
Abstract
Alzheimer’s disease (AD) is a devastating illness in elderly individuals, that currently has no known cure. Causal genetic factors only account for 1-2% of AD patients. However, other causal factors are still unknown for a majority of AD patients. Currently, multiple factors are implicated in late-onset AD, including unhealthy diet, physical inactivity, traumatic brain injury, chronic conditions, epigenetic factors, and environmental exposures. Although clinical symptoms of dementia are common to all races and ethnic groups, conditions that lead to dementia are different in terms of lifestyle, genetic profile, and socio-economic conditions. Increasing evidence also suggests that some elderly individuals age without cognitive impairments in their 60–90s as seen in rural West Texas, while some individuals progress with chronic conditions and cognitive impairments into their 60s. To understand these discriminations, we assessed current literature on demographic features of health in rural West Texas. This paper also outlines our initiated clinical study with a purpose of understanding the factors that allow some individuals to live without cognitive impairments at the age of 60–90 years, whereas others develop deficits in cognitive function around or above 60 years. Our ongoing study hopes to determine the factors that delay aging in some individuals by investigating various aspects including genetics, epigenetics, ethnicity, biology, culture, and lifestyle. This will be achieved by gathering information about participants’ ethnographic profiles, cognitive assessments, blood-profiles, brain scans, and blood-based genomic analyses in relation to lifestyle. The outcomes of our study will provide insights into healthy aging in rural West Texas.
INTRODUCTION
Dementia is an increasing worldwide phenomenon that is only projected to become more severe as majority of the population globally, including the United States (US), continues to age. The impact is substantial as every 3 seconds a new case of dementia is diagnosed around the world. In 2018, 50 million people were living with dementia and this number is expected to increase to 152 million by 2050. This translates into a worldwide cost of US$1 trillion in 2018 and with the increase in prevalence the cost is estimated to reach US$ 2 trillion by 2030 [1]. As the most common form of dementia, Alzheimer’s disease (AD) plays a significant role in these daunting numbers and with no current drug or therapeutic agent that may restore and/or prevent AD in elderly individuals.
AD is associated with the loss of synapses, synaptic dysfunction, mitochondrial structural and functional abnormalities, microRNA deregulation, inflammatory responses, neuronal loss, and accumulation of amyloid-β (Aβ) and phosphorylated tau (p-tau) [2–14]. Despite the progress that has been made in better understanding the pathogenesis of AD, we still do not have any early detectable markers, drugs, or agents that can prevent or slow the progression of AD.
Ethnic and/or racial factors may play a large role in addition to lifestyle conditions in developing dementia in elderly individuals, particularly in rural West Texas populations. There are disparities within the population as some individuals age 60 to 90 progress through their later stages of life without any sign of cognitive impairments. On the other hand, some elderly individuals develop chronic conditions and dementia around 60 years of age or even earlier. The causal factors behind these discriminations are largely unknown. To determine the reasons for these differences, we recently initiated a large-scale human study to collect data and assess the factors that lead to cognitively healthy individuals as well as the factors that lead to cognitive impairment in some elderly individuals.
The purpose of our article is to assess dementia and AD in rural West Texas, as well as outline a current clinical trial protocol that is being executed at the Texas Tech University Health Sciences Center in Lubbock, TX. This study aims to evaluate the biological, environmental, and sociodemographic factors that may impact the cognitive health of individuals age 60 and above in rural West Texas.
WHAT IS DEMENTIA?
Dementia is an overarching term for a decline in cognition that is severe enough to interfere with day-to-day life and independent function [15]. It is best to regard dementia as a syndrome or a group of symptoms rather than one particular disease as there are many forms of dementia, such as Lewy body dementia, frontotemporal dementia, vascular disorders, mixed dementia, or a combination of types; included in this is the most common form of dementia, AD which accounts for 60–80% of cases [15–17]. It is important to highlight that dementia is not a normal part of aging and is directly caused by damage to the brain that affects an individual’s ability to communicate which in turn affects thinking, behavior, and feelings. There are four elements to this syndrome 1) dementia affects cognition (memory, attention, organization, learning, executing actions, etc.); 2) the affect is global meaning multiple areas of cognition are affected; 3) the symptoms show a decline in functioning meaning over time they grow in severity; 4) there is a distinct absence of delirium (a sudden state of severe confusion and rapid changes in brain function) [18]. With these four hallmarks come neuropsychiatric and neurological symptoms which include changes in mood, agitation, and at times violence as well as changes in gait, continence, and in some cases seizures [18].
WHAT IS ALZHEIMER’S DISEASE?
AD is defined as a late-onset progressive neurodegenerative disorder, characterized by memory loss and multiple cognitive impairments. Currently over 50 million people worldwide, including 6.2 million Americans suffer from AD [1]. It is a well-known fact that two thirds of women and one third of men are at a lifetime risk for AD [18]. It is hypothesized that this discrepancy is due to a higher incidence of depression and anxiety in women [19]. There are also known correlations between AD and women undergoing ovarian failure and the inability to produce ovarian steroids. Without estradiol, serotonin neurons deteriorate and become dysfunctional which is believed to precede or occur alongside AD in female patients [18, 20].
The major pathological hallmarks of the disease are Aβ plaques, neurofibrillary tangles (phosphorylated tau), mitochondrial abnormalities, and synaptic damage [18, 21]. From what research has shown so far, loss of synapses and synaptic damage are the best measures of correlation between physical manifestations of the disease and cognitive decline in AD patients [22–24]. It has also been established that synaptic loss/damage and mitochondrial dysfunction are early events in the pathogenesis of AD [22, 26]. The current known sites of pathology within the brain are the entorhinal cortex, temporal cortex, frontoparietal cortex, hippocampus, and subcortical nuclei [27]. Outlined in the figure below are factors that may contribute to AD, including both non-modifiable and modifiable factors (Fig. 1).

Summary of risk factors associated with Alzheimer’s disease (AD). Multiple risk factors are involved in late-onset AD, including lifestyle-unhealthy diet and physical inactivity, traumatic brain injury, chronic conditions such as diabetes/obesity, cardiovascular, hypertension, kidney disease, epigenetic factors, and environmental and occupational exposures.
In addition to this there have been many studies conducted focusing on early-life exposure on late life disorders including AD. This idea is based on the Latent Early-Life Associated Regulation model (LEARn) and has experimental evidence from studies involving rodents, primate, and humans [28]. LEARn proposes that exposure to environmental agents at the early developmental stages of life can disturb gene regulation in such a way that creates long term effects which eventually build up to cause pathological symptoms later in life [28, 29]. The model operates through the promoter of specific genes that has been changed via methylation or oxidative damage within the regulatory region [28]. This novel idea is significant in our proposed protocol as it combines both genetic and environmental risk factors in an epigenetic fashion that may explain the origin of neurobiological disorders.
