
Abstract
Background:
With increasingly aging societies, a comprehensive strategy for dementia research is important. The Organized Registration for the Assessment of dementia by the Nationwide General consortium toward Effective treatment (ORANGE) Registry is the first longitudinal multicenter prospective trial-ready cohort in Japan.
Objective:
To establish a large cohort for use in clinical trials and research in Japan.
Methods:
This registry, based on communities, hospitals, and nursing homes, covers three dementia stages (preclinical, mild cognitive impairment [MCI], and advanced dementia), and includes more than 30 hospitals. We analyzed enrollment and 1-year follow-up data for disease progression.
Results:
There were 1450 registered patients (649 men, 801 women; mean age, 77.92±6.70 years; mean Mini-Mental State Examination [MMSE] score, 25.19±2.76). The conversion rates from MCI to dementia and MCI to normal were 14.3% and 1.1%, respectively. High Clinical Dementia Rating score (odds ratio [OR] = 11.085, 95% confidence interval [CI]:1.619–75.913, p = 0.014), low MMSE score (OR = 0.835, 95% CI: 0.761–0.917, p < 0.001), high Geriatric Depression Scale score (OR = 1.093, 95% CI: 1.005–1.189, p = 0.038), and low body mass index (OR = 0.895, 95% CI: 0.829–0.967, p = 0.005) at enrollment were significant factors for conversion.
Conclusion:
The ORANGE MCI Registry is an established registry that facilitates creation of trial-ready cohorts to accelerate promotion of clinical trials with low reversion rates as it originates from a hospital. One-year follow-up analysis suggested assessing various factors for conversion risk. Further analyses will be possible in future with registry expansion. We will continue to refine this registry, including how it can be used more efficiently.
Keywords
INTRODUCTION
Dementia has become a prominent and growing challenge for health and social services globally [1]. The number of people with dementia is expected to increase to 75 million by 2030. The medical and care costs associated with dementia were estimated to be as large as 808 billion (USD) in 2015 [2]; the burden has worsened with the aging world population.
Japan is a rapidly aging country and could be a model for future super-aging societies [3]. In Japan, the prevalence of dementia was approximately 15% in 2020, which is higher than in many other countries [4] and is estimated to continue to rise [5]. Therefore, a comprehensive policy that could alleviate the increasing burden of dementia is necessary in Japan. In 2015, the Japanese Ministry of Welfare and Labor declared a new policy for dementia termed the “New Orange Plan.” The New Orange Plan covers several policies derived from the standpoint of persons with cognitive decline and their caregivers [6]. Following the New Orange Plan, in 2020, the Japanese government announced a new national dementia trunk strategy based on the following five pillars: (a) public awareness and communication support; (b) prevention; (c) medical care, nursing care services, and support for caregivers; (d) promotion of barrier-free dementia, support for people with juvenile dementia, and social participation; and (e) research and development, industrial promotion, and international development. Based on these five pillars, Japan aims to coexist with and prevent dementia.
With these national policies, a comprehensive research strategy for dementia is crucial. However, to date, the development of therapies, i.e., disease-modifying drugs, which is the main focus of research, has not been successful. For comprehensive research, recruitment and costs are major issues. To date, each study has been carried out with a new registry, resulting in a significant loss of time and cost-effectiveness because the registry for one study is not utilized for other studies. This has also led to delays in enrollment and remarkable costs. Clinical trials for people with mild cognitive impairment (MCI) and early Alzheimer’s disease (AD) in the preclinical phase require a so-called “clinical trial expressway” to enable large-scale and rapid enrollment of patients into clinical trials without a significant loss of time.
Considering the above background, Japan has not yet established a national registry, unlike many other countries. The Swedish Dementia Registry, for example, is intended to ascertain the nationwide medical situation and facilitate epidemiological studies on the progression course of dementia [7]. In contrast, in Japan, only community-based studies exist [8]. In addition, from the viewpoint of clinical studies, many countries have established registries in the past 10 years, which are mainly web-based registries for the purpose of recruitment to clinical trials [9–12], and some of them have formed panels across countries [13, 14]. These registries support many clinical tests at one time. For example, TrialMatch [10], which launched in 2010, reported that it has supported recruitments to 460 studies, and the Brain Health Registry [11] to 25 studies. In contrast, in Japan each facility recruits its own patients for each study.
