
Abstract
Background:
Participants in Alzheimer’s disease (AD) prevention studies are generally required to enroll with a study partner; this requirement constitutes a barrier to enrollment for some otherwise interested individuals. Analysis of dyads enrolled in actual AD trials suggests that the study partner requirement shapes the population under study.
Objective:
To understand if individuals can identify someone to serve as their study partner and whether they would be willing to ask that individual.
Methods:
We conducted semi-structured interviews with cognitively unimpaired, English-speaking older adults who had previously expressed interest in AD research by signing up for a research registry. We also interviewed their likely study partners. Audio-recorded interviews were transcribed and coded in an iterative, team-based process guided by a content analysis approach.
Results:
We interviewed 60 potential research participants and 17 likely study partners. Most potential participants identified one or two individuals they would be willing to ask to serve as their study partner. Interviewees saw value in the study partner role but also understood it to entail burdens that could make participation as a study partner difficult. The role was seen as relatively more burdensome for individuals still in the workforce or with family responsibilities. Calls from the researcher to discuss the importance of the role and the possibility of virtual visits were identified as potential strategies for increasing study partner availability.
Conclusion:
Efforts to increase recruitment, particularly representative recruitment, of participants for AD prevention studies should reduce barriers to participation by thoughtfully designing the study partner role.
INTRODUCTION
Participant recruitment is a consistent challenge in Alzheimer’s disease (AD) research [1, 2]. AD trials typically enroll dyads comprised of a research participant and the participant’s study partner [3]. Study partners serve as knowledgeable informants, providing data about a participant’s cognition and function that is used both to establish the participant’s eligibility to enroll and to assess the value of the intervention under study. In AD trials that require participant-partner dyads, otherwise eligible individuals cannot enroll if they lack a study partner.
In prior research, the requirement to identify and secure a study partner numbered amongst the most important factors in a prospective participant’s decision to enroll in a hypothetical AD prevention study [4]. Analysis of dyads enrolled in actual AD prevention trials suggests that the study partner requirement in fact shapes the population under study [5, 6]. Yet, it has not been empirically examined to what extent these findings are because: prospective participants do not have anyone in their lives who satisfies the requirements of the study partner role; prospective participants are unwilling to ask anyone to serve as their study partner; or, if asked, others are not willing or not able to serve as the prospective participant’s study partner. Better understanding this should inform researchers’ efforts to overcome barriers to recruitment created by the study partner requirement.
Here, we report the results of the Study Partner Availability Limitations Study (PALS), an interview study of older adults who had previously signed up for either the University of California, Irvine Consent-to-Contact Registry (UCI C2C) or the University of Pennsylvania Brain Health Research Registry (Penn BHRR) [7]. Recruitment registries are structured opportunities for individuals to express preliminary interest in and grant permission to be contacted about studies for which they might be eligible. Such registries are increasingly used to improve recruitment for clinical research, particularly AD prevention studies [8–10]. Given that older individuals already enrolled in brain health-related registries like UCI C2C or Penn BHRR might be recruited for AD prevention studies, we sought to understand whether they would be able to identify—and willing to ask—someone to serve as their study partner in an AD prevention study. Moreover, we examined their perceptions—and their most likely study partners’ perceptions—of the study partner role’s benefits and burdens.
METHODS
Sampling and recruitment
PALS participants were English-speaking adults aged 60 to 85 who had previously registered with either UCI C2C or Penn BHRR and self-reported that they had not previously received a diagnosis of AD, mild cognitive impairment (MCI), or another neurological disorder. Eligibility criteria for PALS mirrored those for many AD prevention studies, which recruit cognitively unimpaired older adults. We sent recruitment emails to 110 individuals purposively sampled from the UCI C2C and Penn BHRR. The sampling strategy sought to achieve balance in gender and to oversample non-White race/ethnicity given the very high percentage of White participants in both registries. The participation rate was 54% for UCI C2C and 56% for Penn BHRR. Of those who did not participate, one was deemed ineligible, 10 declined due to being too busy or uninterested, and 39 were not interviewed because PALS had closed to enrollment after reaching the pre-planned sample size of 60 interviewees. See Fig. 1 for the recruitment flow.