Currently, it is not known in AD when the progression of the disease begins or how long the process takes and while some studies have established that risk for AD occurs in early adulthood much is still left unclear [28]. The confusion is then further elucidated as research has well-established risk factors in both genetic and environmental studies. Thus resulting in the emergence of the LEARn model which takes into account both genetic and environmental factors. The proposed theory in relation to AD believes it to be a “two-hit” disorder where the first hit would occur due to environmental stress likely during early childhood [30]. This first hit would cause stress within the regulatory sequences of AD-associated genes and is then maintained by the resulting epigenetic changes such as DNA methylation. The second hit would cause further stress and examples include head trauma, poor diet in mid-life, or other changes in expression of genes that occur later in life separate from the pathology of the disorder [30].
Stages of AD
There are 3 broadly classifiable stages of AD based on physiological disease progression and appearance of clinical symptoms. These are early-stage (mild), middle-stage (moderate), and late-stage (severe). However, before an individual begins to show symptoms of AD, they might be placed within a preclinical stage of AD for several years and then progress to mild cognitive impairment (MCI) [16, 31].
Preclinical AD
This is characterized by a pathological progression of the disease in the absence of clinical symptoms. This stage can last anywhere from 10–20 years [31, 32]. Currently, there are no therapeutic strategies that target this stage, but it is an area of investigation that has received increased attention in recent years.
Mild cognitive impairment
MCI is a concept that has received traction over the past two decades. It can be defined as the state of cognitive decline that exceeds normal aging, but precedes dementia. MCI is not exclusive to AD as it is seen to present in other neurodegenerative conditions as well. However, it is almost always a precursor to clinical AD and if treated can reduce or prevent the disease progression of AD [16, 32]. Hence, the increase in attention to both MCI and preclinical AD over the past several years.
Early-stage (mild) Alzheimer’s disease
This is the stage where symptoms of AD first start to appear. AD is often diagnosed in this stage. At this stage the person may feel as if he or she is having memory lapses, such as forgetting familiar words or the location of everyday objects. Symptoms of early stage include difficulty with problem-solving, complex tasks and sound judgments, changes in personality, difficulty organizing and expressing thoughts, getting lost or misplacing belongings, forgetting material that was just read and experiencing increased trouble with planning or organizing.
Middle-stage (moderate) Alzheimer’s disease
This is the longest stage and can last for several years. As the disease progresses, people with AD require an increased level of care. At this stage, nerve cells in the brain are damaged which makes it difficult for the person to express thoughts and perform routine tasks without assistance. Symptoms at this stage may include being forgetful of events or past and personal history, feeling moody or withdrawn in socially or mentally challenging situations, difficulty to recall information about themselves like their address or telephone number, and the high school or college they attended, experiencing confusion about their status like where they are or what day it is, requiring help choosing proper clothing for the season or the occasion, difficulty controlling their bladder and bowel movements, experiencing changes in sleep patterns such as sleeping during the day and becoming restless at night, increased tendency to wander and get lost and demonstrating personality and behavioral changes, including suspiciousness and delusions or compulsive, repetitive behavior like handwringing or tissue shredding.
Late-stage (severe) Alzheimer’s disease
This is also called severe dementia due to AD. In this stage, mental function continues to decline, and the disease has a growing impact on movement and physical capabilities. In late-stage severe dementia due to AD, people generally lose the ability to communicate coherently, require around-the-clock assistance with daily personal care, lose awareness of recent experiences as well as of their surroundings, experience changes in physical abilities, including walking, sitting and, eventually, swallowing, and become vulnerable to infections, especially pneumonia. Multiple factors are involved in late-onset AD, including lifestyle (unhealthy diet and physical inactivity), traumatic brain injury, chronic conditions such as diabetes/obesity, cardiovascular, hypertension, kidney disease, epigenetic factors, and environmental and occupational exposures [32].
DEMOGRAPHIC CHARACTERISTICS OF WEST TEXAS
The area in rural West Texas is a 131,000 square mile service region, comprising 50% of the landmass and 11% of the population of Texas. The cities of Lubbock, Midland, Odessa, and El Paso are included in the area known as rural West Texas. West Texas has a population of 2.7 million people who live within a highly underserved area by health care professionals and health care facilities, despite the contributions made by Texas Tech University Health Sciences Center and other research and educational institutions in Texas to reach the rural West Texas population [16, 32]. This fact is even more disconcerting as statistics indicate that an unhealthy lifestyle and poor dietary habits have caused Hispanic men and women to have a higher incidence of chronic diseases across the US and in rural west Texas. Non-Hispanic African Americans also have a 17% higher prevalence of chronic diseases. With underserved areas and an inability to access proper healthcare the risk to racial minority patients in rural West Texas is high.
High prevalence of chronic conditions
A high prevalence of chronic conditions has been reported in rural West Texas, these include diabetes/obesity, respiratory diseases, kidney disease, hypertension, and neurological diseases [16, 32]. According to a report published by the Texas Department of State Health Services [33] the leading preventable causes of mortality in Texas were cardiovascular disease, cancer, and diabetes. Among these, heart disease was the leading cause of death among all ethnic groups [33]. According to the Center for Disease Control & Prevention, rates of heart disease are higher in rural West Texas, particularly in Hispanic populations. Hispanic men are also reported to have their first stroke at younger ages than non-Hispanic whites: the average age for a first stroke among Hispanic men was 67, far younger than the age of first stroke for non-Hispanic whites, which was 80 years [32]. However, age adjusted rate of death caused by stroke were significantly higher among the African American population according to a Texas DSHS report published in 2014 [34]. According to the Texas Demographics Center, the prevalence of diabetes is higher in Texas (11.2%) compared to the rest of the US (9.4%) 328]. The African-American (17%) and Hispanic populations (12.2%) continue to have the highest deaths caused by diabetes related complications after adjusting for age. The prevalence of diabetes is also highest among older adults (>65 years) [34, 35].
According to the CDC, Hispanic men and women in the US are at a greater risk for kidney disease than non-Hispanic white men and women and are also 1.5 times more likely to have kidney failure compared to non-Hispanic white men and women [32]. In 2015, the CDC reported that 13% of new kidney failure patients were Hispanic, compared to 5% of non-Hispanic whites, but it is not yet fully understood as to why. Researchers have speculated that these differences may be due to the higher percentage of Hispanic men and women who have type 2 diabetes (T2DM), which is the leading cause of kidney disease: 10% of Hispanics were determined to have T2DM, compared to 3% of non-Hispanic whites [32]. Lifestyle features influencing the onset of diseases such as stroke, T2DM, and kidney disease—and of dementia—have not been researched in Hispanic and non-Hispanic white populations in the US nor has it been researched for rural populations. It has been hypothesized that the lifestyle of Hispanic men in rural West Texas impacts not only the prevalence of dementia, stroke, T2DM, and kidney disease on this population, but their lifestyle also impacts the age at which they develop these diseases.