Therefore, we aimed to establish a multicenter registry. This study is part of a nationwide clinical registry established in July 2015 in Japan called the ORANGE Registry (Organized Registration for the Assessment of dementia on Nationwide General consortium toward Effective treatment) [15]. The ORANGE Registry is a longitudinal multicenter prospective observational registry. As shown in Fig. 1, this registry covers the three stages of dementia progression as follows: preclinical stage [16], MCI stage [17, 18], and dementia care stage. A feature of this project is the inclusion of different dementia stages at recruitment. In particular, the preclinical stage is targeted in communities, the MCI stage in hospitals, and the dementia care stage in nursing homes.
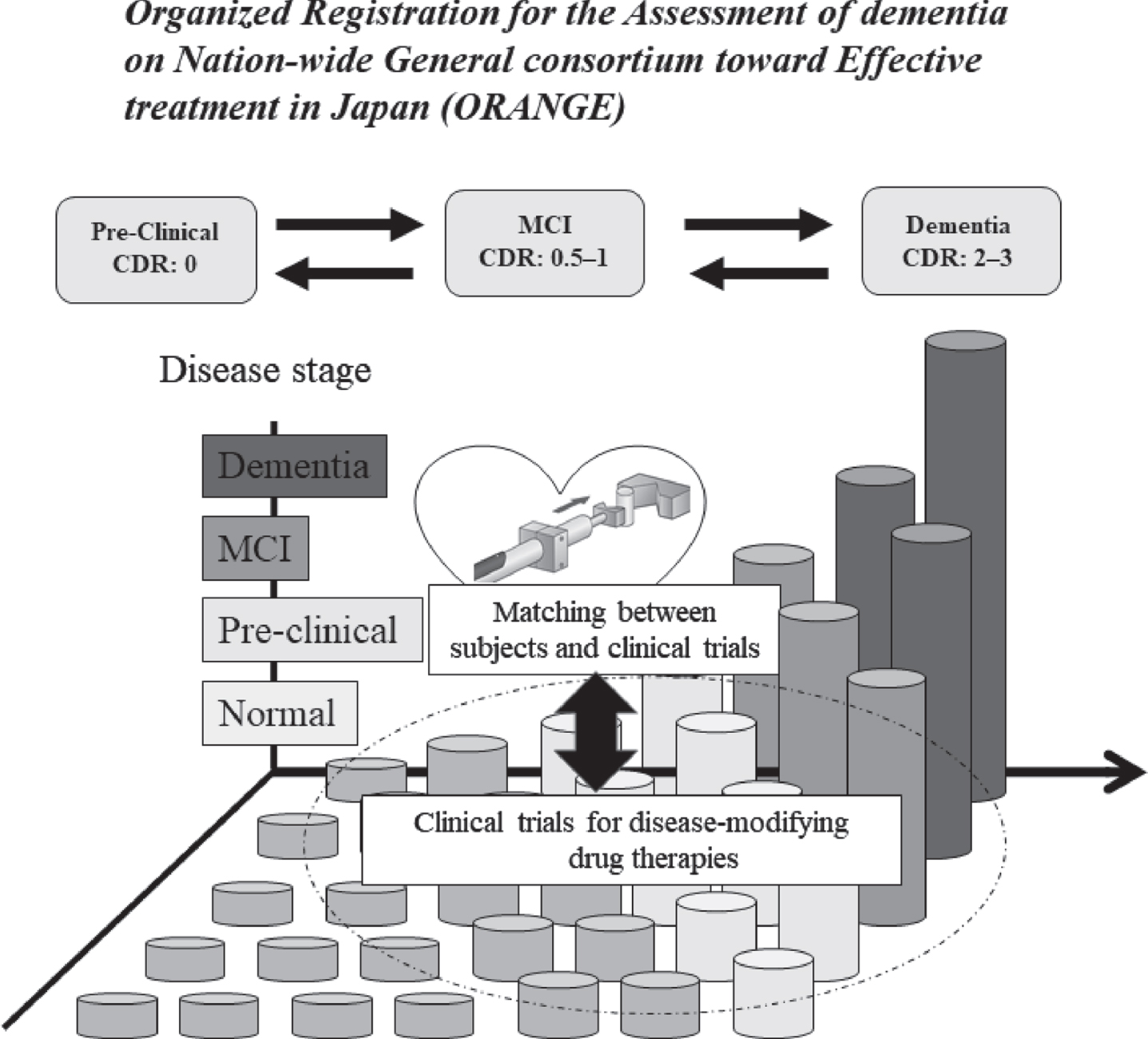
Scheme of the ORANGE Registry research [46].