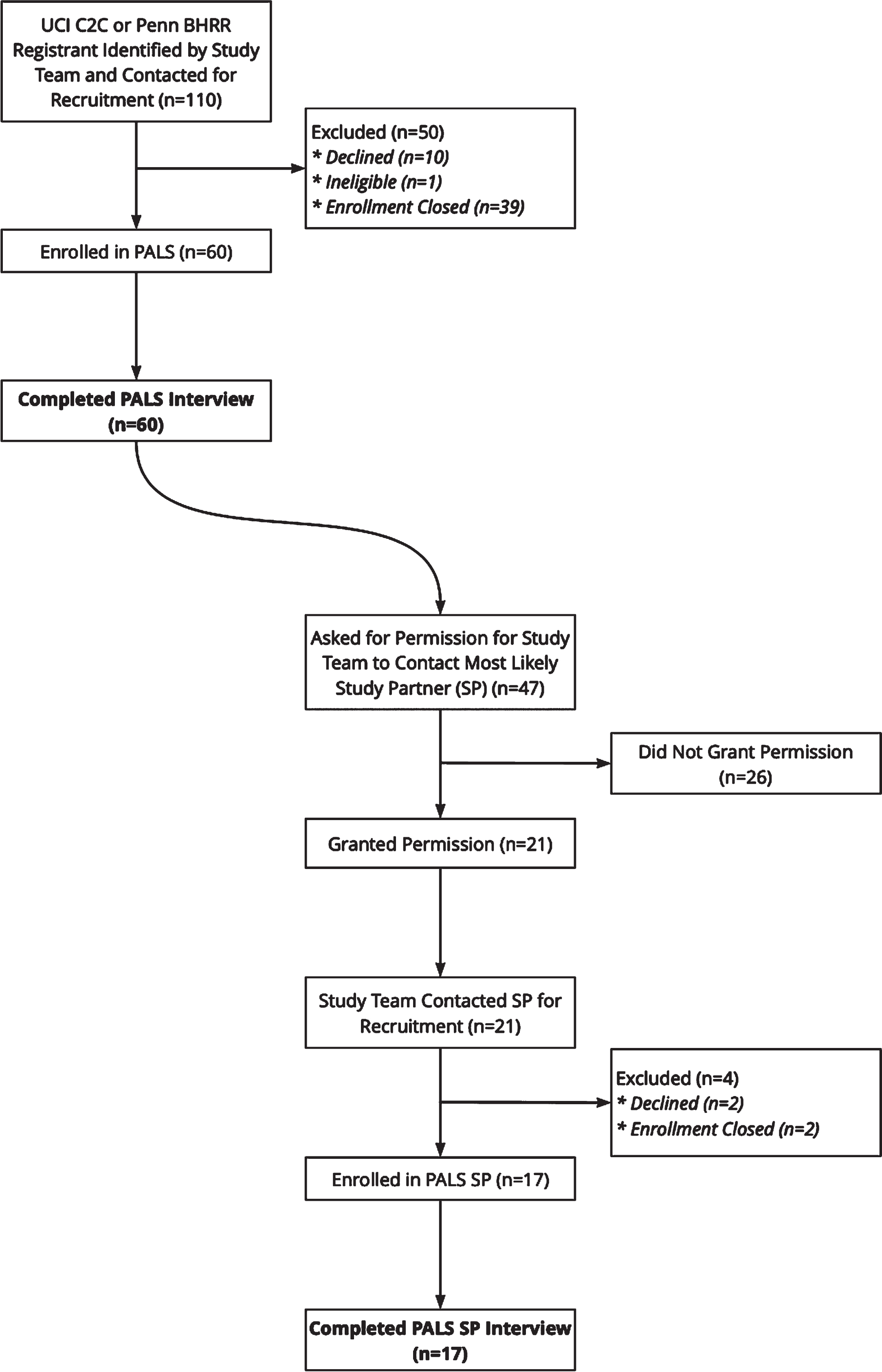
PALS recruitment flow. The study team recruited English-speaking older adults who self-reported that they had not previously received a diagnosis of Alzheimer’s disease, mild cognitive impairment, or another neurological disorder and who had previously registered with either the University of California, Irvine Consent-to-Contact Registry (UCI C2C) or the University of Pennsylvania Brain Health Research Registry (Penn BHRR). Most individuals who completed the PALS interview were asked for permission to contact the individual they had identified as most likely to be their study partner; some were not asked for permission because they had identified a spouse or significant other as their most likely study partner, and the study team sought variety in participant-study partner relationship types.