Ethnic factors
A large portion of Hispanic/Latinos have been reported to reside in rural West Texas. As of 2018, Hispanics or Latinos comprise 40.2% of the total Texas population. In fact, current projections predict that Hispanic Americans will face the largest increase in burden with regards to AD due to their rapid population growth within the US. To be specific, the state of Texas has seen a steady increase in the population growth of Hispanic Americans; especially the counties of West Texas.
Racial disparities with regards to the development of age-related chronic diseases as well as various risk factors reveals that the future burden of AD lies upon individuals of specific racial backgrounds such as Hispanic or Latino Americans as well as African Americans. Furthermore, due to differences in pre-existing medical conditions, social behaviors, and socioeconomic status, minority populations face a higher risk of AD dementia and other dementias when compared to the non-Hispanic white population. In addition, health conditions such as diabetes, high cholesterol, atherosclerosis, cardiovascular disease, and kidney disease are more prevalent in racial minority groups leading to an increased risk in developing AD. A low socioeconomic status in turn contributes to the increase in the prevalence of such health conditions thereby further increasing the risk of AD in racial minority groups.
Economic conditions
The per capita income is low in Texas compared to the overall US per capita income; however, per capita income of rural West Texas is even lower than Texas [16, 31]. This indicates a low economy in rural West Texas—in other words, most residents of rural West Texas are below the poverty line. Percent of poverty is also increased in children and persons above 65 years of age in rural West Texas. Health care is a major economic industry in the rural area. In communities that still have a local hospital or nursing home, health-related businesses are often the largest employers. For every health care dollar generated locally, an estimated 1.5 dollars are brought into the community economy. Therefore, immigration of Hispanic persons from rural counties in West Texas to more urban areas is a major contributor to the loss of local revenues, which ultimately reduces the funds available to spend on health care in rural West Texas, and 70–80% of out–migration is due to the availability of care facilities [16, 31].
Throughout West Texas, population density is low, making it difficult to maintain health care services since there are not enough patients to support medical practices and institutions. The lack of access to proper healthcare in this region occurs whether the population is comprised of Hispanics or non-Hispanics, people who are homeless or own homes, whether they are single or married mothers of young or adolescent children, whether they are poor or middle-income, and whether they are living with chronic diseases and disabilities or not.
Education
Education levels are reported to be low in Texas compared to the US national average. Between 2014 to 2018, the percentage of individuals aged 25 years and older who held a bachelor’s degree or higher in the US was 31.5% while Texas fell below the national average at 29.3%. Similar patterns were noted where Hispanic or Latino Americans registered for the lowest level of educational attainment when directly compared to other groups in Texas [32]. Although they accounted for over 40% of the total population of Texas in 2018, a mere 15.2% of Hispanic or Latino Americans held a bachelor’s degree or higher. The percentage of students who do not graduate from high school is significantly higher among the Hispanic and African American populations as compared to Caucasians. 54% Hispanics and 56% African Americans complete high school as compared to 78% [36].
WHAT IS AGING?
Aging is any time-dependent physiological deterioration that occurs in all organ systems and may lead to changes such as cardiac output decreasing, blood pressure increasing, and lean body mass declining primarily seeing a loss of muscle cells [37, 38]. As we age, the brain naturally changes, affecting memory, learning, and other cognitive functions including signs of shrinking which occurs due to changes in vasculature [38] (Fig. 2). All of these aspects are normal parts of senescence; however, aging is still a major risk factor for age-related diseases such as AD, Parkinson’s disease, cancers, and many others [39].
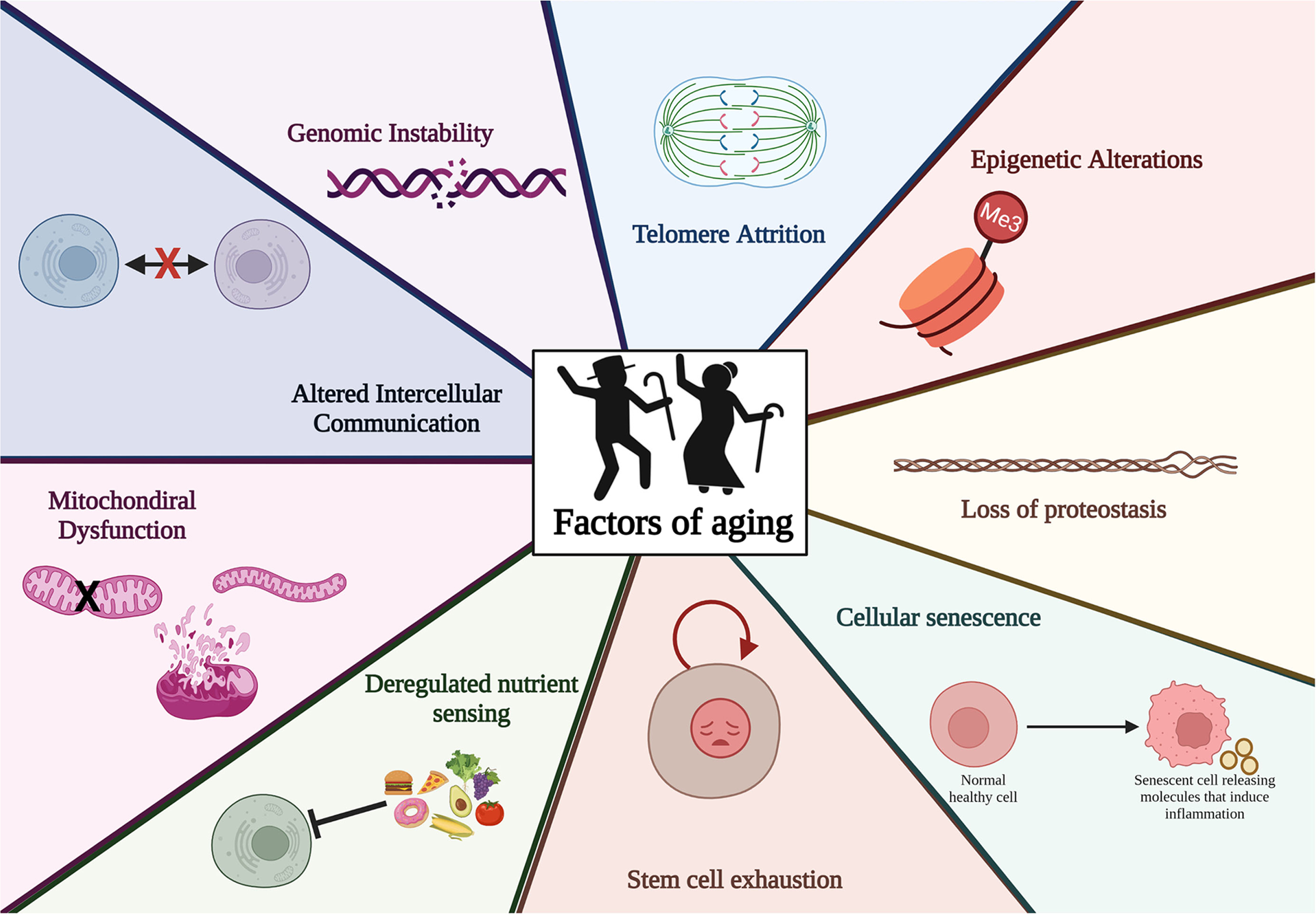
Factors associated with aging in elderly individuals. The nine factors associated with aging including genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, cellular senescence, stem cell exhaustion, deregulated nutrient sensing, mitochondrial dysfunction, altered intercellular communication.