This registry was developed for research and development for every stage of dementia, involving longitudinal work and collaboration with other researchers and cohorts to collect and combine evidence from multiple studies for the development of treatments and methods of care for patients with dementia. Furthermore, because this registration covers every stage of dementia, recruitment of participants based on their need for various studies is possible. Thus, this registry paves the way to accelerate clinical trials and research.
The MCI stage is the most important stage from the viewpoint of disease-modifying therapy and analysis of risk factors [19]. MCI is regarded as the most promising therapeutic target, and research is ongoing [20]. There is also a lack of analysis of the risk factors for conversion to dementia. Various factors, such as hypertension [21], diabetes [22, 23], smoking [24, 25], depression [26], and lack of exercise [27], may contribute to the progression of dementia. However, these factors have not yet reached a complete consensus. The analysis of conversion factors is also an important task in MCI studies. This study aimed to establish a large cohort for use in clinical trials and research in Japan using the ORANGE Registry. Furthermore, we will evaluate the quality of the MCI stage in the ORANGE Registry.
MATERIALS AND METHODS
ORANGE MCI registry
ORANGE MCI is the core stage among the three stages in the ORANGE Registry. The MCI stage is important for observing the progression to dementia and the development of disease-modifying drugs and recruitment to clinical trials. This registry is a dynamic registry that focuses on people with MCI and early dementia, and updates various data longitudinally. More than 30 medical centers across Japan participated in this study. All participating facilities are medical institutions specializing in dementia and all doctors, who diagnose and follow up in this registry, specialize in dementia. The diagnosis of MCI is based on the Petersen criteria [28] and the National Institute on Aging–Alzheimer’s Association [17]. The diagnosis of dementia and AD are based on the National Institute on Aging–Alzheimer’s Association [29]. Dementia with Lewy bodies (DLB) is defined as per the criteria specified in the International workshop criteria of the DLB Consortium [30]. The frontotemporal dementia criteria are also adopted to the Lund-Manchester criteria [31] and, depending on the symptoms, also uses the criteria of behavior variant [32] and verbal disturbance types [33]. The criteria for vascular dementia are based on the Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 criteria [34].
The main purpose of this registry is to rapidly recruit participants for clinical trials and research on disease-modifying drugs and other trials and analyze risk factors through continuous follow-up. The inclusion criteria for this registry were as follows: 1) age ≥40 years, 2) cognitive level: a Clinical Dementia Rating (CDR) [35, 36] score of 0.5 or 1 and Mini-Mental State Examination (MMSE) [37] score between 20 and 30, 3) a study partner in contact with the participant at least once a week who can monitor the living conditions of the participant. This registry aims to register a wide range of MCIs by creating more inclusive selection criteria. Registration of different types of MCI will allow the analyses of the natural history, risk factors, and enrollment in different studies. Furthermore, participant recruitment based on the clinical trial criteria can also be facilitated.