PALS participants were asked for permission to contact the individual they had identified as most likely to be their study partner; participants also had the option to share the research team’s contact information with their most likely study partner. Of the 47 PALS participants asked, 21 granted permission or agreed to share information about PALS with the individual most likely to serve as their study partner. Some PALS participants were not asked because they had identified a spouse or significant other as their most likely study partner, and we sought variety in participant-study partner relationships. Of the 21 likely study partners contacted, 2 declined to participate and 2 had not been reached when PALS enrollment closed. PALS participants who declined to provide permission or to share information about PALS with their likely study partner explained that the individual was too busy to participate in PALS, expressed a belief that the individual would not wish to participate, described a tumultuous relationship with the individual, or indicated they would not trouble the study partner if it was not a requirement of their participation in PALS.
Data collection
A research assistant (OSS) conducted interviews between August 2019 and May 2020; because interviews were telephonic, implementation of COVID-19 precautions did not affect this study. Semi-structured interview guides were developed by the multi-disciplinary research team following a review of literature and collection of pilot data. A study partner was defined for interviewees as someone who would “periodically attend research visits; have information about your memory, thinking, and daily function; and be someone you trust with personal information about your memory and thinking.” PALS participants completed a one-time interview examining five domains: (i) who, if anyone, was available to serve as their study partner, (ii) willingness to ask others to serve as their study partner; (iii) perceived burden of the study partner role; (iv) acceptability and perceived efficacy of proposed interventions to improve study partner engagement; and (v) demographics. Participants provided a self-report of race and ethnicity; these data were collected because AD is disproportionately more prevalent among Black and Hispanic older adults, but minority participation in AD research remains low [11]. Likely study partners completed a one-time interview examining similar domains, with a focus on their willingness to serve as a study partner. Interviews lasted 45 minutes on average.
Qualitative content analysis
Interviews were recorded and professionally transcribed. Data analysis began after interviews were complete. NVivo (QSR International) was used to manage coding. Analysis used a qualitative content analysis approach [12], which was chosen because our central goal was to inform AD researchers about the practical problems posed by the study partner requirement for research participation and to suggest interventions, not to generate an explanatory theory of these problems. The authorship team first annotated a subset of transcripts to identify pertinent themes, which were formalized into a codebook [13, 14]. Using this codebook, OSS, TB, and KH double coded a subset of 10 transcripts and assessed intercoder reliability. Coding differences were rectified through discussion, and the codebook was revised to capture missing themes, eliminate redundancies, and refine ambiguous thematic definitions. Using this refined codebook, the remaining transcripts were single coded by OSS or TB. Codebook revisions were applied to previously coded transcripts. As we found the codebook comprehensively captured interview themes once it had been revised after the round of double coding, we determined that we had reached code saturation—i.e., that performing additional interviews would not alter the codebook [15].
Human subjects’ protections
The University of Pennsylvania Institutional Review Board deemed PALS exempt. Interviewees gave verbal consent.
RESULTS
We interviewed 30 individuals from UCI C2C and 30 from Penn BHRR (“PALS participants”), as well as 17 likely study partners (Table 1). A majority of PALS participants were female (60%), and their average age was 72. Most were White (85%); 15% identified as Black or African American. Likely study partners were predominantly White (77%); more than half were the PALS participant’s spouse or significant other (59%).
Demographics
Research-related decision making
After hearing a description of a hypothetical AD prevention study “testing a new drug that may delay or prevent the onset of Alzheimer’s dementia in people who are at increased risk of developing Alzheimer’s dementia,” PALS participants were asked whom they would speak with if they were considering joining the study. Half (48%) indicated they would discuss participation with their spouse or significant other, a third (35%) with their adult children, and a quarter (27%) with friends. Several (15%) also mentioned consulting with their physician or the study staff. Four (7%) indicated they would keep their own counsel, saying “I think I could make that decision myself.”
While most PALS participants indicated that they would speak with others, the anticipated degree of others’ influence over research-related decision making could be divided into three general categories. Just over a third (38%) of PALS participants desired minimal involvement of others. One individual indicated that he “would certainly let them know, but the decision at this point would be mine.” Another third (32%) preferred an intermediate level of involvement, wherein others would “give me enough input that I could make an educated decision” but their opinions “wouldn’t be determinative.” Roughly one-in-five PALS participants (18%) sought to engage others—typically their spouse or significant other—in collaborative decision-making. For example, one individual stressed that he and his wife “don’t make unilateral decisions. If she was opposed to it . . . I would not do it.”