Aging is generally thought of as the time-dependent accumulation of cellular damage and decline in physiological function [40, 41]. Although many events can lead to cellular dysfunction, nine factors have been identified and commonly accepted as the defining characteristics of aging: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient sensing, cellular senescence, stem cell exhaustion, altered intercellular communication, and mitochondrial dysfunction [40–42]. These factors are divided into three distinct categories 1) primary hallmarks, 2) antagonistic hallmarks, and 3) integrative hallmarks. All primary hallmarks are considered explicitly negative in their effects on the body which includes DNA damage, mitochondrial dysfunction, telomere loss, epigenetic drift, and defective proteostasis [42]. However, antagonistic hallmarks effects on the body depend on the intensity of the processes at work, specifically at low levels they may have beneficial effects while at high levels they can become toxic. This is where senescence, reactive oxygen species, and optimal nutrient sensing come into play. At low levels they serve protective functions but when increased and chronically functioning these processes can cause more harm than good. The integrative hallmarks play their role in aging when primary and antagonistic hallmarks have accumulated so much damage that tissue homeostatic mechanism cannot compensate properly. Thus, resulting in stem cell exhaustion and altered intercellular communication [42].
WHAT IS HEALTHY AGING?
Healthy aging is defined by the WHO as the process of developing and maintaining the functional ability that enables wellbeing in older age [43]. This is done by adopting what is deemed as healthy habits and behaviors, staying involved in the community or having a strong social support network, using preventative services (regular checkups with doctors, etc.), managing health conditions (taking prescribed medications, etc.) (Fig. 2), and understanding all the factors that contribute to a productive and meaningful life [43]. Good brain health is also of utmost importance in the preservation of optimal brain integrity as well as maintaining proper cognitive, emotional, psychological, and behavioral functioning to continue to cope with life situations and changes [20, 43].
Healthy aging is not as easily definable as aging itself as there are many ways to describe healthy aging for example vital aging, active aging, productive aging, etc. [44]. The common indicators of healthy aging include good quality of life/well-being, survival to a specific age in good health, autonomy in activities of daily living (ADL), no or only a few chronic diseases, little or no disability, little or no mild cognitive or functional impairment, high social participation, and regular healthy habits of behavior (physical activity, diet, etc.) [45].
STUDIES CONDUCTED AT TTUHSC SINCE 2015
We have been studying several aspects of aging, chronic conditions, and dementia in rural West Texas populations for the last 2 decades here at TTUHSC and have published a multitude of articles [32, 46–55].
Recently, several human studies have been conducted focusing on age-related chronic diseases and AD in Texas: a Hispanic focused study [32], lifestyle and reduced risk of dementia in rural west Texas [16], current issues in chronic conditions, a focus on dementia and hypertension [51], sex differences in cardiovascular disease and cognitive dysfunction in rural West Texas [52], gender differences in prevalence of myocardial infarction in rural West Texas [54], can healthy lifestyle reduce disease progression of AD during a global pandemic of COVID-19 [55], and chronic conditions such as disparities in breast cancer in rural West Texas [56].
Table 0
In addition, in 2018 we conducted a symposium on healthy aging and dementia research in rural West Texas.’ The purpose of the ‘First Regional Healthy Aging and Dementia Research Symposium’ was to discuss the latest research in healthy aging and dementia, public health trends related to neurodegenerative diseases of aging, and community-based programs and research studying health, nutrition, and cognition. This symposium was organized by the Garrison Institute on Aging (GIA) of the Texas Tech University Health Sciences Center (TTUHSC), and was held in Lubbock, Texas, October 24-25, 2018. The Symposium joined experts from educational and research institutions across the US and included presentations from GIA staff and researchers, students, postdoctoral fellows, and faculty members involved in dementia research as well as healthcare professionals from geriatricians to social workers working with patients with neurodegenerative diseases. This event was comprised of multiple sessions, each with several oral presentations, followed by questions and answers, and discussion [50].
WHY OUR STUDY IS UNIQUE
Our healthy aging study is a large paradigm shift in that we intend to understand the biology of healthy brain aging and the factors that may promote heathy brain aging. As mentioned above, the aging process is an unavoidable, time-dependent physiological and pathological accumulation in the body and brain. Despite these age-dependent pathologies, some individuals can maintain healthy brain and body function into their later stages of life. Our ongoing study hopes to unravel the factors that promote healthy brain aging and cognitive functions.
In the last several decades, researchers have focused on changes in the brain and body in patients with AD by utilizing brain scans and assessments based on cognitive abilities/function and correlating these changes with blood and cerebrospinal fluid markers (Aβ, P-tau, and other proteins). We have learned a great amount during these intense investigations in patients with AD. However, currently, we do not have a complete understanding of normal, healthy brain changes, particularly in various racial and ethnic groups with different genetics, lifestyles and genders.
What is positive deviance?
Positive deviance is an observation that in every community there are certain individuals or groups whose uncommon behaviors and strategies enable them to find better solutions to problems than their peers, while having access to the same resources and facing similar or worse challenges [57]. The positive deviance approach is an asset-based, problem-solving, and community-driven approach that enables the community to discover these successful behaviors and strategies and develop a plan of action to promote their adoption by all concerned parties [57].
The positive deviance collaboration seeks to provide resources for those wanting to use this approach for both programmatic and research purposes, which will allow for access to practitioners, and periodic updates on positive deviance materials, guides, current projects, and publications. In the current study, we seek to understand the underlying factors that promote healthy brain aging in aged individuals in rural West Texas. The outcome of our study will be useful in that it can be applicable to families of patients with chronic conditions and dementia.