The obtained information for this registry consists of the following: (a) patient identifiers: sex, date of birth, education, and body mass index (BMI); (b) present diagnosis: type of dementia or MCI; (c) cognitive assessment results: MMSE, CDR, AD assessment scale [38], frontal assessment battery [39], and trail making test [40], with the first two mandatory and the others optional; (d) comprehensive functional assessment: Barthel Index [41], the Lawton Instrumental Activities of Daily Living (IADL) scale [42]; (e) mental evaluation including Geriatric Depression Scale (GDS) [43]; (f) core blood test (Yes/No); (g) structural neuro-imaging, e.g., computed tomography and magnetic resonance imaging (Yes/No); (h) functional neuroimaging, e.g., positron emission tomography and single-photon emission computed tomography; (i) comorbidities (e.g., diabetes, hypertension, hypercholesterolemia, and heart disease); (j) cerebrospinal fluid test (Yes/No); and (k) APOE gene (Yes/No).
Of the above endpoints, diagnosis, CDR, MMSE score, Barthel Index, and IADL must be evaluated once a year or every six months, if possible. In cases where a participant converts from MCI to dementia, follow-up is continued. The continuous collection of information will not only allow the analysis of the natural history and risk factors for dementia, but also facilitate early intervention after conversion to dementia. This continuous follow-up data also serve as a model for efficient referral to clinical trials and research as the present symptom will be easily identified.
Ethical approval
This study was approved by the Medical Ethics Committee of the National Center for Geriatrics and Gerontology (Obu, Japan) and all participating facilities (No. 883). This study was conducted in accordance with the principles set forth in the Helsinki Declaration. Informed consent was obtained from all study participants. Data were analyzed to preserve the anonymity of the participants.
Statistical analysis
Basic descriptive statistics were provided for population characteristics and are presented as the mean and standard deviation or count and percentage. Comparison of the no-dementia and dementia groups was performed using the Wilcoxon rank-sum test and the χ2 test. We examined the factors associated with the conversion to dementia using multivariable logistic regression, and the odds ratios (ORs) and 95% confidence intervals (CIs) were calculated after