The individuals that participants indicated they would speak with if they were considering enrolling in a study were also, ultimately, the people they were most likely to ask to serve in the study partner role. For instance, the majority of PALS participants who were married or had a significant other indicated both that they were most likely to discuss participation with their spouse or significant other and also that this individual was their most likely study partner.
Willingness to ask others to serve as a study partner
All but three PALS participants (95%) indicated that they would “be willing” to ask someone to be their study partner if they wanted to join the hypothetical AD prevention study described above. The three participants who said they would not be willing to ask—two who identified as Black and one who identified as White—felt “that’s a lot to ask someone.”
Most participants (87%) indicated that their willingness extended to only “one or two people,” such as “my daughter” or “a couple of friends.” A typical quote comes from a man who explained, “I’d ask [my wife] at the drop of a hat. . . . I have some friends who if it were absolutely necessary, I might ask them, but I would feel uncomfortable.” No differences were observed by race or ethnicity in the overall number of people PALS participants were willing to ask to be their study partner.
Twenty percent of PALS participants exhibited ambivalence about asking someone to be their study partner. Though willing to ask, they indicated that asking “sure would be hard for me” or would require building up “courage to do it.” Several indicated they would “be very apologetic [and] . . . feel bad about” asking or “would hate to impose.” These individuals were more likely than others to suggest that the people they were willing to ask would not be able to serve as their study partner. One woman explained, “The only person that I would even consider would be my daughter... But she’s got her hands full.”
Most likely study partners
PALS participants were asked to identify the one individual who was most likely to be their study partner if they were to participate in an AD prevention study. Half (47%) identified a spouse or significant other, while a quarter (25%) identified an adult child; others identified a friend (18%), sibling (7%), or other family member (3%). Nearly all PALS participants who were married or had a significant other identified their spouse or significant other as their most likely study partner; White PALS participants were more likely than Black participants to be married or have a significant other and, thus, to identify a spouse or significant other as their most likely study partner.
More than three-quarters of PALS participants (79%) reported daily contact with their likely study partner. One individual joked that she communicates with her likely study partner, her husband, “every five minutes.” Others (20%) reported weekly communication. Only one PALS participant reported less than weekly contact with their likely study partner.
PALS participants were asked why they would select a particular person as their study partner, while likely study partners were asked why they would agree to serve as a study partner. Similar themes emerged across both groups (Table 2). More than two-thirds of PALS participants (67%) and likely study partners (71%) indicated that their relationship was characterized by “closeness” and “support that we just automatically give each other.” PALS participants (65%) and their likely study partners (82%) also identified traits—such as being “detail-oriented” or “understand[ing] the value of research”—that made the likely study partner well-suited for the role. Roughly half of PALS participants (47%) and their likely study partners (53%) spoke to logistical considerations—typically, that the likely study partner was “retired” and therefore “available” or that geographical proximity (e.g., to the PALS participant or to the study site) minimized “inconvenience.”
Reasons for identifying a particular study partner, reasons for agreeing to be a study partner
*Interviewees could identify more than one reason.
Benefits of the study partner role
PALS participants and their likely study partners identified potential benefits associated with the study partner role (Table 3). Nearly all PALS participants (82%) and their likely study partners (94%) indicated that the study partner could promote research integrity. Both groups viewed the study partner as an “objective observer” who could ensure researchers received “unbiased” information. They felt study partners could promote adherence to study procedures—for instance, seeing if “the medication was taken properly”—or monitor participants between study visits.
Perceived benefits of the study partner role
*Interviewees could identify more than one benefit.
PALS participants (78%) and their likely study partners (82%) identified an important role for study partners in providing logistical and “emotional support” during a study. Some PALS participants (25%) and their likely study partners (24%) felt study partners would be better positioned to support the research participant even after study completion because study partners could “be more attuned” and have insights into cognitive “difficulties we might face in our future.” More than half (57%) of PALS participants and a third of their likely study partners (35%) believed study partners would experience positive emotions by supporting the research participant and “doing very important work” contributing to AD research.