Summary
Our goal is to understand what makes some individuals live without cognitive impairments even at the age of 60–90 years, whereas others develop chronic conditions such as diabetes/obesity, hypertension, kidney disease, and cognitive impairments much earlier, around 50–60 years. We also aim to understand the factors that delay aging in some individuals, but not in all. Therefore, in our healthy aging study, we propose to collect the following information and material and investigations: ethnographic profile, cognitive assessment, blood-profile investigation, brain scans, and blood-based on genomic analysis (RNA-seq, microRNA, and RNA species) in relation to lifestyle. In addition to this, we hope to share resources and information found during the course of this study and others with the community of rural West Texas.
Table 1
OUR PROTOCOL
Individuals will be classified into two groups: the healthy cognition group (n = 4,000) and general group (n = 500) (Fig. 3). The healthy cognition group are composed of individuals without any of the following diagnoses: possible AD, dementia due to other diseases, degenerative dementia, Parkinson’s disease, primary or secondary brain tumors, Huntington’s disease, Pick’s disease, Creutzfeldt-Jakob disease, thyroid disease, intellectual or developmental disability, human immunodeficiency virus, MCI, and diffuse white matter disease. The general groups are composed of individuals without any of the conditions mentioned above but having MCI and/or AD and related disorders.
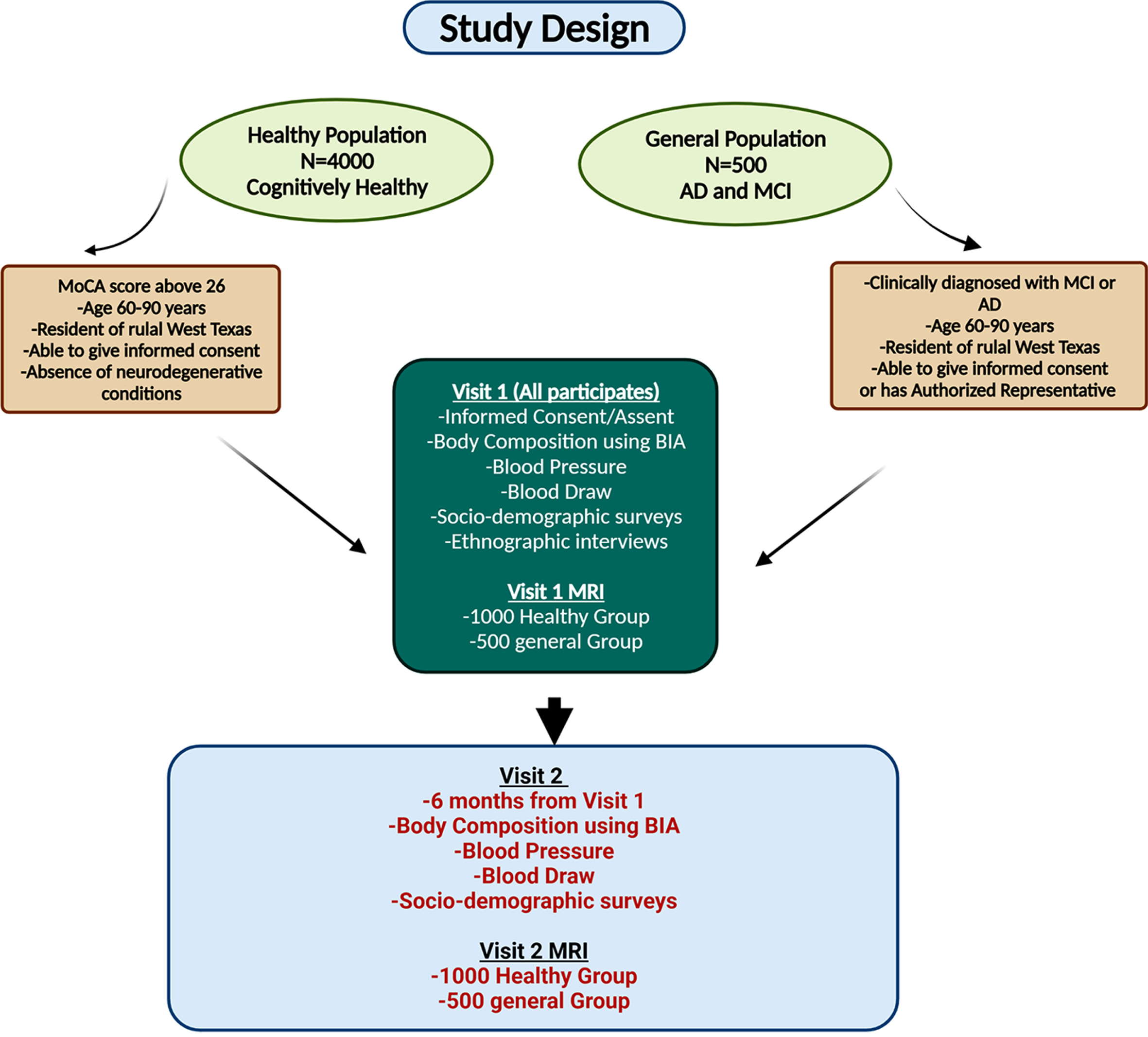
Summary of healthy aging study design in healthy aging individuals and Alzheimer’s disease (AD) patients. The study consists of two population groups Healthy (no known cognitive impairments) and General (diagnosed with mild cognitive impairment (MCI), dementia, and/or AD). Each group will undergo an initial visit that consists of informed consent, bioelectrical impedance (BIA) scan, blood pressure and draw, sociodemographic surveys, and an ethnographic interview. 1,000 of the healthy group and all participants from the general group will undergo an MRI. A second visit will be conducted six months later that is the same as visit 1 also with 1,000 of the healthy group and all the general group undergoing a second MRI.
A factorial analysis will be performed by our statistician to determine the factors that differ between the healthy cognition group (positive deviants) and the general group. Wellness will be measured by a series of survey instruments. Cognition and anthropometrics will be assessed by direct measurement. Health history will be obtained by means of self-report.
Table 2
The survey instruments contain total of 115 items; thus, the respondent burden is a potential issue. A meta-analysis of survey research has shown no significant associations between instrument length and the number of missing values [58]. The most important issue was not length, rather it was how the survey was administered, with in-person administration having the highest response rates. Participant interest in the survey topic increased responses even in long surveys [59, 60], because this is a long survey, to minimize item order effect, we will randomly assign the survey order for each participant [60–62]. The data collectors will be trained in administering surveys in interview format in either English or Spanish while simultaneously recording the subject responses in corresponding digital data sheets created using Microsoft Excel. We will train all data collectors to 0.80 agreement on all surveys that require clinical assessment. For patients with MCI or dementia, a medical Power of Attorney (POA) or a Legally Authorized Representative (LAR) may answer survey questions on their behalf, when applicable.