controlling for the following potential confounders: age, sex, education, MMSE, BMI, Barthel Index, IADL, GDS, and comorbidities (diabetes, hypertension, hypercholesterolemia, and heart disease). IADL was calculated as score/total score (men: 5, women: 8)×10 because the total scores for the men and women were different. All data management and statistical analyses were performed using the SPSS® Statistics software program, version 26.0 (IBM Corp., Armonk, NY, USA). p < 0.05 was considered statistically significant.
RESULTS
Quality of MCI registry
There were 211 people registered by 2016, 725 by 2017, 1,094 by 2018, 1,326 by 2019, and 1,450 by September 2021 (after exclusion of a total of 34 participants over the five years). Overall, 1450 participants were registered (men: 649; women: 801). The follow-up rate for one year was 63.7% (Fig. 2).
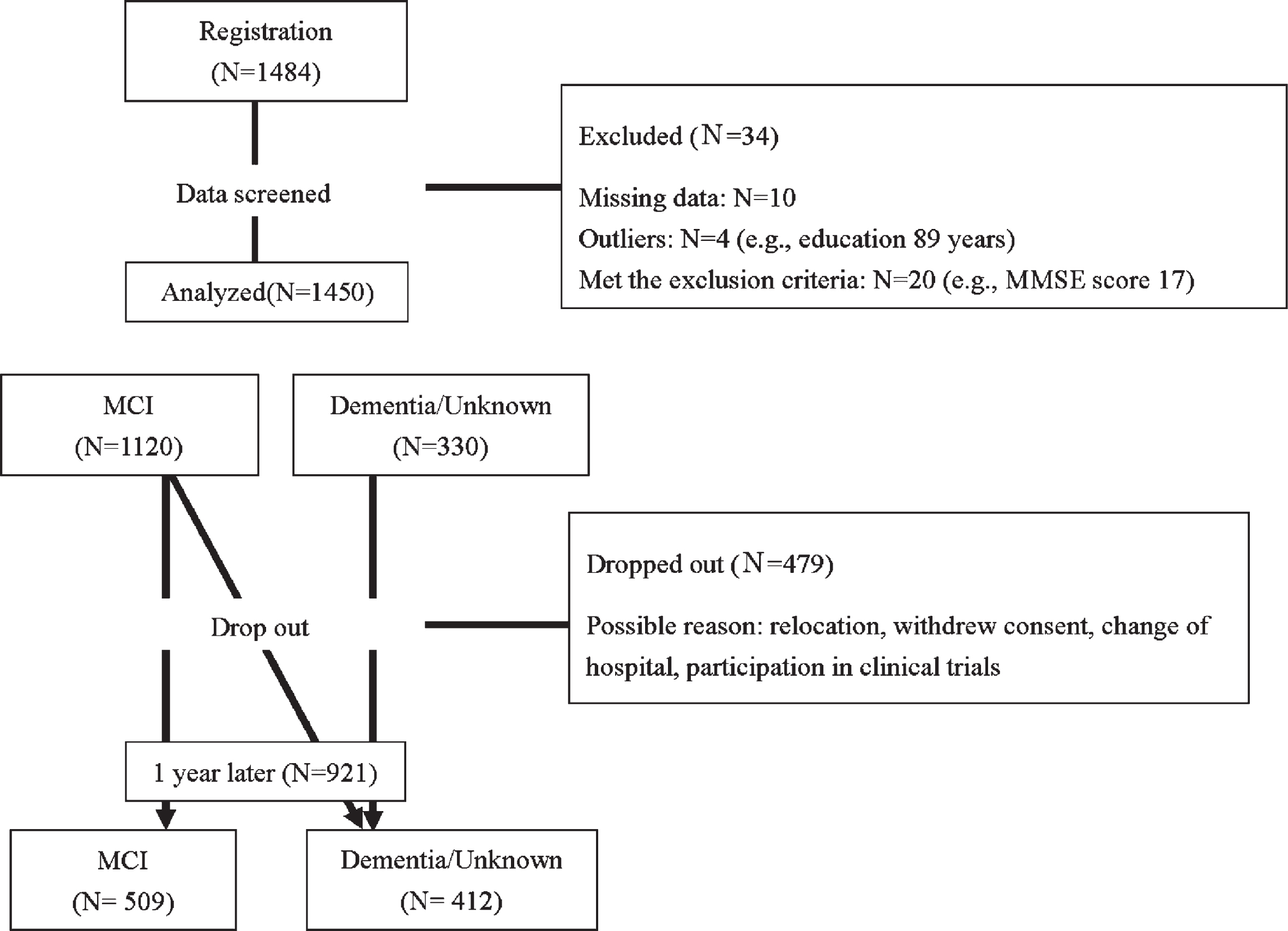
Study flow chart. MCI, mild cognitive impairment.
Registration data
The baseline characteristics of the registered participants are shown in Table 1. The mean age was 77.92±6.70 years (<60 years: 2.2%, 60–69 years: 7.0%, 70–79 years: 48.4%, ≥80 years: 42.4%). The mean MMSE score was 25.19±2.76 points. The breakdown of the MMSE scores is as follows: 29.0% for 20–23 points, 48.1% for 24–27 points, and 22.9% for 28–30 points. Among all participants, the CDRs were 0.5 and 1 in 90.6% and 9.4% of participants, respectively. MCI and dementia accounted for 77.3% and 21.0% of the registered diseases, respectively. Women tended to have a slightly lower education level and BMI than men, although this was not statistically significant. In contrast, diabetes and heart disease were more common complications in men.
Baseline demographic data (n = 1,450)
Data are presented as the mean±SD. BMI, body mass index; MMSE, Mini-Mental State Examination; CDR, The Clinical Dementia Rating; IADL, instrumental activities of daily living; GDS, Geriatric Depression Scale; MCI, mild cognitive impairment; SD, standard deviation.
Follow-up data after 1 year
A review of the 1-year assessment of participants who were enrolled with a diagnosis of MCI was conducted. Among participants diagnosed with MCI, the diagnosis of 509 (70.9%) patients remained unchanged, whereas that of 103 patients (14.3%) changed from MCI to dementia, and that of 8 (1.1%) changed from MCI to normal (Table 2). AD was the most common disease that progressed and converted to dementia (12.4%).