Barriers to and burdens of being a study partner
A fifth (22%) of PALS participants described the study partner role as burdensome, while a third (35%) said it was not. The largest proportion (43%) felt burdensomeness should be assessed in light of other demands on the study partner. For example, several explained that “a retiree would probably be the best kind of study partner” because retirees have fewer demands on their time; this was contrasted with individuals who “don’t have a lot of time after work” or who “have young families.” Single PALS participants were more likely than partnered participants to view the role as burdensome (29% versus 14%).
The likely study partners we interviewed—two thirds (65%) of whom were retired—generally did not view the study partner role as burdensome. While 82% did not “view it as a burden whatsoever,” the remainder felt it would be somewhat burdensome, but “a burden that I would welcome.” Several individuals identified potential burdens such as the “emotional demand” of the role or expressed “reservations about [the PALS participant] being on an experimental medication.” A handful also discussed the time commitment (12%) and the burden of travelling (12%), especially into the city of Philadelphia, where Penn’s urban campus is located.
Interventions to increase study partner availability
PALS participants and their likely study partners were provided with a list of interventions and asked which would be useful for increasing prospective study partners’ availability and willingness to serve in that role. These interventions included: researchers calling prospective study partners to discuss the research; providing free transportation to/from study visits; giving study partners a choice of completing study visits in-person or by telephone or video chat; scheduling study visits on nights or weekends; allowing multiple people to share the study partner role; and offering study partners a modest payment for completing study visits.
More than half (58%) of PALS participants and most (88%) of their likely study partners felt that a call with a researcher would be beneficial, as speaking with researchers allows prospective study partners to “hear firsthand exactly what they would be expecting of me” and makes a study seem “a little bit more legitimate.” One PALS participant speculated that “if you could get a professional to explain to them how important it [the study partner role] is, that might make a difference.” By contrast, individuals who indicated that a call would not be helpful said that speaking with the researcher would not address the true obstacle to participation, which is often “time constraints” rather than skepticism about “the value and the purpose” of the research.
While most (83%) PALS participants anticipated that conducting research visits by telephone or video chat would be helpful, fewer (59%) of their likely study partners were drawn to this option. Study partners speculated that virtual visits would “be an hour” compared to “half a day” for an in-person visit, but some indicated they would still “prefer it more in person.” Just under half (46%) of PALS participants and only 2 likely study partners indicated that visits on weekends or in the evening would be helpful to them.
PALS participants recruited from Penn BHRR and their likely study partners were more likely than those associated with UCI C2C to indicate that a free Lyft or Uber to the study site would or might make a difference. A third (33%) of PALS participants and half (47%) of their likely study partners favored offering payment to study partners as compensation for their time and effort, noting that “everyone loves money. Money’s good.” And just under half of PALS Participants (47%) and their likely study partners (47%) expressed interest in the possibility of sharing the study partner role amongst multiple individuals.
Additional suggestions provided by interviewees included providing “snacks, coffee, [and] good magazines while I wait,” conducting the research at a “closer location,” or providing “free parking.” Others said they would value “an occasional update on how the research is going.”
DISCUSSION
PALS was an interview study of cognitively unimpaired older adults who had previously indicated their willingness to be recruited for AD research by signing up for a brain health-related registry. In AD prevention trials, standard practice is to require participants to enroll with a study partner who provides data about participant cognition and function. The study partner requirement is understood to be a barrier to research participation [4, 16]. Nearly all PALS participants indicated that they would be able to identify and would be willing to ask a potential study partner to participate in AD research with them.
Most PALS participants indicated that they would talk with others when deciding whether to participate in an AD prevention study. In prior studies of MCI patients and their study partners, dyads reported that they would decide in partnership whether to enroll in a clinical trial [17]. Caregivers of persons with symptomatic disease have described a caregiver-led, albeit collaborative, approach to research decision-making [18]. The fact that PALS participants were cognitively unimpaired and thus able to be self-directed, as well as the fact that there was no caregiver, may explain these different approaches to research-related decision making. Notably, PALS participants were most likely to talk about research participation with the person whom they ultimately identified as their likely study partner; yet, a majority of participants indicated that, while they would solicit this individual’s input, the decision to participate in research would ultimately be their own. For prospective participants, the decision to participate in an AD prevention study appears distinct from the decision to ask someone to be a study partner; once asked, study partners must then decide if they want to serve as a study partner. This sequential decision-making is not as evident in studies of symptomatic disease, where the participant and study partner appear to make these three key decisions jointly and nearly simultaneously. This multi-step process may complicate recruitment for AD prevention studies.