Wellness (Refer to attached document titled: Wellness Surveys)
Measured by 1) ADL, 2) stress/anxiety, 3) well-being, 4) sleep, 5) spirituality, 6) physical activity, and 7) healthy food intake using the following survey instruments. ADL will be measured by the Functional Autonomy Measurement System (SMAF), a 29-item scale [63].
All available information is used for the rating (data collector questions the individual and/or the POA/LAR, observes the individual and their environment). SMAF measures functional ability in 5 areas: ADL [7 items], mobility [6 items], communication [3 items], mental functions [5 items] and instrumental activities of daily living (IADL) [8 items]. For each item, the disability is scored on a 5-point scale: 0 (Independent), –0.5 (with difficulty), –1 (needs supervision), –2 (needs help), –3 (dependent). SMAF test-retest reliability is 0.96 (95% confidence interval) and 0.93 to 0.98 for interrater reliability. All 7-variables will be collected and analyzed.
Health
Measured by the Charlson Comorbidity Index (CCI). We will calculate the CCI [64]. The CCI adds explanatory power to account for variations in factors due to the immediacy of a disease. The data will be obtained using self-report.
Medical diagnosis
Screened for the type and duration of chronic diseases. Medications are screened for the potential for affecting memory and cognition.
We will perform in-depth qualitative interviews to elucidate themes on an individual’s perception of their aging and cognition.
Sample
We will purposively sample individuals in the healthy cognition group (positive deviants) for in-depth qualitative interviews. Purposive criterion sampling will select individuals to obtain diverse perspectives by gender, poor physical health, and socio-economic status. Selection will further be informed by the factorial analysis, should other relevant group differences emerge in analysis of that data [65].
Interview procedures
Each interview will be audiotaped and transcribed for analysis. By inter-and intra-comparison of participant responses (constant comparison), we will describe salient patterns. Interviews will use semi-structured format and explore how the individual perceives their aging and memory. Responses will be reviewed periodically for theme saturation as interviews from individuals with similar characteristics have been obtained.
Ethnographic data will be analyzed using Atlas.ti [66] and assigned in-vivo codes (line-by-line) to the words of respondents; these in-vivo codes are then grouped under more abstract (axial) codes by the patterns or themes that emerge from comparing shared characteristics and meanings (a dictionary of code meanings is provided). Under the supervision of, and after training by Dr. Gittner, coding reliability is to be established by several researchers independently coding a sample of interviews; these efforts are to be merged and a master codebook created. A validity assessment of the final data set is to be produced by: 1) double-checking to assure the codes referring to quotations are consistently applied across all interviews; 2) double-checking to assure codes are appropriately grouped under the thematic categories; and, 3) double-checking to assure themes are appropriately grouped under the axial codes. Member checking will be used to assure the trustworthiness of the themes. Member checking is a hermeneutic approach to take the results back to participants to assure we have interpreted their words consistently and credibly.
Biologic wellness
Data collectors will be trained in appropriate calibration and use of all equipment. We will train all data collectors to 0.80 agreement. Anthropometric measurements will be measured using all medical grade equipment. Biologic wellness will be measured by body fat percentage, blood pressure, body mass index, and carotenoid value.
Body fat percentage and body mass index
These will be measured by a bioelectrical impedance (BIA) device, TANITA BC-418 segmental body composition analyzer, or a similar device. BIA is simple, quick, and noninvasive and provides reliable measurements of body composition with small intra- and interrater variability [67]. The accuracy of BIA devices measurement may be influenced by several factors, such as body shape, hydration status, and obesity [67, 68]. Participants will be informed about taking the following standard measures prior to the testing in order to get the most accurate results:
They will be asked not to eat a meal and drink large amounts of fluid at least 2 to 3 h prior to the test.
They will be advised to drink sufficient fluids over the 24 h before the test, with the exception of coffee for 3 h and alcohol for 24 h before the test respectively.
Participants will be told to not exercise 12 h before the test.
They will be asked to empty their bladders (urinate) at least 30 min prior to testing.
In order to ensure comfort of the participants, study visits may be scheduled in the mornings which will help reduce the amount of time the subjects have to stay in a fasted state (must have fasted about 4 h) since the time of awakening if they so choose to. Participants will stand barefoot on metal electrodes on the scale pad while grasping a pair of electrodes fixed on a handle with arms extended in front of their chest for 30 s. All BIA measurements will be completed by a trained investigator according to the device manufacturers’ instructions.
Blood pressure
Blood pressure will be measured by the OMRON R3 blood pressure self-measuring device which has been validated for use in research [69]. Resting blood pressure measurements will be collected after the participant has been sitting for at least 10 min. Measurements will be performed in a sitting position; systolic and diastolic blood pressure will be measured using the Omron R3 around the left wrist held at the subjects’ heart level [69]. The instrument will be set to where it will take two consecutive measurements with a 1 min gap between the two and provide the average reading for both.
Biomarkers in blood analysis
Fasting blood samples contain various biomarkers that can indicate the presence or absence of diseases. A trained phlebotomist/nurse will draw 10–15 millimeters of blood from the subject which will then be sent to the UMC pathology lab where the blood sample collected will be tested for: Complete Metabolic Panel (CMP), Complete Blood Count (CBC), thyroid stimulating hormone (TSH), free thyroxine (fT4), Rapid Plasma Reagin (RPR) with reflex to Venereal Disease Research Laboratory (VDRL) test for syphilis, Vitamin B12 and Methylmalonic acid to test for vitamin B12 levels, Red Blood Cell (RBC) count, Folate levels, hemoglobin A1C to test for diabetes or prediabetes, Lipid panel the will include levels of total cholesterol, triglyceride, High Density Lipoproteins (HDL), and Low Density Lipoproteins and Erythrocyte Sedimentation Rate (ESR) to test for presence of inflammation. A sample of blood will also be assessed for global microRNA analysis using RNA-sequencing at the Texas Tech University Genomic Facility. The data obtained will help provide vital information about the status of the subject’s physical and cognitive health. Standard methods of assay will be used for all blood tests, which will ensure reproducibility of the same.
Cognitive assessment
The Montreal Cognitive Assessment (MoCA) test has 30 questions and can be taken online or on a paper version. This is a standardized test used to screen for dementia and MCI. The test takes between 10–15 min to administer and tests for the following aspects of cognition: attention and concentration, executive functions, memory, language, visuo-constructional skills, conceptual thinking, calculations, and orientation [70]. A trained researcher will administer the test following all instructions of the test protocol and record the scores. The MoCA score will be used to determine the subject’s cognitive status and used as an eligibility criterion for the Healthy group. As per recommendations of our study clinicians, a score of 26 or higher will be required to be recruited in the Healthy group.
