum concentrations of them [40]. In two large cohort studies, consumption of vegetables was associated with slower rates of age-related cognitive decline [41, 42]. Even diet supplementation with L can increase cognitive function in adults [43].
Evidence from double masked, randomized clinical trials
It is worthy to note that one research group [12, 44– 47] did four double masked, randomized clinical trials with either young [12] or older [45–47] adults. The ratio between L and Z is 5:1 (10 mg L + 2 mg Z/day) for five studies [12, 45– 48]. Supplementation of L + Z was associated with increased MPOD [12, 45– 47] and their levels in the serum [12, 47]. Four trials found beneficial effects of the L + Z supplementation on cognitive performance with improvements on spatial memory (p < 0.04) [12], reasoning ability (p < 0.05) [12], complex attention (p < 0.04) [12], verbal learning (p < 0.05) [45], inter-network of default mode connectivity (p = 0.016) [46], complex attention (p < 0.02) [47], and cognitive flexibility (p < 0.02) [47].
For the Age-Related Eye Disease Study 2 (AREDS2), a double masked, randomized clinical trial was conducted with participants who were older adults and also at risk for developing AMD [48]. With a large sample size, the 5-year study did not observe any significant effects of L + Z supplementation on cognition [48]. Since cognitive function change was not the primary study aim for the AREDS2, the cognitive testing results were not controlled for different vision issues, which could explain the non-significant cognitive changes in the studied population.
There were two double masked, randomized clinical trials with supplementing L + Z + MZ in older adults [49, 50] and one in young adults [44]. For the two studies with older adults [49, 50], the L:MZ:Z ratio is 5:5:1 (10 mg: 10 mg: 2 mg/day). After supplementing L + Z + MZ for 6 months [50] or 1 year [48], the MPOD and serum level of L + Z + MZ were increased (Table 1). However, cognitive improvement in memory (p = 0.009) was seen in only one study with relatively large sample sizes with healthy adults (45.42±12.4 years old) for a supplementation duration of 12 months [49]. No cognitive benefits were observed in the other study with a shorter supplementation duration of 6 months and older adults (76±6.6 years old) (p > 0.05 for all measured cognitive function outcome variables) [50]. However, cognitive improvements including memory and attention (p < 0.05) were seen in the third study with a supplementation duration of 6 months and young adults (18– 25 years old) [44]. The ratio of L:MZ + Z supplementation was around 5:1 (22.33 mg:4.7 mg for group 1; 10.86 mg:2.27 mg for group 2).
Clinical trials on L, Z, and/or MZ supplementation on cognition
L, lutein; MPOD, macular pigment optical density; MZ, meso-zeaxanthin; Z, zeaxanthin.
Participants receiving the L/Z supplement had statistically significant increases in MPOD [12, 50], which suggest diet supplementation is an effective way to increase the macular pigment. The supplementation of L + Z can increase MPOD as well as their levels in the serum.
The potential underlying mechanism of beneficial effects of L + Z supplementation on cognition
Carotenoid intake was shown to have beneficial effects on cognitive performance [51]. The xanthophyll carotenoids L and Z function as both antioxidants and anti-inflammatory agents [52–54]. Their antioxidant and anti-inflammatory effects might reduce the cognitive burden, maintain the homeostasis of central nervous system, and help optimize the neurocognitive environment. Besides the antioxidant and anti-inflammatory effects, L and Z supplementation appears to benefit neurocognitive function by enhancing cerebral perfusion [45]. Using functional MRI, L and Z were found to significantly and negatively relate to blood-oxygen-level-dependent signal in different regions of the brain [55]. The brain needs a stable blood supply and uses a good portion of the cardiovascular output. The improved cerebral perfusion after L + Z supplementation is consistent with its beneficial effects on cognitive functions in older adults [55]. Supplementation of L and Z for one year had limited effects on structural brain outcomes overall [56]. However, serum L + Z and MOPD were related to white matter integrity, particularly in regions vulnerable to age-related decline [57]. Further, L and Z might also have a role in maintaining optimal auditory function [58]. On the cellular level, L has been shown to enhance gap junction communication [59]. The possible effects of L + Z supplementation on white matter integrity, gap junction communication, and auditory function might be through improving signal transduction and sensory input to central nervous system. Finally, the beneficial effects of L + Z or L + Z + MZ supplementation on cognition might be mediated by their effects of improving visual processing speed [60–63].

Potential underlying mechanisms for the macular pigment’s effects on cognition. L, lutein; Z, zeaxanthin; MZ, meso-zeaxanthin.
Based on results of the eight clinical trials, supplementing carotenoids L + Z or L + Z + MZ has shown beneficial effects on cognitive functions. After the beneficial effects of macular pigment supplementation are validated with a more powerful experimental design for a certain patient population, a specific plan can be made to make it available for those with a low measure of MPOD. For patients diagnosed with MCI, a timely intervention with macular pigment supplementation may be an effective way to improve cognition [64]. A recent clinical trial has shown the effectiveness of supplementation interventions in older adults for working memory improvement [65]. The main advantage of having macular pigment supplementation is that the MPOD can be improved in a relatively short period of time (3– 4 months). Second, the MPOD can be measured conveniently with devices. Third, it is more convenient and efficient with taking supplemental pills than getting the macular pigments from food resources [7– 9, 29– 34]. Lastly, the timing for starting the supplemental therapy can be decided based on the individual measure of MPOD, which is consistent with the concept of precision medicine.
Conclusion
Based on the available evidence, cognitive functions in adults are related to the amount of macular pigment in blood or retina, which is also inversely related to the risk of MCI or AD. More importantly, diet supplements of L + Z or L + Z+MZ is an effective way to improve cognitive functions, which the underlying mechanism may be related to the beneficial effects of macular pigments on vision.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $1,492,465 with 0% financed with non-governmental sources (Award number: 1D57HP40200-01-00). The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.