In studies of symptomatic AD, many study partners are individuals who are already serving as the participant’s caregiver and, thus, are already involved in the participant’s medical care and health-related decision making. In AD prevention studies, prospective participants are cognitively unimpaired; they do not have caregivers who naturally step into the study partner role. Nevertheless, all PALS participants could identify one or more individuals in their lives who could plausibly serve as their study partner. Study partners must be familiar with participants’ personal and medical situation [3]. Based on PALS participants’ reported frequency of contact with their likely study partners—daily to weekly—the individuals identified appear to satisfy requirements set out for study partners in prior studies [5]. Moreover, PALS participants and their likely study partners appreciated and underscored the importance of the study partner’s role in assuring high quality data and evinced commitment to scientific integrity. Both PALS participants and their likely study partners considered personal characteristics like interest in research, insight into the participant, and attention to detail as important in a study partner.
Nearly all PALS participants expressed willingness to ask someone to serve as their study partner if they wished to participate in an AD study that required it. This willingness, however, generally extended to only one or two people close to the PALS participant, suggesting that people are selective about involving others in research. This may reflect the stigma of AD and reluctance to share AD-related health information beyond a small circle of others [19, 20]. It also seems to reflect a desire not to impose on or burden others, as evidenced, for example, by weighing logistical considerations when choosing whom to ask.
It is encouraging that most PALS participants were able to identify several people they would be willing to ask, and who are likely qualified for the study partner role. Yet, if these select individuals cannot or will not serve as a study partner, the study partner requirement will quickly become a barrier to participation, as there is not a “deep bench” of potential study partners. In fact, some PALS participants expressed concern that those individuals they were willing to ask would be unwilling or unable to serve in that role, suggesting that despite their stated openness to participating in AD research (e.g., as evidenced by signing up for a registry), they would not ultimately be able to participate if recruited for a study requiring a study partner. Difficulty recruiting individuals for the PALS study partner interviews is indicative of how this challenge may play out: many participants declined to give permission to our study team to contact their most likely study partner and to recruit them for this study. They indicated that their most likely study partner was too busy to participate or would not wish to participate in this interview study. Having a study partner was not an eligibility criterion for PALS, but had it been, our sample would likely have been smaller or more difficult to recruit.
Half of PALS participants identified a spouse or significant other as their most likely study partner, while a quarter identified an adult child. In actual AD trials, as many as two-thirds of participants enroll with a spouse or significant other, whereas only a quarter enroll with an adult child. This is striking, as individuals without a spouse or significant other comprise the majority of the population of potential older adult research participants [2, 21]. Though we have a small number of Black PALS participants, our results are consistent with prior research finding that minority participants who enroll in research are more likely to enroll with a non-spousal study partner [22, 23]. This observation may be explained, in part, by the racial gap in marriage [24]. Though we did not look at retention in this study, analyses of actual AD trials suggest that participants who enroll with a spousal study partner may be less likely to drop out [22, 25]. Overrepresentation of spousal study partners in recruitment and retention might be explained, in part, by the fact that PALS participants viewed the study partner role as more burdensome—and therefore less feasible—for individuals, like adult children, shouldering work and family responsibilities than for spouses, who tended to be retired.
Our results suggest, consistent with past studies, that structural barriers exist to the participation of some individuals as study partners and that this contributes to the lack of representativeness in AD research [6, 11]. To promote equity and inclusion, greater efforts are needed to address these barriers [5]. Such efforts should include questioning the study partner role itself and asking whether alternative study designs or research modalities can meet the need for information about cognition and function underlying the study partner requirement [6]. There is mixed evidence on whether cognitively unimpaired research participants or their study partners provide more accurate reports; this evidence may reflect differences in accuracy by cognitive domain and also differences due to study partner characteristics (e.g., relationship to participant) [26–29]. Considered together, these results suggest that study partners may be more important for study integrity in longer trials. Thus, depending on the goals and design of a particular trial, participant reports may be prioritized. Study partners in AD prevention studies do not generally need to perform the same range of tasks they do in studies of symptomatic disease, which may further minimize the need for a study partner [30]. To the extent that study partners are, however, necessary for the goals of a particular trial, it is important to design studies thoughtfully, and PALS offers preliminary ideas to this end.