Change ratio in MCI at registration after 1 year (n = 718)
Data are presented as counts (%). MCI, mild cognitive impairment; AD, Alzheimer’s disease; DLB, dementia with Lewy body disease; FTLD, frontotemporal lobar degeneration; VaD, vascular dementia.
Data at the time of registration of dementia (converters and non-converters) were compared to analyze the risk factors for dementia (Table 3). Patients with stable cognitive conditions were considered non-converters and patients who exhibited progression to dementia were considered converters. Compared with the non-conversion group, the conversion group included older participants (p = 0.023) and more women (p = 0.032). The MMSE and CDR scores for the two groups were significantly different (p < 0.001). There was a significant difference in BMI and IADL between the two groups (BMI, non-conversion versus conversion: 22.85±3.42 versus 21.81±3.02, p = 0.005; IADL, 8.44±2.42 versus 7.75±2.52, p = 0.009). In contrast, the presence of comorbidities (diabetes, hypertension, hypercholesterolemia, and heart disease) showed no significant differences.
Comparison of data at enrollment and after 1 year stratified by converter type (n = 509)
MMSE, Mini-Mental State Examination; CDR, The Clinical Dementia Rating; BMI, body mass index; IADL, instrumental activities of daily living; GDS, Geriatric Depression Scale and p < 0.05 statistically significant.
Table 4 reports the results of the logistic regression for conversion to dementia. High CDR scores, low MMSE scores, BMI, and GDS scores were associated with dementia conversion (OR: 11.085, 95% CI: 1.619–75.913, p = 0.014; OR: 0.835, 95% CI: 0.761–0.917, p = 0.000; OR: 0.895, 95% CI: 0.829–0.967, p = 0.005; OR: 1.093, 95% CI: 1.005–1.189, p = 0.038, respectively). Other factors were not associated with a risk of conversion.
Odds ratios for conversion to dementia by baseline data
CI, confidence interval; MMSE, Mini-Mental State Examination; BMI, body mass index; IADL, instrumental activities of daily living; GDS, Geriatric Depression Scale and p < 0.05 statistically significant. aMale, code 0; female, code 1.
DISCUSSION
The ORANGE Registry is the first in Japan to provide longitudinal follow-up data for all stages of dementia linked to communities, hospitals, and care centers. Since its establishment in 2015, each of the three main registries, focused on the preclinical, MCI, and care stages, has accumulated data that is useful for various studies and clinical situations. Our present paper is the first report to summarize the Orange MCI Registry since its initiation in 2015.
Features of the MCI registry
Regarding the MCI registry, approximately 1500 cases have already been registered since 2015. One of the features of this registry is that it contains various clinical data. Therefore, it has been used to study the relationship between various systemic diseases and cognitive decline. A part of this MCI registry, which is one enrolled region in Japan, was used in a comparative observational study along with non-MCI subjects [44]. Furthermore, participants were already referred from ongoing studies. For example, “The Strawberry study: Strategy to obtain warfarin or direct oral anticoagulant’s benefit by evaluating registry” investigated the effect of oral anticoagulants on cerebrovascular diseases and cognitive impairment in patients with atrial fibrillation and patients with dementia [45]. Another study evaluated the relationship between dementia and gut microbiome-associated metabolites [46]. The registry plays an effective role in international clinical trials of disease-modifying drugs and can be used to recruit participants at the appropriate stage for each clinical trial. The slowness of recruitment in Japan compared with that in Europe and the United States is a pressing concern. When compared to the number of people registered in others databases, such as the Dutch Brain Research Registry [9], TrialMatch [10], Brain Health Registry [11], APR [12], and EPAD [13, 14], and the number in our registry, which uses a web system, is smaller. With the expansion of this registry, the efficient recruitment of participants using this registry can speed up corporate clinical trials in Japan.
Unlike other international registries, the main feature of this registry is that dementia-specialized facilities throughout Japan are enrolled. Some clinical trial registries are based on web-based registration and evaluation is done mainly at the time of registration; thus, there are many cases not eligible for clinical trials. Conversely, in this registry, evaluation of memory disturbance symptoms is conducted regularly by physicians, who diagnose and follow up every 6 months or 1 year and evaluate the current stage, such as conversion. This feature of our registry makes it possible to assess the current status of the participants more accurately and guide them to the appropriate clinical trial.