Neuroimaging using magnetic resonance imaging (MRI)
A standard MRI scan of the brain provides high resolution images of the various parts of the human brain. Early onset of AD can be detected through structural atrophy in certain susceptible parts of the brain like the hippocampus and the entorhinal cortex [71]. Loss of volume aside from the structures of the forebrain have been proven to be predictors of future Aβ plaque formation which is an indicator of AD [72]. Therefore, MRI scans of healthy subjects can be compared with MCI, early AD, and severe AD subjects in order to draw comparisons of the degree of structural and white cell atrophy. The MRI scans will be conducted at the University Medical Center Radiology department. At the facility the subject will fill out and sign a standard safety sheet provided by the facility that ensures that magnetic exposure does not run any immediate risks to their health. The questionnaire will include questions about medical implants, surgical devices, metallic cosmetic implants, etc. After that the MRI technician on site, will escort the subject to the 3 Tesla magnet, 48 channel head coil scanner for imaging. The scan will last about 40 min. The images obtained from the scans will be developed by expert neuro-radiologists using the following specifications:
If an MRI result is seen during the study that may be important to the participants’ health (called” incidental findings”), the study team will notify the participant and/ or their POA/LAR. Our clinicians will also relay the incidental findings to their primary care physician for further follow up.
DNA damage
The typical pathological hallmarks of AD, include accumulation of Aβ, tau hyperphosphorylation, synaptic damage, and cell death. Nevertheless, heterogeneity in AD populations, and failure of Aβ-targeted drug trials signal a need to investigate alternative targetable-pathways that may occur upstream in the disease process. A large number of studies supports evidences that oxidative stress is a major contributor to neuronal death in AD. Oxidative stress refers to an imbalance between the productions of reactive oxygen species (ROS) and the efficiency of ROS detoxification. Excessive ROS may be generated by mitochondrial dysfunctions. Numerous studies show increased lipid peroxidation, oxidation of proteins and oxidative DNA damage in brain of patients with AD. Increased level of 8-oxoG, Aβ, and phospho-Tau in the serum are well established in AD, suggesting that oxidative damage to DNA of patients with AD. The presence of oxidative stress markers, including oxidative DNA damage, markers of oxidative damage to cellular macromolecules can be detected in peripheral blood samples of AD patients and useful to detect oxidative damage-related biomarkers of AD. However, further studies on DNA damage are needed to assess the results of ELISA for measuring effective DNA damage markers of AD. We planned to examine the following markers in serum as well as in buffy coats from the blood of AD patients and cognitively healthy aging subjects.
Sample collection
For buffy coat separation, 8 ml venous blood samples will be collected into purple/lavender cap tubes (EDTA coated, BD Vacutainer, BD Biosciences). This sample will be collected during the an already scheduled study visit 1. However, if any participants would like to separate this collection, it can be done anytime within 30 days of the study visit. For serum, 3 ml blood sample will be collected in red cap tubes from BD without additive, from 100 AD patients and 100 age-matched control individuals. Blood samples will be transported to Dr. Reddy’s laboratory to TTUHSC, Internal Medicine department 4th floor by CRI personnel in biohazard container (orange) within 1 h after collection. Serum will be separated by the centrifugation at 5000×g for 15 min and stored at –80°C until the further testing. To determine the protein concentration the Bradford protein assay will be employed.
ELISA assays
Serum samples of known concentration will be used to conduct the following assays. For evaluation of the levels of DNA Damage in both group, enzyme-linked immunosorbent assay (ELISA) for Aβ, Tau, phospho-Tau (ThermoFisher Scientific, MA, USA and Immuno-Biological Laboratories, Inc. MN, USA), and 8OHdG (Cell Biolabs Inc. San Diego, CA, USA) will be used by commercially available kits as per manufacturer’s instructions.
For buffy coat preparation
The buffy coat (BC) will be obtained from high-speed centrifugation of the whole blood by Ficoll–Hypaque density gradient. Ficoll extraction: Whole blood will be diluted at room temperature with an equal volume of 1X phosphate-buffered saline (PBS). And layered over 20 mL of Ficoll-Paque and centrifuged. BC composed mainly of lymphocytes and monocytes granulocytes mononuclear cells (MNC), will then be recovered from interfaces and will be subjected to two washing steps. After that, total number of cells will be counted and cell viability will be measured with trypan blue exclusion. Washed cells will be used to evaluate the extent of DNA damage by very well-established methods routinely used in our laboratory.
To examine the double DNA strand breaks and accumulation of mitochondrial damaged DNA in AD samples compared to their age matched controls, following assays will be performed in the cells from buffy coats:
Comet assay
The Comet assay has been in use for some years, as a method to detect DNA strand breaks in single cells. We examined DNA strand breaks within single cells by comet assay. Assays will be performed under alkaline pH conditions using the Comet Assay Single cell gel electrophoresis Kit (R&D Systems, Minneapolis), as per manufacturer’s instructions. Measurement of percent of DNA in the head and the tail regions of each comet will be analyzed by using the ImageJ open comet program. Means of the median values of % tail DNA and standard deviations will be calculated from AD and age matched control cases.
TUNEL analysis to assess oxidative DNA damage
A terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay (Invitrogen) will be utilized to assess and validate for double DNA strand breaks and apoptotic cell death. Assay for FACS analysis will be performed using an APO-BrdU TUNEL assay kit (Invitrogen). At least 10,000 cells will be analyzed per staining with the BD Accuri C6 Flow Cytometer (BD Biosciences, San Jose, CA, USA).
Western blotting
Cells obtained from the buffy coats will be used to prepare total protein lysates. Equal amount of protein samples will be loaded on gel and electrophoresed. Aβ, Tau, phospho-Tau, gammaH2AX, and EndoG utilizing appropriate mono or polyclonal antibodies, following the standard protocols.
Immunofluorescence analysis (IF)
Western blot analysis will be confirmed by complementary assays as IF and Flow cytometry (FC). For IF staining total cells will be seeded in 4-well BD chamber slides (Fisher Scientific), at a density of 1000 x 103 cells/chamber in complete RPMI medium for 24 h than will be stained for Aβ, Tau, phospho-Tau, gammaH2AX, and EndoG utilizing mono or polyclonal antibodies following the standard protocols.
Flow cytometric analysis
Cells will be analyzed for expression of Aβ+/Tau+/P-Tau+/ gammaH2AX+, and EndoG + cells by flow cytometry. In brief, cell samples (0.5x106–1x106 cells) will be incubated on ice with sample blocking buffer (10% mouse/goat serum+1% BSA) to block nonspecific sites. After 20 min of incubation, samples will be washed and stained with PE (Phycoerythrin)/FITC or APC (Allophycocynin)) conjugated mouse or goat antibodies for Aβ, Tau, phospho-Tau, gammaH2AX, and EndoG. At least 10000 cells will be analyzed per staining with the BD Accuri C6 Flow Cytometer (BD Biosciences, San Jose, CA, USA).