PALS participants and their study partners agreed that a promising strategy to reduce barriers to enrollment was direct contact between researchers and potential study partners to discuss the nature of the study and the importance of the study partner role. We hypothesize that this outreach and education may be more important in the context of AD prevention studies than in studies of symptomatic disease, as the prospective participant in an AD prevention study does not yet have clinically measurable cognitive impairment and is not functionally impaired. This may make research participation appear less urgent and, perhaps less beneficial, from the perspective of the prospective study partner; meanwhile, the burdens of participation (e.g., taking time out of a busy schedule to drive to a study site for visits) are clear. Outreach and education may help to motivate study partners under these circumstances. Further, the emphasis on recruitment of the study partner speaks to the ways, discussed above, in which AD prevention studies are not recruiting dyads to participate in research so much as they are recruiting two distinct individuals who subsequently participate in research as a dyad.
PALS participants and their study partners also identified conducting study visits by telephone or video chat as a viable strategy for increasing enrollment in AD prevention studies. Fortunately, this would be logistically and financially feasible in the setting of AD prevention studies. Moreover, this should not undermine scientific rigor, as evidence suggests it is possible to carry out accurate and reliable remote assessments [31]. PALS interviews were largely conducted before the onset of the COVID-19 pandemic increased the frequency of remote clinical and research visits. With greater familiarity, individuals may feel even more favorable about phone and video data collection now than they did at the time of the interviews. Further, researchers’ abilities to administer assessments remotely should also be more advanced now, given a multitude of learning opportunities during the pandemic.
Some likely study partners expressed interest in being reimbursed for research-related expenses, like parking, and in being compensated for the time and effort expended on the study partner role. Offers of payment would be ethically appropriate given the importance of and work entailed by the study partner role [32, 33]. Moreover, payment could help overcome known financial barriers to research participation, such as transportation costs and lost wages [34]. In oncology, payment has been shown to increase the socioeconomic diversity of research participants [35]. This would be beneficial in AD prevention studies, as many participants come from higher socioeconomic strata—another dimension along which there is a lack of representativeness in AD research.
Consistent with prior research with persons with dementia and their caregivers, PALS participants and their likely study partners indicated that driving to the study site can be a barrier to research participation [18, 36]. We saw differences in the perceived value of transportation to the study site, such as an Uber or Lyft, between participants recruited from UCI C2C and from Penn BHRR. This may be because Penn BHRR participants were more likely to identify driving to Penn’s large, urban campus for study visits—and the gnarly Philadelphia traffic—as a burden of the study partner role, whereas UCI C2C participants were relatively less likely to discuss the challenges of driving to UCI. This difference in perceived ease of driving to the study site is an example of why efforts to promote prospective study partners’ willingness and availability to participate in research should be study- and site-specific. It highlights the importance of designing outreach and recruitment efforts in collaboration with patient advisors or community members, who can provide insights into potential barriers and facilitators [37].
Limitations
Our study has several limitations that must be noted when considering our findings. First, the sample was drawn from the research registries of two academic medical centers. The purposive sampling method used to recruit subjects could lead to selection bias. We interviewed a limited number of likely study partners. Many PALS participants indicated that their likely study partner would be unwilling or unable to complete this brief one-time interview—a less burdensome task than being a study partner in an AD prevention study. This raises questions about whether these individuals would, in fact, be available or willing to serve as study partners in an actual AD prevention study. Our findings are likely to be biased in favor of lower perceived burdensomeness of the study partner role.
CONCLUSIONS
The requirement that participants enroll in AD prevention studies with a study partner is scientifically and ethically important but can also constitute a barrier to research participation even for those who want to participate [38]. Thus, efforts to improve recruitment—and particularly to increase representativeness—must focus not just on participants but also on their likely study partners. This entails acknowledging the value of study partners’ contributions and designing the study—for example, through virtual visits—in a way that makes participation feasible for more individuals.
Footnotes
ACKNOWLEDGMENTS
This research was supported in part by the Institute for Translational Medicine and Therapeutics of the Perelman School of Medicine at the University of Pennsylvania and the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR001878. This research was supported in part by the National Institute on Aging (P30-AG-010124 and P30-AG-072979). Dr. Largent is supported by the National Institute on Aging (NIA) (K01-AG064123) and a Greenwall Faculty Scholar Award. Dr. Grill is supported by NIA P30 AG066519, NIA U24 AG057437, and NCATS UL1 TR001414. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.