However, some cases are not entered into this registry due to possible selection bias at enrollment. Only the participants who go to the specialized hospitals are enrolled to the registry, which implies that those with poor healthcare access or with low socioeconomic status have limited opportunity to be registered. Nevertheless, the risk of selection bias might be lower because this registry has 30 participating facilities across Japan, which span almost the entire country for easy access, and with the universal health insurance system in Japan, it is relatively easy for the Japanese to visit specialized hospitals compared to other countries.
Analysis of the MCI registry
To promote referrals to various research in MCI, it is important to assess registry quality. In this study, we analyzed the currently available registry data. As approximately 90% of the patients had a CDR of 0.5, the registration is in line with the diagnostic criteria for MCI. In contrast, the variability of scores (20–23 points: 29.0%, 24–27 points: 48.1%, 28–30 points: 22.9%) for the MMSE stages suggests that a wide range of MCI diagnoses is registered. We believe that the breadth of the MMSE score represents the reality of MCI and can be widely used in research depending on the stage of MCI.
We found a 1-year conversion rate of 15%, which is similar to those in previous reports [47–49]. On the other hand, another feature is the reverse rate, where approximately 1% of healthy patients converted. This is extremely low compared with previous reports of 16–41% [47–49]. This difference can be attributed to the fact that previous studies used community-based cohorts. Because physicians perform diagnoses based on the results of detailed examinations, cognitive decline due to non-neurodegenerative diseases is often diagnosed before inclusion in the registry. Based on the rate of conversion and reversion, the ORANGE MCI Registry facilitates a more accurate diagnosis, as it accurately excludes temporary cognitive decline due to various factors, including psychiatric disorders or metabolic diseases. Therefore, this registry can efficiently recruit patients for clinical research and trials, as cognitive decline due to non-neurodegenerative diseases can be excluded and MCI leading to neurodegenerative diseases, such as AD, can be registered. Nevertheless, we have not been able to gather data on the reasons for dropout. A potential reason for the low re-conversion rate might be discontinuation of the visits due to an improvement in memory impairment. In addition, further influencing factors may include difficulty in continuing to take part in this registry due to relocation or death, sudden worsening of cognitive symptoms, or difficulty in attending due to other illnesses.
Therefore, we need to investigate the reasons for the dropout cases as a registry. Unlike regional- and country-based registries, this registry is for specialized hospitals only, which makes it difficult to track dropout cases. In the future, it will be necessary to track these cases in cooperation with the government and private clinics in the region.
In a registry that is evaluated and followed up by physicians, the analysis of conversion factors associated with longitudinal evaluation is also important. Previous observational studies identified various potentially modifiable risk factors for dementia, including lifestyle-related factors (e.g., physical activity and smoking), cardiovascular risk factors (e.g., midlife obesity, hypertension, diabetes, and hyperlipidemia), and psychological factors (e.g., depression) [50–52].
In our one-year analysis, we identified high CDR scores, low MMSE scores, low BMI, and high GDS score as risk factors for dementia conversion. High CDR scores and low MMSE scores are imaginable factors for conversion because an increase in the CDR score and a decline in the MMSE score directly indicate a decline in cognitive function. Regarding body weight, obesity in middle age has been reported to increase the risk of dementia, whereas it decreases the risk for those aged >65 years [53]. In this registry, only a few participants were obese based on their BMI (BMI >25). However, even within the normal range, the converted group tended to have a lower BMI than the non-converted group, suggesting that cognitive decline can occur even when it is not severely low. Additionally, based on the logistic regression model, BMI and depressive scores were significant factors, suggesting that a lower score could be a risk factor for conversion, even if the values are within the normal range. Like BMI, obesity in middle age is reported to be a risk factor for dementia [50, 51]. In contrast, in old age, a low BMI is reported to be a risk factor [54, 55].