Statistical analysis
To calculate difference between AD and normal groups all analyses will be performed using Prism 6.0 for Windows (GraphPad, San Diego, CA). Each parameter of DNA damage among AD, and normal control will be compared using a Kruskal-Wallis test, followed by the Mann-Whitney and two tailed student’s t–test for pairwise comparisons, or using Wilcoxon matched pairs test. A two-way analysis of variance (ANOVA) with Post-hoc Tukey’s test will be applied when comparing three or more parameters. p values less than 0.05 will be considered statistically significant.
Subjects/recruitment
The general group will comprise 500 patients, both male and female, between the ages of 60–90 years who will be recruited from the investigators’ patient population/clinics over the course of 5 years.
Standard medical practice will be followed diagnose patients with AD. Patients will have to be accompanied by a close family member or friend. Past medical history, surgical history, family history (with focus on dementia in family members, detailed social history, functional history with ADL/IADL, depression screening (using Geriatric Depression Scale) will be obtained during the initial screening. Then the clinician will take a detailed history from patient and from family members of the memory loss, with onset, progression, any triggering factors, course of the memory loss, and which areas of cognition are affected. Clinician will then go through the neuropsychiatric symptoms list and assess social support, caregiver burden, financial state, advance directives, need for medical Power of Attorney. Medication list review will be done in detail: MoCA screening test will be conducted, and blood work will be ordered.
The clinician/medical assistant will give a brief introduction to our study. If the patient is interested in learning about the study, the research team will be contacted to schedule a meeting with them.
The healthy group will consist of 4,000 (2,000 male and 2,000 female) subjects, between the age ranges of 60–90 years who will be recruited from within the community at large by distributing flyers. Interested participants will be able to contact us via email or telephone.
Participants belonging to both groups will be verified for initial eligibility using a telephone or in person screening based on the inclusion and exclusion criteria of the study listed below.
Inclusion criteria: 1) Age range: 60–90 years of age; 2) Location: west Texas, mainly Lubbock and its surrounding areas; 3) Able to answer oral questions in English or Spanish; 4) Healthy group only: A MoCA score of less than 26; 5) General group only: Having been diagnosed with MCI and/or AD and related dementias.
Exclusion criteria: Both groups: 1) Persons with undiagnosed depression or psychosis, mental retardation, cerebral palsy, alcohol use disorder; substance abuse disorder based on self-report; 2) HIV/AIDS, Down syndrome, based on self-report; 3) Post-traumatic brain injury, undiagnosed metabolic disorders, delirium/ metabolic encephalopathy, Parkinson’s disease, Huntington’s disease, or stroke; 4) Primary or secondary brain tumors, Pick’s disease, Creutzfeldt-Jakob disease, thyroid disease, iodine deficiency disorder; 5) Persons taking the following medication: first-generation antihistamines (e.g., diphenhydramine, chlorpheniramine), tertiary tricyclic antidepressants (e.g., amitriptyline), benzodiazepines, nonbenzodiazepine hypnotics (e.g., zolpidem, eszopiclone), skeletal muscle relaxants, antispasmodics (i.e., atropine, belladonna alkaloids, dicyclomine, etc.), barbiturates (i.e., phenobarbital, butalbital), anticholinergics for treatment of urinary incontinence (e.g., oxybutynin, tolterodine, trospium), high doses of opioids, older antiepileptics (e.g., carbamazepine, gabapentin), over the counter sleep aids.
All 500 recruited participants from the general group and the first 1,000 consenting participants from the healthy group will undergo brain MRI scans.
DISCUSSION
AD is a progressive neurological disease, characterized by memory loss and multiple cognitive impairments. With increasing longevity, dementia rates are alarmingly increasing world-wide and AD is becoming a major healthcare concern in society. Increasing evidence suggests that AD effects all races and ethnic groups, with Hispanics/Latinos and African Americans being affected the most, due to lifestyle, genome polymorphisms and increased prevalence of chronic conditions, such as diabetes/obesity, kidney disease, hypertension, and other conditions.
In the last several decades researchers investigated the disease process using 1) epidemiological data, 2) brain pathologies (Aβ, phosphorylated tau, synaptic defects, oxidative stress, mitochondrial changes, inflammatory responses), MRI based bran-scans and changes in the CSF, 3) blood profile changes in AD proteins, microRNA levels and others, and 4) experts/laboratory scientists made cell and animal models using existing AD genetic mutations and polymorphisms and studied the disease progression from birth to terminal stages.
It is clear now there is no animal model that can mimic one hundred percent of the human AD state because of the disease complexity, genome and lifespan differences between human and other animal species and the involvement of multiple dementias in disease progression of AD; however, studies/discoveries are still ongoing and focusing on disease progression and drug development strategies for AD. These efforts have allowed us to increase the basic understanding of the disease process. However, currently, we do not have a complete understanding of normal, healthy brain changes, particularly in various racial and ethnic groups with different genetics, lifestyles and genders.
As discussed above, our healthy aging study is a large paradigm shift in that we intend to understand the biology of healthy brain aging and the factors associated in promoting heathy brain aging, particularly genetics, epigenetic, ethnic, socio-economic, biological, cultural, and/or lifestyle in all races/ethnic groups. Therefore, in our healthy aging study, we propose to collect the following information and material and investigations: ethnographic profile, cognitive assessment, blood-profile investigation, brain scans, and blood-based on genomic analysis (RNA-seq, microRNA, and RNA species) in relation to lifestyle. We strongly believe that outcome of our study will provide new insights about both healthy brain aging and the elderly population of rural West Texas.
To date, there are no published healthy brain studies in the US and abroad. We need a clear understanding of the molecular mechanisms of healthy brain aging, particularly in elderly individuals as well as how and why some individuals age gracefully without cognitive impairments and others do not. Therefore, the outcome of our ongoing study is a paradigm shift to provide a strong base of knowledge geared towards healthy brain aging. The outcome will help us to educate and create awareness in elderly individuals in rural West Texas and hopefully rural areas of the US and abroad. In regards to policy makers as well as state and federal funding agencies, it is important to pay attention to the outcome and take the appropriate measures necessary to financially support the researchers and healthcare professionals needed to serve our elderly and rural populations.
Footnotes
ACKNOWLEDGMENTS
We sincerely thank all the staff at TTUHSC-Clinical Research Institute for their kind support with the active assistance with our aging study. Special thanks to TTUHSC-IRB committee members for their support. The authors would like to thank NIH for funding of our laboratory with various projects: R01AG042178, R01AG47812, R01NS105473, AG060767, AG069333, and AG066347 (to P.H.R.).