Regarding the risk of conversion from MCI, it has also been reported that, even considering age and comorbidities, higher BMI was associated with a better cognitive performance [56]. The result of our study, evaluated by weight at enrollment, is consistent with these previous studies [54–56].
Low BMI indicates the importance of conducting regular physical assessment to determine dementia risk, and further detailed physical assessment, including muscle mass, walking ability, and weight change over time, is expected to lead to intervention and prevention of conversion. In addition, the relationship between the state of frailty, which leads to a decline in physical, mental, and cognitive function, has been clarified [57], and maintaining physical functions, including body weight, is considered an important aspect to maintain cognitive function. The importance of systemic management, such as exercise and nutrition, for maintaining body weight will play an important role in older adults for maintaining not only their health, but also their cognitive function. Furthermore, some reports suggested that the percentage of weight loss, rather than BMI values, is associated with dementia risk [58, 59]. Further data should be accumulated in the future to examine the relationship between weight loss and dementia and the effect of physical management on dementia prevention.
Depression has been reported as a risk factor for cognitive decline [60]. In this study, depression was only evaluated by GDS score; therefore, the study showed that only a small decrease in score could create a risk factor for conversion. Continuous assessment of cognitive function, as well as mental function, including depression, is considered to play an important role in the early detection of dementia.
In this analysis, comorbidities, such as diabetes, hypertension, hypercholesterolemia, and heart disease, were not identified as risk factors. Patients with hypertension, diabetes, and hyperlipidemia had a higher conversion rate from MCI [61]. In contrast, with treatment, the rate of cognitive decline slowed [62]. Because this study was conducted using a hospital-originated registry, appropriate treatment may be the reason comorbidities were not identified as risk factors. In the future, we will continue to evaluate the importance of the treatment of other diseases in maintaining cognitive function.
As a limitation, our analysis of risk factors is restricted to one year after enrollment. Although this can be comprehended as the one-year conversion risk, it is essential to accumulate more data. In the future, as data gets accumulated longitudinally, we will be able to further analyze the natural history and risk factors.
Future scope
As mentioned before, the unique feature of this registry is that it will cover all stages of dementia and lead to research as a trial-ready cohort (TRC) to conduct longitudinal observational studies and recruit eligible participants for various studies and research, including corporate clinical trials. The ORANGE Registry established Japan’s first multi-institutional nationwide registry to contribute to a TRC. This registry is expected to facilitate multicenter clinical studies effectively. As a result, it has already been used in several studies.
In a clinical trial, the confidentiality of participants is also crucial. The registry is anonymized; thus, not all personal information is available. At present, owing to the confidentiality of personal information, referrals to clinical studies and trials depend on each facility where the participants are registered. This situation leads to a delay in recruitment to various clinical studies and makes it difficult to share appropriate information with the enrolled participants. To address this limitation, we are working to develop a direct connection system (Clinical Trial Information Center in Dementia [63]) that will enable recruitment across institutions of each study when participants meet the eligibility criteria. This system will lead to an “expressway” for recruitment to clinical trials.
In addition, as with any registry, maintenance is an issue. To maintain the registry, it is necessary to increase the follow-up rate and the number of new registrants. Moreover, although the registry covers as many as 30 dementia-specialized facilities throughout Japan, cooperation among surrounding medical institutions and facilities is weak. As a result, as mentioned above, the reasons for dropout cannot be tracked in this registry. To improve the tracking rate and increase the number of new participants, it is necessary to establish a more well-connected nation-wide registry by adding private clinics and geriatric facilities, including nursing homes around the participating hospitals.
Overall, we established the ORANGE Registry, which covers the period from the pre-clinical stage to the dementia care stage, and aimed to use it in clinical trials and clinical research as a TRC. In terms of guiding clinical trials and clinical research, we were able to construct a high-quality MCI registry. In the future, it is important to promote a more effective use of registries in clinical trials and to accumulate longitudinal data, including analysis and intervention of conversion factors.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to all the family members included in the ORANGE Registry. The ORANGE study is supported by funds for Research and Development Grants for Longevity Science from the Japan Agency for Medical Research and Development (P15dk0207019 and JP20dk0207027).